
Abstract
Gestational trophoblastic disease (GTD) is a term that encompasses a spectrum of disorders all arising from the placenta, and specifically, from the villous trophoblast of the placenta. These diseases include hydatidiform mole (both complete and partial), invasive mole, choriocarcinoma (CCA), and placental site trophoblastic tumor (PSTT). The term gestational trophoblastic neoplasia (GTN) includes the disorders of invasive mole, CCA, and PSTT, as they have significant clinical impact. While in the past, this spectrum of diseases was known to have serious morbidity and mortality, with current diagnosis and treatment, cure rates are quoted to upwards of 98 % (Sebire and Seckle, BMJ 227:A1193, 2008). In this chapter, diagnosis, staging, and management of gestational trophoblastic disease are discussed.
Similar content being viewed by others



Keywords
Epidemiology
Incidence
-
Difficult to determine true incidence due to uncommon diagnosis of GTD and inaccuracy of documentation of pregnancy loss [2].
-
North America, Australia, New Zealand, and Europe incidence ranges from 0.57 to 1.1 per 1,000 pregnancies; Southeast Asia and Japan 2.0 per 1,000 [2].
-
In Europe and North America, incidence of CCA estimated at 1 in 40 hydatidiform moles and 1 in 160,000 term pregnancies [3].
-
In Southeast Asia and Japan, incidence of CCA is higher, ranging from 3.3 to 9.2 per 40,000 term pregnancies [3].
-
Incidence rates of CCA and hydatidiform moles have declined over past 30 years [3].
-
Most consistent risk factors for GTD:
-
Extremes of reproductive age (RR 1–5).
-
History of prior molar pregnancy (RR 10–40) [4].
-
-
Only consistent environmental association: Inverse relationship between β carotene and dietary animal fat intake [5].
-
CCA risk factors: Prior complete hydatidiform mole, ethnicity, advanced maternal age.
Pathology
-
All GTD originate from placental trophoblast.
-
Normal trophoblast includes: cytotrophoblast, syncytiotrophoblast, intermediate trophoblast [7].
-
Cytotrophoblast: supplies syncytium with cells and becomes chorionic villi.
-
Basalis layer of endometrium and villous chorion adjacent to endometrium form functional placenta [4].
-
-
Syncytiotrophoblast: Invades endometrial stroma and produces hCG.
-
Intermediate trophoblast: Located in villi, implantation site, and chorionic sac [7].
-
Hydatidiform moles and CCA from villous trophoblast (Fig. 5.1a).
Fig. 5.1. 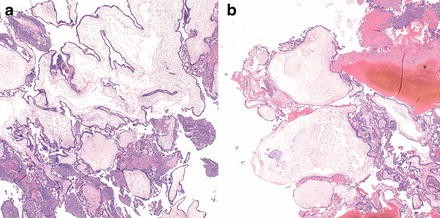
(a) Complete hydatidiform mole. All chorionic villi are enlarged and have abnormal shapes. There is marked hyperplasia of the trophoblast. Circumferential proliferation of the trophoblast around the villi is also noted, best seen in the upper left corner. Hematoxylin and eosin, original magnification 20×. (b) Partial hydatidiform mole. A few markedly enlarged chorionic villi containing central fluid-filled spaces (cisterns) are interspersed with smaller villi, creating a dimorphic population of villi. There is hyperplasia of the trophoblast, best seen in the upper right corner. Hematoxylin and eosin, original magnification 20×.
-
PSTT from intermediate trophoblast.
-
-
Hydatidiform moles: Varying degrees of trophoblastic proliferation.
-
Complete moles: Absence of fetus or embryo.
-
Trophoblast is hyperplastic.
-
-
Partial moles: Identifiable fetal tissue (Fig. 5.1b).
-
Villi with focal edema [7].
-
-
10–17 % of hydatidiform moles become invasive mole: Myometrial invasion of hydatidiform mole via direct extension through tissue or venous channels [7].
-
15 % of invasive moles metastasize: Lung and vagina most common.
-
Clinically diagnosed with persistently elevated hCG levels.
-
CCA: Abnormal trophoblastic hyperplasia and anaplasia, absence of chorionic villi, hemorrhage, and necrosis [4] (Fig. 5.2).
Fig. 5.2. 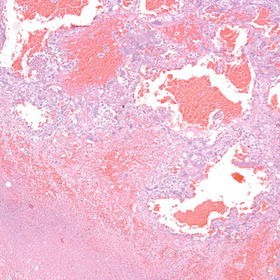
Choriocarcinoma. The tumor is highly hemorrhagic. Necrosis is seen in the lower left corner. The tumor is composed of neoplastic cytotrophoblast (clear cells) and syncytiotrophoblast (purple-staining cells with multiple nuclei). Hematoxylin and eosin, original magnification 100×.
-
-
-
-
PSTT: From placental implantation site with mononuclear intermediate trophoblasts without chorionic villi.
-
More lymphatic metastasis.
-
Diffuse cytokeratin and human placental lactogen (HPL) staining [9] (Fig. 5.3).
