
Abstract
Kawasaki disease (KD) is the commonest cause of acquired heart disease in children in the developed world and is increasingly being reported from developing countries. KD has a predilection for the coronary arteries. Etiology of this disorder is remains an enigma. Diagnosis of KD is essentially clinical with the help of set of clinical criteria. Incomplete KD is said to occur when these criteria are not fulfilled. However, incomplete KD should not be considered as a milder form of the disease. 2D-echocardiography remains the imaging modality of choice for evaluation and monitoring of cardiac complications but often needs to be supplemented by CT coronary angiography. Intravenous immunoglobulin along with aspirin is the gold standard therapy of treatment for KD. However, there is no consensus on treatment of resistant forms of KD. Patients with KD should be on long-term follow-up especially if they have developed coronary artery abnormalities during the acute stage.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
Kawasaki disease (KD) is an acute and usually self-limiting medium vessel vasculitis of childhood that has a predilection to involve the coronary arteries. It is characterized by the sequential appearance of a constellation of clinical features [1]. However, none of these clinical findings is, in itself, pathognomonic of KD. Many of these clinical features can, in fact, be seen in other common febrile illnesses of children. It is for this reason that the diagnosis of KD is often considered to be a clinical challenge [2]. Approximately 15–25% of untreated patients may go on develop coronary artery abnormalities (CAAs) and this remains the major cause of morbidity, and occasional mortality, in KD [3].
4.1 History
KD was first recognized in 1961 by Dr. Tomisaku Kawasaki while working at the Japan Red Cross Medical Centre at Tokyo. He saw a 4-year-old boy with fever and a constellation of clinical features that did not seem to fit into any known clinical disease entity. By 1967, he had collected 50 such cases of mucocutaneous lymph node syndrome and published his series in the Japanese Journal of Allergy (Arerugi) [4]. It is remarkable that to this day, the case definition proposed by Dr. Kawasaki in 1967 has remained largely unchanged.
4.2 Epidemiology
KD is arguably the second commonest vasculitis of childhood after Henoch–Schonlein purpura. It is a disease of young children with 80% of affected patients being below the age of 5. Peak age of onset is around 6–11 months in Japan and 2–3 years in North America. KD occurs more commonly in boys and the male female ratio is 1.3:1 [5]. Siblings can be affected in 3% of patients [6].
KD has been reported from all continents and is now increasingly being identified in many resource-challenged countries (Fig. 4.1). Although this disease is being diagnosed worldwide, the highest number of cases has been reported from the North-East Asian countries, viz. Japan, Korea, and Taiwan [7]. The current incidence of KD in Japan is more than 300 per 100,000 children <5 years (highest worldwide) [8]. Approximately 1% of Japanese children develop KD by age 10 [9]. Incidence rates from Korea and Taiwan are 194.7 and 69.5, respectively [10, 11]. Incidence of KD in Europe and the United States has plateaued and ranges from 5 to 30/100,000 children below 5. Data from North America show that there is significant ethnic variation with higher rates being reported in African Americans and Pacific islanders [7]. KD is currently being diagnosed and reported from both China and India but nationwide data are not available in these countries [12,13,14,15,16]. In North India, the KD incidence is 4–5/100,000 children below 5 [16].

Epidemiologic variation of KD in different areas
Epidemiologic studies have shown distinct seasonality in occurrence of KD. Japan and Korea have two peaks—in June/July and December/January [17], while Taiwan has a peak in May/June [7]. In Chandigarh (India), the peak incidence is in April and October, with a nadir in February [16].
4.3 Genetics
KD is a complex disorder in which an infectious/environmental agent is believed to trigger the onset of disease in a genetically susceptible host [18]. Various susceptibility genes have been identified to have association with KD. These includes inositol 1,4,5-trisphosphate 3-kinase C (ITPKC), Caspase-3 calcium release-activated calcium modulator 1 (ORAI1), and CD 40 [19,20,21]. Knowledge about these susceptibility genes may provide new insights in etiopathogenesis of KD. Reports have suggested association of transforming growth factor (TGF)-β variants with development of CAAs in patients with KD [22].
4.4 Etiopathogenesis of KD
Although etiopathogenesis of KD is not clear, various epidemiological and laboratory studies have shown that an infectious agent triggers a cascade that causes the illness (Fig. 4.2). Histopathologic studies have emanated from children with KD who have died from unrelated causes [23]. The vasculitic process shows three distinct phases [24]:
-
(a)
Acute necrotizing arteritis phase: in which there is neutrophilic infiltration of intima and media.
-
(b)
Subacute/chronic arteritis phase: in which the neutrophilic infiltrate gets replaced by lymphocytes, plasma cells, and macrophages.
-
(c)
Luminal myofibroblastic phase: in which there is proliferation of smooth muscle cells in the media that can result in luminal narrowing [24, 25].

Etiopathogenesis of KD. Abbreviations: ABCC4 ATP-binding cassette sub-family C member 4, BLK B-cell lymphoid kinase, FCγR2A Fc γ receptor 2A, HLA human leukocyte antigen, IL interleukin, ITPKC inositol 1,4,5-trisphosphate kinase-C, ORAI1 calcium release-activated calcium modulator 1, TGF-β transforming growth factor-β, TLR toll like receptor, TNF-α tumor necrosis factor
The etiopathogenesis of KD is closely linked to an infectious process. Evidence for this comes from both seasonability and clustering of cases of KD [7, 26]. The presence of febrile exanthemata and cervical lymphadenopathy, uncommon occurrence in babies below 3 months, and the rarity of cases in adults, further lends support to this hypothesis. Some of the infectious agents that have been linked to the etiology of KD are parvovirus, Epstein–Barr virus, Staphylococcus aureus, chlamydia, and mycobacteria. It has been hypothesized that the putative infectious trigger sets up a cytokine storm that manifests as KD [23]. Some investigators have also proposed a super-antigen theory that triggers an immune response against vascular endothelium [27].
