
Abstract
Hepatitis C is a global public health problem. Globally, an estimated 170 million persons (3 % of the world’s population) have been infected with the hepatitis C virus, and an estimated 350,000 persons die annually from complications of chronic hepatitis C. Furthermore, an increasing trend in hepatitis C mortality in the USA was observed over the last decade; in 2007, mortality associated with hepatitis C surpassed mortality associated with HIV. As the hepatitis C epidemic continues, it is increasingly important to accurately measure hepatitis C-related morbidity and mortality in order to inform public health programs and policies and prioritize and evaluate prevention efforts. This chapter provides an overview of hepatitis C surveillance and methods used in the USA with some examples from other countries.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Hepatitis C virus infection
- Hepatitis C surveillance
- Hepatitis C reporting
- Hepatitis C mortality
- Hepatitis C laboratory testing
- Hepatitis C laboratory reporting
- Health information technology
This chapter provides an overview of hepatitis C surveillance methods.
1 Importance and Aims of Hepatitis C Surveillance
Hepatitis C virus (HCV) infection is a common type of chronic blood-borne infection [1]. The World Health Organization estimates that 170 million persons are HCV infected globally [2]. In countries that conduct hepatitis C surveillance, hepatitis C may be required to be reported by laboratories and healthcare providers to health departments.
Hepatitis C surveillance includes acute and chronic hepatitis C cases; however, some countries or local areas may not have the necessary confirmatory laboratory tests to distinguish current (or present) from resolved (or past) HCV infection. Additionally, because the chronic hepatitis C burden is large and conducting follow-up investigation can be labor intensive, some countries and local areas might lack the capacity to investigate and confirm cases. Despite the challenges of conducting hepatitis C surveillance, there is hope for hepatitis C eradication because primary prevention is effective, and secondary transmission and complications are preventable through case management, new effective treatments, and alcohol counseling. Surveillance data are essential to the planning, implementation, and evaluation of public health programs and policies [3].
2 Epidemiology
2.1 Characteristics
Hepatitis C traces back to the mid-1970s, though at the time, the virus was broadly termed “non-A, non-B hepatitis” when serologic tests ruled out hepatitis A or B as the cause of acute hepatitis following a blood transfusion [4]. In 1989, hepatitis C was fully distinguished from non-A, non-B hepatitis [4, 5].
HCV infection may be difficult to measure because 70–85 % of HCV-infected persons are asymptomatic. When symptoms are present, they can include jaundice, fever, abdominal pain or discomfort, nausea, vomiting, dark urine, fatigue, joint pain, loss of appetite, and clay-colored stools [6]. For symptomatic HCV-infected individuals, the onset of symptoms usually occurs 6–7 weeks after exposure [7, 8]. For asymptomatic HCV-infected individuals, diagnosis usually occurs incidentally during blood donation screenings and other medical screenings. In the USA, federally supported surveillance captures only a fraction of all acute HCV infections because the identification of acute HCV infection requires the presence of symptoms [9], and the proportion of those with symptoms is relatively small (20–30 %) [6]. However, procedures have been developed that account for asymptomatic HCV infections in estimating the total number of reported acute cases (estimation procedures are discussed in Sect. 5.5). Table 6.1 describes the general characteristics of acute and chronic HCV infection.
2.2 Geographic Distribution
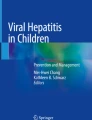
Although the overall estimated global prevalence of past/present HCV infection is high (3 %; 170 million persons) [2], there is wide variability in prevalence between geographic regions [10]. Typically, developing countries, such as parts of Africa and Asia, have the highest reported prevalence of >3.5 % (Fig. 6.1). In Egypt, for example, 15 % of persons aged 15–59 years had evidence of past/present HCV infection [11]. In comparison, more developed countries, such as those in North America, northern and western Europe, and Australia, have a low to moderate reported prevalence (<3.5 %) (Fig. 6.1). In the USA, for example, the estimated prevalence of HCV infection is approximately 1.0 %, or 2.7 million persons [12]—disproportionately affecting persons who are middle aged [1, 12, 13]. Hepatitis C has at least six distinct genotypes widely distributed across the globe. In the USA, Europe, and Japan, genotypes 1a and 1b are most predominant although genotypes 2a and 2b are also common [14]. Genotype 2c is prevalent in northern Italy while genotype 3a is prevalent among intravenous drug users in Europe and the USA [14]. In North Africa and the Middle East, genotype 4 is predominant while genotypes 5 and 6 are confined to South Africa and Hong Kong [14].

Seroprevalence of hepatitis C antibody by global burden of disease region, 2005. Adapted from Mohd HK, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology. 2013; 57(4):1333–42. Permission to use this figure was obtained from Hepatology
2.3 Mode of Transmission
HCV is primarily transmitted through percutaneous exposure to infected blood [15]. One of the most common ways by which HCV is transmitted is injection drug use (IDU) [1, 2]. In the USA, among persons with acute hepatitis C who responded to questions about IDU, approximately 60 % reported injection of street drugs [16]. From 2007 to 2011, US surveillance data detected a 44 % increase in the hepatitis C incidence [16], which may be due to a rise in injection drug users among young persons [17–19].
In healthcare settings where standard precautions and infection control measures are less strictly implemented, needle stick injuries and unsafe medical practices are common causes of HCV transmission. In developed countries like the USA, the risk of HCV transmission in healthcare settings has dramatically declined due to the implementation of safe injection and universal infection control practices [20]. Despite the decline, from 2008 to 2012, 16 healthcare-associated hepatitis C outbreaks that resulted in 160 cases of HCV infection were reported to the United States Centers for Disease Control and Prevention (CDC) [21]. Healthcare-associated hepatitis C outbreaks are indicators of failure to implement and strictly adhere to standard precautions and infection control measures. Since the development of the hepatitis C antibody screening test in 1990 and screening of the blood supply for hepatitis C in 1992, HCV transmission from blood transfusions has been greatly reduced in developed countries [22]. In developing countries, this mode of transmission remains significant [22, 23].
HCV also can be transmitted from HIV-coinfected mothers to their infants, and HIV-infected men who have sex with men (MSM) have an increased likelihood of acquiring HCV infection [24]. The risk of HCV transmission among HIV-infected MSM is also increased in the presence of genital ulcerative disease and sexual practices that lead to mucosal trauma [25]. Heterosexual contact among monogamous partners is an unlikely route of transmission [24].
Other demographic groups also are disproportionately affected by hepatitis C, evident by a higher prevalence among those groups. For example, in the USA, the overall hepatitis C antibody prevalence is estimated to be 1.6 %; however, it is 3 % among persons born during 1945–1965 [13]; 5 % among military veterans [26, 27]; 6 % among blacks aged 30–49 years [28]; 14 % among HIV-infected persons [1]; and 23–39 % among the incarcerated [26]. Additionally, some hepatitis C epidemics are fueled by contaminated injection equipment used in mass treatment campaigns, such as schistosomiasis treatment in Egypt during 1960–1980; HCV transmission is still ongoing today [29].
2.4 Complications of Chronic Infection
The burden of hepatitis C, mostly among persons who are undiagnosed and not in care, is evidenced by increasing complications. One such complication is the development and progression of chronic liver disease (CLD). In addition, alcohol use is independently associated with liver disease progression [13]. Based on representative samples of published reports from at least 1990 and 11 World Health Organization regions, hepatitis C was identified as one of the most common etiologies of CLD throughout most of the world [30] and was associated with 27 % of liver cirrhosis and 25 % of hepatocellular carcinoma (HCC) [30]. From the same study, death due to HCV infection was identified in approximately 211,000 persons with liver cirrhosis and 155,000 persons with liver cancer [30]. Among US adult residents in two sentinel surveillance sites and one healthcare network site, 64 % of newly diagnosed CLD had underlying hepatitis C during 1999–2001 [31]. In the USA, over 15,000 hepatitis C-related deaths occurred in 2007, of which 57 % had CLD, including HCC [32].
