
Abstract
At the time of the Workshop in 2017, the scientific evidence was certain: ambient air pollution, that is, contamination of outdoor air consequent to man’s activities, is a major cause of morbidity (ill health) and premature mortality (early death). While the rise of ambient air pollution is relatively recent, air pollution has probably had adverse effects on human health throughout history. In fact, the respiratory tract, which includes the nose, throat and lungs, has a remarkable system of defense mechanisms to protect against inhaled particles and gases. The use of fire for heating and cooking came with exposure to smoke, an exposure that persists today for the billions who use biomass fuels for cooking and heating. The rise of cities concentrated the emissions of pollutants from dwellings and industry and led to air pollution that was likely affecting health centuries ago. Continued industrialization and also electric power generation brought new point sources of pollution into areas adjacent to where people lived and worked. During the twentieth century, cars, trucks, and other fossil fuel–powered vehicles became a ubiquitous pollution source in higher-income countries and created a new type of pollution—photochemical pollution, or “smog”—first recognized in the Los Angeles air basin in the 1940s. The unprecedented growth of some urban areas to form “megacities,” such as Mexico City, São Paulo, London, and Shanghai, has led to unrelenting air pollution from massive vehicle fleets and snarled traffic and from polluting industries and coal-burning power plants. With population growth and urbanization, ever more megacities are anticipatesd; the current total of cities with a population over 10 million has now reached 31.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
Summary In 2017, the scientific evidence was certain: ambient air pollution (i.e., contamination of outdoor air consequent to man’s activities) is a major cause of morbidity (ill health) and premature mortality (early death). While the rise of ambient air pollution is relatively recent, air pollution has probably had adverse effects on human health throughout history. In fact, the respiratory tract, which includes the nose, throat and lungs, has a remarkable system of defense mechanisms to protect against inhaled particles and gases. The use of fire for heating and cooking came with exposure to smoke, an exposure that persists today for the billions who use biomass fuels for cooking and heating. The rise of cities concentrated the emissions of pollutants from dwellings and industry and led to air pollution, which was likely affecting health centuries ago. Continued industrialization and also electric power generation brought new point sources of pollution into areas adjacent to where people lived and worked. During the twentieth century, cars, trucks, and other fossil fuel–powered vehicles became a ubiquitous pollution source in higher-income countries and created a new type of pollution—photochemical pollution, or “smog”—which was first recognized in the Los Angeles air basin in the 1940s. The unprecedented growth of some urban areas to form “megacities,” such as Mexico City, São Paulo, London, and Shanghai, has led to unrelenting air pollution from massive vehicle fleets and snarled traffic and from polluting industries and coal-burning power plants. With population growth and urbanization, ever more megacities are anticipated; the current total of cities with a population over 10 million has now reached 31.
This chapter provides an overview of the current state of knowledge concerning the adverse health effects of ambient air pollution and the associated burden of premature death. It draws on various authoritative reviews, particularly those carried out by the US Environmental Protection Agency in support of revisions to the National Ambient Air Quality Standards (NAAQS), which apply to the major outdoor pollutants. Emphasis is given to airborne particulate matter, a ubiquitous type of ambient pollution that derives from multiple sources; the most widely used indicators are PM10 and PM2.5 (particulate matter less than 10 and 2.5 μm in aerodynamic diameter, respectively) and to ozone. The chapter also addresses the burden of disease attributable to air pollution, documenting the target for air quality improvement and the global gains in public health that can be made.
While the emphasis here is on ambient air pollution that has adverse effects at local and regional levels, climate change also comes from air pollution with greenhouse gases. The connections are direct; the same combustion processes that release particles and toxic gases also generate carbon dioxide.