4.5 Clinical Features and Diagnosis
Diagnosis of KD is essentially clinical. Criteria for diagnosis of KD have been updated from time to time. Currently there are two sets of guidelines—American Heart Association (AHA) guidelines (2004 [3] and 2017 [28]) and Kawasaki Disease Research Committee guidelines (Japanese guidelines), 2002 (Table 4.1) [29]. AHA 2017 guidelines (clinical criteria) for diagnosis of KD are given in Table 4.2. Patients who fulfil the criteria are classified as having complete KD (also known as classical or typical KD), while those who do not fulfil criteria are classified as incomplete KD [28]. Principal clinical features in KD are reviewed in Table 4.3.
The clinical course of KD has three distinct phases: (a) acute febrile phase, (b) subacute phase, and (c) convalescent phase [4]. However in clinical practice, these features often overlap.
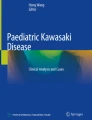
Acute phase: This phase starts with abrupt onset of high grade fever that is characteristically accompanied by significant irritability. It usually lasts for 10–14 days. Fever with marked irritability may be the initial clinical presentation of KD, especially in young infants [30]. Presence of intermittent or remittent fever is not characteristic of KD. Cough can be present in a small subset of patients but nasal catarrh is unusual for KD. Rash in KD is usually generalized, erythematous, polymorphic (Fig. 4.3b), but is never vesicular or bullous. Cervical lymphadenopathy (≥1.5 cm size) is usually unilateral and is often more commonly seen in the anterior cervical triangle. Cervical lymphadenopathy may be mistaken for suppurative lymphadenitis. AHA 2017 guidelines have highlighted the importance of ultrasonogram and computed tomography (CT) for differentiation of bacterial lymphadenitis from KD lymphadenopathy. In KD, there is enlargement of multiple lymph nodes along with retropharyngeal edema while bacterial lymphadenitis is mostly associated with a single lymph node with a central hypoechoic region [28]. However, such differentiation on basis of ultrasound examination requires lot of expertise and that may not be readily available in the usual clinical setting. Oral cavity and lip changes include redness of lips with bleeding and vertical cracking, oral mucosa redness and a strawberry tongue (Fig. 4.3d). Oral ulcers are distinctly unusual in KD. Conjunctival injection is characteristically nonexudative and with typical sparing of limbus (Fig. 4.3a). Conjunctivitis with discharge is a strong pointer towards an alternative diagnosis. Edema of the dorsum of extremities is an early sign and is usually transient (Fig. 4.3e). Perianal desquamation is virtually pathognomonic of KD and is a useful clinical sign for diagnosis of the disease during the acute phase (Fig. 4.3c). Arthritis in KD is typically oligoarthritis, involving large joints and resolves without sequelae [31]. Erythema at BCG injection site is an important clinical sign during acute stage of KD and more common in infants [32]. Hydrops of gall bladder is also an important finding during acute stage. Mild pericardial effusion is a common finding on 2Dechocardiography (2DE). CAAs are usually not seen during the first week of illness.

Clinical manifestations of typical KD. (a) Conjuctival injection; (b) maculopapular erythematous rash; (c) classical perianal desquamation; (d) strawberry tongue and cracked red lips; (e) dorsal edema over feet; (f) classical periungual desquamation; (g) Beau’s line
Subacute phase: This stage usually lasts for another 2–3 weeks during which fever usually subsides. Periungual peeling is characteristically seen during this stage (Fig. 4.3f). Irritability that is prominent during acute phase subsides completely in this phase. Arthritis in KD can also develop in subacute phase. CAAs most commonly become apparent during this time. An important laboratory manifestation that is seen in the subacute phase is development of thrombocytosis and this in conjunction with periungual desquamation is very suggestive of KD.
Chronic phase: It lasts for few weeks to months; there are no symptoms during this phase and the inflammation tends to subside. Beau’s lines presents as horizontal ridging over nails and first manifest at the subsidence of the subacute phase (Fig. 4.3g). This is the only clinical sign of KD that can be seen for several weeks.
4.6 Differential Diagnosis
Measles can present with similar clinical features; however, the presence of a viral prodrome, exudative conjunctivitis and Koplik spots will help to differentiate measles from KD. In measles, lymphocytic leucocytosis is usually prominent (unless there is secondary infection) while children with KD have polymorphonuclear leucocytosis. Procalcitonin levels are normal in measles but may be elevated in KD. Other infectious causes that can mimic KD include viral infections (cytomegalovirus, adenovirus, Epstein Barr virus, and enterovirus), bacterial infections (bacterial cervical lymphadenitis, scarlet fever, toxic shock syndrome, staphylococcal scalded skin syndrome, and leptospira), and systemic juvenile idiopathic arthritis. Absence of eye changes and lip changes, presence of sand paper rash, elevated antistreptolysin O titres, and a brisk response to antimicrobials are pointers towards scarlet fever. Presence of exudative conjunctivitis, ulcerative lesions in oral cavity, exudative pharyngitis, generalized lymphadenopathy and significant running nose are certain clinical features that make the diagnosis of KD less likely [28].
