
Abstract
There is growing interest in the role of nutrition in modifying the development and/or progression of vision disorders in older persons. Eye diseases of particular interest are agerelated cataract and macular degeneration. Deficiencies of certain nutrients can result in visual impairment or blindness. This review evaluates the role of dietary components in the prevention of onset or progression of ocular diseases in older adults. The nutrients of interest are vitamins C and E, lutein, zeaxanthin, omega-3 fatty acids, and zinc. The evidence to date points to beneficial effects of these key nutrient, however, it is not entirely consistent regarding the doses and combinations of nutrients which provide the optimal beneficial effects. It may be most practical to recommend specific food choices rich in vitamin C and E, lutein, zeaxanthin, omega-3 fatty acids and zinc, which may also provide additional benefits from other components from these food sources.
Similar content being viewed by others


Keywords
Key Points
-
There is growing interest in the role that nutrition plays in modifying the development and/or progression of vision disorders in older persons, including age-related cataract and macular degeneration.
-
Available evidence to date supports a possible protective role of several nutrients, including vitamins C and E, the carotenoids lutein and zeaxanthin, and the omega-3 fatty acids.
-
Due to inconsistencies among the findings of currently available studies regarding doses and combinations of nutrients, it may be most practical to recommend specific natural diet choices rich in vitamins C and E, lutein and zeaxanthin, omega-3 fatty acids and zinc, which would also provide potential benefits from other components of these natural food sources.
Introduction
Vision loss among the elderly is an important health problem. Approximately one person in three has some form of vision-reducing eye disease by the age of 65 [1]. Age-related cataract and age-related macular degeneration (AMD) are the major causes of visual impairment and blindness in the aging US population. Approximately 50 % of the 30–50 million cases of blindness worldwide result from unoperated cataracts [2, 3]. A clinically significant cataract is present in about 5 % of Caucasian Americans aged 52–64 years and rises to 46 % in those aged 75–85 years [4]. In the United States, cataract extraction accompanied by ocular lens implant is currently the most common surgical procedure done in Medicare beneficiaries [5]. Lens implantation is highly successful in restoring vision. However, the procedure is costly, accounting for 12 % of the Medicare budget and accounts for more than $3 billion in annual health expenditures [5, 6]. For these reasons, there is much interest in the prevention of cataract as an alternative to surgery.
The prevalence of AMD also increases dramatically with age. Nearly 30 % of Americans over the age of 75 have early signs of AMD and 7 % have late stage disease, whereas the respective prevalence among people 43–54 years are 8 and 0.1 % [4]. Dry AMD is the most common form of AMD in its early or intermediate stages. It occurs in about 90 % of the people with the condition. Wet AMD is more severe than the early and intermediate stages of the dry form. Wet AMD occurs when abnormal blood vessels behind the retina start to grow under the macula. These new blood vessels can be fragile and leak blood and fluid. The blood and fluid cause the macula to swell and damage occurs rapidly. The damage may also cause scarring of the retina.
AMD is the leading cause of blindness among the elderly in industrialized countries. Because there are currently no effective treatment strategies for most patients with AMD, attention has focused on efforts to stop the progression of the disease or to prevent the damage leading to this condition [7].
Cataract and AMD share common modifiable risk factors, such as light exposure and smoking [7, 8]. Of particular interest is the possibility that nutritional counseling or intervention might reduce the incidence or retard the progression of these diseases. The components of the diet that may be important in the prevention of cataract and AMD are vitamins C and E, the carotenoids, lutein and zeaxanthin, the omega-3 polyunsaturated fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), and zinc.