The Health Effects of Air Pollution
Overview
Ambient air pollution comprises a complex and dynamic mixture of gaseous and particulate air pollutants. The array of health effects linked to ambient air pollution is broad and includes increased risk for respiratory infections, exacerbation of asthma, and chronic obstructive pulmonary disease (COPD —a disease involving destruction of the lung structure) and cardiac (heart) events, contributions to development of major chronic diseases (coronary heart disease, COPD, and cancer), and impaired lung growth and respiratory symptoms during childhood. Additional adverse health outcomes are under investigation: autism and other neurodevelopmental disorders, adverse reproductive outcomes, and more rapid “brain aging,” for example. There are several general mechanisms underlying these health effects, particularly oxidant stress, an excess of reactive molecules, and a heightened inflammatory state, given the oxidative nature of ambient air pollution. The increased risk for cancer causally linked to air pollution likely comes primarily from the presence of specific carcinogens (i.e., cancer-causing agents) in ambient air pollution (e.g., polycyclic aromatic hydrocarbons, and inflammation); particles collected in outdoor air are mutagenic, which means that they can damage DNA (IARC, 2015). Table 6.1 provides a listing of major pollutants and associated health effects, as well as some of the current standards and guidelines for controlling their concentrations.
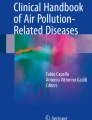
While the problem of air pollution was noted centuries ago, the contemporary era of research on air pollution and health and evidence-driven air quality regulation and management began in the mid-twentieth century following a series of episodes of very high pollution with disastrous health consequences (Brimblecombe, 1987). The most dramatic was the London Fog of 1952, which caused thousands of excess deaths and prompted some of the first epidemiological studies of the health effects of air pollution (Fig. 6.1) (Bell & Davis, 2001). In the United States, recognition of the public health dimensions of air pollution also began in the mid-twentieth century, driven by the rising problem of smog in southern California, episodes of visibly high pollution in major cities, and the 1948 air pollution episode in Donora, Pennsylvania, which caused 20 excess deaths and thousands of illnesses in one small town.

Approximate weekly mortality and SO2 concentrations for Greater London, 1952–1953
Multiple investigational approaches have been used to characterize the health effects of ambient air pollution. Initially, the dramatic pollution episodes made clear that high levels of air pollution caused excess mortality, particularly in elderly people with chronic diseases and in infants and young children. As air pollution levels declined with regulation, increasing emphasis was placed on understanding the quantitative risks of air pollution so that air quality standards could be set that would be protective of public health. In other words, researchers did studies to understand by how much risk changes as air pollution increases or decreases. Epidemiological studies (i.e., research based in populations) were critical for that purpose. Cohort or longitudinal studies were most informative. Such studies involved following participants over time, estimating pollution exposures, and tracking health events; analyses focused on quantifying the risks associated with air pollution exposure during follow-up. For example, the Children’s Health Study in Southern California tracked lung growth and respiratory health in school children from communities having a range of pollution concentrations (Gauderman et al., 2015). Now in progress for two decades, the study has shown that higher levels of air pollution slow lung growth and that reduction of pollution enhances it.
These epidemiological approaches are complemented by toxicological studies that provide insights into the mechanisms by which air pollution causes adverse health effects. Such evidence is critical in reaching causal conclusions on the adverse health effects of air pollution. In the past, toxicological studies often involved exposure of animals to a single pollutant, such as ozone, to isolate the pollutant’s effect from those of other pollutants present in the air pollution mixture. For studying some pollutants, human volunteers have inhaled the pollutants in an exposure chamber over a short interval and their responses closely monitored. Additionally, pollutants are also studied in cell systems; these systems are likely to gain increasing prominence as new, sophisticated systems probe gene expression of different kinds of cells following exposure.
There are a number of national groups that periodically assess the evidence on adverse effects of air pollution and provide guidance to the setting of standards and guidelines. In the United States, the Environmental Protection Agency carries out reviews of the evidence as the basis for renewal of major air quality standards (the National Ambient Air Quality Standards or NAAQS) on a 5-year cycle. Reviews are conducted by the United Kingdom, the European Commission and other nations. The World Health Organization releases air quality guidelines, which are currently being updated. In reviewing the evidence, a judgment that the findings are strong enough to infer a causal relationship has great weight for regulation. The health risks associated with major air pollutants are reviewed below.