4.7 KD in Special Situations
4.7.1 Incomplete KD
The diagnosis of KD is challenging and requires experience. Clinical features of KD are nonspecific and overlap with various common childhood disorders especially infections [33]. Patients who are not fulfilling clinical criteria completely are labelled as incomplete KD. In these situations, one has to rely largely on clinical assessment supplemented by laboratory parameters. Incomplete form of KD is more commonly seen in infants (especially in babies below 6 months). Approach for diagnosis of incomplete KD has been simplified in new AHA 2017 guidelines [28]. Incomplete KD should, by no means, be considered a milder form of KD.
4.7.2 Atypical KD
A patient can be said to have atypical KD if the clinical manifestations are unusual. These atypical manifestations may include arthritis [31], nephritis [34], pneumonia [35], myositis, central nervous system involvement, uveitis [36], and retinal vasculitis [37]. Common neurological findings include extreme irritability and aseptic meningitis. Rare neurological manifestations include transient peripheral facial nerve palsy (mostly unilateral) and profound sensorineural hearing loss. Vomiting, diarrhea, and transient hepatitis are common gastrointestinal manifestations [38]. Other relatively uncommon findings include jaundice, gall bladder hydrops, and pancreatitis. Genitourinary findings include urethritis which usually presents as sterile pyuria [39]. Atypical presentations of KD can pose difficult clinical problems for the attending physician.
4.7.3 KD in Infants
In infancy, and especially in babies below 6 months, KD is often a diagnostic challenge because it may present with incomplete manifestations. KD in this age group may often remain undiagnosed for several days, leading to increased incidence of development of CAAs . This group of patients also has higher intravenous immunoglobulin (IVIg) resistance [28, 30, 40, 41]. Sterile pyuria is another clinical presentation of KD in this age group and may mistakenly get treated as a urinary tract infection. The consequent delay in diagnosis can result in serious clinical sequelae [39]. Due to these reasons, KD in infants has been given special consideration in new AHA guidelines. It has been highlighted that if an infant has fever for more than 7 days without explanation, KD should always be in list of differential diagnosis.
According to AHA 2017 guidelines KD should be considered as a clinical possibility in the following situations:
-
Babies <6 months who present with fever and extensive irritability.
-
Infants having prolonged fever and unexplained aseptic meningitis.
-
Children presenting with longer duration of fever and
-
Culture-negative hypotensive shock.
-
Cervical adenopathy that is unresponsive to antibiotic therapy.
-
Parapharyngeal or retropharyngeal phlegmon that is unresponsive to antibiotic therapy.
-
4.7.4 KD in Older Children and Adolescents
KD is uncommon in older children and may often go unrecognized. Due to missed or delayed diagnosis, there is higher risk of CAAs in this age group. It may be difficult to assess CAAs by 2DE in this age group of patients because of limited acoustic window and thick chest wall [42, 43].
4.7.5 KD Shock Syndrome
Myocarditis in KD is said to be very common and may even be universal. It is not often recognized and can, at times, be severe and symptomatic. Myocarditis can develop during acute stage and manifest with unexplained tachycardia, hemodynamic compromise, or cardiovascular collapse [44]. Approximately 5% patients with KD can present with cardiovascular collapse. This entity is known as KD shock syndrome (KDSS). The shock in these patients is multifactorial and may have both cardiogenic and distributive components. The distributive shock may result from cytokine storm leading to uncontrolled inflammation [45]. Patients with KDSS are usually present to emergency room and intensive care units with shock and may be inappropriately treated for bacterial sepsis and presumed septic shock. Diagnosis of KD gets often delayed in these cases and can have devastating consequences. Differentiation between KDSS and septic shock in the early phase of clinical diagnosis is often challenging. However, 2DE should always be performed in patients with fever and shock as presence of CAAs will suggest KDSS. Differentiation of KDSS and septic shock is critical as management of both diseases is entirely different. Presence of conjunctival injection, dorsal edema, perineal desquamation, incomplete response to antimicrobials, and no microbiological evidence for infection are indicators towards KD in these patients. These patients are reported to have increased risk of having IVIg resistance, CAAs , and myocardial dysfunction [28, 46, 47]. It is said that KDSS should always be considered in children presenting with fever, cardiovascular collapse and myocardial dysfunction. KDSS has been discussed at length in the AHA 2017 revised guidelines because of these highlighted facts [28].
4.7.6 Infection Triggered KD
Infections have been commonly considered as triggers for KD. At the bedside, it is often difficult to differentiate the clinical features of KD from that of viral exanthemata. However, if a child is having typical clinical features of the KD, the diagnosis cannot be excluded even in the presence of a documented infection. Adenovirus, coronavirus, dengue virus, enteroviruses, measles virus, respiratory syncytial virus have been reported to trigger the KD in children [23]. Toxin-mediated diseases (e.g., staphylococcal and streptococcal infection) have also been also closely associated with the pathogenesis of KD [27]. Candida infection has been linked to the causation of KD in mice models and as well as in epidemiological studies carried out on tropospheric wind patterns in Japan and Hawaii [48].