Both vitamins C and E are found in the lens [9–11]. Omega-3 fatty acids, lutein, and zinc are highly concentrated in the eye [12–15]. Given that the lens and retina suffer oxidative damage, some of these nutrients are thought to be protective through their role as antioxidants. Vitamin E and carotenoids are lipid-soluble oxidant scavangers that protect biomembranes. Vitamin C is an important water-soluble antioxidant and also promotes the regeneration of vitamin E. Of the 20–30 carotenoids found in human blood and tissues [16], only lutein and zeaxanthin are found in the lens and retina [10, 17]. Lutein and zeaxanthin are concentrated in the macula or central region of the retina and are referred to as macular pigment. In addition to their role as antioxidants, lutein and zeaxanthin are believed to limit retinal oxidative damage by absorbing incoming blue light and/or quenching reactive oxygen species. Many putative risk-factors for AMD have been linked to a lack of macular pigment, including female gender, lens density, smoking, light iris color, obesity, and reduced visual sensitivity [7, 18]. Given that inflammation is also a component to the etiology of age-related eye disease [13, 19], the omega-3 fatty acids are thought to be protective. It has been suggested that atherosclerosis of the blood vessels that supply the retina contributes to the risk of AMD, analogous to the mechanism underlying coronary heart disease [20]. Long-chain omega-3 fatty acids may have a special role in the function of the retina in addition to their antithrombotic and hypolipidemic effects on the cardiovascular system. DHA is the omega-3 fatty acid of key interest. DHA is a major fatty acid found in the retina [21]. Rod outer segments of vertebrate retina have a high DHA content [21, 22]. Since photoreceptor outer segments are constantly being renewed, a constant supply of DHA may be required for proper retinal function and a marginal depletion may impair retinal function and influence the development of AMD.
Physiological Basis of Cataracts and AMD
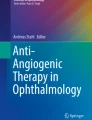
The role of the lens is to transmit and focus light on the retina. Therefore, for optimal performance the lens must be transparent. The lens is an encapsulated organ without blood vessels or nerves (Fig. 4.1). The anterior hemisphere is covered by a single layer of epithelial cells containing subcellular organelles. At the lens equator the epithelial cells begin to elongate and differentiate to become fiber cells. Fully differentiated fiber cells have no organelles but are filled with proteins called crystallins, organized in a repeating lattice. The high density and repetitive spatial arrangement of crystallins produce a medium of nearly uniform refractive index with dimensions similar to light wavelengths [23]. Cataracts result when certain events, e.g., light exposure, cause a loss of order and results in abrupt fluctuations in refractive index causing increased light scattering and loss in transparency in the lens. It is proposed that lens opacity results from damage to lens enzymes, proteins, and membranes by activated oxygen species, e.g., hydrogen peroxide, superoxide anion, and hydroxyl free radicals, which are the results of exposure to light and other types of radiation. There are three types of cataract, defined by their location in the lens. Nuclear cataract occurs in the center, or nucleus of the lens. Cortical cataract begins at the outer rim of the lens, which is referred to as the cortex, and progresses towards the center. Posterior subcapsular cataract (PSC) occurs in the central posterior cortex, just under the posterior capsule, the membrane that envelops the lens. Nuclear cataract is the most common type of cataract [1]. It interferes with a person’s ability to see distant objects and is usually the result of advancing age. Cortical cataract is most commonly seen in patients who have diabetes. PSC can be present in younger individuals and progresses more rapidly resulting in glare and blurriness [24]. This type of cataract is usually seen in patients who use steroids, or who suffer from diabetes or extreme nearsightedness.

The human eye showing typical organization and terminology. Courtesy of National Eye Institute, National Institute of Health
AMD is a disease affecting the central area of the retina (macula) (see Fig. 4.1) resulting in loss of central vision. In the early stages of the disease, lipid material (drusen) accumulates in deposits underneath the retinal pigment epithelium (RPE). This is believed to arise after failure of the RPE to perform its digestive function adequately and can be seen as pale yellow spots on the retina. The presence of a few small, hard drusen is normal with advancing age. However, the presence of indistinct, soft, larger, reticular, and more numerous drusen in the macula is a common early sign of AMD [25]. The pigment of the RPE may become disturbed with areas of hyperpigmentation and hypopigmentation. In the later stages of the disease, the RPE may atrophy completely. This loss can occur in small focal areas or can be widespread. In some cases, new blood vessels grow under the RPE and occasionally into the subretinal space (exudative or neovascular AMD). Hemorrhage can occur which often results in increased scarring of the retina. The early stages of AMD are in general asymptomatic. In the later stages there may be considerable distortion of vision and complete loss of visual function, particularly in the central area of vision [7]. Although the specific pathogenesis of AMD is still unknown, chemical and light-induced oxidative damage to the photoreceptors is thought to be important in the dysfunction of the RPE. The retina is particularly susceptible to oxidative stress because of its high consumption of oxygen, its high proportion of polyunsaturated fatty acids, and its exposure to visible light. Currently, there is no treatment which can restore vision in AMD. Therefore, efforts have focused on its prevention or delay in progression.
Given the role of light damage in the etiology of cataracts and AMD, many antioxidant nutrients may prevent damage in the lens by reacting with free radicals produced in the process of light absorption as well as decrease oxidative stress in photoreceptors in the retina.