While air pollution research and regulation generally focuses on specific pollutants, air pollution outdoors is a complex mixture. Effects attributed to a single pollutant, particularly when studied in the “real world” context, may reflect the toxicity of the mixture as indexed by a particular pollutant. Ambient particulate matter (PM), for example, comes from myriad sources and is emitted as a primary pollutant from combustion and other sources; it is also formed through chemical transformations of gaseous pollutants, such as the formation of particulate nitrates from gaseous nitrogen oxides. The mixture of pollutants formed from vehicle emissions, generally referred to as traffic-related air pollution, may have specific toxicity beyond that of well-studied individual components.
Particulate Matter
The literature on the health effects of particles is enormous, comprising many epidemiological and toxicological studies (U.S. Environmental Protection Agency, 2009). With regard to ambient air pollution, the risks of particulate matter have assumed great prominence because particles are widely monitored and used as the principal indicator for estimating the burden of morbidity and premature mortality attributable to air pollution. Particles are a robust indicator of ambient air pollution because of their myriad sources and the contributions of sulfur and nitrogen oxides and organic compounds to secondary particle formation. Particles in outdoor air have numerous natural and man-made sources. The man-made sources are diverse and include power plants, industry, and motor vehicles, including diesel-powered vehicles that emit particles in the size range that penetrates into the lung. In areas where biomass fuels are used, the contributions of indoor combustion to outdoor air pollution may be substantial.
Particles in outdoor air span a wide range of sizes (Fig. 6.2) and are highly diverse in composition and physical characteristics, including size as indicated by aerodynamic diameter. Thus, PM2.5 includes those particles less than 2.5 μm in aerodynamic diameter, a size band that contains most man-made particles in outdoor air and also the particles of a size that can reach the smaller airways and air sacs of the lungs. The very small ultrafine particles, which include freshly generated combustion particles, are another set of particles of concern. Much research has been done on characteristics of particles that determine toxicity. Hypotheses on determinants of particle toxicity have focused on acidity, transition metals such as iron that can cause damaging injury, organic compounds, bioaerosols, and size; as a further complication, different characteristics could be relevant to different health outcomes. However, in spite of extensive toxicological and epidemiological research, the evidence is not yet sufficiently definitive to link particular characteristics to toxicity. Making such linkages would be helpful for targeting control approaches.

Changes in economic indicators, pollutant emissions, and concentrations of criteria pollutants over time. Note: Shown are changes in criteria pollutant concentrations during 1990-2015 (Panel A) and changes in economic growth indicators and emissions during 1970-2015 (Panel B). (Source: Drawn from EPA data at https://gispub.epa.gov/air/trendsreport/2016/)
There has been extensive epidemiological and toxicological investigation of the effects of particles on health since the air pollution disasters of mid-century. The toxicological studies have used approaches including exposing volunteers to generated particles or concentrated air particles, animal exposures, and diverse in vitro assays. This extensive body of evidence shows that particles are injurious and indicates mechanisms by which particles could cause adverse effects on the respiratory and cardiovascular systems. The epidemiological studies have grown in size and in the sophistication of their methodology. Recent studies involve large, national-level populations, such as all people in the United States who are 65 years and older, and estimation of exposures at all household addresses using models that incorporate available monitoring data, satellite information, and land-use data, such as on roadways and manufacturing. Table 6.2 lists the findings of the most recent comprehensive review of the evidence on airborne particles (the Integrated Science Assessment) by the US Environmental Protection Agency. Both short-term and long-term adverse effects were found to be caused by particulate matter. The most recent epidemiological studies continue to find associations of PM2.5 with increased risk for mortality, even at contemporary concentrations in the United States. In a recent study utilizing the Medicare data for persons 65 years of age and older, over 60 million people, Di et al. showed increased mortality at annual averages below 12 μg/m, the current annual standard in the United States3 (Di et al., 2017).
One analysis has suggested that reductions in particulate air pollution during the 1980s and 1990s have led to measurable improvements in life expectancy in the United States. The researchers estimated that for each 10 μg/m3 reduction in air pollution over this period, the average gain in life expectancy was 0.61 years (about 7.3 months). The authors concluded that as much as 15% of the total life expectancy increase seen during this time in the United States was attributable to the air pollution reductions.