4.8 Laboratory Investigations
The acute phase is characterized by a mild normocytic normochromic anemia, polymorphonuclear leucocytosis, raised erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and usually a normal platelet count. Serum procalcitonin, that is usually thought to be a sensitive and specific marker for bacterial infection, may get elevated in KD as well. Thrombocytosis develops during the end of second week or in the third week; however it may even develop earlier [49]. Presence of thrombocytopenia during acute stage suggests either macrophage activation syndrome or thrombotic microangiopathy—this is associated with poor prognosis [28]. Progressive thrombocytosis has been correlated with development of CAAs . Urine may show sterile pyuria, secondary to urethritis and easily mistaken as urinary tract infection especially during infancy, thereby resulting in delay in diagnosis of KD [39]. It is said that KD is the commonest cause of sterile pyuria in children.
4.9 Biomarkers in KD
Diagnosis of KD is essentially clinical and there is no gold standard for confirmation of diagnosis. It is no surprise, therefore, that several biomarkers have been extensively evaluated for their role in diagnosis of this condition. Various cytokines (e.g., tumour necrosis factor-α (TNF-α), interleukin 6) have been found to be raised during the acute phase of KD and decrease promptly following IVIg administration. In patients with refractory KD or CAAs levels of TNF-α continue to remain elevated [50]. Various microarray based studies have been carried out to identify the genes associated with KD. Expression of these genes may be used as a novel diagnostic and prognostic biomarker for KD [51].
N terminal pro-B-type natriuretic peptide (NT-proBNP) is a cardiac biomarker that has recently been found to be raised in children with KD during the acute phase. Age-based nomograms for Pro-BNP are available. These are helpful in differentiation of KD from other febrile illnesses [52]. The values for Pro-BNP are comparatively higher in patients who develop CAAs as compared to patients with normal coronaries [53]. ProBNP levels also correlate with myocardial dysfunction [45].
4.10 Two-Dimensional Echocardiography (2DE)
Cardiac evaluation is an essential component in patients with KD. 2DE is an important tool for coronary artery assessment and, evaluation of cardiac structures during acute phase as well as on follow-up. However, diagnosis of KD should never be ruled out on basis of normal 2DE examination. The quality of scan obtained by 2DE is operator dependent [43].
Criteria for definition of CAAs have been given by AHA as well as by the Japanese Ministry of Health. According to the latter coronary involvement in KD is categorized on basis of absolute internal diameter of coronary artery (Table 4.4) [54]. Manlhiot et al. have proposed definition of CAAs on the basis of Z score which is widely accepted currently and also has been adapted by AHA 2017 guidelines (Table 4.4) [28, 55]. It is mandatory to use body surface area-adjusted ‘Z’ scores for grading the severity of CAAs . Patients with a maximal Z score >+2.5 are classified to have aneurysm, while between 2 and 2.5 is considered dilatation. CAAs can presents in the form of absence of tapering of coronary arteries, coronary artery ectasia, dilation and aneurysms. Other than CAAs these patients can have myocardial dysfunction (reduced ejection fraction, fractional shortening), valvular regurgitation, pericardial effusion and aortic root dilation [44]. It is recommended to perform frequent 2DE examinations during acute phase of KD. After discharge, 2DE should be done 2 weeks and then 4–6 weeks later. It should be noted that normal 2DE examination in first 7 days of illness does not exclude development of CAAs . More frequent 2DE assessment should be carried out in children with KD having >2 Z score coronary artery diameters [28].
4.11 Interpretation of 2DE Examination: A Word of Caution
-
1.
Assessment of Z scores on 2DE is operator dependent and inter-individual variations are not uncommon. This can influence both acute and long-term management.
-
2.
During the first 5–7 days of illness, CAAs are usually not seen. A normal 2DE during this period may be mistakenly interpreted as having excluded coronary involvement.
-
3.
While normative data are available only for proximal segment of coronary arteries, there is paucity of literature on data for middle and distal segments of coronary arteries. Isolated involvement of distal segments of coronary arteries is uncommon but has been described [56].
-
4.
It has been suggested that an aneurysm may be better defined as a dilatation that is 1.5 times or more than an adjacent segment. This circumvents the problems associated with Z scores.
-
5.
Detailed and better evaluation of coronary arteries requires multiple transducer positions, imaging in multiple planes and high frequency transducers. Coronary artery diameters refer to the maximal internal luminal diameter. Measurements should not be taken at branching points.
-
6.
Limitations of 2DE include difficulty in visualization of distal coronaries, frequent non-visualization of left circumflex coronary artery, difficulty in commenting on stenosis or thrombosis and limited field of vision in older children because of thick chest walls. Another problem is due to artifacts especially while scanning the right coronary artery or left circumflex coronary artery.
-
7.
Several nomograms on Z scores are available and there may be variations in the measurements. Body surface area calculations have to be carried out meticulously and there is no consensus on the ideal method. It cannot be over-emphasized that a trivial difference in measurement of weight and height (especially in infants and young children) can significantly impact the calculations of Z scores.
-
8.
There are no normative data for “Z” scores for left circumflex coronary artery.
4.12 Coronary CT Angiography (CTCA)
Although 2DE has hitherto been considered the imaging modality of choice for coronary artery evaluation, CTCA is now increasingly being performed for better delineations of coronary arteries. CTCA is a useful modality for better characterization and delineation of coronary arteries dilatations, ectasia and aneurysms especially in the mid- and distal segments. It also provides precise details of aneurysm size, morphology, and thrombus. In the last decade, due to advancements in CT technology and the development of dual-source CT scanners (DSCT), it is now possible to obtain high resolution motion-free images at acceptable radiation dose. In the convalescent phase, CTCA can be used for delineation of complications such as intra-aneurysmal thrombus, segmental stenosis, and mural calcifications [57].
