
Abstract
Postural tachycardia syndrome (POTS) is a syndrome defined as an increase in heart rate (HR) of ≥30 bpm within 10 min of assuming an upright posture in the absence of orthostatic hypotension (decrease in blood pressure (BP) >20/10 mmHg). The prevalence of POTS has been estimated as 500,000–3,000,000 patients in the USA. Because it affects mainly women between 13 and 50 years of age, the impact on productivity at work and lifestyle can be devastating. Considerable clinical overlap exists between POTS and vasovagal syncope (VVS) with patients experiencing similar orthostatic symptoms related to insufficient adaptation to blood volume shifts during upright posture. Nevertheless, differences emerge during head up tilt table testing. In patients with POTS, during upright tilt, sympathetic tone increases, there is an early and sustained tachycardia, and patients complain of presyncope without frank syncope. In contrast, patients with VVS experience delayed symptoms and abrupt drops in BP and HR and are more likely to lose consciousness. Treatment of POTS includes exercise and medications directed at decreasing sympathetic tone or increasing blood volume.
Research Funding
Supported in part by NIH grants R01 HL102387, P01 HL56693, and UL1 TR000445 (Clinical and Translational Science Award).
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Key Points-
Postural tachycardia syndrome (POTS) is a syndrome in which an excessive increase in heart rate upon assumption of upright posture, in the absence of orthostatic hypotension, is the final common pathway for multiple overlapping pathophysiologies.
-
Presyncopal symptoms in POTS may resemble those in vasovagal syncope (VVS).
-
In contrast to the immediate increase in heart rate during upright posture in POTS, there is a delayed, albeit abrupt fall in blood pressure and heart rate with standing in VVS.
-
Treatment of POTS includes exercise and medications directed at decreasing sympathetic tone or increasing blood volume.
1 Introduction
Postural tachycardia syndrome (POTS) was first officially described as a syndrome by Schondorf and Low in 1993 [1] and was most recently defined in 2011 [2]. A diagnosis of POTS is currently based on an increase in heart rate (HR) of ≥30 bpm, within 10 min of assuming an upright posture (standing or upright tilt), in the absence of orthostatic hypotension [decrease in blood pressure (BP) > 20/10 mmHg]. In young children, a higher HR threshold (≥40 bpm) should be used, since healthy younger children have a greater physiological orthostatic tachycardia.
The exact prevalence of POTS is not known, with estimates that range from 500,000 [3] to 3,000,000 patients in the United States, and a female:male ratio of 4–5:1. Because POTS usually presents between 13 and 50 years of age, the impact on productivity at work and lifestyle can be devastating [4–6]. The prognosis for adolescents diagnosed with POTS is more favorable for recovery than for newly diagnosed adults [7, 8], but long-term follow-up data is lacking. Patients with a postviral onset may have a better chance of symptom resolution than patients with more hyperadrenergic features, who may require therapy indefinitely [8].
2 Differential Diagnosis of POTS
The evaluation of a patient suspected to have POTS first requires a detailed history and physical examination. Known causes of orthostatic tachycardia must be considered and excluded. These include, but are not limited to, acute dehydration, diabetes mellitus, cardiomyopathy, heavy-metal poisoning, Sjögren’s syndrome, systemic lupus erythematosus, deconditioning, inappropriate sinus tachycardia, pheochromocytoma, thyrotoxicosis, or manifestations of a paraneoplastic syndrome [2]. Potentially deleterious medications, such as diuretics, anxiolytics, stimulants, and vasodilators, must be taken into account [2, 9].
The tachycardia of POTS is a sinus tachycardia, and an ECG or Holter monitor should exclude the presence of an accessory bypass tract and arrhythmogenic causes of syncope [7]. Structural problems and cardiomyopathy should be ruled out. The chest pains in POTS are almost never due to coronary artery obstruction, but are sometimes associated with electrocardiographic changes in the inferior leads, particularly when upright [10]. Inappropriate sinus tachycardia (IST) can resemble POTS, though IST patients generally have an elevated resting HR (often >100 bpm during daytime rest) [11] in contrast to the high normal heart rates seen in POTS. Whereas patients with IST may benefit from sinus node ablation, this procedure is rarely effective for the orthostatic tachycardia of POTS [8]. In addition to a cardiac consult, a neurologist may be asked to evaluate headaches or dizziness. A gastroenterology consultation may be requested if abdominal pain and nausea are present. Blood tests for serum electrolytes, a complete blood count, liver and thyroid functions, a celiac panel, and vitamin B12 are generally normal, but may be useful to rule out other conditions that cause dizziness, fatigue, and gastrointestinal symptoms.