This strong evidence on the adverse health effects of particulate matter has led to ever tighter ambient air quality standards (Table 6.1). Nonetheless, adverse health effects are still observed and much of the world’s population is exposed to high concentrations at which adverse effects are certain.
Ozone
Ozone is a specific gas that has been studied for its toxicity using toxicological approaches. It is also used as an indicator of photochemical pollution, or “smog,” which is the complex oxidant mixture produced by the action of sunlight on hydrocarbons and nitrogen oxides. Smog has become a worldwide problem as vehicle fleets have grown. The problem of tropospheric (ground-level) ozone pollution is distinct from the problem of depletion of the strato-pheric (high-level) ozone layer.
Ozone, a highly reactive molecule, has been extensively investigated using toxicological approaches that have included exposures of human volunteers and short- and long-term exposures of animals (U.S. EPA, 2013). The human studies have involved exposures of volunteers, generally young and healthy, to concentrations of ozone found in urban areas in the United States and elsewhere. Collectively, the studies show that exposures of up to 6–8 h with intermittent exercise result in temporary drops in lung function and that some individuals have greater susceptibility to ozone. While the effects are transient, they are of sufficient magnitude in some people (loss of around 10% of function) to be considered adverse. In some of the studies, the lungs have been sampled and evidence of inflammation was found by measuring concentrations of molecules that reflect the tissue’s response. In experimental animals, sustained low-level exposure damages the small airways and leads to early changes of COPD; thus, there is concern about permanent structural alteration in ozone-exposed populations. In human studies, asthmatics have not been shown to have increased susceptibility to ozone compared with non-asthmatics.
Epidemiological studies provide coherent evidence on the short-term effects of ozone on respiratory health. There is also evidence from daily time-series studies (studies examining day-to-day variations in death counts in relationship to variations in pollution levels) that ozone increases the risk for mortality. There is inconsistent evidence for cardiovascular effects and a just-completed exposure study of older persons with cardiovascular disease did not find adverse effects.
Reflecting the evidence on short-term effects on lung function, standards for ozone concentrations are directed at brief time spans (Table 6.1). Given the range of susceptibility of the population, it is likely that feasibly achieved standards will not protect the full population from adverse respiratory effects.
Nitrogen Oxides
Gaseous nitrogen oxides are produced by combustion processes and also contribute to the formation of aerosols. Nitrogen dioxide (NO2) , an oxidant gas, is the indicator that is generally monitored. The principal source of NO2 in outdoor air is motor vehicle emissions, and NO2 is considered to be a useful indicator of traffic-related air pollution in urban environments. Power plants and industrial sources may also contribute. The health effects of NO2 emitted into outdoor air probably come mainly from the formation of secondary pollutants, including ozone and particles. NO2, along with hydrocarbons, is an essential precursor of ozone and the nitrogen oxides also form acidic nitrate particles.
Nitrogen dioxide itself has been studied in animal models and in clinical studies. It can reach the small airways and air sacs of the lung because of its low solubility. The toxicological evidence at high exposures has raised concern that NO2 exposure can impair lung defenses against infectious agents such as viruses and cause airway inflammation, thereby increasing the risk for respiratory infections. Supporting epidemiological research is lacking and population studies directed at NOs are complicated by its role in the formation of ozone and its presence in the complex mixture of traffic-related pollutants. Human exposure studies have been performed to investigate the immediate effects of NO2 on persons with asthma. Nitrogen dioxide could plausibly increase airway responsiveness (the extent to which the airways constrict when irritated) by causing airway inflammation. The findings of the exposure studies have been inconsistent, but suggest that some people with asthma may be susceptible.
Carbon Monoxide
Carbon monoxide (CO) is an invisible gas formed by incomplete combustion. It is a prominent indoor pollutant with sources including biomass fuel combustion and space heating with fossil fuels. At high levels indoors, fatal CO poisoning may result. Outdoors, vehicle exhaust is the major source and concentrations are highly variable, reflecting vehicle density and traffic patterns. Urban locations with high traffic density (“hot spots”) tend to have the highest concentrations. The toxicity of CO comes from its tight binding to hemoglobin, which carries oxygen in the blood, and the resulting reduction of oxygen delivery to tissues. Exposures to CO can be assessed by using the level of carboxyhemoglobin as a marker of exposure or by measuring the concentration of CO in the breath.