4.13 Management
4.13.1 Acute Management
Main aim of therapy in KD is halting of acute phase inflammation and arterial damage. Management includes use of IVIg , aspirin with or without anticoagulant therapy.
4.13.2 Intravenous Immunoglobulin (IVIg)
IVIg is the standard of care for the patients with KD. It should ideally be administered in first 10 days of illness. In the acute stage, IVIg (2 g/kg) is given over 10–12 h as a single infusion along with oral aspirin [3, 28]. If diagnosis is made after 10 days, IVIg should still be given if fever is persistent, inflammatory parameters are raised or if CAAs are present. Administration of IVIg during acute stage has reduced the rate of coronary artery complications to less than 5%. Approximately 1–3% patients with KD can have recurrences [58].
4.13.3 Aspirin and Anticoagulation Therapy
Aspirin has anti-inflammatory and antiplatelet activity depending on the dose being used. It remains an essential component of management in KD. However, effect of aspirin on development of CAAs is inconclusive. During the acute phase of illness, aspirin should be administered at high (50–100 mg/kg/day) or moderate (30–50 mg/kg/day) doses 6–8 hourly [59, 60]. Anti-inflammatory dose of aspirin is usually continued until 48–72 h after the patient becomes afebrile. After discontinuation of anti-inflammatory dose of aspirin, low-dose aspirin (3–5 mg/kg/day) is started and continued for 6–8 weeks. At this time if there are no CAAs on 2DE, aspirin can be discontinued. For children who develop CAAs , aspirin may need to be given indefinitely [28].
Complications related to CAAs during the acute phase of KD include thrombotic occlusion of a coronary artery aneurysm and rarely coronary artery rupture leading to sudden cardiac death. Coronary artery thrombosis in patients with KD is contributed by acute inflammation, high platelet counts, endothelial dysfunction and stasis of blood flow due to abnormal dilatation. In patients with CAAs assessment with 2DE is mandatory to monitor size of aneurysm and presence of thrombus. Patients with large coronary artery aneurysms are at high risk of myocardial infarction especially in the first year after illness. They continue to be at increased life-time risk of developing coronary artery events [28]. Risk stratification of coronary artery aneurysm should take into account both current and maximal Z score. Along with a Z score classification the shape, location, number of aneurysms and coronary artery wall abnormalities should also be considered for prognostication and risk stratification [61].
In patients with small aneurysms, low-dose aspirin is adequate for thromboprophylaxis. However, treating physicians can consider addition of another antiplatelet agent (e.g., clopidogrel) in patients with moderate size aneurysms. Patients having large or giant aneurysms are at very high risk for coronary artery complications including thrombosis and rupture. These patients should be treated with a combination of antiplatelet and therapeutic anticoagulation therapy. This includes low-dose aspirin along with either low-molecular-weight heparin (LMWH) or oral warfarin. LMWH should be given as 1 mg/kg/dose subcutaneously every 12 h. LMWH may be preferred to warfarin in acute phase because of added effects of anti-inflammatory and remodeling action. Transition from LMWH to oral warfarin may be considered in situations where the aneurysm has stopped progressing [28].
4.14 Resistant KD
Majority of patients will respond to first dose of IVIg with rapid defervescence of fever and improvement in general well-being. However, approximately 10–20% of patients with KD may go on to develop recrudescent or persistent fever. Children who have axillary temperature ≥38.0 °C at 36 h after completion of therapy are said to have resistant or refractory KD [28]. There are multiple factors that have been associated with development of IVIg resistance. These include severity of disease and host genetic factors (e.g., polymorphisms in the Fcγ receptors). Patients having refractory KD are at increased risk of developing CAAs . Various scoring systems have been developed in Japan to predict IVIg resistance, but the validity of these scores in other countries remains a contentious issue.
4.14.1 Treatment Options for Resistant KD
There are no clear guidelines on management of patients with refractory KD [62]. The AHA guidelines recommended use of a repeat dose of IVIg (2 g/kg) in these patients. Alternatively, the guidelines emphasize the role of intravenous pulse methylprednisolone (30 mg/kg/day, three doses) with tapering oral prednisolone. Administration of tapering course of prednisolone for 2–3 weeks with second dose of IVIg (2 g/kg) may also be considered in the retreatment of refractory KD patients. Infliximab (TNF-α blocker), given as a single dose (5–10 mg/kg) intravenously, is also an important choice in treatment of refractory KD and appears to decrease the chances of developing CAAs [28]. Use of infliximab is associated with prompt reduction of fever. At our centre we prefer to use infliximab as second line therapy [63]. Cyclosporine may also be considered as an option in these circumstances. In highly refractory cases, plasma exchange, cytotoxic agents, or other biologicals have been used [28]. There are a few recent reports of successful use of the IL-1 receptor antagonist, anakinra, for the treatment of highly refractory KD [64].
4.15 Long-Term Management
Long-term follow-up and management of patients with KD is based on risk stratification. Children with large CAAs may need lifelong follow-up. Long-term management includes counselling about a healthy lifestyle with balanced diet and exercise to avoid obesity and hypertension. Because these patients have already developed a cardiac risk factor (even if there are no obvious CAAs during acute stage), a second risk factor like obesity, hyperlipidemia, or hypertension must be avoided [28]. Uses of statins have also been advocated in these situations. Patients having large and giant aneurysms should undergo frequent 2DE examinations for monitoring of size and associated complications. These patients may also require CTCA at periodic (every 3–5 years) intervals [56].