Although hepatitis C is widely known to increase the risk of dying from liver-related diseases, recent studies have found that HCV infection also increased the risk of dying from non-liver-related diseases [33–35]. In one study, patients with chronic HCV infection had a non-liver-related mortality risk nearly two times higher than uninfected patients [33]. Similarly, in another study, persons who were HCV antibody positive had significantly higher mortality than persons who were HCV antibody negative. Additionally, persons with detectable HCV RNA levels had significantly higher mortality than persons with undetectable RNA levels [34].
2.5 Laboratory Testing
The traditional approach for detecting HCV infection is to screen persons for a history of risk factors and to test those with any identifiable risk factor [36]. While IDU is the most common mode of transmission in developed countries, additional risk factors, including exposure to unsafe blood products and injection practices, are highly prevalent and contribute to significant HCV transmission in developing countries [37]. There are many international recommendations for hepatitis C testing and all have consistency in their recommendation for testing of persons who inject illicit drugs, prior recipients of transfusions or organ transplants, persons with persistently elevated liver enzymes, children born to HCV-infected mothers, and persons exposed to HCV-positive blood in healthcare [38].
Table 6.2 describes the interpretation of hepatitis C test results and corresponding further actions. The initial test is for HCV antibodies, which are detectable approximately 4–10 weeks after exposure [39]. In symptomatic cases, this time period usually occurs at or before the onset of clinical symptoms. The HCV antibody test is positive in acute, chronic, and resolved infections (Table 6.2). Consequently, HCV antibody tests do not have the capacity to distinguish current infection from past, resolved infection [40]. In addition to standard serologic assays, there are also rapid tests to detect HCV antibodies [41]. The availability of standard and rapid assays varies significantly and is dependent on availability of resources [40]. Over the past decade, new generations of standard tests with high sensitivity and specificity have been developed [40, 42]. However, the proportion of false-positive HCV antibody results is inversely related to the HCV prevalence in that setting [40, 43]. False-negative HCV antibody results also occur, particularly in individuals with severe immunodeficiency [39, 44], but rarely among the general population.
In contrast to HCV antibodies, HCV RNA can detect current infection and is detectable in serum as early as 1–2 weeks after exposure [41]. There are a number of qualitative and quantitative HCV RNA assays [43]. However, these tests are expensive and not widely available. Further, because these tests detect HCV RNA, they are important for differentiating current infection from past, resolved infection [45]. Therefore, both in the clinical practice and in epidemiologic studies, it is important to follow up on every HCV antibody-positive result with an RNA assay [43]. In conditions where the HCV antibody test is likely a false negative, RNA testing may provide the correct diagnosis [43]. For these reasons, quantitative HCV RNA assays and genotype studies are important in the clinical management of chronic HCV infection.
Other tests available for hepatitis C detection and diagnosis include the HCV core antigen test [46] and core antigen/antibody tests [47]. These tests are available only in some countries. While the HCV core antigen test is sensitive, will yield results early in the course of infection, and detects active infection [46, 48], the HCV core antigen/antibody test is positive in the presence of either one or both antigen and antibody [47] making it difficult to differentiate between active and resolved infection. Blood donations are screened by testing for HCV RNA and core antigen [49].
Dried blood spot assays are well developed and validated for HIV detection [50]. HCV antibody and RNA testing on a dried blood spot sample are used in research activities whereby a blood draw is not feasible [51, 52]. However, these tests are not well validated and require highly qualified personnel. Therefore, its use is restricted to research use only.
In many sub-Saharan African countries, a high rate of false-positive HCV antibody test results have been reported, even when the latest generation of serologic assays are used [53]. In the majority of HCV antibody-positive samples, the recombinant immunoblot assay (RIBA) yields either a negative or indeterminate result [53]. RIBA is a more specific blood test for detecting HCV antibodies and is sometimes used as a confirmatory test to less specific antibody tests [43]. In the USA, RIBA was phased out in 2013 [41]. Even among RIBA-confirmed HCV antibody-positive samples, the large majority are HCV RNA negative. Such findings have been a challenge for clinical diagnosis, epidemiological studies, and screening of blood products for transfusion. While the cause of the high false positivity is still unknown [54], it raises questions about the best strategy to test for HCV infection in some countries.
2.6 Treatment
The goal of treatment for chronic HCV infection is to achieve sustained virologic response (SVR), or cure, currently defined as having an undetectable viral load 24 weeks after the end of treatment [55]. Achieving SVR, in turn, is associated with long-term clearance of the virus and reduced long-term health complications such as cirrhosis, HCC, liver failure, and all-cause mortality [56, 57]. Novel therapies with direct-acting antivirals have demonstrated high virus eradication rates. Persons diagnosed as HCV positive should be medically evaluated and entered into routine care, as appropriate. The evaluation should include confirmation of chronic infection by viral testing including genotype and viral load, an assessment of liver function, stage of liver fibrosis, evidence of liver cancer, and eligibility for treatment [58].
The traditional treatment is pegylated interferon with ribavirin [7]. The duration of treatment is determined by the virologic response, which in turn is associated with the person’s genotype. With pegylated interferon and ribavirin therapy, a 24-week treatment course is recommended for genotypes 2 and 3 and a 48-week treatment course for other genotypes [7]. Persons with genotypes 2 and 3 who followed this regimen have ≥80 % SVR rate compared with a 40–50 % SVR rate for persons with genotype 1 [7].
Pegylated interferon and ribavirin is associated with many side effects, requires frequent injections, and has shown low success rates with hepatitis C genotype 1 [59]. In 2011, the United States (US) Food and Drug Administration approved the use of two new protease inhibitors, boceprevir and telaprevir, for the treatment of hepatitis C genotype 1 [7, 59]—the most common genotype reported in the USA. When used in combination with pegylated interferon and ribavirin, boceprevir and telaprevir demonstrated SVR rates of 63–66 % and 69–75 %, respectively [7], a marked increase from traditional standard of care therapy alone.
In November and December 2013, the US Food and Drug Administration approved the use of two new drugs for the treatment of chronic HCV infection, simeprevir and sofosbuvir. These drugs are approved for use in HCV-infected patients with genotypes 1 and 4, which showed >90 % SVR rates in clinical trials [60]. Although treatment is very costly, these are among the new drugs that offer promising hope towards the global eradication of hepatitis C. As new therapies continue to be developed, evidence-based hepatitis C management recommendations are continuously updated to address issues ranging from testing and linkage to care to the optimal treatment regimen in specific patient situations [36].
3 Assessment of Priorities
The success of a surveillance system for hepatitis C is dependent on the dedicated resources and established priorities for the surveillance system. For example, if the priority is to measure the overall burden of disease, the design of the system might be to conduct a seroprevalence survey. However, if the objective is to obtain data for case management and evaluation of local area prevention programs, then individual cases should be monitored and records updated over time [61]. Furthermore, the population for which information is needed is an important determinant of surveillance methods. For example, in an enhanced surveillance pilot study in select neighborhoods in England, there were concerns about increases in HCV infection among MSM. Health officials quickly recruited and collected information from certain drug treatment facilities and implemented a surveillance project that provided results that were applied and published in less than a year [62]. In another study, researchers sought to determine which hepatitis C genotypes were circulating among injection drug users in Hungary [63]. They approached needle exchange programs and drug treatment facilities in all health districts and found that HCV strains among injection drug users were very different compared to HCV-infected persons who did not acquire their infections from injecting drugs [63]. The objectives and expected use of the surveillance data also should be tempered with the resources available to conduct the activities.