Because of the reduction of oxygen delivery, persons with cardiovascular disease are considered to be at greatest risk from CO exposure; research has focused on CO and adverse effects in this susceptible group. The research has used an approach referred to as a “clinical study”; volunteers with cardiovascular disease are exposed to levels of CO of interest and clinical measurements made, such as by taking an electrocardiogram. The evidence from such studies indicates that CO exposure leads to earlier evidence of myocardial ischemia (inadequate oxygenation of the heart) following exposure compared with unexposed controls. There are other potential susceptible groups: fetuses and persons with COPD may also be harmed by CO, and normal persons may have reduced oxygen uptake during exercise at low levels of CO exposure.
The exposure studies have provided robust evidence for standards for CO, which are based on brief time windows, reflective of the handling of CO in the body. In higher-income countries, outdoor levels of CO have fallen greatly over recent decades as controls have greatly reduced emissions (see Fig. 6.3). Nonetheless, CO may be a concern in some high-traffic locations. Less is known about CO exposure in middle- and low-income countries, where ambient CO may be added to indoor exposure from biomass fuel combustion.

Ambient particulate matter size distribution. (Source: Adapted from the EPA)
Sulfur Oxides
Sulfur oxides are generated by combustion of fuels containing sulfur, such as coal, crude petroleum, and diesel, and by smelting operations. The water-soluble gas, sulfur dioxide or SO2, is the indicator that is generally monitored. However, other sulfur oxides are emitted and the sulfur oxides undergo transformation to form particulate sulphate compounds. Scientific research has been directed primarily at SO2, although epidemiological studies provide information on sulfur oxide exposure more generally. Sulfur dioxide is a reactive gas that is effectively scrubbed or cleaned from inhaled air in the upper airway. With exercise and a switch to oral breathing as ventilation increases, the inhaled dose of SO2 increases and more reaches the lung.
Much of the evidence that has driven regulation comes from clinical studies that involve exposure of people with asthma and that show adverse effects without exposures to other pollutants. Asthmatics are particularly sensitive, with some asthmatics having more severe health responses at a particular concentration than others with asthma. With exercise and hyperventilation, some people with asthma respond with increased resistance of the lung to airflow with an associated drop in lung function and with respiratory symptoms. Such effects have been demonstrated at concentrations that might be reached in the United States in high-exposure situations and that may be common in some heavily industrialized countries. Epidemiological studies from Hong Kong examined the consequences of a major and rapid reduction in sulfur content in fuels. The investigators found an associated substantial reduction in health effects (childhood respiratory disease and all age mortality outcomes).
Lead
Although lead in gasoline is now phased out in almost all nations, exposure continues from industrial activities, such as smelting, and sometimes results in dangerous exposures for children. Exposure to lead may occur through inhalation and also ingestion in food and water, routes of exposure that have become the most important in high-income countries. A substantial body of epidemiological evidence links lead exposure of children to adverse neurodevelopmental effects, such as lowering the level of intelligence; as a result of that evidence, recommendations as to the acceptable level of lead for children have been lowered progressively. Lead has also been linked to higher blood pressure and cardiovascular disease and to low bone mineral density and osteoporosis.
The Disease Burden from Ambient Air Pollution
Given these adverse health effects and ubiquitous pollution of outdoor air, estimates of the burden of disease caused by air pollution are needed as a basis for priority setting and air quality management. Such estimates of disease burden can also prove useful for motivating action, as they have done recently in China. The conceptual basis for estimating disease burden draws on the conceptual framework of attributable risk, originally proposed in the early 1950s for smoking and lung cancer by Levin (Levin, 1953). He proposed a statistic, the population attributable risk (PAR), which incorporates the prevalence of the exposure of concern (P) and the relative risk (RR) for disease associated with that exposure, as follows: PAR = (Px[RR − 1])/(1 + Px[RR − 1]). Thus, the PAR rises as either P or RR increases; in other words, the burden rises as more people are exposed or the risk is increased. For lung cancer, for example, in a population with 40% smokers and a lung cancer RR of 20, the PAR is 0.88, interpreted as 88% of the cases resulting from smoking. The PAR is interpreted based on comparison to a comparison group involving no or lower exposure; for smoking, for example, the comparison is a hypothetical world in which smoking never existed.