4.16 Consequences of KD in Adulthood
Children with missed and untreated KD can have significant clinical consequences later in life. Even though coronary arteries with remodeled aneurysms may become anatomically normal, they continue to remain functionally abnormal. An increasing number of young adults are presenting to cardiologists with myocardial ischemia and infarction—it is not often realized that these could well be late manifestations of KD that has been missed in childhood. These consequences of KD in adulthood are grossly under recognized [65]. There is very little awareness amongst adult cardiologists regarding cardiovascular sequelae of KD and their management. Clearly there is a need for an improved evidence base to guide the care and management of adults with coronary artery damage following KD in childhood. Whenever a young adult is presenting with myocardial ischemia and there is marked ectasia or proximal coronary artery involvement, possibility of untreated KD in past should be entertained [66].
4.17 AHA 2017 Guidelines: The Debate Continues
The AHA has published an update on criteria for diagnosis of KD in 2017. While the presence of fever remains an essential criterion and there is no change in the five principal clinical manifestations of the disease, the scientific committee has suggested several amendments. The new guidelines emphasize that some clinical features of KD may subside by the time the patient reaches a clinician. In such situations the clinical findings that have disappeared can also be taken into account for fulfilment of criteria. Similarly, the issue of diagnosis in young infants has been addressed at length. The guidelines mention that any infant with unexplained fever lasting for a week or more should be evaluated for underlying KD. This cannot be overemphasized.
In the 2017 guidelines, the terms incomplete KD and atypical KD have been used interchangeably. However, these are distinct clinical entities and this fact needs to be kept in mind while evaluating a patient. Desquamating groin rash has been included as one of the other clinical findings. It is known that erythema or desquamation of perineal/perianal region occurs earlier than classic periungual peeling and thus may facilitate early consideration of the diagnosis.
The AHA 2017 guidelines emphasize on the use of Z score for assessment of coronary artery size. However, the difficulties involved in calculation of an accurate ‘Z’ score that is reproducible across centres have not been detailed at length.
4.18 Difference Between Japanese Ministry of Health and AHA Guidelines [28, 29, 54]
-
1.
In the Japanese criteria fever is not taken as an essential prerequisite for diagnosis. In other words, a diagnosis of KD can be offered even in absence of fever while using the Japanese criteria.
-
2.
Definition of coronary artery lesion in Japanese Ministry of Health guidelines is based on absolute dimensions, while AHA 2017 guidelines have classified the CAAs on basis of “Z” scores (Table 4.4).
-
3.
Refractory KD has been defined as persistence of fever more than 36 h despite treatment as per AHA guidelines. However, the cut-off for duration of fever is 24 h in Japanese guidelines.
References
Newburger JW, Takahashi M, Burns JC. Kawasaki disease. J Am Coll Cardiol. 2016;67:1738–49.
Singh S, Jindal AK, Pilania RK. Diagnosis of Kawasaki disease. Int J Rheum Dis. 2018;21:36–44.
Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110:2747–71.
Kawasaki T. Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children. Arerugi. 1967;16:178–222.
Uehara R, Belay ED. Epidemiology of Kawasaki disease in Asia, Europe, and the United States. J Epidemiol. 2012;22:79–85.
Nakamura Y. Kawasaki disease: epidemiology and the lessons from it. Int J Rheum Dis. 2018;21:16–9.
Singh S, Vignesh P, Burgner D. The epidemiology of Kawasaki disease: a global update. Arch Dis Child. 2015;100:1084–8.
Makino N, Nakamura Y, Yashiro M, Sano T, Ae R, Kosami K, Kojo T, Aoyama Y, Kotani K, Yanagawa H. Epidemiological observations of Kawasaki disease in Japan, 2013–2014. Pediatr Int. 2018;60:581–7.
Nakamura Y, Yashiro M, Yamashita M, et al. Cumulative incidence of Kawasaki disease in Japan. Pediatr Int. 2018;60:19–22.
Kim GB, Park S, Eun LY, Han JW, Lee SY, Yoon KL, Yu JJ, Choi J-W, Lee K-Y. Epidemiology and clinical features of Kawasaki disease in South Korea, 2012–2014. Pediatr Infect Dis J. 2017;36:482–5.
Lin M-T, Wu M-H. The global epidemiology of Kawasaki disease: review and future perspectives. Glob Cardiol Sci Pract. 2017;2017:e201720.
Chen J-J, Ma X-J, Liu F, Yan W-L, Huang M-R, Huang M, Huang G-Y, Shanghai Kawasaki Disease Research Group. Epidemiologic features of Kawasaki disease in Shanghai from 2008 through 2012. Pediatr Infect Dis J. 2016;35:7–12.
Zhang X, Zhang Z, Liu S, Sun J. Epidemiologic survey of Kawasaki disease in Jilin from 1999 through 2008. Pediatr Cardiol. 2012;33:272–9.
Tang Y, Gao X, Shen J, Sun L, Yan W. Epidemiological and clinical characteristics of Kawasaki disease and factors associated with coronary artery abnormalities in East China: nine years experience. J Trop Pediatr. 2016;62:86–93.