Fig. 5.3. 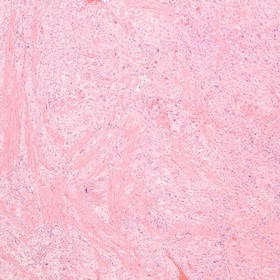
Placental site trophoblastic tumor. The tumor is composed of masses of atypical intermediate trophoblast (pale-staining cells) infiltrating between the bundles of myometrium (staining bright pink). Hematoxylin and eosin, original magnification 100×.
-
-
-
Matrix metalloproteinases (MMPs): Involved in metabolism of extracellular matrix, needed for invasion of maternal tissues [10].



Genetics
-
Partial moles typically are triploid in nature (69 XXX or 69 XXY) (Table 5.1) [8].
Table 5.1. Characteristics of complete and partial moles [8]. -
Normal ovum with two spermatozoa [13].
-
-
Complete moles are diploid with all chromosomes from paternal origin (46 XX or XY).
-
Recurrent molar pregnancies have biparental rather than androgenic complete moles [16].
-
Associated with a strong family history, with imprinting abnormalities noted that resemble fully paternal chromosomes [17].
-
Affected chromosome noted in familial cases: 19q13.3–13.4 with mutations in NLRP7 [18].
-
NLRP7 is a cytoplasmic protein, with members of the NLRP family associated with inflammatory processes and apoptosis [15].
-
Diagnosis
Symptoms
-
Complete hydatidiform moles:
-
Partial moles:
-
Present with incomplete or missed abortion 90 % of the time, followed by vaginal bleeding (75 %) [20].
-
Imaging
-
Ultrasound has replaced any other diagnostic tool to diagnose complete or partial moles [21].
-
Complete moles are characterized by a heterogenous mass (snowstorm pattern) without fetus.
-
Ultrasound can demonstrate cystic spaces in the placenta and vesicular pattern of multiple echoes [22].
-
Only 40–60 % of complete moles are detected as molar on ultrasound.
-
American Congress of Obstetrics and Gynecology (ACOG) recommends pathologic evaluation of tissue after spontaneous and therapeutic abortions to confirm diagnosis [23].
-
Presentation of gestational trophoblastic neoplasia is dependent on the antecedent pregnancy event, extent of disease, and histopathology [19].
-
Postmolar GTN presents with enlarged irregular uterus, persistent ovarian enlargement, and irregular bleeding [19].
-
GTN can be diagnosed after metastases are found, and these metastases can bleed.
-
HCG Levels in GTD
-
hCG is composed of an α- subunit, and β-subunit; the β-subunit is specific to the placenta.
-
hCG is hyperglycosylated in the first trimester of normal pregnancies; in GTD there are other subunits, such as β core, free β-hCG, nicked free β, or c-terminal peptide [24].
-
Hydatidiform moles have markedly elevated hCG levels above normal pregnancy.
-
Complete moles pre-evacuation have hCG levels >100,000 [25].
-
Less than 10 % of partial moles have pre-evacuation hCG levels >100,000.
-
-
Postmolar GTN is diagnosed with rising or plateauing hCG levels after evacuation. CCA is diagnosed with elevated hCG levels after other pregnancy event, likely associated with metastatic disease. PSTT only associated with slight elevation of hCG, but elevated human placental lactogen.
-
Postmolar GTN diagnosed by one of the following [26].
-
hCG level plateau of 4 values plus or minus 10 % recorded over a 3-week period (days 1, 7, 14, and 21).
-
hCG level increase of more than 20 % of 3 values recorded over a 2-week period (days 1, 7, and 10).
-
Persistence of detectable hCG for more than 6 months after molar evacuation.
-
Histopathologic diagnosis of CCA.
-
Presence of metastatic disease.
-
New pregnancy must be excluded prior to diagnosis.
-
-
Important to use an assay that can detect intact hCG molecules, but also H-hCG and H-freeβ, as well as degradation products.
-
Different assays can have up to 58-fold variation of hCG results [27].
-
-
Diagnosis of GTD confirmed by cervical dilation and suction curettage; [28]. GOG 242 (results discussed below) illustrated utility of second D&C as a curative measure.
Persistently Low Levels of hCG
-
Multiple conditions can cause low levels of hCG.
-
Pregnancy, GTD, false positive or phantom hCG, other malignancies, pituitary hCG.
-
High proportion of women with persistent hCG, without findings of pregnancy or GTD, can go on to unnecessary chemotherapy or hysterectomy [29].
-
Guidelines recommended by the USA hCG reference service for persistent hCG values include ruling out pregnancy, determining if hCG values are real, and determining if active GTN, PSTT, or non-trophoblastic malignancy is present.
-
Serum should be sent to special laboratories to check for H-hCG and free βhCG [29].
-
-
Phantom or false hCG values can be present in 3–4 % of healthy women [30].
-
Caused by cross-reactivity with heterophilic antibodies in the serum.
-
Product of “sandwich” assays that measure mixtures of hCG.
-
-
Not present in urine hCG tests; and thus negative urine hCG can be used to confirm false positive [31].
-
Serum can be diluted serially and run through assays to check for false positives (dilution does not affect false titers), or sent for additional tests (see above) [32].
-
No treatment is required for false positive hCG results [32].