Epidemiological Studies on Dietary Intake and Blood Levels of Nutrients and Eye Disease
Studies with human subjects provide information on the strength of associations between nutritional factors and the frequency of a disease. Such studies can be a valuable means of identifying and evaluating risk factors. Although there are limitations to such studies, consistency of findings among studies lends credibility to the role that nutrition can play in age-related eye health.
Cataract
Vitamin C
Several studies have found a relationship between increased dietary vitamin C and decreased risk of cataract (Table 4.1). For example, it was observed that the prevalence of nuclear cataract was lower for men with total vitamin C intakes in the highest quintile category relative to the lowest intake quintile [26]. It has also been observed that the prevalence of cataract was about 75 % lower in persons with vitamin C intakes >490 mg/day than in those with intakes <125 mg/day [27]. Others have reported that vitamin C intake had no effect on cortical cataract, posterior subcapsular (PSC) and cataract extraction [26, 28–32].
Compared to diet, plasma concentrations of a nutrient are considered to be a better measure of nutrient status. There are many reports of an inverse relationship between plasma ascorbic acid concentrations and the prevalence of cataract [27, 33–36]. For example, the National Health and Nutrition Examination Survey II (NHANES II) correlated a 1 mg/dL increase in plasma ascorbate with a 26 % decreased risk of cataracts in older (62–70 years) Americans [33]. However, others have observed that plasma vitamin C concentrations were not associated with risk of nuclear or cortical cataract [30, 37]. Furthermore, the India-United States case control study of age-related cataracts found an increased prevalence of (PSC) and nuclear cataracts with increased plasma vitamin C concentrations [38]. In this study, however, when vitamin C status was combined with other indicators of antioxidant status (glutathione peroxidase, vitamin E, and glucose-6-phosphate dehydrogenase) the relationship became significantly protective (Table 4.2). This may reflect the synergistic actions of antioxidant systems.
Vitamin E
A protective effect of dietary vitamin E has been observed in several studies (Table 4.3). Persons in the highest quintile for vitamin E intake were reported to be 50 % less likely to undergo cataract extraction compared to those in the lowest quintile for vitamin E intake [31]. Mares-Perlman et al. [26] observed a lower prevalence of nuclear cataract in men in the highest quintile category of total vitamin E intake relative to those in the lowest vitamin E intake. Similarly, Leske et al. [39] reported that persons with vitamin E intakes in the highest quintile category had an approximately 40 % lower prevalence of cataract relative to persons with intakes in the lowest quintile category. Jacques and Chylack [27] found that although persons with vitamin E intake greater than 35.7 mg/day had a 55 % lower prevalence of cataract than did persons with intakes less than 8.4 mg/day, a significant difference was not found. Two other studies also reported no difference in cataract prevalence between persons with high and low vitamin E intake [26, 29]. In the first of these two studies, the null relationship was in women only (in men, dietary vitamin E was protective). In the second study only women were studied.
Results from studies reporting relationships between plasma vitamin E and cataract have been mixed. In five of eight studies examining this issue, increased plasma vitamin E was observed to be protective against the risk of cataract [30, 40–43] (Table 4.4). However, one study observed that the prevalence of cataract was not related to plasma vitamin E concentrations [28] and one study observed that the prevalence of cortical cataract did not differ between those with high (>30 μmol/L) and low (<19 μmol/L) plasma vitamin E concentrations [30]. Mares-Perlman et al. reported a significantly increased prevalence of nuclear cataract among women and men in the highest serum vitamin E quintile relative to those in the lowest quintile. Several other studies have found increased levels of plasma alpha-tocopherol to be a risk factor for nuclear cataract [44], cortical [28, 37], and PSC cataracts [28]. These results are contrary to what would be expected. Because these are cross-sectional observational studies, there is the possibility that unadjusted confounding affected the findings.
Lutein and Zeaxanthin
The majority of the epidemiological data suggest that dietary lutein and zeaxanthin function in cataract prevention. The Melbourne Visual Impairment Study, an observational study of >3,000 over the age of 40 years, reported an inverse correlation between high lutein and zeaxanthin intake and the risk of nuclear cataracts [45].