Du Z-D, Zhao D, Du J, Zhang Y-L, Lin Y, Liu C, Zhang T, Beijing Kawasaki Research Group. Epidemiologic study on Kawasaki disease in Beijing from 2000 through 2004. Pediatr Infect Dis J. 2007;26:449–51.
Singh S, Aulakh R, Bhalla AK, Suri D, Manojkumar R, Narula N, Burns JC. Is Kawasaki disease incidence rising in Chandigarh, North India? Arch Dis Child. 2011;96:137–40.
Makino N, Nakamura Y, Yashiro M, Ae R, Tsuboi S, Aoyama Y, Kojo T, Uehara R, Kotani K, Yanagawa H. Descriptive epidemiology of Kawasaki disease in Japan, 2011–2012: from the results of the 22nd nationwide survey. J Epidemiol. 2015;25:239–45.
Onouchi Y. Genetics of Kawasaki disease: what we know and don’t know. Circ J. 2012;76:1581–6.
Onouchi Y. The genetics of Kawasaki disease. Int J Rheum Dis. 2018;21:26–30.
Dietz SM, van Stijn D, Burgner D, Levin M, Kuipers IM, Hutten BA, Kuijpers TW. Dissecting Kawasaki disease: a state-of-the-art review. Eur J Pediatr. 2017;176:995–1009.
Onouchi Y, Fukazawa R, Yamamura K, et al. Variations in ORAI1 gene associated with Kawasaki disease. PLoS One. 2016;11:e0145486.
Shimizu C, Jain S, Davila S, et al. Transforming growth factor-beta signaling pathway in patients with Kawasaki disease. Circ Cardiovasc Genet. 2011;4:16–25.
Rowley AH. Is Kawasaki disease an infectious disorder? Int J Rheum Dis. 2018;21:20–5.
Orenstein JM, Shulman ST, Fox LM, et al. Three linked vasculopathic processes characterize Kawasaki disease: a light and transmission electron microscopic study. PLoS One. 2012;7:e38998.
Takahashi K, Oharaseki T, Yokouchi Y. Histopathological aspects of cardiovascular lesions in Kawasaki disease. Int J Rheum Dis. 2018;21:31–5.
Kao AS, Getis A, Brodine S, Burns JC. Spatial and temporal clustering of Kawasaki syndrome cases. Pediatr Infect Dis J. 2008;27:981–5.
Matsubara K, Fukaya T. The role of superantigens of group A Streptococcus and Staphylococcus aureus in Kawasaki disease. Curr Opin Infect Dis. 2007;20:298–303.
McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135:e927–99.
Ayusawa M, Sonobe T, Uemura S, Ogawa S, Nakamura Y, Kiyosawa N, Ishii M, Harada K, Kawasaki Disease Research Committee. Revision of diagnostic guidelines for Kawasaki disease (the 5th revised edition). Pediatr Int. 2005;47:232–4.
Singh S, Agarwal S, Bhattad S, Gupta A, Suri D, Rawat A, Singhal M, Rohit M. Kawasaki disease in infants below 6 months: a clinical conundrum? Int J Rheum Dis. 2016;19:924–8.
Gong GWK, McCrindle BW, Ching JC, Yeung RSM. Arthritis presenting during the acute phase of Kawasaki disease. J Pediatr. 2006;148:800–5.
Kumar A, Singh S. BCG site reactivation in Kawasaki disease. Arthritis Rheumatol. 2016;68:2026.
Pilania RK, Bhattarai D, Singh S. Controversies in diagnosis and management of Kawasaki disease. World J Clin Pediatr. 2018;7:27–35.
Chuang G-T, Tsai I-J, Lin M-T, Chang L-Y. Acute kidney injury in patients with Kawasaki disease. Pediatr Res. 2016;80:224. https://doi.org/10.1038/pr.2016.81.
Singh S, Gupta A, Jindal AK, Gupta A, Suri D, Rawat A, Vaidya PC, Singh M. Pulmonary presentation of Kawasaki disease-a diagnostic challenge. Pediatr Pulmonol. 2017;53:103. https://doi.org/10.1002/ppul.23885.
Madhusudan S, Singh S, Suri D, Gupta A, Gupta A. Acute anterior uveitis as the presenting feature of Kawasaki disease. Indian J Pediatr. 2014;81:415.
Burgner D, Curtis N. Kawasaki disease as a cause of encephalitis. Arch Dis Child. 2011;96:988–9.
Eladawy M, Dominguez SR, Anderson MS, Glodé MP. Kawasaki disease and the pediatric gastroenterologist: a diagnostic challenge. J Pediatr Gastroenterol Nutr. 2013;56:297–9.
Watanabe T. Pyuria in patients with Kawasaki disease. World J Clin Pediatr. 2015;4:25–9.
Salgado AP, Ashouri N, Berry EK, Sun X, Jain S, Burns JC, Tremoulet AH. High risk of coronary artery aneurysms in infants younger than 6 months of age with Kawasaki disease. J Pediatr. 2017;185:112–116.e1.
Singh S, Bhattad S, Gupta A, Suri D, Rawat A, Rohit M. Mortality in children with Kawasaki disease: 20 years of experience from a tertiary care centre in North India. Clin Exp Rheumatol. 2016;34:S129–33.
Stockheim JA, Innocentini N, Shulman ST. Kawasaki disease in older children and adolescents. J Pediatr. 2000;137:250–2.