-
Diagnostic Evaluation
-
When GTN diagnosed or greatly suspected, patient should undergo thorough evaluation for assessment of extent of disease prior to initiation of therapy.
-
Blood work: Hepatic function, renal function, baseline serum hCG, blood count (CBC), thyroid function tests, blood type.
-
Pelvic imaging: By ultrasound or CT to assess for residual disease within uterus, evidence of pelvic spread.
-
Chest imaging: Can be performed via Chest X-ray or CT scan. While there is a higher sensitivity for detection of pulmonary metastasis with Chest CT (as high as 40 % in patients with negative Chest X-ray) compared to Chest X-ray, mandatory Chest CT is not necessary if detection of occult pulmonary metastasis does not change treatment protocol [33].
-
Patients who are asymptomatic with normal pelvic and chest imaging do not require any additional radiologic imaging [23].
-
In all patients with choriocarcinoma or in those patients with vaginal or lung metastasis, Brain MRI should be obtained.
-
If lesion in vagina suggestive of GTN present, biopsy is not recommended due to severe bleeding risk [34].
-
Staging
-
FIGO Committee on Gynecologic Oncology in 2000 set forth a staging and classification system for Gestational Trophoblastic Neoplasia [35].
-
The staging system is used in combination with the World Health Organization risk-factor scoring system for GTN [36] (see Tables 5.2 and 5.3).
Table 5.2. FIGO anatomic staging for gestational trophoblastic neoplasia [36]. Table 5.3. Modified WHO prognostic scoring system as adapted by FIGO [36]. -
The FIGO staging system is anatomically based.
-
Diagnosis should be presented with Stage (denoted by roman numerals I–IV), followed by the sum of actual risk factors (in Arabic numerals) separated by a colon. For example, II: 4 [35].
-
Non metastatic and low risk metastatic GTN (Stage I and Stages II–III with scores <7) can be treated with single agent chemotherapy (see Sect. 6) [4].
-
High risk metastatic disease (Stage IV and Stages II–III with scores ≥7) should be treated with multi-agent chemotherapy (see Sect. 6) [4].
Treatment
-
Pretreatment workup includes: CBC including platelet count, clotting studies, renal and liver function tests, blood type with antibody screen, hCG level, and chest X-ray (pre-evacuation) [23].
-
Prior to suction evacuation and curettage, include possible cross match of 2 units.
-
Suction evacuation and curettage is standard of care for those who desire fertility; hysterectomy is appropriate for those who do not [37].
-
The largest cannula that can be introduced through the cervix should be utilized to facilitate rapid evacuation [23].
-
Intraoperative ultrasound can be used to decrease risk of uterine perforation.
-
Oxytocin IV should be used at the start of evacuation to increase uterine contractility and minimize blood loss [23].
-
Rh negative patients should be given rhesus immunoglobulin at the time of the evacuation; Rh is expressed on the trophoblast [38].
-
Medical induction of labor, or hysterotomy is not recommended as they can increase the risk of postmolar GTN and maternal morbidity [39].
-
Prophylactic administration of methotrexate or actinomycin-D chemotherapy should be used only in those with greater than normal risk of postmolar GTN; associated with increased morbidity, and those developing postmolar GTN can be cured with chemotherapy [40].
-
No clear guidelines of management for twin pregnancies with molar and normal fetal pregnancy; may continue pregnancy if desired after close evaluation, although risk of persistent or invasive mole approaches 50 % [23, 41].
-
Close monitoring of patients after evacuation is essential. Serial hCG should be obtained within 48 h of evacuation, followed by weekly assessments during evaluation (until 3 normal values), and at monthly intervals for at least 6 months [23].
-
Contraception recommended for 6–12 months after 1st normal value.
-
Future pregnancies should have first trimester ultrasound, pathologic examination of placenta and other products of conception, and 6 week postpartum hCG value [19].
-
LOW RISK GTN: Stage I, Stage II, or Stage III with score <7, can be treated with single agent Methotrexate (MTX) or actinomycin D chemotherapy [42].
-
Weekly IM or IV MTX, biweekly single dose actinomycin D, 5 day MTX or actinomycin D, and 8 day MTX plus folinic acid can be used (see Treatment Algorithms).
-
hCG levels should be monitored weekly during treatment and consolidation chemotherapy continued for 1–2 cycles after three negative weekly hCG levels have been achieved [4].
-
-
GOG protocol 242 (initially presented at SGO in March 2014).
-
Evaluated the utility of second curettage in the management of persistent GTN.
-
Low risk patients (WHO score 0–6); nonmetastatic disease; excluded CCA and PSTT.
-
64 patients enrolled, 59 eligible for assessment.
-
39 % surgical cure with secondary curettage—efficacy in those with WHO score 0–4.
-
-
High risk GTN: Stage II or III with score ≥7, or Stage IV should be treated with multi agent chemotherapy with or without adjuvant surgery and radiotherapy.
-
Etoposide, high dose methotrexate with folinic acid, actinomycin D, cyclophosphamide, and vincristine (EMA-CO) as primary therapy for high risk GTD [43].
-
Chemotherapy should be used for 2–3 courses after first normal hCG evaluation.