3 Clinical Characteristics of POTS
POTS is a chronic condition with symptoms of orthostatic intolerance persisting at least 6 months. Symptoms improve with recumbence [9], and can also be triggered by exercise, heat, or sometimes by food [12]. Patients complain of both cardiac symptoms (palpitations, lightheadedness, chest discomfort, shortness of breath) and noncardiac symptoms (mental clouding, headache, nausea, tremulousness, blurred vision) [9]. Acrocyanosis is apparent in the legs and feet of approximately 50 % of patients. Gastrointestinal complaints are fairly common [12]. Sudomotor testing may be abnormal [12]. Some patients meet the diagnostic criteria for chronic fatigue syndrome [13]. Exercise intolerance exacerbates deconditioning, and the activities of daily life are limited [9, 14].
Significant diurnal variability has recently been reported for the orthostatic tachycardia of POTS [15], with an exaggerated orthostatic tachycardia in the morning compared to that in the evening. The standing HR decreases by late-morning [16]. It is therefore recommended that postural testing be performed in the morning to optimize diagnostic sensitivity for POTS [9].
Patients with POTS frequently have hyperextensible joints [17]. Wallman et al. [18] reported an 18 % prevalence of Ehlers–Danlos syndrome in their POTS population, compared with a 0.02 % prevalence cited for the general population, and 4 % prevalence in their autonomic clinic patients without POTS.
Most patients with POTS complain of fatigue. The prevalence of chronic fatigue in POTS patients has been reported as 48–77 % and of chronic fatigue syndrome (CFS) is 17–23 % [13]. Bagai et al. reported that compared to healthy subjects, POTS patients describe poorer sleep quality, more daytime sleepiness, and greater fatigue [6]. By actigraphy, POTS patients have diminished sleep efficiency [19].
The quality of life for patients with POTS is comparable to chronic obstructive pulmonary disease or congestive heart failure [20], likely due to exercise intolerance, fatigue, and orthostatic symptoms [6, 20]. Physical health domains are primarily affected, while mental health domains are relatively preserved.
4 Comparison of Vasovagal Syncope and POTS
Considerable clinical overlap exists between vasovagal syncope (VVS) and POTS. VVS can be diagnosed at any age, though the first fainting episode usually occurs in the second and third decades, also the period during which POTS is often diagnosed. The female predominance is somewhat less in VVS than POTS (60 % vs. 85 %). Many patients with POTS do not have frank syncope, though presyncope may occur daily [9, 21]. Though VVS may also occur with pain, anxiety, and exercise, head-up tilt table testing can be used in the clinic to differentiate between POTS and VVS. In addition to a syncope outcome, the hemodynamic response to upright posture differs between the two disorders.
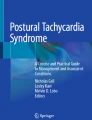
A series of physiological adaptations occur with standing to maintain BP and cerebral perfusion [5]. The characteristic hemodynamic patterns of VVS and POTS result from failures of these physiologic compensatory mechanisms (Fig. 14.1). In patients with POTS, venous return remains inadequate in the face of enhanced plasma volume shifts from the vascular space to the interstitial space, sympathetic tone increases vigorously, and orthostatic tachycardia is exaggerated with BP unchanged (or even increased) [5]. Patients may complain of symptoms throughout the tilt test, but do not faint. On the other hand, in VVS, upright posture is associated with a generally delayed but abrupt decrease in stroke volume and cardiac output with bradycardia and hypotension [22], and resultant cerebral hypoperfusion leading to a sudden loss of consciousness [23] (Fig. 14.1).

Traces from head-up tilt table tests for a patient with POTS (top) and with VVS (bottom). For POTS, there is an early and sustained increase in heart rate and a slight increase in blood pressure with tilt. For VVS, heart rate and blood pressure increase slightly at the tilt onset, but are maintained at levels close to the baseline, until abrupt falls just before the tilt table is lowered
5 Pathophysiological Mechanisms in POTS
POTS is not a single disease. POTS should be considered as a “final common pathway” for a number of overlapping pathophysiologic processes. Thus, POTS is a heterogeneous syndrome with multiple contributing causes.