For air pollution, estimates of the burden of attributable disease have been made by the World Health Organization and the Institute for Health Metrics and Evaluation (IHME) in the United States, which carries out the Global Burden of Diseases, Injuries, and Risk Factors Study (Cohen et al., 2017). A detailed analysis of the global burden of disease attributable to ambient air pollution was recently reported for the 25 years from 1990 to 2015. With regard to the exposure prevalence (P), PM2.5 and ozone concentrations are estimated for smaller level spatial grids that capture variation in urban areas and then aggregated to provide national mean exposures. The IHME estimates for PM2.5 include ischemic heart disease (IHD), cerebrovascular disease, lung cancer, chronic obstructive pulmonary disease (COPD), and lower respiratory infections (LRI), while only COPD is considered for ozone. The RRs for these diseases come from complex analyses of epidemiological data. The counterfactual values for burden estimation are derived from the lowest values considered in the epidemiological studies.
The latest estimates confirm that outdoor air pollution is a leading cause of premature mortality around the world, ranking at the fourth position in 1990 and the fifth in 2015. The total of deaths attributed to PM2.5 globally in 2015 is 4.2 million distributed by cause as follows: IHD—1.52 million, cerebrovascular disease—898,000, lung cancer—283,000, COPD—864,000, and LRI—675,000. There is substantial geographic variation globally (Fig. 6.4) with China and India together accounting for more than half of the attributable burden of premature mortality. From 1990 to 2015, estimates have increased in some countries (e.g., India and China), as the population has grown and aged, and air pollution levels have risen. For ozone, the global mortality estimate is much smaller at 254,000.

Global and regional distributions of population as a function of annual average ambient PM2.5 concentration for the 10 most populous countries in 2013. Note: Plotted data reflect local smoothing of bin-width normalized distributions computed over 400 logarithmically spaced bins; equally sized plotted areas would reflect equal populations. Dashed vertical lines indicate World Health Organization Interim Targets (IT) and the Air Quality Guideline (AQG). (Source: Brauer, M., et al. (2016). Ambient air pollution exposure estimation for the global burden of disease 2013. Environmental Science & Technology, 50(1), 79–88. Figure 3)
From a policy perspective, these estimates offer a strong rationale for air quality control and are cautionary in their implications. The estimates of exposure globally describe a stratified target (Fig. 6.4): the high-income countries that have lowered air pollution concentrations over the last half century and the numerous low- and middle-income countries where air pollution has worsened with industrialization and vehicle numbers have increased rapidly. Additionally, many of these countries still face the added challenge of household air pollution, also a leading cause of premature mortality.
Research Needs
There is a robust body of evidence on the health effects of ambient air pollution, which has both acute and chronic consequences. Given the underlying mechanisms of injury and commonalities among pollution sources, the collective evidence should have general applicability to people around the world. Nonetheless, many nations still lack basic monitoring and air quality management, even as pollution levels have risen in recent decades. In motivating action, locally generated data are likely to be more powerful than the external evidence, particularly if from high-income countries. At the least, monitoring data are needed for PM2.5 and other pollutants if relevant to a particular place. Local research could use cross-sectional epidemiological designs, for example, of the respiratory health of school children, and time-series studies of morbidity (e.g., hospitalization counts) and mortality. The Health Effects Institute in the United States has supported time-series studies of air pollution in multiple Asian countries through its Public Health and Air Pollution in Asia (PAPA) Project (Public Health and Air pollution in Asia (PAPA), 2010). The Global Burden of Disease estimates provide a valuable starting point for priority setting around ambient air pollution as a public health issue. The Health Effects Institute has made this information available in a useful form through its State of Global Air/2019 (https://www.stateofglobalair.org/).