-
Whole brain radiation can be used for brain metastasis; surgery can be used for chemotherapy resistant disease or to control for bleeding metastasis [44].
-
30 % of high risk GTN patients will have an incomplete response to chemotherapy or relapse [45].
-
Salvage chemotherapy with platinum based drugs or surgical resection can treat resistant tumors [46].
-
-
-
Patients with high risk GTN who have high risk prognostic factors can be treated with EP (etoposide-cisplatin induction therapy) [47].
-
High risk features: High thoracic burden of disease, concerns for respiratory compromise, FIGO score greater than 12, hemorrhage, and rapid tumor destruction.
-
Low dose induction with etoposide and cisplatin reduced the number of deaths from 11 of 140 patients (7.8 %) to 1 of 140 patients (0.7 %) [47].
-
-
PSTT are relatively resistant to chemotherapy, and treatment should begin with hysterectomy and lymph node dissection [48].
-
Chemotherapy for PSTT should be limited to metastatic disease or nonmetastatic disease with adverse prognostic factors [48].
-
Chemotherapy regimens include paclitaxel/cisplatin-paclitaxel/etoposide doublet or EMA-EP [49].
-
-
In patients with GTN, after hCG is returned to normal, quantitative hCG levels should be evaluated monthly for 12 months.
-
3 % of patients will relapse in 1st year, and less than 1 % in subsequent years [34].
-
Contraception in cases of GTN should continue for 12 months.
-
Similar subsequent pregnancy evaluation as to molar pregnancy should be utilized.
Clinical Trials
-
GOG 57: Poor prognosis GTD received methotrexate, dactinomycin, and chlorambucil (MAC) or methotrexate, dactinomycin, cyclophosphamide, doxorubicin, melphalan, hydroxyurea, vincristine (CHAMOMA).
-
MAC equally effective and much less toxic than CHAMOMA regimen [50].
-
-
GOG 69: Phase 2 study of nonmetastatic gestational trophoblastic disease patients given Actinomycin-D.
-
ACT-D efficacy and toxicity comparable to conventional nonmetastatic GTD therapy [51].
-
GOG 79: Study of nonmetastatic GTD patients to determine efficacy, toxicity, and cost-effectiveness of weekly IM methotrexate.
-
Weekly IM methotrexate found to be efficacious, minimally toxic, and cost-effective [52].
-
In GOG 79 follow-up study, 40 mg/m2 weekly IM methotrexate therapy had comparable efficacy and had similar toxicity to the 30 mg/m2 weekly dosing.
-
-
GOG 26U: Phase II study of refractory malignant GTD.
-
Ifosfamide (IFX) has activity against choriocarcinoma; addition of etoposide and cisplatin (known as VIP) had significant response in hCG levels and may be curative [53].
-
-
GOG 174: Phase 3 trial of the GOG, JGOG, NCIC, and ECOG in patients with low risk GTN.
-
Compared biweekly intravenous actinomycin-D to weekly IM methotrexate. The remission rate with Actinomycin D was 69 %, compared to 53 % in the methotrexate arm. In the low-risk GTN population, RR with act-D was 73 and 58 % with MTX. No differences in toxicity were reported [54].
-
-
GOG 275 (currently enrolling): Phase 3 randomized trial of the GOG in patients with low risk GTN.
-
Comparing pulsed actinomycin D (1.25 mg/m2) every 14 days versus IV methotrexate (0.4 mg/kg) daily for 5 days every 14 days versus IM methotrexate (50 mg) on days 1, 3, 5, 7 (4 doses per cycle) with leucovorin (15 mg) on days 2, 4, 8, repeated every 14 days.
-
-
Thailand trial: Randomized controlled trial of actinomycin D versus MTX-folinic acid in Stage I low risk GTN patients.
-
Complete remission achieved in 74 % of MTX therapy, and 100 % of actinomycin D arm [55].
-
-
Brazil trial: Retrospective analysis of low risk GTD patients treated with 5 day regimen of single agent MTX or single agent actinomycin D or combination of MTX and actinomycin.
-
Response rates were not statistically significantly different.
-
Adverse side effects increased with combination therapy (62 %) versus single agent MTX (29 %) or actinomycin D (19 %) [56].
-
-
Northwestern trial: Prospective single institution trial of patients with high risk gestational trophoblastic tumors treated with EMA-CO.
-
EMA-CO therapy was well tolerated and had 71 % complete response rate and 91 % survival rate [57].
-
-
Dutch working party on GTD trial: Randomized controlled trial of EMA-CO versus EMA-CP (cisplatin based combination therapy).
-
Remission rates were similar with only slightly shorter duration of treatment [58].
-

Current Standard of Care Chemotherapy
Low Risk GTN [4]
-
Methotrexate alone:
-
Methotrexate 0.4 mg/kg (maximum 25 mg) IV push daily for 5 days every 14 days (89 % primary remission).
-
Methotrexate 30–50 mg/m2 IM weekly (30 mg/m2 most commonly used).
-
-
Methotrexate and Folinic Acid:
-
Methotrexate 1.0 mg/kg–1.5 mg/kg IM or IV days 1, 3, 5, 7.
-
Folinic acid IM (0.1 mg/kg) or po (7.5–15 mg depending on protocol) on days 2, 4, 6, 8.
