
Abstract
Currently, healthcare is a crucial issue for the entire population, especially for individuals who suffer from a chronic disease such as hypertension or diabetes. However, this care is carried out in medical centers, limiting the scope of health professionals. In fact, some monitoring, early warning processes, and health supporting that are not presently performed, could be carried out at the patient’s location. The aim of this paper is to integrate WSN, ambient intelligence, multi-agent systems, and ontologies, in order to develop an ambient intelligence model that provides alerts, personalized recommendations, and adaptive health-care agendas. Personalized agendas based on chronic patient profiles offer appropriate physical activity, personalized food diet, and specific activities in order to control stress levels. For the validation of the proposed model, a prototype was constructed and applied to a case study considering several chronic patients. The results demonstrate the effectiveness of the proposed health-care ambient intelligence multi-agent model.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others



Keywords
1 Introduction
In recent years, there has been a lot of research and development using information technology (IT) in the field of medicine and health. Applying such technologies leads to the improvement of quality, safety and efficiency in medical care [1]. Technologies such as Mobile Health (m-Health) allow the interaction between health professionals and their patients, where mobile devices are used ubiquitously. This allows for noticeably improved medical care and diagnostic decision-making in health centers and at home [2, 3].
In addition, there are wireless sensor networks (WSN) in order to monitor all types of variables. In particular, in human health monitoring there are functional devices that alert when levels are out of the acceptable limits [4, 5]. However, if we strive for an autonomous and immediate reaction system to safeguard the life and well-being of patients, monitoring and alerting alone is not enough.
Therefore, it is necessary to develop a system that complements the existing systems by implementing technologies such as ambient intelligence, multi-agent systems, ontologies, and recommendation systems. It is required to develop a context-aware adaptive ambient intelligence system that by itself can adapt its behavior to the context that is monitoring. In addition, it is required that the patient can visualize the sampled data through a human-computer interface, and that the system is able to suggest, recommend, and provide feedback to the user about the actions to adopt in order to obtain the desired result.
The aim of this paper is to propose an ambient intelligence model that integrates technologies such as WSN, multi-agent systems, ambient intelligence, ontologies, in order to provide adaptive health-care functions to chronic patients. We develop a prototype that consists of several modules that allow the deployment of adaptive functions on a human-computer interface. The system allows monitoring, alerting and offering recommendations, and healthy agendas to patients who do not have health professionals during their daily life. In addition, the system makes it possible for a health professional to visualize all the patient information.
The rest of the paper is organized as follows: Sect. 2 presents the conceptual framework of this research. Section 3 reviews some related works concerning AmI systems for healthcare. Section 4 describes the proposed model. Section 5 offers the model implementation and validation of the proposed model. Finally, the main conclusions and future research directions are presented in Sect. 6.
2 Conceptual Framework
This section provides main definitions used in this research work such as ambient intelligence, wireless sensor networks, ontologies, multi-agent systems, healthcare, among others.
2.1 Ambient Intelligence
Ambient Intelligence (AmI)) [6] is a concept raised by the ISTAG (Information Society Technologies Advisory Group) through a report [7] that was presented to the General Directory of INFSO (Information Society) of the European Commission. In this report, AmI consists of the creation of habitable spaces where the users interact in a natural and intuitive way through computational services in order to assist the accomplishment of their daily tasks. Among the main features of an AmI system are the following:
-
The AmI environment must be context-aware, that is, it must be able to adapt its behavior based on the previously monitored variables.
-
Information, communication, and services are offered to users in a ubiquitous, wireless, and transparent manner.
-
Human-machine interaction is accomplished naturally and not intrusively.
According to Marzano [8], the five main characteristics of the AmI are the following:
-
Embedded: many networked devices integrate and operate into the environment.
-
Context-aware: these devices can recognize people and their contextual situation at any specific time.
-
Personalized: AmI devices can adapt their behavior to the people’s needs.
-
Adaptive: AmI devices can autonomously change in response to people and their environment.