4 United States Surveillance Methods
4.1 Passive Surveillance
In a population-based passive surveillance system, sources of hepatitis C reports (e.g., hospitals, clinics, laboratories) routinely report cases to health departments [64]. However, in this type of surveillance system, notification may not be timely enough to alert health officials of a potential outbreak. In addition, the data reported are often incomplete because few, if any, incentives are given to the laboratories and healthcare providers to report information [64].
In the USA, as of 2013, acute hepatitis C is reportable in all states and the District of Columbia, and past/present hepatitis C is reportable in 43 states and the District of Columbia. Due to resource constraints, it is oftentimes difficult for health departments to obtain the necessary confirmatory laboratory tests from laboratories or healthcare providers to distinguish current from resolved or past HCV infection. Therefore, these cases are labeled as “past/present hepatitis C.” Under the current national surveillance system, acute and past/present hepatitis C are passively and voluntarily reported on a weekly basis by health departments to a national surveillance network at CDC. The system relies on laboratories and healthcare providers to submit case reports to health departments, as mandated by states. Health departments process case reports to determine that they represent new, unique cases and store data with personal identifiers.
Most laboratory reports and some physician reports are submitted electronically to health departments. However, reporting can be accomplished by fax or telephone, even using toll-free numbers or automated recording devices available at all hours. Time and lack of resources greatly limit such a system to a small percentage of most reportable diseases, but as long as the reporting system and requirements remain unchanged, the changes in incidence may reflect meaningful patterns of disease.
The advantage of a case reporting system is that there is an organized system of reporting and tabulating cases at both the local and national level. Also, at the local level, individuals are identified for intervention. However, case-reporting systems also have a number of disadvantages, including the following: (1) not all cases are reported despite legal requirements, primarily because of the lack of both symptoms and resources; (2) the variability in reporting from one jurisdiction to another; and (3) the lack of hepatitis C laboratory tests that distinguish between acute and chronic HCV infection.
Due to the large volume of past/present hepatitis C case reports and the resource-intensive process of identifying and classifying a case, chronic hepatitis C is grossly underreported in the USA. Current estimates indicate 2.2–3.2 million persons chronically infected with HCV [12].
4.2 Active Surveillance
Active surveillance requires health departments to contact sources of hepatitis C reports at regular intervals and request specific information for case reports [64]. Reporting frequency is monitored and data on epidemiologic features, such as complications of infections, which would not otherwise be collected through passive surveillance, are obtained. In addition, the data are reported in a more timely fashion than in a passive system. However, unlike passive surveillance, active surveillance is expensive and resource intensive.
4.3 Enhanced Surveillance
CDC provides additional funding to support enhanced surveillance programs. These programs conduct follow-up investigation on cases to obtain additional information, including information about risk behaviors and/or exposures. As a result, data are more complete than passive surveillance. These additional data allow the surveillance infrastructure to answer discrete surveillance and research questions. From 1982 through 2006, the Sentinel Counties Study of Acute Viral Hepatitis enrolled all acute viral hepatitis patients in six county/city health departments in the USA [65]. From this project, funded sites collected data about cases of acute viral hepatitis from hospitals, healthcare providers, and other agencies and patient care sources. These data were used to describe the incidence of acute viral hepatitis [66], characterize individual cases, and identify and describe risk behaviors/exposures. From 2005 through 2011, CDC funded seven sites to conduct enhanced viral hepatitis surveillance throughout major US cities and states. Because of additional resources, completeness of reporting significantly improved in the enhanced surveillance sites [67].
4.4 Analysis of Specimens/Supplementary Data Sources
In the USA, there are existing data from other sources to augment hepatitis C surveillance data. For example, cancer registries have information on HCC [68]. Vital statistics generally include information on the number of deaths for which hepatitis C was listed among causes of death and calculating trends in HCV infection as a cause of death relative to other causes is useful [32]. Healthcare administrative data are available electronically and may be a useful source of data as well. Events available from administrative data include diagnosis, procedure codes, and cost information to examine the economic impact of hepatitis C [69].
Currently, CDC uses data from a variety of sources to further understand the burden of chronic HCV infection; characterize persons who receive treatment; describe treatments, results of treatment, and sequelae of disease; and characterize those who die with and as a consequence of hepatitis C:
-
(a)
Vital Statistics: The oldest form of surveillance in the USA is mortality registration. Registration of death, using a death certificate, is legally required in the USA. As a result, virtually all deaths are included in the registries. Cause of death listed on the death certificate is dependent on the presence/absence of a physician or family member who is knowledgeable about the health of the deceased, severity of disease, complexity of the disease, associated illnesses, and whether or not an autopsy or diagnostic laboratory testing was performed.
Death certificates are completed by funeral directors based on information from attending physicians, medical examiners, coroners, and family members. Death certificates are filed in vital statistics offices within each state and the District of Columbia. States share information from death certificates with CDC through the National Vital Statistics System, which then produces public-use mortality files containing death information with cause of death coded in accordance with the International Classification of Disease, Tenth Revision [70]. These data are used to determine the national burden of mortality associated with specific diseases, including viral hepatitis. A recent analyses of these mortality data from 1999 through 2007 indicated that the hepatitis C mortality rate exceeded the HIV mortality rate in 2007 [32].
-
(b)
Surveys: Health surveys are used for a variety of reasons, including augmenting our understanding of viral hepatitis from surveillance. Currently, the CDC uses several national surveys, which may include seroprevalence data, to describe and understand hepatitis C-related prevalence, hospitalizations, treatments, and development of CLD. For example, the National Health and Nutrition Examination Survey (NHANES) has provided valuable seroprevalence data on hepatitis A [71], hepatitis B [72], and hepatitis C [12] that are representative of the US noninstitutionalized civilian population [73]. The National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey use a national sample of visits from nonfederal employed office-based physicians who provide direct patient care and from emergency departments and outpatient department of noninstitutional general and short-stay hospitals, respectively, to obtain information about the use and provision of ambulatory medical care services, including viral hepatitis-related visits [74], in these settings. The National Hospital Discharge Survey was a nationally representative survey conducted from 1965-2010 that provided information from patients of non-federal, short-stay hospitals in the USA about the characteristics of these patients, conditions for which they were treated, cost of treatment, and a number of other public health topics of interest. The National Hospital Care Survey is a new survey which links the inpatient data that was collected by the National Hospital Discharge Survey with the emergency department, outpatient department, and ambulatory surgery center data collected by the National Hospital Ambulatory Medical Care Survey. Together, these population-based surveys provide a wealth of readily available data that are already in electronic format. As a result, they can be relatively inexpensive sources of useful information in addition to that obtained from surveillance.
5 Sequence in Case-Based Surveillance Processes
5.1 Sequential Flow of Case Data for Hepatitis C Surveillance to CDC
CDC uses message mapping guides to standardize the data transmitted for all notifiable diseases monitored by health departments transmitted to the national surveillance network. States report basic demographic, clinical, and risk information on cases of notifiable conditions to the national surveillance network. The CDC Division of Viral Hepatitis retrieves data from servers once a week. These data are used to detect outbreaks, flag cases requiring immediate public health follow-up, and perform data quality checks. Viral hepatitis data are summarized in annual surveillance reports and are made available to the public on the CDC Division of Viral Hepatitis website [75].
