
Abstract
In Japan, which has the highest aging rate in the world, demand for long-term care (LTC) is rapidly increasing. However, the labor force is decreasing nationwide, and in particular the shortage of staff for LTC services is a serious problem. Japanese government aims to reduce the burden on staff at old people’s homes and improve the quality of LTC services by introducing ICT/IoT. The organizational culture in old people’s homes is the basis of the quality of LTC services; hence, we aimed to visualize it. For the purposes of this research, organizational culture is divided into the following eight domains: “teamwork,” “information sharing,” “morale,” “professional growth,” “common values,” “resource allocation prioritization,” “responsibility and authority,” and “improvement orientation.” A questionnaire survey on organizational culture was administered to 366 staffs in 23 old people’s homes and 4053 staffs in 4 hospitals. The response rates were 71.9% and 82.0%, respectively. The results revealed that old people’s homes have higher scores compared to hospitals on teamwork, information sharing, and organizational values, and that old people’s homes have problems in securing and fostering middle managers. It was suggested that effectively introducing ICT/IoT could enhance the organizational culture and increase the job satisfaction.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others

Keywords
1 Introduction
Japan currently has the highest proportion of people aged 65 years or older in the world, and has become one of the first “super-aged” societies. Following the increase in demand for long-term care (LTC) services, the number of old people’s homes has greatly increased in Japan [1]. On the other hand, the number of staffs engaged in LTC services is not sufficient. According to the Ministry of Economy, Trade and Industry in Japan, with the increase in the demand of LTC services due to the aging of the population, there will be a shortage of 790,000 care workers [2]. Due to the declining birthrate, human resources are lacking in all industries, particularly in the service industry. However, it is said that physical and mental burden and low salaries are responsible for human resource shortage in old people’s homes [3].
Under these circumstances, Japanese government is actively promoting the introduction of ICT/IoT/robots in LTC services to resolve the problem of staff shortage. These measures are not intended to merely reduce the physical burden of staff. Rather, by introducing ICT/IoT/robots, it is expected that the quality of LTC services can be improved by increasing the duration of contact with the user, and it will facilitate quick detection of the change in the user’s state. If these initiatives can help improve the satisfaction level of staff, it may contribute to securing staff.
The organizational culture of the staff can be considered as the basis of the quality of LTC services. Organizational culture is defined as the pattern of shared basic assumptions, invented, discovered, or developed by a given group, as it learns to cope with its external and internal problems [4]. In particular, in medical care and LTC services, human-human interaction is very frequent. Previous studies have shown that the organizational culture of hospital staff is related to the quality of medical care provided at a given hospital [5]. It is assumed that a similar relationship is found in LTC services. However, organizational culture in LTC services has hardly been investigated and elucidated so far. Kobuse et al. (2014) developed the questionnaire for organizational culture in hospitals and confirmed statistical validity [6]. Based on the questionnaire, we developed a revised questionnaire for LTC services, and its statistical reliability and validity was confirmed [7].
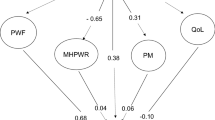
As shown in Fig. 1, organizational culture is related to the interaction between staff, the interaction between staff and users, and the interaction between staff and system (including ICT/IoT). Thus, through the visualization of organizational culture, it is also possible to verify the effect of introducing ICT/IoT. Therefore, we aimed to visualize the organizational culture in LTC services, which is the basis of the quality of LTC services, and describe its characteristics. To clarify the characteristics of organizational culture in old people’s homes, we compared it with that of hospitals. In the future, these findings can become the basis for verifying the impact of introducing IoT/ICT on organizational culture.