Altman CA. Clinical assessment of coronary arteries in Kawasaki disease: focus on echocardiographic assessment. Congenit Heart Dis. 2017;12:636–40.
Dahdah N. Not just coronary arteritis, Kawasaki disease is a myocarditis, too. J Am Coll Cardiol. 2010;55:1507; author reply 1507–1508.
Dionne A, Dahdah N. Myocarditis and Kawasaki disease. Int J Rheum Dis. 2018;21:45–9.
Lin Y-J, Cheng M-C, Lo M-H, Chien S-J. Early differentiation of Kawasaki disease shock syndrome and toxic shock syndrome in a pediatric intensive care unit. Pediatr Infect Dis J. 2015;34:1163–7.
Dominguez SR, Friedman K, Seewald R, Anderson MS, Willis L, Glodé MP. Kawasaki disease in a pediatric intensive care unit: a case-control study. Pediatrics. 2008;122:e786–90.
Rodo X, Curcoll R, Robinson M, et al. Tropospheric winds from northeastern China carry the etiologic agent of Kawasaki disease from its source to Japan. Proc Natl Acad Sci U S A. 2014;111:7952–7.
Kushner HI, Macnee RP, Burns JC. Kawasaki disease in India: increasing awareness or increased incidence? Perspect Biol Med. 2009;52:17–29.
Rawat A, Singh S. Biomarkers for diagnosis of Kawasaki disease. Indian Pediatr. 2015;52:473–4.
Jiang J, Cai Y, Li Z, et al. Screening of differentially expressed genes associated with Kawasaki disease by microarray analysis. Exp Ther Med. 2017;14:3159–64.
Reddy M, Singh S, Rawat A, Sharma A, Suri D, Rohit MK. Pro-brain natriuretic peptide (ProBNP) levels in North Indian children with Kawasaki disease. Rheumatol Int. 2016;36:551–9.
Lin K-H, Chang S-S, Yu C-W, Lin S-C, Liu S-C, Chao H-Y, Lee M-TG, Wu J-Y, Lee C-C. Usefulness of natriuretic peptide for the diagnosis of Kawasaki disease: a systematic review and meta-analysis. BMJ Open. 2015;5:e006703.
JCS Joint Working Group. Guidelines for diagnosis and management of cardiovascular sequelae in Kawasaki disease (JCS 2013). Digest version. Circ J. 2014;78:2521–62.
Manlhiot C, Millar K, Golding F, McCrindle BW. Improved classification of coronary artery abnormalities based only on coronary artery z-scores after Kawasaki disease. Pediatr Cardiol. 2010;31:242–9.
Singhal M, Singh S, Gupta P, Sharma A, Khandelwal N, Burns JC. Computed tomography coronary angiography for evaluation of children with Kawasaki disease. Curr Probl Diagn Radiol. 2018;47:238–44.
Singhal M, Singh S, Gupta P, Khandelwal N, Burns JC. Computed tomography coronary angiography for evaluation of children with Kawasaki disease. Curr Probl Diagn Radiol. 2018;47(4):238–44.
Maddox RA, Holman RC, Uehara R, Callinan LS, Guest JL, Schonberger LB, Nakamura Y, Yashiro M, Belay ED. Recurrent Kawasaki disease: USA and Japan. Pediatr Int. 2015;57:1116–20.
Dallaire F, Fortier-Morissette Z, Blais S, et al. Aspirin dose and prevention of coronary abnormalities in Kawasaki disease. Pediatrics. 2017;139:e20170098. https://doi.org/10.1542/peds.2017-0098.
Ho LGY, Curtis N. What dose of aspirin should be used in the initial treatment of Kawasaki disease? Arch Dis Child. 2017;102:1180.1. https://doi.org/10.1136/archdischild-2017-313538.
McCrindle BW, Cifra B. The role of echocardiography in Kawasaki disease. Int J Rheum Dis. 2018;21:50–5.
Tremoulet AH. Adjunctive therapies in Kawasaki disease. Int J Rheum Dis. 2017;21:76. https://doi.org/10.1111/1756-185X.13208.
Singh S, Sharma D, Suri D, Gupta A, Rawat A, Rohit MK. Infliximab is the new kid on the block in Kawasaki disease: a single-centre study over 8 years from North India. Clin Exp Rheumatol. 2016;34:S134–8.
Kone-Paut I, Cimaz R, Herberg J, Bates O, Carbasse A, Saulnier JP, Maggio MC, Anton J, Piram M. The use of interleukin 1 receptor antagonist (anakinra) in Kawasaki disease: a retrospective cases series. Autoimmun Rev. 2018;17:768. https://doi.org/10.1016/j.autrev.2018.01.024.
Vijayvergiya R, Bhattad S, Varma S, Singhal M, Gordon J, Singh S. Presentation of missed childhood Kawasaki disease in adults: experience from a tertiary care center in North India. Int J Rheum Dis. 2017;20:1023–7.
Gordon JB, Burns JC. Management of sequelae of Kawasaki disease in adults. Glob Cardiol Sci Pract. 2017;2017:e201731.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Pilania, R.K., Singh, S. (2020). Kawasaki Disease. In: Cimaz, R. (eds) Periodic and Non-Periodic Fevers. Rare Diseases of the Immune System. Springer, Cham. https://doi.org/10.1007/978-3-030-19055-2_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-19055-2_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-19054-5
Online ISBN: 978-3-030-19055-2
eBook Packages: MedicineMedicine (R0)