Summary and Conclusions
Ambient air pollution is a well-documented threat to global health. Through man’s expanding use of fossil fuels for manufacturing, vehicles, and power generation, the numbers of people exposed to risky levels of air pollution has increased progressively; some are exposed at levels historically associated with evident excess mortality. Ambient air pollution now affects large swathes of the world, as contaminated air crosses national boundaries and moves globally. Of course, greenhouse gases represent another form of global pollution. The evidence is sufficiently certain and the burden of disease sufficiently large to motivate action at national and global levels. Evidence-driven regulations have had substantial impact on air quality in the United States and elsewhere, driving down levels of the most prominent pollutants (Fig. 6.3). Unfortunately, in many low- and middle-income countries, outdoor air pollution is a rising problem consequent to population growth, industrialization, and increasing numbers of vehicles—and, in too many countries, insufficient attention to air quality management and regulation. Control of greenhouse gases has the co-benefit of reducing ambient air pollution.
References
Bell, M. L., & Davis, D. L. (2001). Reassessment of the lethal London Fog of 1952: Novel indicators of acute and chronic consequences of acute exposure to air pollution. Environmental Health Perspectives, 109, 389–394.
Brimblecombe, P. (1987). The big smoke: A history of air pollution in London since medieval times (1st ed.). London: Routledge Kegan & Paul.
Cohen, A. J., Brauer, M., Burnett, R., Anderson, H. R., Frostad, J., Estep, K., et al. (2017). Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet, 389, 1907–1918. https://doi.org/10.1016/s0140-6736(17)30505-6
Di, Q., Wang, Y., Zanobetti, A., Wang, Y., Koutrakis, P., Choirat, C., et al. (2017). Air pollution and mortality in the medicare population. New England Journal of Medicine, 376, 2513–2522. https://doi.org/10.1056/NEJMoa1702747
Gauderman, W. J., Urman, R., Avol, E., Berhane, K., McConnell, R., Rappaport, E., et al. (2015). Association of improved air quality with lung development in children. New England Journal of Medicine, 372(10), 905–913. https://doi.org/10.1056/NEJMoa1414123
IARC (2015). Outdoor air pollution (Vol. 109). Lyon, France: International Agency for Research on Cancer.
Levin, M. L. (1953). The occurrence of lung cancer in man. Acta Unio Internationalis Contra Cancrum, 9, 531–541.
Public Health and Air pollution in Asia (PAPA). (2010). Coordinated studies of short-term exposure to air pollution and daily mortality in four cities (Research Report 154), Boston, MA. Retrieved on February 16, 2020 from https://www.healtheffects.org/publication/public-health-and-air-pollution-asia-papa-coordinated-studies-short-term-exposure-air-0
U.S. Environmental Protection Agency (2009). Final report: Integrated science assessment for particulate matter (EPA/600/R-08/139F). Washington, DC: U.S. Environmental Protection Agency. Retrieved on February 16, 2020 from https://cfpub.epa.gov/si/si_public_record_Report.cfm?dirEntryId=216546
U.S. Environmental Protection Agency (2013). Integrated science assessment for ozone and related photochemical oxidants (EPA/600/R-10/076F). Research Triangle Park, NC: U.S. Environmental Protection Agency. Retrieved on February 16, 2020 from https://cfpub.epa.gov/ncea/isa/recordisplay.cfm?deid=247492
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2020 The Author(s)
About this chapter

Cite this chapter
Samet, J.M. (2020). Air Pollution: Adverse Effects and Disease Burden. In: Al-Delaimy, W., Ramanathan, V., Sánchez Sorondo, M. (eds) Health of People, Health of Planet and Our Responsibility. Springer, Cham. https://doi.org/10.1007/978-3-030-31125-4_6
Download citation
DOI: https://doi.org/10.1007/978-3-030-31125-4_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-31124-7
Online ISBN: 978-3-030-31125-4
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)