5.2 Case Definitions in the USA, Europe, and Australia
Cases of notifiable conditions must meet standard case definitions. In the USA, these case definitions are developed and updated in collaboration with the Council of State and Territorial Epidemiologists and CDC. The 2012 hepatitis C surveillance case definitions require a combination of symptoms and laboratory findings for acute disease and laboratory findings only for past/present hepatitis C [9]. Because the clinical characteristics are the same for acute hepatitis A, B, and C, laboratory testing is needed to identify the specific viral cause of illness. For both acute and past/present hepatitis C cases, laboratory findings include a positive antibody to hepatitis C virus screening test, nucleic acid test for HCV RNA, and genotype testing. A special definition is applied to identify new seroconversions that require only one positive test and a previous negative test within the past 6 months [9].
In 2012, the European Union decided not to require clinical signs/symptoms for a confirmed case. Instead, at least one laboratory finding (RNA, core antigen, or antibody) in a person aged >18 months represents a confirmed case. The definition classifies an acute hepatitis C case as one that has a seroconversion within 12 months or has detected either RNA or core antigen but is antibody negative. A chronic case is defined as two samples positive for RNA or core antigen detected at least 12 months apart [76]. In Australia, case reports supplement other sources of information on HCV infection. A confirmed case in Australia requires laboratory evidence of either an antibody or nucleic acid test (either genotype or RNA) in a person aged at least 24 months, and who does not meet the criteria for a newly acquired case; that is, there is no evidence that the infection was acquired in the 24 months before diagnosis [77].
5.3 Follow-Up Investigation and Case Management
A hepatitis C case report is usually initiated with a positive antibody test, which can indicate either acute or chronic infection. After checking the surveillance database to determine whether the potential case was previously reported and had other epidemiologic or laboratory information, health departments can either attempt follow-up investigation or wait for future laboratory information to be received. Follow-up might require contacting the case patient’s provider to determine whether symptoms of hepatitis were present. Together with information that the case was not previously reported suggests a newly reported acute hepatitis C case. Follow-up with the case patient and/or the healthcare provider is required to obtain additional epidemiologic data. Cases might be divided into groups of interest, such as persons aged <30 years that may indicate IDU [78] or adults aged >65 years that may indicate transmission in healthcare and extended care facilities. Prioritizing groups of interest reduces the number of cases to be investigated, which makes the task more achievable. Basic demographic, clinical, and risk information are collected using a standard case report form (Fig. 6.2). This information is needed to confirm the classification, determine the most likely source of infection, and limit further transmission [79].







Viral hepatitis case report form
5.4 Uses of Surveillance Data in the USA
The uses of surveillance data vary depending on the public health agency’s need for the data. In general, at the national level, surveillance data are used to understand the burden of disease, inform local partners of disease clusters or outbreaks within and across jurisdictions, identify high-risk populations, and inform, prioritize, and evaluate prevention activities. At the local level, surveillance data are used to identify the most likely mode of transmission in the community to limit further transmission, detect and control local outbreaks, improve outreach services, and provide appropriate case management including screening and linking infected persons into care and counseling. Additionally, hepatitis C surveillance data can be matched with other disease registries, such as HIV, in order to integrate medical services for each individual and further understand disease burden. Surveillance data can also be used to evaluate the quality of care, including implementation of hepatitis A and B vaccine recommendations, among HCV-infected patients. Hepatitis A and B vaccine history can be obtained through follow-up investigation of cases and can be used to improve vaccine coverage rates.
5.5 Estimation of Hepatitis C Incidence in the USA
Most HCV infections are not captured through surveillance because many of these infections are asymptomatic. Estimation methodologies are used to account for underreporting of asymptomatic hepatitis C infections. The methodology employed by the CDC to estimate the incidence of HCV infections in the USA was revised in 2011. This methodology uses a simple probability model to estimate all new hepatitis C infections that occur in the USA during a calendar year [80].
Under this model, the estimated number of acute HCV infections in the USA is the number of reported confirmed acute hepatitis C cases multiplied by the joint probability that acute HCV-infected persons who would have developed symptoms, sought healthcare tests, and been reported to health officials [80]. CDC conducted a meta-analysis of peer-reviewed studies to inform the three parameters [80]. However, more sophisticated models informed by representative and comprehensive studies are needed to best estimate acute HCV infections in the USA.
5.6 Security and Confidentiality
While hepatitis C surveillance data can serve many useful public health purposes, these data must be collected, stored, shared, and used in a way that protects the identity of infected individuals [81]. Countries with a well-established hepatitis C surveillance system may have data security and confidentiality policies and procedures in place while countries that are still developing their surveillance system may not. In general, there are guiding principles [82] that can be followed by all countries in order to guarantee security and confidentiality of public health data. These principles are summarized below:
-
Data collection and use policies should respect the rights of individuals and community groups and minimize undue burden.
-
Program officials should be active, responsible stewards of public health data.
-
Programs should:
-
Require that public health data be acquired, used, disclosed, and stored for legitimate public health purposes
-
Collect the minimum amount of personally identifiable information necessary to conduct public health activities
-
Have strong policies to protect the privacy and security of personally identifiable data
-
Have policies and procedures to ensure the quality of any data they collect or use
-
Have the obligation to use and disseminate summary data to relevant stakeholders in a timely manner
-
Have public health data maintained in a secure environment and transmitted through secure methods
-
Share data for legitimate public health purposes and establish data-use agreements to facilitate sharing data in a timely manner
-
Minimize the number of persons and entities granted access to identifiable data
-
6 Limitations and Challenges of Surveillance
6.1 Distinguishing Acute and Chronic HCV Infection
Many countries do not distinguish between acute and chronic HCV infection and use a case definition based on HCV antibody results alone [76]. For example, in a survey of countries, the European Centre for Disease Prevention and Control found that Germany, the Netherlands, Sweden, England and Wales, and Scotland were enumerating hepatitis C cases based on an antibody test alone [76].
Jaundice may be a practical method for conducting viral hepatitis surveillance in areas where laboratory testing is not routinely included in healthcare visits. For example, in a surveillance system developed to measure the frequency of hepatitis E in northern Uganda, epidemiologists implemented a system originally designed for malaria surveillance [83]. Upon presentation of a person with jaundice to one of the facilities where providers were trained, providers completed a brief case report form, and collected a specimen that was then sent to a central laboratory [83]. At a centralized location, the information from the case report forms and the laboratory results were processed and analyzed to determine the frequency of the different etiologies of jaundice [83].
6.2 Underreporting
Even with the technological advances made in the areas of health information in the USA, the surveillance of hepatitis C continues to be hampered by underreporting, misclassification of cases, and need for more complete data since hepatitis C reporting to the national surveillance network is voluntary. In the USA, CDC estimates that for every reported case of acute hepatitis C, another 12 infections go unreported [80]. There are many reasons why hepatitis C is underreported in the USA. First, HCV infections can only be considered acute if symptoms are present or there is a documented seroconversion. However, 70–85 % of HCV-infected individuals are asymptomatic; about one-half are unaware of their infection [84]. Second, a large percentage of HCV-infected persons may lack access to healthcare services and are thus not reported to health departments. In addition, many states lack the funding needed to conduct enhanced surveillance and do not have the capacity to develop a surveillance system capable of receiving and processing the large number of positive HCV antibody laboratory reports. The number of hepatitis C cases annually reported to health departments often outpaces the amount of resources on hand to fully conduct follow-up investigations to determine if the newly reported case is acute. For these reasons, identifying hepatitis C cases is challenging.