Lower intake of lutein-rich foods, e.g., green leafy vegetables, was reported to be related to an increased rate of cataract extraction [29]. Similarly, it was observed that women in the highest quintile of lutein intake had a 27 % lower prevalence of nuclear cataract than those in the lowest lutein intake quintile [26]. In this study, this was not observed in men. In the Nurses’ Health Study, those with the highest quintile of intake of lutein and zeaxanthin had a 22 % decreased risk of cataract surgery and nuclear cataract compared with those in the lowest quintile after adjusting for other risk factors [46]. The intake of other dietary carotenoids was not associated with nuclear cataract. Similar findings were observed in the US male Health Professional’s prospective study, in which men in the highest fifth of lutein and zeaxanthin intake had a 19 % lower risk of cataract surgery relative to men in the lowest fifth. There was no relationship observed with the other carotenoids [47]. The Beaver Dam Eye Study found that the incidence of nuclear cataract in subjects in the highest quintile of lutein intake was half of that found in those in the lowest quintile [48]. Data from an observational study of 372 volunteers found that the risk of PSC cataract was lowest in those with the highest plasma concentrations of lutein [49]. There was no relationship between plasma lutein and zeaxanthin and cortical and PSC cataract. In a prospective observational study higher intakes of lutein and zeaxanthin from both food and supplements were significantly related to a 20 % decreased risk of cataract [50]. Delcourt et al. [51] observed a 75 % lower risk of nuclear cataracts among individuals with high plasma zeaxanthin, but not lutein, in a prospective study of 899 adults aged ≥60 years. A summary of studies evaluating the relationship between lutein and cataract is found in Table 4.5.
Omega-3 Fatty Acids
Cataract formation is associated with perturbations of lens membrane composition, structure, and function [52–54], as well as changes in fatty acid composition [55]. Studies in rats find that high intake of polyunsaturated fatty acids delays the cataract formation [56, 57]. High intakes of dietary omega-3 polyunsaturated fatty acids were shown to reduce the incidence of nuclear cataract in the Blue Mountains Eye Study cohort [58]. In a prospective study examining the relationship between dietary fat and cataract extraction in women (n = 71,083, 16-years follow-up), women in the highest quintile of long-chain omega-3 fatty acids (0.21 % of energy) had a 12 % lower risk of cataract extraction compared to those in the lowest quintile (0.03 % of energy) (relative risk = 0.88, 95 % CI: 0.79–0.98, p for trend = 0.02) [59]. Both Arnarsson et al. [60] and Cumming et al. [61] report that there was no association between the intake of foods or oils containing omega-3 fatty acids and age-related cataract prevalence.
AMD
Vitamin C
Seddon et al. [62] observed that persons in the highest and lowest intake quintiles for vitamin C had the same prevalence of advanced AMD. No relationship between dietary intake of vitamin C and cataract risk was observed in the Age-Related Eye Disease Study [63]. However, in that study results examining relationships between plasma levels of vitamin C and AMD suggests that increased plasma vitamin C may decrease the risk of AMD. West et al. [64] reported that individuals with plasma vitamin C concentrations >80 μmol/L had a 45 % lower prevalence of AMD compared with individuals who had concentrations <60 μmol/L. Others have reported that individuals with serum vitamin C concentrations ≥91 μmol/L had a 30 % lower prevalence of neovascular AMD compared with those who had concentrations <40 μmol/L [65] (Table 4.6).
Vitamin E
A protective effect of increased diet and plasma vitamin E against AMD has been found in some [62, 64, 65], but not in others [44, 66] (Table 4.7).
Lutein and Zeaxanthin
Findings from several case control studies suggest that high intakes of carotenoids, particularly lutein and zeaxanthin, are related to lower risk of advanced neovascular AMD [62, 65, 67]. A relationship between carotenoid status and age-related eye disease risk was evaluated in the Carotenoids in Age-Related Eye Disease Study (CAREDS), a cross sectional study of 1,678 women (54–86 years) [68]. In CAREDS, high dietary lutein and zeaxanthin were related to a decreased risk of intermediate AMD in women <75 years, but not in women ≥75 years [68]. Similarly, the Blue Mountain Eye Study found that high intake of lutein/zeaxanthin was related to a reduced risk of incident neovascular AMD and indistinct soft or reticular drusen over 5 and 10 years [69]. In the Age-Related Eye Diseases (AREDS) study, lutein/zeaxanthin intake was associated with a decreased risk of prevalent neovascular AMD and large or extensive intermediate drusen when comparing the highest and lowest quintiles of intakes [63]. However, a nested case control study from the Beaver Dam Eye Study found no difference in serum levels of lutein/zeaxanthin between early AMD and age-, sex-, and smoking-matched controls [44].