-
Anticipatory: AmI devices can anticipate user needs and desires without a conscious mediation.
Consequently, an environment will be intelligent when it is unnoticeable, unobtrusive, and the different technologies that surround it complement each other to provide useful services to people. Thus, AmI environments could be implemented within different scenarios where the user lives, for example, domestic, mobile, public, and private environments [9].
2.2 Wireless Sensor Networks
Wireless sensor networks (WSN) are networks made up of several autonomous de-vices that have sensors, through which a monitoring and data acquisition system of the environment can be created. The WSN is a subfield of embedded systems that attempts to improve well-being and quality of life through home automation and health AmI environments. In addition, many companies and public organizations currently build WSN-based large-scale applications such as monitoring systems to provide early alerts to natural disasters, monitoring in the agricultural sector, industrial control, and transport. In a WSN, each device is autonomous and has the capacity of processing, storage, and sampling through its sensors [9].
2.3 Ontologies
Ontologies can be defined as a formal representation of a particular domain using a well-defined methodology that allows for the representation of the domain entities and the relationships existing among them [10]. Based on this, it is important to generate a formal representation of the adaptive learning course structure, in order to make inferences and generate recommendations for improving the learning process. Similarly, designing formal representations of a specific domain allows for readable and reusable information for computers and intelligent systems [11].
2.4 Multi-agent Systems
Multi-agent systems (SMA) issued from distributed artificial intelligence, are complex systems that are made up of autonomous agents. Each has the knowledge of a specific domain and the ability to interact with other agents to achieve a common goal [12]. In addition, agents are entities that have enough autonomy and intelligence to accomplish specific tasks with little or no supervision [13].
2.5 Healthcare
Chronic cardiovascular diseases (CVD) are a group of heart disorders and are the main cause of death in the world. Arterial hypertension (the most important preventable cause of CVD) is a disorder in which the force exerted by the blood on the walls of the arteries is higher than normal. The higher the tension, the more effort the heart has to exert to pump blood, increasing the risk of damage to the heart and blood vessels of major organs [14].
Diabetes is a chronic disease that occurs when an organism does not efficiently use the insulin it produces, or does not produce enough insulin. Insulin is the hormone responsible for regulating blood sugar. Hyperglycemia (blood sugar level higher than normal) degrades many organs and systems overtime, especially blood vessels and nerves [15].
Finally, for both diseases, monitoring, alerts, recommendations, and a healthy agenda, allows patients (if they are rigorous) to maintain stable blood pressure and/or suitable blood sugar levels, thus minimizing the chances of premature death and increasing healthy life habits.
3 Related Works
This section examines some related research that focuses on fields including ambient intelligence, ontologies, multi-agent systems and WSN. We will consider the advantages and disadvantages of various models and prototypes.
Corchado et al. [16] propose an autonomous intelligent agent developed for the control of healthcare of patients with Alzheimer in geriatric residences. The agent operates in wireless devices and integrates with complementary agents within an ambient intelligence multi-agent system, called ALZ-MAS (ALZheimer Multi-Agent-System) that interacts with the environment. An agent called AGALZ (Autonomous aGent for monitoring ALZheimer patients) was developed, with the objective of providing efficient work schedules, in real time, to the geriatric staff of the residences and therefore improving the quality of healthcare and supervision of patients in nursing homes. Each of the AGALZ agents is assigned to a nurse or doctor of a residence and additionally provides information on patient locations, historical data, and alarms. While staff members are carrying out their functions (following the plan envisaged by the agent), the plan may need to be modified due to delays or alarms. In this case, the agent is able to re-plan the initial proposed plan in real time.
Agreda et al. [17] analyze a possible solution to the problem of autonomy and independence of the elderly, which is mainly caused by the physical and physiological changes and the total or partial abandonment experienced by these people. In addition, authors attempt to solve this problem by analyzing and designing a model to provide the control of an intelligent environment that supplies aid and support to these people. The AmI environment attempts to help them in their daily lives by automating household processes, and by using all the information produced by the daily activity recorded to provide feedback to an intelligent model. This model serves as an information base to make decisions based on their behavior patterns and thus perform preventive actions to many of the typical problems of age with the appropriate alerts and additional procedures.