The concept of organizational culture and user, staff, system in old people’s home
In this study, we compared the organizational culture in hospitals and old people’s homes, and across professions and management/non-management positions in old people’s homes. In addition, we investigated factors related to job satisfaction. Finally, we will provide examples of initiatives that utilize ICT and IoT at old people’s homes.
2 Methods
2.1 Organizational Culture
As shown in Table 1, organizational culture is composed of the following eight domains: “collaboration,” “information sharing,” “professional growth,” “morale,” “common values,” “resource allocation prioritization,” “responsibility and authority,” and “improvement orientation.” In addition to organizational culture, domains related to work/workplace environments such as “job satisfaction” and “workload and burden” are also measured. There are 2 to 7 questions for each domain, and the total number of questions is 58. We used the established scoring method where a higher score is better.
2.2 Questionnaire Survey and Statistical Analysis
We administered the questionnaire survey to 366 staffs in 23 old people’s homes of 3 corporations. In addition, 4,053 hospital staffs in 4 hospitals were surveyed as comparison subjects. These included doctors, nurses, allied health personnel, administrative staff, and others. These surveys in both LTC and hospitals settings were conducted from October 2017 to August 2018. The participants were informed that there was no obligation to participate in the study, but that submitting a questionnaire would imply consent to participation. The answered questionnaires were sealed and collected by the researchers. Confidentiality and anonymity were protected during the entire study procedure. This study was approved by the Ethics Committee, Kyoto University Graduate School and Faculty of Medicine.
For the comparison, t test and one-way analysis of variance were used. To clarify factors related to job satisfaction, we performed multiple regression analysis. Our model used job satisfaction as the objective variable. Explanatory variables included the eight domain scores, as well as the respondents’ profession, position, and dummy variable of each corporation. Analyses were performed using R 3.5.1.
2.3 Interview
Among old people’s homes cooperated in our questionnaire survey, we conducted an interview with the administrator of an advanced old people’s home (Home A) that had effectively adopted ICT/IoT. We asked what aspects of ICT/IoT were introduced, what impact they had on the work of staff. In addition, the organizational culture survey was also conducted at that home (its data are included in the above analysis).
3 Results
Of the 366 staffs surveyed in old people’s home, 263 responded (overall response rate: 71.9%). Of the 4053 staffs surveyed in hospitals, 3323 responded (overall response rate: 82.0%).
As shown in Fig. 2, when comparing the results for the hospitals and the old people’s homes, it was found that the old people’s homes had a significantly higher score in “team work,” “information sharing,” and “organization values” (p < 0.05). On the other hand, “growth as a professional” and “improvement orientation” were higher in the hospitals, but the difference was not significant. With regard to work/workplace environment, the old people’s homes had higher “job satisfaction” than the hospitals (p < 0.05) (Table 2).

Comparison of organizational culture scores of hospitals and old people’s homes
In addition, when comparing staffs across positions in old people’s homes, executives had a high overall score compared to other positions (see Fig. 3). Note that the scores of the middle managers were lower than those of the non-managers in all domains except “responsibility and authority.” In the case of hospitals, the score of middle managers was higher than that of non-managers. There may be a problem in the middle management positions in old people’s homes.

Comparison of organizational culture scores across positions in old people’s homes
Multiple regression analysis showed that “Teamwork,” “Professional growth,” “resource allocation prioritization,” “responsibility and authority,” middle manager, and non-manager were significantly associated with job satisfaction.
We conducted interviews at Home A, an old people’s home actively using ICT/IoT. The characteristic of this home is the three monitors in the office (see Fig. 4). The monitor on the left shows activity status and sleeping state of each resident sent from the air conditioner equipped with monitoring system. This system reduces the number of staff visits to the residents’ rooms, which leads to the reduction of burden on staff. The right side of it is the picture of the surveillance camera installed in the corridor, cafeteria, and building surroundings. It is possible for the camera to capture falls, wandering residents, and other troubles among residents. By looking at these two monitors, the staff instantaneously grasps the situation of the residents and prioritize their tasks. The monitor in the middle has a different function; it is interlocked with a car navigation system of a shuttle car, and provides business support by using AI in pickup scheduling, route guidance, safe driving, etc. This system can reduce business hours.

Photo showing the use of ICT/IoT in the office of Home A
In fact, home A had higher scores in “resources” and “responsibility and authority” than in other homes (see Figs. 5 and 6). In addition, “employee satisfaction level,” “workload and burden,” “work improvement,” “facility effort” also gave higher scores than other homes.