Evidence that high macular pigment concentrations may lower the risk of AMD comes from analysis of retinas from donors with AMD and controls for lutein and zeaxanthin [70]. Concentrations of lutein and zeaxanthin in retinal tissue were less, on average, for the AMD donors than for the controls. Macular pigment can be measured noninvasively in vivo [71]. In subjects (21–81 year) with healthy eyes and in healthy eyes of subjects at high-risk of AMD due to advanced disease in the fellow eye, at-risk eyes had significantly less macular pigment than eyes not at risk [72]. In another study, macular pigment in the eyes of AMD patients were 32 % lower in than that in healthy eyes [73]. In a prospective study in patients with early and late AMD, their children, and normal controls, it was found that macular pigment density was reduced in late AMD [74]. In contrast, in CAREDS, macular pigment density was not related to AMD [75]. Inconsistencies among studies may be due to the cross-sectional study design, suggesting that prospective studies are needed to determine if there is a relationship between AMD risk and macular pigment density. A summary of studies evaluating the relationship between lutein/zeaxanthin status and AMD risk is found in Table 4.8.
Omega-3 Fatty Acids
A meta-analysis, including nine prospective studies and three randomized clinical trials, reported that a high dietary intake of omega-3 fatty acids was associated with a 38 % reduction in the risk of late AMD [76]. Fish intake at least twice a week was associated with a 24 % reduced risk for early AMD and 33 % reduced risk for late AMD (pooled OR, 0.67; 95 % CI, 0.53–0.85). In a prospective follow-up study of the Nurses’ Health Study and the Health Professionals Follow-up Study, odds of AMD decreased with increased DHA intake. Consumption of >4 servings of fish per week was associated with a 35 % lower risk of AMD compared with ≤3 servings per month in pooled multivariate analysis [77]. Of the individual fish types examined, a significant inverse association was found only with tuna intake.
The Dietary Ancillary Study of the Eye Disease Case–Control Study [65] reported results for participants with neovascular AMD and control subjects without AMD [78]. In demographically adjusted analyses, increasing intake of linoleic acid (an unsaturated n-6 fatty acid) was significantly associated with higher prevalence of AMD (p for trend = 0.004). This association remained in multivariate analyses (p for trend = 0.02). However, intake of omega-3 fatty acids was not associated with AMD after controlling for confounding variables. When the study population was stratified by linoleic acid intake (≤5.5 or ≥5.6 g/day), the risk for AMD significantly decreased with high intake of omega-3 fatty acids only among those with low linoleic acid intake (p for trend = 0.05; p for continuous variable = 0.03). A prospective cohort study reported similar findings. In this study, 261 persons aged 60 years or older at baseline with an average follow-up of 4.6 years were evaluated for progression to late AMD. Higher fish intake was associated with a 64 % lower risk of progression to advanced AMD among subjects with lower linoleic acid intake [79]. Others have also observed a benefit of a high omega-3 fatty acid intake with low intake of linoleic acid [80]. These findings indicate an interaction or competition between omega-3 and omega-6 fatty acids such that both the levels of omega-3 fatty acids and its ratio to the n-6 acids may be important when considering the risk/benefit to AMD.
The Blue Mountain Eye Study was a population-based survey of vision, in which patients (≥49 years) were evaluated for AMD at baseline, 5 and 10 years after initial enrollment and energy-adjusted nutrient intakes were assessed for relationships with AMD risk [81]. In the 2,915 subjects, more frequent consumption of fish was related to a decreased risk of late AMD after adjusting for age, sex, and smoking. The protective effect of fish intake was observed at a relatively low consumption (1–3 times per month compared with intake <1 time per month (OR = 0.23, 95 % CI: 0.08–0.63 after adjusting for age, sex, and smoking). Although the OR was approximately 0.5 at higher intakes, this was not significant. There was little evidence of a decreased risk for early AMD with increased fish intake. A prospective cohort study from the AREDS trial found that increased intakes of omega-3 fatty acids reduced the risk by 30 % of developing central geographic atrophy and neovascular AMD [82].