Restrepo et al. [18] propose an intelligent laboratory (SmartLab) located in a university environment. The authors use a meta-model to abstract the environment and its users, using WSN to acquire the contextual characteristics of the environment. It also uses intelligent agents to provide the required adaptation to offer personalized services according to the user’s environment. The architecture of the SmartLab comprises a physical layer, an agent layer, an application domain, and a service layer. The physical layer is composed of WSN which senses environmental physical variables (temperature and luminosity) and monitors the users. The agent layer implements the context, user, and adaptation models by using several intelligent agents. The application domain layer formalizes and transfers the knowledge acquired by the system in a language that is understandable to intelligent agents. Finally, the service layer uses software to implement the AmI services provided to the users.
Roda et al. [19] develop a multi-agent architecture for environmental intelligence systems in health, which contributes to the treatment of people with brain injuries (ABI). It uses specific devices to control the movements of the patient taking into consideration physiological responses, such as the variation of heart rate, during their rehabilitation process. In addition, author describes the manner in which this system designs and executes therapies for people with ABI. Its design offers a meta-model to define the rehabilitation environment. Finally, the AmI uses fuzzy inference systems that allow the system to adapt the therapies and make decisions about the order of activities, tasks to be performed, and steps to follow in real time.
Su and Peng [20] deal with ontological and epistemological problems, developing a rehabilitation information service based on an ontology called as OntoRis, and using the agent technology to explore external ontologies for its integration with the OntoRis foundation. The AmI environment offers a rehabilitation service based on OntoRis ontology to help patients acquire prescribed practical knowledge about their rehabilitation. The rehabilitation service also accelerates recovery through suggestions and advice provided by evidence-based medicine. In addition, OntoRis can also serve as an interactive learning platform for people who are interested in rehabilitation medicine.
From the previously reviewed research works, we can conclude that some works still present shortcomings such as the following: (1) they do not use ontologies for knowledge representation; (2) they do not define user profiles to offer personalized services; (3) some of them do not integrate WSN for contextual monitoring; (4) they do not offer user adaptive recommendations including a healthy personalized agenda. The aim of this paper is to face these shortcomings and to provide a comprehensive solution concerning the use of adaptive systems and patient profiles for monitoring, alerting and adaptively recommending patient’s health-care agenda.
4 Model Proposed
Figure 1 shows the architecture of the AmI model which is composed of six components as follows:

AmI system architecture for healthcare
-
Ontology: in this component the knowledge representation used by system is defined.
-
Sensors: this component contains the WSN that monitors blood pressure and blood glucose in patients. This network integrates technologies that allow monitoring, storage, and real-time transmission (minute-by-minute) of the monitored variables.
-
Database: this component stores all the information about the patient. This information contains not only the medical history of the patient but also its alerts, recommendations, and healthy agendas offered by the system.
-
Human-computer interface: this component represents the interface through which the system interacts with the user. This interaction is bi-directional, that is, both user and system are always ready to provide information to each other.
-
Users: this component represents the people who will use the system, in this case, patients and health professionals.
-
Multi-agent system: this component is composed of five agents that will be described below.
Figure 2 shows the ontological structure designed for the healthcare based system. Within the development of the ontological structure, the following three stages have been considered: the first examines the characterization of user profiles, the second is related to a healthy agenda, and the third concerns alerts and recommendations. The patient profile is composed of personal information (full name, identification, etc.), as well as features of the medical condition (medical history, diseases, etc.). The structure of the healthy agenda in turn, comprises information about scheduling tasks that the patient has to perform. The structure of the third component is divided into three fields: monitoring, alerts, and recommendations. Those fields correspond to a specific patient profile. The aim is to store all of the health information concerning a given patient.