5.1 Hyperadrenergic POTS
Many POTS patients have excess sympathoneural tone. While supine plasma norepinephrine (NE) is often normal in POTS, a significantly increased upright plasma NE (>3.55 nmol/L and sometimes >5.91 nmol/L) can be seen in many POTS patients [4]. Patients have an exaggerated sympathetic pressor response during the recovery and overshoot phases of the Valsalva maneuver [5, 9]. These hyperadrenergic patients may increase their BP with standing and complain of tremor, anxiety, and cold, sweaty extremities [8]. Yet, the correlation between hyperadrenergic symptoms and a high plasma NE remains to be established [12].
Though elevated sympathetic tone is usually secondary to another pathophysiological mechanism in POTS, it may also be the primary problem. Shannon et al. [24] reported a family with a loss-of-function genetic mutation causing NE transporter (NET) deficiency and POTS in the proband. NET is a clearance transporter, which leads to increased synaptic NE when defective. While this mutation is not common, many drugs act through NET blockade and can worsen tachycardia in POTS [25].
Furlan et al. [26] evaluated the sympathetic tone in patients with POTS using microneurographic recording from the peroneal sympathetic nerve, plasma norepinephrine, and spectral analysis of BP and HR variabilities. Sympathetic drive to vessels and the heart was enhanced in the supine position. During upright tilt, however, the increase in sympathetic drive to vessels was blunted in patients, whereas sympathetic modulation of HR was maintained or enhanced. These results might indicate a central nervous system cause of a hyperadrenergic state in some patients with POTS [26].
5.2 Hypovolemic POTS
Blood volume is frequently low in patients with POTS [27–29]. Raj et al. reported significant deficits in total blood, plasma, and red cell volume in POTS when patients were controlled for sodium intake and withdrawn from medications prior to testing [27]. Chronic hypovolemia could contribute to a hyperadrenergic state. An expected compensatory response for hypovolemia is activation of the renin–angiotensin–aldosterone system to promote sodium and volume retention, but some POTS patients with hypovolemia have inappropriately low standing plasma renin activity and aldosterone compared with the controls [4, 30]. These can be accompanied by high circulating angiotensin II levels [31] without a parallel increase in its metabolite, angiotensin (1–7), suggesting that angiotensin-converting enzyme 2 abnormalities might contribute to the plasma volume deficit in POTS [9, 32].
5.3 Neuropathic POTS
Up to 50 % of POTS patients may have a preferential denervation of sympathetic nerves in the lower limbs [33], as first shown by diminished NE spillover [34]. The inability of the peripheral vasculature to maintain sufficient constriction during upright posture allows blood pooling in the splanchnic vasculature [35, 36] and lower extremities [8]. A partial dysautonomia in POTS has also been indicated by impaired sudomotor function [37], excessive venous pooling in standing patients [38], and reduced intraepidermal nerve fiber density [33].
5.4 Mast Cell Activation Disorder
Some POTS patients report severe flushing in association with their tachycardia and may have a mast cell activation disorder. These patients often have a hyperadrenergic appearance, with orthostatic tachycardia and hypertension, as well as dramatic BP overshoots in phase 4 of the Valsalva maneuver. It has not been determined whether the sympathetic activation induces mast cell degranulation or if mast cell activation causes the release of vasoactive mediators and sympathetic activation compensates for the ensuing vasodilation [39]. Measuring urinary methylhistamine levels around a spell can make the diagnosis.
5.5 Autoantibodies
A diagnosis of POTS following a virus-like syndrome in some patients has stimulated a quest for autoantibodies that affect autonomic functions in POTS. Rare cases are associated with a low titer of an antibody targeting the ganglionic acetylcholine receptor [12]. Recently, Li et al. found evidence of functional autoantibodies to α-adrenergic receptors (AR) and β-AR in POTS patients, with much lower activity in the control subjects [40]. This is an emerging area of POTS research.
6 Treatment of POTS
6.1 Nonpharmacological Treatment of POTS
The initial step in the care and treatment of patients with POTS is education about behaviors and medications that can precipitate symptoms. Patients must be examined for any existing illnesses, which could be causing their POTS. Medications that might contribute to POTS should be discontinued or reduced.
Patients should be advised to avoid extreme heat and activities that lead to dehydration. In an effort to increase intravascular volume, they should be encouraged to drink water 2–3 L/day, while increasing their sodium intake to >200 mEq/day. Intravenous saline (1–2 L) can quickly expand blood volume and curb tachycardia in POTS patients [41], but this treatment is associated with an increased risk of vascular access complications (including infections) when used chronically.
Venous pooling as a result of upright posture in POTS appears to occur primarily in the splanchnic region [36], and abdominal compression to inhibit pooling may improve stroke volume and cardiac output. Elastic waist-high support hose or body-shaper garments may be effective at increasing venous return.