-
High dose Methotrexate (100 mg/m2 IV push followed by 200 mg/m2 IV over 12 h) with Folinic acid rescue. Treatment interval based on post-treatment hCG trends (increased need for second line therapy and expensive).
-
-
The New England Trophoblastic Disease Center (NETDC) found patients who received the high dose IV MTX 1 day infusion 3–6× more likely to require more courses of chemotherapy compared to patients who received the 8-day regimen [60].
-
Actinomycin D.
-
Actinomycin D 10–12 μg/kg/day for 5 days every other week.
-
Actinomycin D 1.25 mg/m2 IV every 2 weeks (2 mg max dose; more side effect profile).
-
Conclusions Regarding Treatment of Low-Risk GTN
-
No consensus of optimal first line chemotherapy regimen for low risk GTN [61].
-
8 day Methotrexate most cost-effective when compared to weekly methotrexate or pulsed actinomycin D [62]. Active area of investigation in GOG 275.
-
hCG levels should be followed on a weekly basis during treatment until negative. Once normalization of hCG has been achieved, an additional 2–3 cycles of consolidation therapy should be administered. Lybel et al. showed a significantly higher relapse rate (8.3 %) in patients treated with two courses of consolidation MTX compared to those treated with three courses (4.0 %) [63].
High Risk GTN
-
EMA-CO regimen: Current treatment of choice [58].
-
Day 1: Etoposide 100 mg/m2 IV over 30 min, Methotrexate 100 mg/m2 IV push followed by 200 mg/m2 IV over 12 h, Actinomycin D 0.5 mg IV bolus.
-
Day 2: Etoposide 100 mg/m2 IV over 30 min, Actinomycin D 0.5 mg IV bolus.
-
Day 8: Cyclophosphamide 600 mg/m2 IV, Vincristine 1 mg/m2.
-
Folinic Acid: 15 mg po every 12 h × 4 doses, starting 24 h after initiation of MTX.
-
Cycle repeated every 2 weeks until normalization of hCG and then continued for an additional three cycles (6 weeks).
-
In resistant cases, cisplatin 80 mg/m2 IV can be added on day 8 and etoposide 100 mg/m2 to cyclophosphamide and vincristine portions of protocol [64].
-
-
EMA-CP regimen [58]:
-
Day 1: Etoposide 100 mg/m2, Methotrexate 300 mg/m2, Cyclophosphamide 600 mg/m2.
-
Day 2: Etoposide 100 mg/m2, Actinomycin D 0.6 mg.
-
Day 3: Etoposide 100 mg/m2.
-
Day 4: Etoposide 100 mg/m2, Cisplatin 60 mg/m2.
-
Day 5: Etoposide 100 mg/m2.
-
Comparable remission rate to EMA-CO, but not more effective [58].
-
-
Low dose induction chemotherapy with EP: Patients with high risk GTN who were at high risk of death during EMA/CO chemotherapy can be treated with EP (etoposide-cisplatin) induction therapy [47].
-
Patients with high thoracic burden of disease, concerns for respiratory compromise, FIGO score more than 12, hemorrhage, as well as rapid tumor destruction all at increased risk of early death when treatment initiated with standard EMA/CO regimen [47].
-
Giving patients low dose induction with etoposide 100 mg/m2 and cisplatin 20 mg/m2 (for 1–2 cycles) greatly reduced the number of deaths from 11 of 140 patients (7.8 %) to 1 of 140 patients (0.7 %) [47].
-
Treatment of Specific Metastatic Lesions
-
Surgical procedures to resect isolated metastasis can help to reach curative states, especially in cases with concern for hemorrhage [44].
-
Central Nervous System.
-
Whole brain irradiation performed, 3,000 cGy at 200 cGy fractions can achieve cure rates of 50–80 % [65].
-
Stereotactic radiosurgery for isolated lesions (oligometastasis), selected patients.
-
-
Lung.
-
Surgical resection especially in setting of resistant disease, isolated lung nodule.
-
Study by Tomodo et al. identified criteria for appropriate patient selection:
-
Good surgical candidate, controlled primary malignancy, no other evidence of metastatic disease, pulmonary metastasis confined to one lung, and hCG <1,000.
-
If all 5 criteria met, complete remission achieved in 93 % [66].
-
-
-
Liver [61].
-
Surgical resection for isolated lesions or acute bleeding [67].
-
Embolization for bleeding.
-
Chemoresistant and/or Recurrent GTN
-
Of the high risk GTN patients treated with EMA/CO, 30 % will either have an incomplete response or relapse [68].
-
Metastasis to other sites common in these patients.
-
Chemotherapy can be combined with surgical excision to reach cure [44].
-
-
EMA-EP: Can be used for plateauing low levels of hCG or rising levels after complete response to EMA-CO [69].
-
Day 1: Etoposide 100 mg/m2IV over 30 min, Methotrexate 100 mg/m2 IV push followed by 200 mg/m2 IV over 12 h, Actinomycin D 0.5 mg IV bolus.
-
Day 8: Etoposide 150 mg/m2 IV, Cisplatin 75 mg/m2.