Ontological structure
The multi-agent system consists of five software agents as follows:
-
Patient management agent: this agent is responsible for handling and supervising all the components of the system. Its functions include communication with all other agents, storage in databases, ontology implementation, and human-computer interface execution.
-
Monitoring agent: this agent is responsible for managing the communication with the sensors, receiving the monitoring information that sensors perform. In addition, it sends the gathered information to the patient’s management agent.
-
Alert agent: this agent is responsible for constantly monitoring the information gathered by the monitoring agent. Continuous supervision is performed in order to immediately alert the patient in case of some of the monitored values are outside of the normal range.
-
Recommendation agent: this agent is responsible for analyzing the alerts issued by the alert agent. This allows it to recommend actions that should be taken as soon as possible to stabilize the levels of the monitored variables.
-
Healthy agenda agent: this agent is responsible for analyzing the responses given by the patient through the questionnaire. The user profile and the analysis of the patient’s responses allow to create an agenda of tasks that must be executed by him. These tasks help the diabetes and hypertension patients to maintain healthy lives.
5 Implementation and Validation
The prototype was implemented using various technologies depending on the particular system component. Next, we describe how each component was addressed and the technology used:
-
Ontology: this component was developed using the Protégé tool V5.2.0. In addition, inference rules were developed that allow the system to make decisions. Inference rules were made with the support of WHO (World Health Organization) information about diseases (https://www.who.int/es).
-
WSN: this component employed a commercial electronic card along with custom development software. The Arduino card was used in order to simulate the variables monitored to the chronic patient. The Xbee module was used as an interface for wireless communication between the Arduino and the AmI system. Figure 3 shows the AmI system components.
Fig. 3. 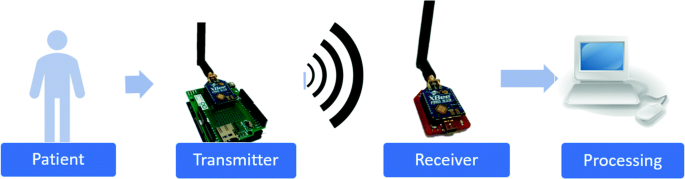
AmI system components. From left to right: patient, Arduino-based wireless monitoring system, Xbee receiver module, computer.
-
Database: this component developed in MySQL stores the patient’s information as well as the relevant information offered by the system to the patient.
-
Human-computer interface: this component was developed using NetBeans, a platform of modular components used to develop Java desktop applications.
-
Users: this component was implemented, simulating five patient profiles considering several possible cases. It is considered for example how advanced the disease is and if the patient has both diabetes and hypertension at the same time.
-
SMA: this component was implemented, using JADE as a platform for agent development. Figure 4 shows the communication performed between agents.
Fig. 4. 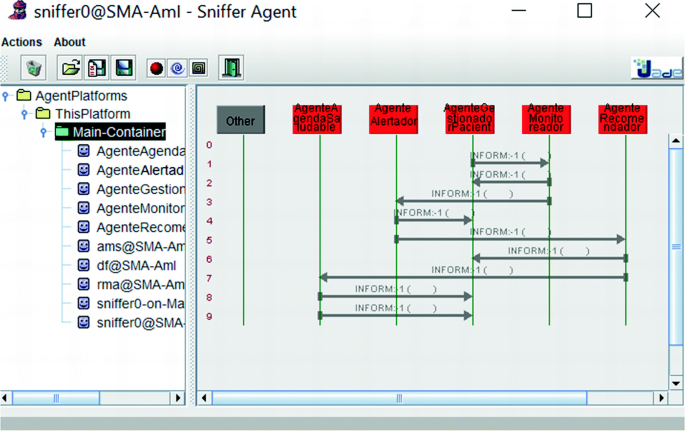
Communication performed between agents using the JADE platform.


The AmI system autonomously performs alerts and recommendations in the presence of abnormal values of blood pressure or blood glucose.