6.3 Resources
Case-based hepatitis C surveillance is a resource-intensive process. Because of many low-resource settings and competing priorities to dedicate the majority of resources to surveillance for acute and effectively preventable conditions, hepatitis C surveillance is often not well developed. As a result, many health departments do not have the capacity to fully investigate every newly reported hepatitis C case. The inability to depend solely on serologic testing to identify acute hepatitis C cases combined with the inability to fully investigate all newly reported cases often leads to the inability to determine if hepatitis C cases are confirmed; these cases instead have a case status label of “probable,” “suspect,” or “unknown.” Unconfirmed cases may never be tested or investigated to determine if they are currently infected [85]. An important decision should be made about the specific objectives and needs for hepatitis C surveillance data such that resources can be used most efficiently and effectively.
6.4 Laboratory Issues
Although a number of highly sensitive and specific rapid tests are available in order to accurately and quickly identify HCV-infected persons and link them to the appropriate care, these tests are often not available in resource-limited settings. The barriers for correctly identifying HCV-infected persons include the lack of simple laboratory assays, need for additional confirmatory testing, and lack of a test for delineating acute from chronic infection.
7 Future Directions
7.1 Health Information Technology
Health information technology (HIT) provides the tools necessary for healthcare providers to better manage patient care through the secure electronic exchange of health information [86]. In a fragmented healthcare system such as that in the USA where multiple healthcare providers are making individual healthcare decisions on the same patient, benefits of the widespread use of HIT include improved quality of healthcare, significantly reduced medical errors, decreased healthcare costs, increased administrative efficiencies, decreased paperwork, and expanded access to affordable healthcare [86, 87]. For example, in 2004, the Massachusetts eHealth Collaborative was formed to establish an electronic health record (EHR) system that would improve the quality, efficiency, and safety of patient care in Massachusetts [88]. By August 2007, nearly 600 physicians participating in the initiative were using EHRs [89].
Historically, a series of critical events which occurred during the late 1990s and early 2000s drew concerns regarding the ability of the USA to respond effectively to acts of bioterrorism and natural epidemics while continuing to protect the health of the nation. These events included the anthrax attacks; destruction of the World Trade Center and the attack on the Pentagon; and emerging disease epidemics such as SARS, avian influenza, and West Nile virus [90]. Having a national system with medical and health information on its citizens would be critical. In response, on April 27, 2004, the president of the USA signed Executive Order 12225, which created the Office of the National Coordinator of Health Information Technology, the principal federal entity charged with supporting the widespread meaningful use of HIT and coordinating efforts to implement and use a nationwide interoperable and secure health information exchange system [90].
7.1.1 Electronic Integration
Ideally, electronic sources of data on HCV infections would have some standardization allowing easy aggregation, supplementation, and analyses. In the USA, with the exception of 16 states, viral hepatitis surveillance systems are neither integrated nor interoperable to produce a singular national electronic surveillance system. Such a system would help to prevent the spread of viral hepatitis and help understand the relationship between viral hepatitis and comorbidities [91]. Hepatitis C surveillance can be greatly improved by expanding health information exchanges (HIEs) and electronic laboratory reporting (ELR).
Where electronic medical records are not integrated, separate data streams can be used to identify persons with HCV infection, for example, using pharmacy records that list antiviral medications specific for hepatitis C [60].
7.1.2 Health Information Exchanges
The framework for a nationwide health information network that connects independent but interoperable public health data systems dates back to 2004 [92]. A key goal of a nationwide health information network is to create an electronic system that can accurately and in a timely fashion exchange patient health information while following security and other protection protocols [93]. HIEs facilitate information flow across various healthcare delivery systems including hospitals, healthcare provider groups, insurers, and government agencies, and are characterized by formal agreements and technologies that facilitate the electronic movement of health-related information [94]. In the USA, funding by the CDC and other public health agencies have supported the development of HIEs and a nationwide health information network [95, 96].
The ability of HIEs to strengthen patient safety through improving laboratory result processing, diagnoses, treatment modalities, and communication between providers and patients has magnified the potential uses for HIEs. Despite the potential uses of HIEs and the great amount of progress that has occurred over the past 10 years, resource constraints prevent widespread implementation of HIEs [97, 98].
7.1.3 Electronic Laboratory Reporting
In the USA, electronic laboratory reporting is conducted by the automated transmittal of laboratory test results of notifiable diseases from commercial, public health, and hospital laboratories to health departments through a laboratory information management system. The goal of ELR for reporting of hepatitis C is to improve the accuracy, timeliness, and completeness by reducing the number of laboratory reports that are manually entered by health departments. When using ELR, laboratories export data from their information systems in a standard file format and electronically transmit it to their health departments through the laboratory information management system.
Prior to the advances in ELR technology in the USA, manual data entry of paper laboratory reports was the standard procedure for collecting data on viral hepatitis infections. However, manual data entry of paper laboratory reports is both labor intensive and costly. ELR has been shown to identify almost three times as many hepatitis C cases as the traditional paper-based method, and, on average, identified those cases nearly 5.5 days earlier than the conventional method [99].
Although ELR shows promising hope for timely and accurate laboratory reporting, there are challenges. First, these systems report only data listed on laboratory reports and do not contain the clinical information required to confirm a hepatitis C case. Secondly, these systems do not report any enhanced epidemiologic data including risk behaviors/exposures, hepatitis A and B vaccination history, and pregnancy status. These additional components are obtained through enhanced follow-up investigation with the provider and patient. Because of the overwhelming burden of past/present hepatitis C laboratory reports that are submitted to health departments, follow-up investigations are often an enormous endeavor, and for highly populated areas such as New York State, only a sample of total past/present hepatitis C reports can be followed. Additionally, complex ELR algorithms that are either inept or inefficient often lead to incorrect detection of new viral hepatitis cases [99].
7.2 Lessons Learned from Enhanced Surveillance in the USA
From 2005 through 2011, the CDC funded seven health departments to conduct enhanced hepatitis C surveillance throughout the USA. Experiences from this collaboration suggest that certain elements are critical to the success of conducting complete, useful surveillance:
-
(a)
Electronic infrastructure to receive and process hepatitis C laboratory reports. Most clinical laboratories have the capacity to report tests associated with all notifiable diseases in an electronic format to the health departments. However, because laboratories lack a standardized system and health departments vary in their capacity to receive and process electronic information, the large number of hepatitis C reports easily overwhelmed their systems. The lesson learned was that health departments needed to invest in electronic data systems that allowed significant numbers of test results to be received, de-duplicated to result in patient-level information, and then processed to determine electronically whether the patient had been reported previously or was a new case [100].
-
(b)
Funding for staff at health departments to conduct follow-up investigation. Because of limited human resources, it became clear that attempting to follow-up on all de-duplicated cases was not feasible. The solution to this problem was to conduct follow-up investigation on a random sample of cases. In most sites, sampling was conducted prospectively on recently reported cases, allowing a 3-month waiting period to ensure that providers had notified patients of their test results. The goal in most sites was to sample ≥10 % of reported cases and to obtain supplemental information from the healthcare provider associated with the positive test result.