-
Folinic Acid: 15 mg po every 12 h × 4 doses, starting 24 h after start of methotrexate.
-
-
Other salvage regimens can include paclitaxel, etoposide, cisplatin, ifosfamide, vinblastine, and bleomycin [70, 71].
-
82 % of patients with failure of initial chemotherapy who were treated with etoposide-platinum based salvage chemotherapy as well as surgical and radiotherapy techniques were able to achieve cure [70].
-
Survival
-
Cure rates for both low risk and non metastatic disease states approach 100 %.
-
20 % of low risk patients will develop initial resistance, but will reach 90 % cure rate with single agent chemotherapy [19].
-
10 % of low risk patients will require multi-agent chemotherapy.
-
80–90 % of high risk GTN patients will have curative therapy.
-
30 % of high risk patients will relapse or fail first line therapy.
-
Gastrointestinal tract metastasis has lowest survival rates at 50 % [72].
-
Curative rates for PSTT 50–60 % for metastatic disease [48].
References
Sebire NJ, Seckle MJ. Gestational trophoblastic disease: current management of hydatidiform mole. BMJ. 2008;227:A1193.
Palmer JR. Advances in the epidemiology of gestational trophoblastic disease. J Repro Med. 1994;39(3):155–62.
Smith HO. Gestational trophoblastic disease epidemiology and trends. Clin Obstet Gynecol. 2003;46(3):541–56.
Singh DK. Gestational trophoblastic disease. In: Karlan BY, Brostow RE, Li AJ, editors. Gynecologic oncology: clinical practice and surgical atlas. 1st ed. New York, NY: Mc Graw Hill; 2012. p. 157–71.
Parazzini F, La Vecchia C, Mangili G, et al. Dietary factors and risk of trophoblastic disease. Am J Obstet Gynecol. 1988;158(1):93–9.
Berkowitz RS, Im SS, Bernstein MR, et al. Gestational trophoblastic disease: subsequent pregnancy outcome, including repeat molar pregnancy. J Reprod Med. 1998;43:81–6.
Bentley RC. Pathology of gestational trophoblastic disease. Clin Obstet Gynecol. 2003;46(3):513–22.
Soper JT, Lewis JL, Hammond CB. Gestational trophoblastic disease. In: Hoskins WJ, Perez CA, Young RC, editors. Principals and practice of gynecologic oncology. 2nd ed. Philadelphia, PA: Lippincott-Raven; 1997. p. 1039–77.
Tang X, Yang F, Jia L, et al. Placental site trophoblastic tumor in the pelvic wall: a case report and review of literature. Indian J Pathol Microbiol. 2013;56(3):300–2.
Kessenbrock K, Plaks V, Werb Z. Matrix metalloproteinases: regulators of the tumor microenvironment. Cell. 2010;141:52–67.
Singh M, Kindelberger D, Nagymanyoki Z, et al. Matrix metalloproteinases and their inhibitors and inducers in gestational trophoblastic disease and normal placenta. Gynecol Oncol. 2011;122:178–82.
Butler GS, Dean RA, Tam EM, et al. Pharmacoproteiomics of metalloproteinase hydroxamate inhibitor in breast cancer cells: dynamics of membrane type 1 matrix metalloproteinase-mediated membrane protein shedding. Mol Cell Biol. 2008;28:4896–914.
Szulman AE, Surti U. The syndromes of hydatidiform mole I and II. Am J Obstet Gynecol. 1978;132(1):20–7.
Fukanaga M. Immunohistochemical characterization of p57 (KIP2) expression in early hydatidiform moles. Hum Pathol. 2002;33(12):1188–92.
Hoffner L, Surti U. The genetics of gestational trophoblastic disease: a rare complication of pregnancy. Cancer Genet. 2012;205(3):63–77.
Fisher RA, Hodges MD, Newlands ES. Familial recurrent hydatidiform mole: a review. J Reprod Med. 2004;49(8):595–601.
Kou YC, Shao L, Peng HH, et al. A recurrent intragenic genomic duplication, other novel mutations in NLRP7 and imprinting defects in recurrent biparental hydatidiform moles. Mol Hum Reprod. 2008;14(1):33–40.
Moglabey YB, Kircheisen R, Seoud M, et al. Genetic mapping of a maternal locus responsible for familial hydatidiform moles. Hum Mol Genet. 1999;8(4):667–71.
Lurain JR. Gestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole. Am J Obstet Gynecol. 2010;203(6):531–9.
Berkowitz RS, Goldstein DB, Bernstein MR. Natural history of partial molar pregnancy. Obstet Gynecol. 1985;66(5):677–81.
Benson CB, Genest DR, Bernstein MR, et al. Sonographic appearance of first trimester complete hydatidiform moles. Ultrasound Obstet Gynecol. 2000;16(2):188–91.
Reid MH, McGahan JP, Oi R. Sonographic evaluation of hydatidiform mole and its look-alikes. AM J Roentgenol. 1983;140(2):307–11.
Committee on Practice Bulletins-Gynecology. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin 53. Diagnosis and treatment of gestational trophoblastic neoplasms. Obstet Gynecol 2004;103:1365–73.