Patients with POTS complain of significant exercise intolerance [9, 42]. Deconditioning contributes to the limited ability to exercise, which then exacerbates the deconditioning. A 3-month aerobic exercise program coupled with resistance training improves orthostatic tachycardia, symptoms, and quality of life [28, 43].
Raj et al. found that POTS patients were mildly depressed, which may reflect unhappiness about living with a chronic illness [44]. Behavioral approaches, such as yoga and biofeedback, to help patients cope with their disorder can be important components of the treatment of POTS [7].
6.2 Pharmacological Treatment of POTS
Randomized placebo-controlled trials are lacking for this patient population [9, 14, 42]. Given the heterogeneity of POTS, the success of a medication may be influenced by the POTS subtype, though Thieben et al. reported no difference in the symptomatic improvement of different subtypes of POTS to a variety of medications [12].
A hyperadrenergic phenotype with POTS might respond better to agents that decrease sympathetic tone. Low doses (10–20 mg) of the nonselective β-AR antagonist propranolol can acutely control HR and orthostatic symptoms without causing fatigue [45]. A 4-week trial of long-acting propranolol decreased standing HR without improving the quality of life [28]. Central sympatholytics (e.g., clonidine and methyldopa) can decrease the sympathetic nervous system tone, but need to be used carefully to avoid undesirable side effects such as drowsiness and worsening of the mental clouding [9]. Pyridostigmine can also restrain HR in POTS [46]. It inhibits acetylcholinesterase and raises parasympathetic tone by increasing the availability of acetylcholine at both the autonomic ganglia and the peripheral muscarinic receptors. It has led to long-term symptom improvement in approximately 50 % of patients with POTS, though increased gut motility may lead to discontinuation in 20 % of patients [47].
Ivabradine is a novel agent approved for the treatment of angina in many parts of the world, but not yet in the United States. It slows HR by inhibiting the pacemaker funny channel current in the sinoatrial node and does not affect BP. A retrospective case series found decreased tachycardia in 60 % of POTS patients [48]
Midodrine, an α1-AR agonist, can be used to increase peripheral resistance by stimulating vasoconstriction. It not only improves the symptoms and orthostatic tachycardia, but can also be associated with the unpleasant sensations of scalp-tingling and goose bumps [41].
Fludrocortisone, an aldosterone analog, increases sodium reabsorption in the distal tubules of the kidney, and should thereby increase sodium retention and volume expansion. Fludrocortisone also stimulates potassium excretion, making it necessary to monitor potassium levels, and it can also worsen migraine headaches [9, 21].
The vasopressin analog, desmopressin (DDAVP), can also increase volume and reduce tachycardia and symptoms [49]. It can lead to hyponatremia, as only free water is retained. Erythropoietin may also be used to increase blood volume, via increasing red cell mass, and may cause vasoconstriction as well [8], but its side effects, cost, and need for injection make it a less attractive option [7].
NET inhibitors, or serotonin-norepinephrine reuptake inhibitors (SNRIs), may worsen tachycardia in POTS [25]. In contrast, selective serotonin reuptake inhibitors (SSRIs) such as sertraline do not worsen tachycardia or orthostatic symptoms in POTS patients [50]. Studies on its benefit related to coping with the POTS syndrome have not been conducted.
7 Conclusion
POTS is a heterogeneous disorder, related to multiple, overlapping pathophysiological mechanisms. The hallmark clinical trait is an excessive increase in HR upon assumption of the upright posture, in the absence of orthostatic hypotension. Unlike VVS patients, POTS patients do not generally faint, though a number of cardiac and noncardiac symptoms may be triggered within a few minutes of standing and persist until recumbence in POTS. Presyncopal symptoms in VVS may resemble those in POTS, but their appearance is delayed in VVS (often for several minutes after standing), and they are associated with an abrupt fall in BP and HR. Exercise training is an important therapeutic strategy in POTS. Pharmacological treatments are second- line approaches that often target specific pathophysiological features.