-
(c)
Flexibility of data collection instruments and data entry and storage systems. Previously, information on mode of transmission was considered desirable, but more helpful to prevention was the identification of which individuals were linked to care. Several health departments had the flexibility to pilot new information items including whether the individual had seen a healthcare provider for hepatitis-related care, and whether they had ever been treated for hepatitis C.
-
(d)
Secure and standardized transmission of data to a central office. Difficulties with the larger electronic system for notifiable diseases resulted in the use of an independent, secure transfer protocol mechanism to receive electronic data from sites.
-
(e)
Capacity to conduct analyses at the central office. The application of standardized case definitions was complicated at the local level by subjective interpretations and applications of the definition. Data collected on all positive HCV antibody tests allows surveillance programs to understand the population testing positive, and not only those who have the additional confirmatory testing requirements to meet the case definition (e.g., RIBA, RNA). Therefore, a best practice is to receive all data elements and observations health departments are able to collect and send them to a central office. Then, standardized selection criteria can be applied prior to data analyses. For example, the current US hepatitis C case definition requires a confirmatory antibody test; however, understanding the frequency with which persons test positive and are then not reported to have a follow-up test is useful for prevention [85].
7.3 Conclusions
Hepatitis C surveillance can yield useful information for understanding burden of disease, preventing outbreaks, identifying high-risk populations, and planning and evaluating prevention activities. However, careful consideration of objectives should be balanced with available resources. The current US hepatitis C surveillance system forms the backbone of surveillance and provides incidence data. Enhanced surveillance activities provide additional risk and exposure information on cases. To describe the complete spectrum of HCV disease, HCV-related information from additional sources of data, including population-based surveys, is used. As healthcare services evolve in their application of informatics, surveillance of HCV infection can take advantage of the events generated from HCV-related medical encounters in electronic medical records. Testing data from laboratories could be used to monitor the implementation of screening recommendations, and results from nucleic acid tests could be useful to distinguish between current present and resolved or past HCV infection.
Abbreviations
- CDC:
-
United States Centers for Disease Control and Prevention
- CLD:
-
Chronic liver disease
- EHR:
-
Electronic health record
- ELR:
-
Electronic laboratory reporting
- HCC:
-
Hepatocellular carcinoma
- HCV:
-
Hepatitis C virus
- HIEs:
-
Health information exchanges
- HIT:
-
Health information technology
- IDU:
-
Injection drug use
- MSM:
-
Men who have sex with men
- NHANES:
-
National Health and Nutrition Examination Survey
- RIBA:
-
Recombinant immunoblot assay
- SVR:
-
Sustained virologic response
- U.S.:
-
United States
References
Armstrong G, Wasley A, Simard E, McQuillan G, Kuhnert W, Alter M. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med. 2006;144(10):705–14.
WHO. Global surveillance and control of hepatitis C. Report of a WHO Consultation organized in collaboration with the Viral Hepatitis Prevention Board, Antwerp, Belgium. J Viral Hepat. 1999;6:35–47.
Dobbins J, Stewart J, Demmler G. Surveillance of congenital cytomegalovirus disease, 1990–1991. Collaborating Registry Group. MMWR CDC Surveill Summ. 1992;41(2):35–9.
Houghton M. The long and winding road leading to the identification of the hepatitis C virus. J Hepatol. 2009;51:939–48.
Choo Q, Kuo G, Weiner A, Overby L, Bradley D, Houghton M. Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science. 1989;244:359–62.
Centers for Disease Control and Prevention. Hepatitis C FAQs for health professionals. Available at: http://www.cdc.gov/hepatitis/hcv/hcvfaq.htm#b10. Accessed on August 8, 2013.
Ghany M, Nelson D, Strader D, Thomas D, Seeff L. An update on treatment of genotype 1 chronic hepatitis C virus infection: 2011 Practice Guideline by the American Association for the Study of Liver Diseases. Hepatology. 2011;54:1433–44.
CDC. Recommendations for prevention and control of hepatitis C virus (HCV) infection and HCV-related chronic disease. MMWR Recomm Rep. 1998;47(RR-19):1–33.
Centers for Disease Control and Prevention. CDC/CSTE case definitions. Available at: http://wwwn.cdc.gov/NNDSS/script/casedefDefault.aspx. Accessed on September 5, 2013.
Shepard C, Finelli L, Alter M. Global epidemiology of hepatitis C virus infection. Lancet. 2005;5(9):558–67.
El-Zanaty F, Way A. Egypt demographic and health survey 2008. Cairo, Egypt: Ministry of Health, El-Zanaty and Associates, and Macro International; 2009.
Denniston M, Jiles R, Drobeniuc J, et al. Chronic hepatitis C virus infection in the United States, National Health and Nutrition Examination Survey 2003 to 2010. Ann Intern Med. 2014;160:293–300.
Centers for Disease Control and Prevention. Recommendations for the identification of chronic hepatitis C virus infection among persons born during 1945–1965. MMWR Recomm Rep. 2012;61(RR04):1–18.
Zein N. Clinical significance of hepatitis C virus genotypes. Clin Microbiol Rev. 2000;13(2):223–35.
Liang T, Rehermann B, Seeff L, Hoofnagle J. Pathogenesis, natural history, treatment, and prevention of hepatitis C. Ann Intern Med. 2000;132(4):296–305.
Centers for Disease Control and Prevention. Surveillance for viral hepatitis - United States, 2011. Available at: http://www.cdc.gov/hepatitis/Statistics/2011Surveillance/index.htm. Accessed on September 5, 2013. 2013.
CDC. Notes from the field: hepatitis c virus infection among young adults-rural Wisconsin, 2010. MMWR Morb Mortal Wkly Rep. 2012;61:358.
CDC. Use of enhances surveillance for hepatitis c virus infection to detect a cluster among young injection drug users-New York, November 2004-April 2007. MMWR Morb Mortal Wkly Rep. 2008;57:517–21.
CDC. Hepatitis C virus infection among adolescents and young adults - Massachusetts, 2002-2009. MMWR Morb Mortal Wkly Rep. 2011;60(17):537–41.
Henderson D. Managing occupational risks for hepatitis C transmission in the health care setting. Clin Microbiol Rev. 2003;16:546–68.
Centers for Disease Control and Prevention. Viral hepatitis surveillance – United States, 2010. Available at: http://www.cdc.gov/hepatitis/Statistics/2010Surveillance/index.htm. Accessed on November 21, 2013. 2012.
Selvarajah S, Busch M. Transfusion transmission of HCV, a long but successful road map to safety. Antivir Ther. 2012;17:1423–9.
Averhoff F, Glass N, Holtzman D. Global burden of hepatitis C: considerations for healthcare providers in the United States. Clin Infect Dis. 2012;55 Suppl 1:510–5.
Tohme R, Holmberg S. Is sexual contact a major mode of hepatitis C virus transmission? Hepatology. 2010;52:1497–505.
Centers for Disease Control and Prevention. Sexual transmission of hepatitis C virus among HIV-infected men who have sex with men—New York City, 2005–2010. MMWR Morb Mortal Wkly Rep. 2011;60:945–50.
Chak E, Talal A, Sherman K, Schiff E, Saab S. Hepatitis C virus infection in USA: an estimate of true prevalence. Liver Int. 2011;31:1090–101.
Dominitz J, Boyko E, Koepsell T, Heagerty P, Maynard C, Sporleder J. Elevated prevalence of hepatitis C infection in users of United States Veterans Medical Centers. Hepatology. 2005;41:88–96.
Kim W. The burden of hepatitis C in the United States. Hepatology. 2002;36:S30–4.