Mitchell H, Seckl MJ. Discrepancies between commercially available immunoassays in the detection of tumour-derived hCG. Mol Cell Endocrinol. 2007;260–262:310–3.
Genest DR, Laborde O, Berkowitz RS, et al. A clinicopathologic study of 153 cases of complete hydatidiform mole (1980–1990): histologic grade lacks prognostic significance. Obstet Gynecol. 1991;78:402–9.
Kohorn EL. The new FIGO 2000 staging and risk factor scoring system for gestational trophoblastic disease: description and critical assessment. Int J Gynecol Cancer. 2001;11(1):73–7.
Cole L, Shahabi S, Butler S, et al. Utility of commonly used commercial human chorionic gonadotropin immunoassays in the diagnosis and management of trophoblastic diseases. Clin Chem. 2001;47(2):308–15.
Garner EI, Feltmate CM, Goldstein DP, et al. The curative effect of a second curettage in persistent trophoblastic disease: a retrospective cohort survey. Gynecol Oncol. 2005;99(1):3–5.
Cole L, Khanlian SA, Giddings A, et al. Gestational trophoblastic diseases: 4. Presentation with persistent low positive human chorionic gonadotropin test results. Gynecol Oncol. 2006;102:165–72.
Palmieri C, Dhillon T, Fisher RA, et al. Management and outcome of healthy women with a persistently elevated beta-hCG. Gynecol Oncol. 2007;106(1):35–43.
Rotmensch S, Cole LA. False diagnosis and needless therapy of presumed malignant disease in women with false-positive human chorionic gonadotropin concentrations. Lancet. 2000;355(9205):712–5.
Cole L, Khanian S. Inappropriate management of women with persistent low hCG results. J Reprod Med. 2004;49(6):423–32.
El G, Garrett A, Goldstein DP, et al. Significance of chest computed tomography findings in the evaluation and treatemtn of persistent gestational trophoblastic neoplasia. J Reprod Med. 2004;49(6):411–4.
Berry E, Hagopian GS, Lurain JR. Vaginal metastases in gestational trophoblastic neoplasia. J Reprod Med. 2006;53(7):487–92.
Ngan HY, Bender H, Benedet JL, et al. Gestational trophoblastic neoplasia, FIGO 2000 staging and classification. Int J Gynaecol Obstet. 2003;83 suppl 1:175–7.
Ngan HY, Kohorn EI, Cole LA, et al. Trophoblastic disease. Int J Gynaecol Obstet. 2012;119S2:S130–6.
Berkowitz RS, Goldstein DP. Molar pregnancy. N Engl J Med. 2009;360:1639–45.
Hancock BW, Tidy JA. Current management of molar pregnancy. J Reprod Med. 2002;47(5):347–54.
Tidy JA, Gillespie AM, Bright N, et al. Gestational trophoblastic disease: a study of mode of evacuation and subsequent need for treatment with chemotherapy. Gynecol Oncol. 2000;78(3 pt 1):309–12.
Limpongsanurak S. Prophylactic actinomycin D for high risk complete hydatidiform mole. J Reprod Med. 2001;46(2):110–6.
Steller MA, Genest DR, Bernstein MR, et al. Natural history of twin pregnancy with complete hydatidiform mole and coexisting fetus. Obstet Gynecol. 1994;83:35–42.
Alazzam M, Tidy J, Hancock BW, et al. First line chemotherapy in low-risk gestational trophoblastic neoplasia. Cochrane Database Syst Rev. 2009;(1):CD007102.
Turan T, Karacay O, Tulunay G, et al. Results with EMA/CO (etoposide, methotrexate, actinomycin D, cyclophosphamide, vincristine) chemotherapy in gestational trophoblastic neoplasia. Int J Gynecol Cancer. 2006;16(3):1432–8.
Feng F, Xiang Y. Surgical management of chemotherapy-resistant gestational trophoblastic neoplasia. Expert Rev Anticancer Ther. 2010;10(1):71–80.
Powles T, Savage PM, Stebbing J, et al. A comparison of patients with relapsed and chemo-refractory gestational trophoblastic neoplasia. Br J Cancer. 2007;96(5):732–7.
Wang J, Short D, Sebire NJ, et al. Salvage chemotherapy of relapsed or high-risk gestational trophoblastic neoplasia (GTN) with paclitaxel/cisplatin alternating with paclitaxel/etoposide (TP/TE). Ann Oncol. 2008;19(9):1578–83.
Alifrangis C, Agarwal R, Short D, et al. EMA/CO for high risk gestational trophoblastic neoplasia: good outcomes with induction low-dose etoposide-cisplatin and genetic analysis. J Clin Oncol. 2013;31(2):280–6.
Hassadia A, Gillespie A, Tidy J, et al. Placental site trophoblastic tumour: clinical features and management. Gynecol Oncol. 2005;99(3):603–7.
Lurain JR. Gestational trophoblastic disease II: classification and management of gestational trophoblastic neoplasia. Am J Obstet Gynecol. 2011;204(1):11–8.
Curry SL, Twiggs L, Slayton R, et al. Preliminary report of toxicity in a randomized comparison of methotrexate, actinomycin D, and chlorambucil (MAC) vs modified bagshawe regimen in “poor prognosis4” gestational trophoblastic disease. Obstet Gynecol. 1989;73(3):357–62.