References
Schondorf R, Low PA (1993) Idiopathic postural orthostatic tachycardia syndrome: an attenuated form of acute pandysautonomia? Neurology 43(1):132–137
Freeman R, Wieling W, Axelrod FB et al (2011) Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res 21(2):69–72
Robertson D (1999) The epidemic of orthostatic tachycardia and orthostatic intolerance. Am J Med Sci 317(2):75–77
Garland EM, Raj SR, Black BK et al (2007) The hemodynamic and neurohumoral phenotype of postural tachycardia syndrome. Neurology 69(8):790–798
Raj SR (2006) The Postural Tachycardia Syndrome (POTS): pathophysiology, diagnosis & management. Indian Pacing Electrophysiol J 6(2):84–99
Bagai K, Song Y, Ling JF et al (2011) Sleep disturbances and diminished quality of life in postural tachycardia syndrome. J Clin Sleep Med 7(2):204–210
Johnson JN, Mack KJ, Kuntz NL et al (2010) Postural orthostatic tachycardia syndrome: a clinical review. Pediatr Neurol 42(2):77–85
Grubb BP (2008) Postural tachycardia syndrome. Circulation 117(21):2814–2817
Raj SR (2013) Postural tachycardia syndrome (POTS). Circulation 127(23):2336–2342
Friesinger GC, Biern RO, Likar I et al (1972) Exercise electrocardiography and vasoregulatory abnormalities. Am J Cardiol 30(7):733–740
Nwazue VC, Paranjape SY, Black BK et al (2014) Postural tachycardia syndrome and inappropriate sinus tachycardia: role of autonomic modulation and sinus node automaticity. J Am Heart Assoc 3(2):e000700
Thieben MJ, Sandroni P, Sletten DM et al (2007) Postural orthostatic tachycardia syndrome: the Mayo clinic experience. Mayo Clin Proc 82(3):308–313
Okamoto LE, Raj SR, Peltier A et al (2012) Neurohumoral and haemodynamic profile in postural tachycardia and chronic fatigue syndromes. Clin Sci (Lond) 122(4):183–192
Pilcher TA, Saarel EV (2014) A teenage fainter (dizziness, syncope, postural orthostatic tachycardia syndrome). Pediatr Clin North Am 61(1):29–43
Brewster JA, Garland EM, Biaggioni I et al (2012) Diurnal variability in orthostatic tachycardia: implications for the postural tachycardia syndrome. Clin Sci (Lond) 122(1):25–31
Nwazue VC, Arnold AC, Raj V et al (2014) Understanding the placebo effect in clinical trials for postural tachycardia syndrome. Clin Exp Pharmacol Physiol 41:325–330
Gazit Y, Nahir AM, Grahame R et al (2003) Dysautonomia in the joint hypermobility syndrome. Am J Med 115(1):33–40
Wallman D, Weinberg J, Hohler AD (2014) Ehlers-Danlos syndrome and postural tachycardia syndrome: a relationship study. J Neurol Sci 340:99–102
Bagai K, Wakwe CI, Malow B et al (2013) Estimation of sleep disturbances using wrist actigraphy in patients with postural tachycardia syndrome. Auton Neurosci 177(2):260–265
Benrud-Larson LM, Dewar MS, Sandroni P et al (2002) Quality of life in patients with postural tachycardia syndrome. Mayo Clin Proc 77(6):531–537
Nwazue VC, Raj SR (2013) Confounders of vasovagal syncope: postural tachycardia syndrome. Cardiol Clin 31(1):101–109
Fu Q, Verheyden B, Wieling W et al (2012) Cardiac output and sympathetic vasoconstrictor responses during upright tilt to presyncope in healthy humans. J Physiol 590(Pt 8):1839–1848
Raj SR, Coffin ST (2013) Medical therapy and physical maneuvers in the treatment of the vasovagal syncope and orthostatic hypotension. Prog Cardiovasc Dis 55(4):425–433
Shannon JR, Flattem NL, Jordan J et al (2000) Orthostatic intolerance and tachycardia associated with norepinephrine-transporter deficiency. N Engl J Med 342(8):541–549
Green EA, Raj V, Shibao CA et al (2013) Effects of norepinephrine reuptake inhibition on postural tachycardia syndrome. J Am Heart Assoc 2(5):e000395
Furlan R, Jacob G, Snell M et al (1998) Chronic orthostatic intolerance: a disorder with discordant cardiac and vascular sympathetic control. Circulation 98(20):2154–2159
Raj SR, Biaggioni I, Yamhure PC et al (2005) Renin-aldosterone paradox and perturbed blood volume regulation underlying postural tachycardia syndrome. Circulation 111(13):1574–1582