In the Beaver Dam Eye Study, a retrospective population-based study, a relationship between fish intake, neovascular AMD, or geographic atrophy was not found. A null finding may be due to the observation that fish intakes were very low [83] and not varied enough to measure a difference in risk for AMD. In the NHANES III study, consuming fish more than once a week compared with once a month or less was not associated with either early or late AMD [84]. A summary of the studies that have evaluated the relationship between omega-3 fatty acids and AMD can be found in Table 4.9.
AREDS 2 clinical trial evaluated the benefit of 1 g eicosapentaenoic acid + DHA (2:1) on the progression to late AMD [85]. Addition of DHA + EPA to the AREDS formulation in primary analyses did not further reduce risk of progression to advanced AMD.
Zinc
In a study by Newsome et al. [85], zinc supplementation given to elderly people with early stages of AMD resulted in better maintenance of visual acuity than in those receiving placebo; scientific evidence that zinc intake is associated with the development or progression of AMD is limited. A recent study found zinc levels in the RPE and choroid to be reduced significantly by 24 % in AMD eyes compared to normal eyes, lending support to the possible importance of zinc in AMD [87].
In the Blue Mountain Eye Study, the relative risk comparing the top decile of zinc intake (≥15.8 mg/day) with the remaining population was 0.56 (95 % CI, 0.32–0.97) for all forms of AMD and 0.54 (95 % CI, 0.30–0.97) for early AMD. However, in two large prospective studies (Nurses’ Health Study and the Health Professionals Follow-up Study) involving men and women (n = 72,489) with no diagnosis of AMD at baseline, zinc intake, either in food or in supplements, was not associated with a reduced risk of AMD [88]. Furthermore, no association was observed between zinc intake and prevalence of AMD-related drusen in the cohort of the Nurses’ Health Study who also participated in the Nutrition and Vision project [89]. A protective effect of zinc is in contrast to the findings of high concentrations in sub RPE deposits, with levels being particularly high in eyes with AMD [14].
In summary, the studies examining dietary intakes of certain nutrients and eye disease relationships are not entirely consistent. Methodology differences among studies may, in part, explain the inconsistencies. Also, there are limitations to such studies that examine relationships between a nutrient and disease because calculations from dietary recall may not always accurately estimate nutrient intakes due to limitations of the database or recall abilities of the subjects. Furthermore, a single blood value for a nutrient may not always be an accurate indicator of long-term status. In addition, the high degree of correlation in intake among the various dietary micronutrients makes it difficult to determine which specific nutrient or nutrients are related to the observed relationships. Despite these drawbacks, a possible protective role of certain nutrients cannot be dismissed given the number of studies that found a protective effect and the comparatively fewer studies that found a negative effect. In some cases, it may be difficult to measure an outcome if nutrient intake levels are at those found in diet alone. That is, dietary and plasma levels may not be sufficiently high to see an effect. In this regard, review of studies that have examined the relationship between supplemental nutrient intake with cataract and AMD risk may be useful.
The Effect of Nutrient Supplements on Eye Disease Risk
Supplemental vitamins C and E have been long available to the general public. Currently, there are a variety of supplement products available in health food stores that contain lutein in amounts of 6–25 mg/capsule. At this point lutein can be found in a few multi-vitamin products. Centrum was the first multivitamin supplement with lutein and contains 250 μg per capsule. Alcon Laboratories and Bausch & Lomb have made available multivitamin supplements formulated for eye care. These products contain lutein in higher amounts.
Cataract
Jacques et al. [90] observed a >75 % lower prevalence of early opacities in women who used vitamin C supplement for ≥10 years (Table 4.10). None of the 26 women who used vitamin C supplements for ≥10 years had more advanced nuclear cataract. Hankinson et al. [29] observed that women who reported use of vitamin C supplement for ≥10 years had a 45 % reduction in rate of cataract surgery. The study of Robertson et al. [91] observed that the prevalence of cataract in persons who consumed vitamin C supplement of >300 mg/day was approximately one-third the prevalence in persons who did not consume vitamin C supplements. However, Chasen-Tabar et al. [92] prospectively examined the association between vitamin supplement intake and the incidence of cataract extraction during 12 years of follow-up in a cohort of 73,956 female nurses. After adjusting for cataract risk factors, including cigarette smoking, body mass index, and diabetes mellitus, there was no difference in the incidence of cataract between users of vitamin C supplements for 10 years or more and nonusers. There was an increased risk of cortical cataract in older women (≥60 years) who consumed vitamin C supplements for 5–9 years compared to the those taking vitamin C for 1–4 years, ≥10 years and those who never used vitamin C supplements [93]. Similarly, in a population-based, prospective study involving 24,593 women (≥65 years), a significantly higher risk of cataract was observed in those consuming ~1,000 mg vitamin C supplements but not among those consuming a multivitamin, which contain much lower levels of vitamin C [94]. However, such relationship was not always observed [28–31].