In addition, the AmI system offers a healthy personalized weekly agenda adapted to the patient’s health conditions. To do so, the system takes into account four inputs namely: (1) the information from the sensors that generate alerts; (2) the information provided by the patient through a questionnaire (see Fig. 5); (3) information from the previous healthy agenda, and finally, (4) information from the patient’s medical history. Figure 6 presents the results of an alert and a recommendation provided by the system to a patient with arterial hypertension. In this case, the pressure reaches the value of 183/145 mmHg and therefore the system reacts, sending alerts and recommendations to the patient. An email is also sent to the health professional in charge of this patient.

Questionnaire used as input to generate a healthy agenda.

Alerts and recommendations issued for a hypertension patient.
Figure 7 exhibits an adaptive healthy agenda which is organized into three components: physical, food, and psychological. It is about a patient with diabetes, who is not rigorous this week in complying with the tasks given by the healthy agenda.

Weekly scheduled tasks composing an adaptive healthy agenda.
In addition, the patient had an episode of very high level of blood glucose, during the previous week. Therefore, the new healthy personalized agenda issued from the AmI system brings new tasks and reminds him that he had a worrying event.
To validate the prototype model, several simulated chronic patient profiles are considered and their medical history is charged to the system database. The system takes into account the information of diseases, alerts, recommendations, and healthy agendas according to the patient’s user profile. Later, a health professional can consult all the medical history of monitored data, and the information that the system has given to the patient.
Another case study for the prototype is when the system detects inconsistencies between the healthy agenda of the previous week and the answers obtained in the questionnaire by the patient. The above means that the patient is not complying with the proposed healthy agenda. In this case, the system generates a warning call that will appear in the adapted healthy agenda that the system is currently generating.
We can see that the AmI system reacts adequately to different alert events and takes into account whether or not the patient complied with the previous healthy agendas. Otherwise the system generates a new adaptive healthy week’s agenda.
6 Conclusion and Future Work
From results obtained by the test of the prototype, we can conclude that the proposed AmI model fulfills the goals by providing integration among WSN, ontology, and multi-agent systems. In addition, the proposed model has the capacity to provide alerts, recommendations, and adaptive personalized healthy agendas according to the medical history, complying questionnaire, and previous healthy agenda of chronic patients.
Finally, as future work, it is proposed to complement the research using real patients along with commercial sensors in order to monitor health. Using the information of healthy agendas of other patients with similar profiles and applying a collaborative filtering technique could also be advantageous in order to improve the results obtained by the AmI system.
References
Burney, S., Mahmood, N., Abbas, Z.: Information and communication technology in healthcare management systems: prospects for developing countries. Int. J. Comput. Appl. 4(2), 27–32 (2010). https://doi.org/10.5120/801-1138
Oliveira, R., Frutuoso, S., Machado, J., Santos, M., Portela, F., Abelha, A.: Step towards m-Health in pediatrics. Proc. Technol. 9, 1192–1200 (2013). https://doi.org/10.1016/j.protcy.2013.12.133
Silva, B., Rodrigues, J.: A novel cooperation strategy for mobile health applications. IEEE J. Sel. Areas Commun. 31(9), 28–36 (2013). https://doi.org/10.1109/JSAC.2013.SUP.0513003
Free, C., Phillips, G., Watson, L., et al.: The effectiveness of mobile-health technologies to improve health care service delivery processes: a systematic review and meta-analysis. PLoS Med. 10(1) (2013). https://doi.org/10.1371/journal.pmed.1001363