Fu Q, Vangundy TB, Shibata S et al (2011) Exercise training versus propranolol in the treatment of the postural orthostatic tachycardia syndrome. Hypertension 58(2):167–175
Fouad FM, Tadena-Thome L, Bravo EL et al (1986) Idiopathic hypovolemia. Ann Intern Med 104(3):298–303
Raj SR, Robertson D (2007) Blood volume perturbations in the postural tachycardia syndrome. Am J Med Sci 334(1):57–60
Mustafa HI, Garland EM, Biaggioni I et al (2011) Abnormalities of angiotensin regulation in postural tachycardia syndrome. Heart Rhythm 8(3):422–428
Stewart JM, Glover JL, Medow MS (2006) Increased plasma angiotensin II in postural tachycardia syndrome (POTS) is related to reduced blood flow and blood volume. Clin Sci (Lond) 110(2):255–263
Gibbons CH, Bonyhay I, Benson A et al (2013) Structural and functional small fiber abnormalities in the neuropathic postural tachycardia syndrome. PLoS One 8(12):e84716
Jacob G, Costa F, Shannon JR et al (2000) The neuropathic postural tachycardia syndrome. N Engl J Med 343(14):1008–1014
Stewart JM, McLeod KJ, Sanyal S et al (2004) Relation of postural vasovagal syncope to splanchnic hypervolemia in adolescents. Circulation 110(17):2575–2581
Stewart JM, Medow MS, Glover JL et al (2006) Persistent splanchnic hyperemia during upright tilt in postural tachycardia syndrome. Am J Physiol Heart Circ Physiol 290(2):H665–H673
Peltier AC, Garland E, Raj SR et al (2010) Distal sudomotor findings in postural tachycardia syndrome. Clin Auton Res 20(2):93–99
Streeten DH, Anderson GH Jr, Richardson R et al (1988) Abnormal orthostatic changes in blood pressure and heart rate in subjects with intact sympathetic nervous function: evidence for excessive venous pooling. J Lab Clin Med 111(3):326–335
Shibao C, Arzubiaga C, Roberts LJ et al (2005) Hyperadrenergic postural tachycardia syndrome in mast cell activation disorders. Hypertension 45(3):385–390
Li H, Yu X, Liles C et al (2014) Autoimmune basis for postural tachycardia syndrome. J Am Heart Assoc 3(1):e000755
Jacob G, Shannon JR, Black B et al (1997) Effects of volume loading and pressor agents in idiopathic orthostatic tachycardia. Circulation 96(2):575–580
Medow MS, Stewart JM (2007) The postural tachycardia syndrome. Cardiol Rev 15(2):67–75
Shibata S, Fu Q, Bivens TB et al (2012) Short-term exercise training improves the cardiovascular response to exercise in the postural orthostatic tachycardia syndrome. J Physiol 590(Pt 15):3495–3505
Raj V, Haman KL, Raj SR et al (2009) Psychiatric profile and attention deficits in postural tachycardia syndrome. J Neurol Neurosurg Psychiatry 80(3):339–344
Raj SR, Black BK, Biaggioni I et al (2009) Propranolol decreases tachycardia and improves symptoms in the postural tachycardia syndrome: less is more. Circulation 120(9):725–734
Raj SR, Black BK, Biaggioni I et al (2005) Acetylcholinesterase inhibition improves tachycardia in postural tachycardia syndrome. Circulation 111(21):2734–2740
Kanjwal K, Karabin B, Sheikh M et al (2011) Pyridostigmine in the treatment of postural orthostatic tachycardia: a single-center experience. Pacing Clin Electrophysiol 34(6):750–755
McDonald C, Frith J, Newton JL (2011) Single centre experience of ivabradine in postural orthostatic tachycardia syndrome. Europace 13(3):427–430
Coffin ST, Black BK, Biaggioni I et al (2012) Desmopressin acutely decreases tachycardia and improves symptoms in the postural tachycardia syndrome. Heart Rhythm 9(9):1484–1490
Mar PL, Raj V, Black BK et al (2014) Acute hemodynamic effects of a selective serotonin reuptake inhibitor in postural tachycardia syndrome: a randomized, crossover trial. J Psychopharmacol 28(2):155–161
Conflicts of Interest
None
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Garland, E.M., Raj, S.R. (2015). Differential Diagnosis of Vasovagal Syncope: Postural Orthostatic Tachycardia. In: Alboni, P., Furlan, R. (eds) Vasovagal Syncope. Springer, Cham. https://doi.org/10.1007/978-3-319-09102-0_14
Download citation
DOI: https://doi.org/10.1007/978-3-319-09102-0_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-09101-3
Online ISBN: 978-3-319-09102-0
eBook Packages: MedicineMedicine (R0)