Score of resource allocation prioritization at each old people’s home

Score of responsibility and authority at each old people’s home
4 Discussion
4.1 Characteristics of Organizational Culture in Old People’s Home
Old people’s homes had higher scores than hospitals in “team work,” “information sharing,” “common values.” This difference may be due to the fact that old people’s homes are smaller in size than hospitals (number of staffs, number of patients/users, buildings, etc.). In fact, the average number of staffs at the surveyed hospital was 1013.3 people, whereas at the old people’s home there were 15.9 people. Some old people’s homes that were surveyed have conferences in which all staff members participate. In addition, differences in the length of stay of patients/users may also influence information sharing. The average length of stay in hospitals is about 16.3 days [8], but many users of old people’s homes stay in them for several years. In old people’s homes, staff frequently share information on users.
On the other hand, in the “professional growth” and “improvement orientation” domains, although not statistically significant, the hospital’s score was slightly higher than that of the old people’s home. It is important to provide opportunities for education and training to employees in medical care and LTC services as professionals. However, since old people’s homes generally have limited financial capability and a small number of staffs, many homes are unable to provide such opportunities. In order to raise the quality of nursing staff, Japanese government offers common national training and national qualifications, and is supporting the improvement of their career path [9]. Some homes utilize educational opportunities through e-learning. In addition, it is reported that when staffs for care provided an educational program using printed educational materials on dementia, the stress of staffs reduced [10].
Comparing the organizational culture scores for different positions in old people’s homes, the scores for middle managers tended to be generally lower than non-managers. When interviewing the executives of the surveyed old people’s home, the staff tended not to want to become managers, which was seen as an increase in burden and difficulties in managing staff. For LTC services, securing and fostering middle managers can be mentioned as an issue.
4.2 Job Satisfaction in Old People’s Home
Job satisfaction is an important Key Performance Indicator (KPI) in LTC services, where securing of staff is the most important issue. Our findings showed that job satisfaction was related to “teamwork,” “professional growth,” “resource allocation prioritization,” and “responsibility and authority.” Interestingly, Home A, which actively utilizes ICT/IoT, had high scores on “resource allocation prioritization,” “responsibility and authority,” and job satisfaction. Introduction of ICT/IoT may have the effect of enhancing these domains and help retention management.
4.3 The Introduction of ICT/IoT in Old People’s Home
There are several reasons why the introduction of ICT/IoT does not progress in old people’s homes. In LTC services industry, handwritten documents are used in most workplaces, and many nursing staffs are accustomed to writing in Japan as well as US [11]. Therefore, it is necessary to change workplace practices and educate and skill staff for the introduction of ICT/IoT. Further, as many staffs in LTC services are relatively older compared to those in other industries [12], their IT literacy is insufficient, which is a challenge while introducing ICT/IoT. In addition, it is difficult to introduce new technologies in old people’s homes because they have limited funds and human resources. Finally, there are few easy-to-use products and services. For example, products that take time to set up or cause discomfort to users cannot be used in old people’s homes, even when they can lower the physical burden of staff. In the future, further collaboration between staff in LTC services and engineers is desirable. We will continue research to support the development of products/services that can resolve these problems.
4.4 Limitations
There are several limitations in the study. First, the number of survey participants at the facility utilizing IoT was small, and the effect of IoT could not be verified sufficiently. In the future, we will increase the number of participants. Second, we could not administer a questionnaire survey to users. Improvement of user satisfaction and quality of life is an important outcome in nursing care services, and its relation to IoT introduction is also very interesting. We are currently working on questionnaires for users.
5 Future Work
Through our research, we have clarified the characteristics of organizational culture in old people’s homes. In the future, we will verify the effect before and after introducing IoT concretely through organizational culture survey and user survey.
We have started building monitoring services using IoT in collaboration with Panasonic, with the aim of “reducing the burden on old people’s homes and improving the QoL of users.”
The overall structure of this system is as follows (see Fig. 7).