Petrilli ES, Twiggs LB, Blessing JA, et al. Single dose actinomycin-D treatment for nonmetastatic gestational trophoblastic disease: a prospective phase II trial of the Gynecologic Oncology Group. Cancer. 1987;60:2173–6.
Homesley HD, Blessing JA, Rettenmaier M, et al. Weekly intramuscular methotrexate for nonmetastatic gestational trophoblastic disease (A Gynecologic Oncology Group Study). Obstet Gynecol. 1988;72(3-I):413–8.
Sutton GP, Soper JT, Blessing JA, et al. Ifosfamide alone and in combination in the treatment of refractory malignant gestational trophoblastic disease. Am J Obstet Gynecol. 1992;167(2):489–95.
Osborne RJ, Filiaci V, Schink JC, et al. Phase III trial of weekly methotrexate or pulsed dactinomycin for low-risk gestational trophoblastic neoplasia: a gynecologic oncology group study. J Clin Oncol. 2011;19(7):825–31.
Lertkhachonsuk AA, Isranqura N, Wilailak S, et al. Actinomycin d vs. methotrexate-folinic acid as the treatment of stage I, low-risk gestational trophoblastic neoplasia: a randomized controlled trial. Int J Gynecol Cancer. 2009;19(5):985–8.
Abrao RA, de Andrade JM, Tiezzi DG, et al. Treatment for low-risk gestational trophoblastic disease: comparison of single-agent methotrexate, dactinomycin and combination regimens. Gynecol Oncol. 2008;108(1):149–53.
Escobar PF, Lurain JR, Singh DK, et al. Treratment of high-risk gestational trophoblastic neoplasia with etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine chemotherapy. Gynecol Oncol. 2003;91(3):552–7.
Lybol C, Thomas CM, Blanken EA, et al. Ccomparin cisplatin-based combination chemotherapy with EMA/CO chemotherapy for the treatment of high risk gestational trophoblastic neoplasia. Eur J Cancer. 2013;49(4):860–7.
Reynolds, RK. Overview of gynecologic oncology. University of Michigan Gynecologic Oncology handbook. 11th ed. Ann Arbor; 2010. pp 24–8.
Growden WB, Wolfberg AJ, Goldstein DP, et al. Evaluating methotrexate treatment in patients with low-risk postmolar gestational trophoblastic neoplasia. Gynecol Oncol. 2009;112:353–7.
Berkowitz RS, Goldstein DP. Current advances in the management of gestational trophoblastic disease. Gynecol Oncol. 2013;128(1):3–5.
Shah NT, Barroilhet L, Berkowitz RS, et al. A cost analysis of first-line chemotherapy for low-risk gestational trophoblastic neoplasia. J Reprod Med. 2012;57(5–6):211–8.
Lybol C, Sweep FC, Harvey R, et al. Relapse rates after two vs. three consolidation coursres of methotrexate in the treatment of low-risk gestational trophoblastic neoplasia. Gynecol Oncol. 2012;125:576–9.
Ghaemmaghami F, Behtash N, Soleimani K, et al. Management of patients with metastatic gestational trophoblastic tumor. Gynecol Oncol. 2004;94(1):1870190.
Newlands ES, Holden L, Seckl MJ, et al. Management of brain metastases in patients with high-risk gestational trophoblastic tumors. J Reprod Med. 2002;47(6):465–71.
Tomoda Y, Arii Y, Kaseki S, et al. Surgical indications for resection in pulmonary metastasis of choriocarcinoma. Cancer. 1980;46(12):2723–30.
Grumbine FC, Rosenshein NB, Brereton HD, et al. Management of liver metastasis from gestational trophoblastic neoplasia. Am J Obstet Gynecol. 1980;137:959–96.
Yang J, Xiang Y, Wan X, et al. The prognosis of gestational trophoblastic neoplasia patient with residual lung tumor after completing treatment. Gynecol Oncol. 2006;103(2):479–82.
Mao Y, Wan X, Lv W, et al. Relapsed or refractory gestational trophoblastic neoplasia treated with the etoposide and cisplatin/etoposide, methotrexate, and actinomycin D (EP-EMA) regimen. Int J Gynaecol Obstet. 2007;98(1):44–7.
Lurain JR, Schink JC. Importance of salvage therapy in the management of high risk gestational trophoblastic neoplasia. J Reprod Med. 2012;57(5–6):219–24.
Osborne R, Covens A, Mirchandani D, et al. Successful salvage of relapsed high-risk gestational trophoblastic neoplasia patients using a novel paclitaxel-containing doublet. J Reprod Med. 2004;49(8):655–61.
Hoekstra AV, Lurain JR, Rademaker AW, et al. Gestational trophoblastic neoplasia: treatment outcomes. Obstet Gynecol. 2008;112(2 Pt 1):251–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Dickson, E.L., Mullany, S.A. (2015). Gestational Trophoblastic Disease. In: Eskander, R., Bristow, R. (eds) Gynecologic Oncology. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1976-5_5
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1976-5_5
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1975-8
Online ISBN: 978-1-4939-1976-5
eBook Packages: MedicineMedicine (R0)