Pereira, A., Marinsa, F., Rodrigues, B., et al.: Improving quality of medical service with mobile health software. Proc. Comput. Sci. 63, 292–299 (2015). https://doi.org/10.1016/j.procs.2015.08.346
Haya, P., Montoso, G., Alamán., X.: Un mecanismo de resolución de conflictos en entornos de inteligencia ambiental. In: Actas del Simposio de Computación Ubicua e Inteligencia Ambiental, UCAmI, pp. 11–18 (2005)
Venturini, V.: Sistema Multi-Agente basado en Contexto, Localización y Reputación para dominios de inteligencia Ambiental. Tesis de Doctorado en Ciencia y Tecnología Informática, Universidad Carlos III de Madrid – Escuela Politécnica Superior (2012)
Aarts, E., Marzano, S. (eds.): The New Everyday: Views on Ambient Intelligence. 010 Publishers, Rotterdam (2003)
Restrepo, S.: Modelo de Inteligencia Ambiental basado en la integración de Redes de Sensores Inalámbricas y Agentes Inteligentes. Tesis de maestría, Universidad Nacional de Colombia - Sede Medellín (2012)
Tramullas, J., Sánchez-Casabón, A.-I., Garrido-Picazo, P.: An evaluation based on the digital library user: an experience with greenstone software. Proc. - Soc. Behav. Sci. 73, 167–174 (2013). https://doi.org/10.1016/j.sbspro.2013.02.037
Gaeta, M., Orciuoli, F., Paolozzi, S., Salerno, S.: Ontology extraction for knowledge reuse: the e-learning perspective. IEEE Trans. Syst. Man Cybern. - Part A: Syst. Hum. 41(4), 798–809 (2011)
Mas, A.: Agentes Software y Sistemas MultiAgente: Conceptos, Arquitecturas y Aplicaciones. Pearson-Prentice-Hall (2004)
Wooldridge, M.: An Introduction to MultiAgent Systems (2009). http://books.google.com.br/books/about/An_Introduction_to_MultiAgent_Systems.html?id=X3ZQ7yeDn2IC&pgis=1
OMS: Información general sobre la hipertensión en el mundo, una enfermedad que mata en silencio, una crisis de salud pública mundial. Organización mundial de la salud (2013)
Sarmar, N., Gao, P., Seshasai., S., et al.: Diabetes mellitus, fasting blood glucose concentration, and risk of vascular diseade: a collaborative meta-analysis of 102 prospective studies, Emerging Risk Factors Colladoration. The lancet (2010)
Corchado, J.M., Bajo, J., de Paz, Y., Tapia, D.I.: Intelligent environment for monitoring Alzheimer patients, agent technology for healthcare. Decis. Supp. Syst. 44(2), 382–396 (2008). https://doi.org/10.1016/j.dss.2007.04.008
Agreda, J.A., Gonzalez, E.: Ambient intelligence based multi-agent system for attend elderly people. In: Proceedings of the 9th Computing Colombian Conference (9CCC) IEEE Conferences (2014)
Restrepo, S.E., Pezoa, J.E., Ovalle, D.A.: An Adaptive architecture for ambient intelligence based on meta-modeling, smart agents, and wireless sensor networks. IEEE Latin Am. Trans. 12(8), 1508–1514 (2014)
Roda, C., Rodríguez, A., Lopez-Jaquero, V., Navarro, E., González, P.: A multi-agent system for acquired brain injury rehabilitation in ambient intelligence environments. Neurocomputing 231, 11–18 (2017). https://doi.org/10.1016/j.neucom.2016.04.066
Su, C., Peng, C.: Multi-agent ontology-based Web 2.0 platform for medical rehabilitation. Expert Syst. Appl. 39, 10311–10323 (2012)
Acknowledgments
This research was developed by GIDIA (Artificial Intelligence Development Research Group) of the National University of Colombia, Medellin branch.
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this paper

Cite this paper
Patiño, M.F.J., Ovalle, D.A. (2019). Ambient Intelligence Model for Monitoring, Alerting and Adaptively Recommending Patient’s Health-Care Agenda Based on User Profile. In: Duffy, V. (eds) Digital Human Modeling and Applications in Health, Safety, Ergonomics and Risk Management. Healthcare Applications. HCII 2019. Lecture Notes in Computer Science(), vol 11582. Springer, Cham. https://doi.org/10.1007/978-3-030-22219-2_9
Download citation
DOI: https://doi.org/10.1007/978-3-030-22219-2_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-22218-5
Online ISBN: 978-3-030-22219-2
eBook Packages: Computer ScienceComputer Science (R0)