System diagram of watching security system
System configuration
-
High sensitivity room sensor (Doppler sensor, Pressure sensor, etc.):
-
Detects incidents such as heat stroke and dehydration symptoms in users, monitors safety at night
-
-
IP-Camera system:
-
Extensively captures the activities and condition of the residents in old people’s homes.
-
-
Tablet terminal · Mobile phone
-
Automatic record of staff behavior, such as the behavior of a caregiver. Reflect on progress notes, etc.
-
-
Cloud server
-
Aggregate the big data of user’s activities and visualize them
Health rehabilitation. Creation of LTC services program
-
-
AI prediction technology
-
Forecasting and prediction with AI-based data analysis using all the aspects/elements of health and LTC services data.
-
In the future, we will evaluate and visualize the quality of LTC services before and after introduction of the IoT watching service, using the organizational culture and user satisfaction survey. Moreover, we would like to analyze the causal relation between comparisons and differences among homes.
6 Conclusion
Through the visualization of the organizational culture, which is the basis of the quality of LTC services, we clarified the characteristics of old people’s home. Compared to hospitals, old people’s homes had high score on “team work,” “information sharing,” and “organizational values.” In old people’s homes, challenges were found in securing and fostering middle managers. The scores for resources, responsibilities and authorities, and job satisfaction are high in old people’s homes that have effectively introduced ICT/IoT. We will further conduct surveys before and after ICT/IoT introduction in the future.
References
Cabinet office, Government of Japan, Annual Report on the Aging Society: 2017 (summary) (2017)
Ministry of Economy, Trade, and Industry, the Report by the Study Group on the Provision of Nursing Care Services in Response to Future Nursing Care Demand (2016). (in Japanese)
Ministry of Health, Labour and Welfare: Securing care workers (2014). (in Japanese) https://www.mhlw.go.jp/file/05-Shingikai-12201000-Shakaiengokyokushougaihokenfukushibu-Kikakuka/0000047617.pdf
Schein, E.: Organizational Culture and Leadership. Jossey-Bass, San Francisco (1985)
Ukawa, N., Tanaka, M., Morishima, T., Imanaka, Y.: Organizational culture affecting quality of care: guideline adherence in perioperative antibiotic use. Int. J. Qual. Health Care 27, 37–45 (2015)
Kobuse, H., et al.: Visualizing variations in organizational safety culture across an inter-hospital multifaceted workforce. J. Eval. Clin. Pract. 20, 273–280 (2014)
Hara, K., Nakabe, T., Imanaka, Y.: Visualized organizational culture by type of old people’s home/occupation type and consideration factors related to desire to continue working. In: The 56th Conference of the Japan Society for Healthcare Administration, The Japan Society for Healthcare Administration, Fukushima (2018)
OECD: Health at a Glance 2017 - OECD Indicators. OECD Publishing, Paris (2017)
Ministry of Health, Labour and Welfare: Comprehensive and systematic promotion of securing care workers (2015). (in Japanese) https://www.mhlw.go.jp/file/05-Shingikai-12201000-Shakaiengokyokushougaihokenfukushibu-Kikakuka/document2-1.pdf
Fukuda, K., et al.: Effectiveness of educational program using printed educational material on care burden distress among staff of residential aged care facilities without medical specialists and/or registered nurses: cluster quasi-randomization study. Geriatr. Gerontol. Int. 18, 487–494 (2018)
Bjarnadottir, R.I., Herzig, C.T.A., Travers, J.L., Castle, N.G., Stone, P.W.: Implementation of electronic health records in US nursing homes. Comput. Inform. Nurs. 35, 417–424 (2017)
Ministry of Health, Labour and Welfare: The current state of LTC service labor (2017). (in Japanese) https://www.mhlw.go.jp/file/05-Shingikai-12602000-Seisakutoukatsukan-Sanjikanshitsu_Roudouseisakutantou/0000071241.pdf
Acknowledgments
This work is supported in part by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (Grant number: A16H02634) and a Grant for Academia-Government-Industry collaboration research from the Open Innovation Lab (a general incorporated foundation). We would like to thank old people’s homes and hospitals for cooperating in the study.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this paper

Cite this paper
Hara, K., Nakabe, T., Naka, T., Tanaka, M., Imanaka, Y. (2019). Visualizing Organizational Culture in Old People’s Homes and Hospitals in Japan: Human Interaction in the IoT Era. In: Zhou, J., Salvendy, G. (eds) Human Aspects of IT for the Aged Population. Social Media, Games and Assistive Environments. HCII 2019. Lecture Notes in Computer Science(), vol 11593. Springer, Cham. https://doi.org/10.1007/978-3-030-22015-0_25
Download citation
DOI: https://doi.org/10.1007/978-3-030-22015-0_25
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-22014-3
Online ISBN: 978-3-030-22015-0
eBook Packages: Computer ScienceComputer Science (R0)