Centers for Disease Control and Prevention. Progress toward prevention and control of hepatitis C virus infection—Egypt, 2001–2012. MMWR Morb Mortal Wkly Rep. 2012;61(29):545–9.
Perz J, Armstrong G, Farrington L, Hutin Y, Bell B. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol. 2006;45:529–38.
Bell B, Manos M, Zaman A, Terrault N, Thomas A. The epidemiology of newly diagnosed chronic liver disease in gastroenterology practices in the United States: results from population-based surveillance. Am J Gastroenterol. 2008;103:2727–36.
Ly K, Xing J, Klevens R, Jiles R, Ward J, Holmberg S. The growing burden of mortality from viral hepatitis in the United States, 1999-2007. Ann Intern Med. 2012;156:271–8.
El-Kamary S, Jhaveri R, Shardell M. All-cause, liver-related, and non–liver-related mortality among HCV-infected individuals in the general U.S. population. Clin Infect Dis. 2011;53(2):150–7.
Lee M, Yang H, Lu S, et al. Chronic hepatitis C virus infection increases mortality from hepatic and extrahepatic diseases: a community-based long-term prospective study. J Infect Dis. 2012;206(4):469–77.
Ly K, Xing J, Klevens R, Jiles R, Holmberg S. Causes of death and characteristics of decedents with viral hepatitis, United States, 2010. Clin Infect Dis. 2014;58:40. doi:10.1093/cid/cit642.
AASLD/IDSA. Recommendations for testing, managing, and treating hepatitis C. Available at: http://www.hcvguidelines.org/. Accessed March 17, 2014.
European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B virus infection. J Hepatol. 2012;57:167–85.
World Gastroenterology Organisation. World Gastroenterology Organisation global guidelines: diagnosis, management and prevention of hepatitis C. Available at: http://www.worldgastroenterology.org/assets/export/userfiles/WGO_Hepatitis%20C_Final%20Version.pdf. Accessed on March 20, 2014.
Poynard T, Yuen M, Ratzin V, Lai C. Viral hepatitis C. Lancet. 2003;362:2095–100.
Kamili S, Drobeniuc J, Araujo A, Hayden T. Laboratory diagnostics for hepatitis C virus infection. Clin Infect Dis. 2012;55 Suppl 1:S43–8.
Centers for Disease Control and Prevention. Testing for HCV infection: an update of guidance for clinicians and laboratorians. MMWR Morb Mortal Wkly Rep. 2013;62(18):362–5.
Maity S, Nandi S, Biswas S, Sadhukhan S, Saha M. Performance and diagnostic usefulness of commercially available enzyme linked immunosorbent assay and rapid kits for detection of HIV, HBV and HCV in India. Virol J. 2012;9:290–8.
Centers for Disease Control and Prevention. Guidelines for laboratory testing and result reporting of antibody to hepatitis C virus. MMWR Recomm Rep. 2003;52(RR03):1–16.
Chamie G, Bonacini M, Bangsberg D, et al. Factors associated with seronegative chronic hepatitis C virus infection in HIV infection. Clin Infect Dis. 2007;44:577–83.
Centers for Disease Control and Prevention. Recommended testing sequence for identifying current hepatitis C virus (HCV) infection. Available at: http://www.cdc.gov/hepatitis/HCV/PDFs/hcv_flow.pdf. Accessed on March 20, 2014.
Gu S, Liu J, Zhang H, et al. Core antigen tests for hepatitis C virus: a meta-analysis. Mol Biol Rep. 2012;39:8197–208.
Lambert N. Value of HCV antigen-antibody combined HCV assay in hepatitis C diagnosis. Dev Biol (Basel). 2007;127:113–21.
Dawson G. The potential role of HCV core antigen testing in diagnosing HCV infection. Antivir Ther. 2012;17:1431–5.
U.S. Food and Drug Administration. Complete list of donor screening assays for infectious agents and HIV diagnostic assays. Available at: http://www.fda.gov/biologicsbloodvaccines/bloodbloodproducts/approvedproducts/licensedproductsblas/blooddonorscreening/infectiousdisease/ucm080466.htm#anti_HCV_Assays. Accessed on March 20, 2014.
Vidya M, Saravanan S, Rifkin S, et al. Dried blood spots versus plasma for the quantitation of HIV-1 RNA using a real-time PCR, m2000rt assay. J Virol Methods. 2012;181:177–81.
McCarron B, Fox R, Wilson K, et al. Hepatitis C antibody detection in dried blood spots. J Viral Hepat. 1999;6:453–6.
Abe K, Konomi N. Hepatitis C virus RNA in dried serum spotted onto filter paper is stable at room temperature. J Clin Microbiol. 1998;69:3070–2.
Chasela C, Wall P, Drobeniuc J, et al. Prevalence of hepatitis C virus infection among human immunodeficiency virus-1-infected pregnant women in Malawi: the BAN study. J Clin Virol. 2012;54:318–20.
Mullis C, Laeyendecker O, Reynolds S, et al. High frequency of false-positive hepatitis C virus enzyme-linked immunosorbent assay in Rakai, Uganda. Clin Infect Dis. 2013;57:1747–50.
Pearlman B, Traub N. Sustained virologic response to antiviral therapy for chronic hepatitis C virus infection: a cure and so much more. Clin Infect Dis. 2011;52:889–900.
Backus L, Boothroyd D, Phillips B, Belperio P, Halloran J, Mole L. A sustained virologic response reduces risk of all-cause mortality in patients with hepatitis C. Clin Gastroenterol Hepatol. 2011;9:509–16.
van der Meer A, Veldt B, Feld J, et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA. 2012;308:2584–93.
Chou R, Hartung D, Rahman B, Wasson N, Cottrell E, Fu R. Treatment for hepatitis C virus infection in adults. Comparative Effectiveness Review No. 76. (Prepared by Oregon Evidence-based Practice Center under Contract No. 290-2007-10057-I.) AHRQ Publication No. 12(13)-EHC113-EF. Rockville, MD: Agency for Healthcare Research and Quality. 2012. Available at: http://www.effectivehealthcare.ahrq.gov/reports/final.cfm. Accessed on May 24, 2013.
Casey L, Lee W. Hepatitis C virus therapy update 2013. Curr Opin Gastroenterol. 2013;29:243–9.
U.S. Food and Drug Administration. FDA approves Sovaldi for chronic hepatitis C. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm377888.htm. Accessed on December 24, 2013.
Yawn B, Gazzuola L, Wollan P, Kim W. Development and maintenance of a community-based hepatitis C registry. Am J Manag Care. 2002;8:253–61.
Ruf M, Cohuet S, Maguire H, et al. Setting up an enhanced surveillance of newly acquired hepatitis C infection in men who have sex with men: a pilot in London and South East region of England. Euro Surveill. 2008;13(47):1–3.
Treso B, Takacs M, Dencs A, Dudas M, Par A, Rusvai E. Molecular epidemiology of hepatitis C virus genotypes and subtypes among injecting drug users in Hungary. Euro Surveill. 2013;18(47):1–6.
Nsubuga P, White M, Thacker S, et al. Chapter 53. Public health surveillance: a tool for targeting and monitoring intervention. In: Jamison DT, Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB, Jha P, Mills A, Musgrove P, editors. Disease control priorities in developing countries. 2nd ed. Washington, DC: The World Bank and Oxford University Press; 2006.
Alter M, Hadler S, Margolis H, et al. The changing epidemiology of hepatitis B in the United States: need for alternative vaccination strategies. JAMA. 1990;63(9):1218–22.
Klevens R, Miller J, Vonderwahl C, et al. Population-based surveillance for hepatitis C virus, United States, 2006–2007. Emerg Infect Dis. 2009;15(9):1499–502.
Iqbal K, Klevens R, Jiles R. Comparison of acute viral hepatitis data quality using two methodologies, 2005-2007. Public Health Rep. 2012;127(6):591–7.
Centers for Disease Control and Prevention. Hepatocellular carcinoma – United States, 2001-2006. MMWR Morb Mortal Wkly Rep. 2010;59(17):517–20.
Davis K, Mitra D, Medjedovic J, Beam C, Rustgi V. Direct economic burden of chronic hepatitis C virus in a United States managed care population. J Clin Gastroenterol. 2011;45:e17–24.
World Health Organization. International classification of diseases, 10th revision. Geneva: World Health Organization; 1998.
Klevens R, Kruszon-Moran D, Wasley A, et al. Seroprevalence of hepatitis A virus antibodies in the U.S.: results from the National Health and Nutrition Examination Survey. Public Health Rep. 2011;126(4):522–32.
Wasley A, Kruszon-Moran D, Kuhnert W, et al. The prevalence of hepatitis B virus infection in the United States in the era of vaccination. J Infect Dis. 2010;202(2):192–201.
Centers for Disease Control and Prevention. National health and nutrition examination survey. Available at: http://www.cdc.gov/nchs/nhanes/nhanes_questionnaires.htm. Accessed on January 6, 2014.
Roberts H, Utuama O, Klevens R, Teshale E, Hughes E, Jiles R. The contribution of viral hepatitis to the burden of chronic liver disease in the United States. Am J Gastroenterol. 2014;109:387–93.
Centers for Disease Control and Prevention. Viral hepatitis statistics and surveillance. Available at: http://www.cdc.gov/hepatitis/statistics/. Accessed on January 8, 2014.
European Centre for Disease Prevention and Control. Annual Epidemiological Report 2012. Reporting on 2010 surveillance data and 2011 epidemic intelligence data. Stockholm: ECDC; 2012. doi:10.2900/76137. ISBN 978-92-9193-443-0 ISSN 1830-6160.
The Kirby Institute. HIV, viral hepatitis and sexually transmissible infections in Australia Annual Surveillance Report 2012. Sydney, NSW: The Kirby Institute for infection and immunity in society, University of New South Wales; 2012.
Centers for Disease Control and Prevention. Use of enhanced surveillance for hepatitis C virus infection to detect a cluster among young injection drug users - New York, November 2004-April 2007. MMWR Morb Mortal Wkly Rep. 2008;57:517–21.
Centers for Disease Control and Prevention. Guidelines for viral hepatitis surveillance and case management, Atlanta, Georgia, 2005. Available at: http://www.cdc.gov/hepatitis/PDFs/2005Guidlines-Surv-CaseMngmt.pdf. Accessed on November 25, 2013.
Klevens R, Liu S, Roberts H, Jiles R, Holmberg S. Estimating acute viral hepatitis infections from nationally reported cases. Am J Public Health. 2014;104:482–7.
Centers for Disease Control and Prevention. Data security and confidentiality guidelines for HIV, viral hepatitis, sexually transmitted disease, and tuberculosis programs: standards to facilitate sharing and use of surveillance data for public health action. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2011.
Lee L, Gostin L. Ethical collection, storage, and use of public health data: a proposal for a national privacy protection. JAMA. 2009;302(1):82–4.
Gerbi GB, Williams R, Bakamutumaho B, et al. Hepatitis E as a cause of acute jaundice syndrome in northern Uganda, 2010–2012. Am J Trop Med Hyg. 2015;92:411–4.
Denniston M, Klevens R, McQuillan G, Jiles R. Awareness of infection, knowledge of hepatitis C, and medical follow-up among individuals testing positive for hepatitis C: National Health and Nutrition Examination Survey 2001-2008. Hepatology. 2012;55(6):1652–61.
Centers for Disease Control and Prevention. Vital signs: evaluation of hepatitis C virus infection testing and reporting – eight US sites, 2005-2011. MMWR Morb Mortal Wkly Rep. 2013;62:357–61.
United States Department of Health and Human Services HealthIT.gov. Compatibility & information exchange. Available at: http://www.healthit.gov/providers-professionals. Accessed on August 1, 2013.
Blumenthal D. Stimulating the adoption of health information technology. N Engl J Med. 2009;360(15):1477–9.
Goroll A, Simon S, Tripathi M, Asgenzo C, Bates D. Community-wide implementation of health information technology: the Massachusetts eHealth Collaborative Experience. J Am Med Inform Assoc. 2009;16(1):132–9.
Massachusetts eHealth Collaborative. History. Available at: http://www.maehc.org/about/history/. Accessed on January 6, 2014.
Long Island Patient Information Exchange (LIPIX). History of the health information exchange. New York: LIPIX, Inc. Available at: http://www.lipix.org/about/history.html. Accessed on August 1, 2013.
Centers for Disease Control and Prevention. Program collaboration and service integration: enhancing the prevention and control of HIV/AIDS, viral hepatitis, sexually transmitted diseases, and tuberculosis in the United States. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2009.
National Committee on Vital and Health Statistics. Report to the secretary of HHS functional requirements needed for the initial definition of a Nationwide Health Information Network (NHIN). Available at: http://www.ncvhs.hhs.gov/061030lt.pdf. Accessed on November 20, 2013.
Walker J, Pan E, Johnston D, Adler-Milstein J, Bates D, Middleton B. The value of health care information exchange and interoperability. Health Affairs. 2005;(Suppl Web Exclusives):W5–10.
Office of the National Coordinator for Health Information Technology. Mission statement. Available at: http://www.hhs.gov/healthit/onc/mission. Accessed on November 26, 2013.
Federal Business Opportunities. CDC funding opportunity announcement: accelerating public health situational awareness through health information exchanges. Available at: https://www.fbo.gov/index?s=opportunity&mode=form&tab=core&id=e20621df660665af7606627430ba4108&_cview=0. Accessed on November 20, 2013.
National Prevention Information Network. CDC funding opportunity announcement: viral hepatitis - prevention and surveillance. Available at: http://www.cdcnpin.org/Display/FundDisplay.asp?FundNbr=4546. Accessed on November 20, 2013.
Des Roches C, Campbell E, Rao S. Electronic health records in ambulatory care—a national survey of physicians. N Engl J Med. 2008;359:50–60.
Adler-Milstein J, McAfee A, Bates D, Jha A. The state of regional health information organizations: current activities and financing. Health Aff. 2008;27:W60–9.
Overhage J, Grannis S, McDonald C. A comparison of the completeness and timeliness of automated electronic laboratory reporting and spontaneous reporting of notifiable conditions. Am J Public Health. 2008;98:344–50.
New York State Department of Public Health. Laboratory reporting of 2010 communicable diseases. Available at: http://www.wadsworth.org/labcert/regaffairs/clinical/commdiseaseguide.pdf. Accessed December 24, 2013.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Ly, K.N., Hughes, E.M., Jiles, R.B., Klevens, R.M., Roberts, H., Teshale, E. (2015). Surveillance for Hepatitis C. In: Shapshak, P., Sinnott, J., Somboonwit, C., Kuhn, J. (eds) Global Virology I - Identifying and Investigating Viral Diseases. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-2410-3_6
Download citation
DOI: https://doi.org/10.1007/978-1-4939-2410-3_6
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-2409-7
Online ISBN: 978-1-4939-2410-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)