Nadalin et al. [95] cross-sectionally examined the association between prior supplementation with vitamin E and early cataract changes in volunteers (Table 4.11). Of 1,111 participants 26 % reported prior supplementation with vitamin E. Only 8.8 % of these participants took supplementation greater than the recommended daily intake (10 mg/day). A statistically significant association was found between prior supplementation and the absence of cortical opacity, after adjusting for age. However, the levels of nuclear opacity were not statistically different between those who reported intake and those with no prior vitamin E supplementation. Leske et al. [43] examined the association of antioxidant nutrients and risk of nuclear opacification in a longitudinal study. The risk of nuclear opacification at follow-up was decreased in regular users of multivitamin supplements, vitamin E supplements, and in persons with higher plasma levels of vitamin E. The investigators concluded that in regular users of multivitamin supplements, the risk of nuclear opacification was reduced by one-third. They also reported that in regular users of vitamin E supplement and persons with higher plasma levels of vitamin E, the risk was reduced by approximately half. These results are confirmed by Robertson et al. [91] who reported that the prevalence of cataract was 56 % lower in persons who consumed vitamin E supplement than in persons not consuming supplements. One study observed no relation between risk of cataract and vitamin E supplements [29, 95].
To date, there are few data from intervention trials of vitamins and cataract risk. There has been only one randomized, double-masked, placebo controlled trial evaluating a vitamin E intervention and cataract prevention. Pharmacological doses of vitamin E (500 IU) for 4 years was reported to reduce the incidence or progression of nuclear, cortical, or PSC cataracts in subjects aged 55–80 years [96]. This may provide the best evidence for a role for vitamin E in cataract prevention.
It was reported that a high dose combination of antioxidants (vitamins C and E, beta-carotene, and zinc) had no significant effect on the development or progression of cataract [97]. The LINXIAN trial [98] examined the role of antioxidants in prevention of cataract, and effect is not clear. The intervention was a combination dose of 14 vitamins and 12 minerals. Therefore, a specific role of any one nutrient could not be accurately evaluated. The multivitamin component demonstrated that nutrition can modify the risk of nuclear cataract, but specific nutrients were not evaluated. Also, the population examined had suboptimal nutritional intakes at the study start and the effect may have been due to a correction of certain nutrient deficiencies.
The Roche European-American Anticataract Trial (REACT) was carried out to examine if a mixture of oral antioxidant micronutrients (beta-carotene, 18 mg/day; vitamin C, 750 mg/day; vitamin E, 600 mg/day) would modify the progression of age-related cataract [99]. This was a multi-center prospective double-masked randomized placebo-controlled 3-year trial in 445 patients with early age-related cataract. REACT demonstrated a statistically significant positive treatment effect after 2 years for US patients and for both subgroups (US, UK) after 3 years, but no effect for the UK patients alone. The conclusion from this study was that daily supplementation with these nutrients for 3 years produced a small deceleration in progression of age-related cataract.
AMD
A recent study reported that high levels of antioxidants and zinc significantly reduce the risk of AMD and its associated vision loss [97]. In the AREDS study it was found that people at high risk for developing advanced stages of AMD (people with intermediate AMD or advanced AMD in one eye but not the other eye) lowered their risk by about 25 % when treated with a high-dose combination of vitamins C and E, beta-carotene, and zinc. In the same high risk group the nutrients reduced the risk of vision loss caused by advance AMD by about 19 % [97] (Table 4.12). For those subjects who had either no AMD or early AMD, the nutrients did not provide a measured benefit. Because single nutrients were not evaluated, specific effects could not be determined. AREDS 2 aimed to refine the findings of AREDS by including the xanthophylls lutein and zeathanxin as well as omega-3 fatty acids into the test formulation [100]. In secondary analysis, lutein and zeaxanthin supplements on top of the AREDS supplement lowered the progression to advanced AMD in persons with low dietary lutein and zeaxanthin [85].
It has been reported that the prevalence of AMD in persons who consumed vitamin C supplement for >2 years was similar to those who never took vitamin C supplements [65] (see Table 4.12). In a study conducted by Seddon et al. [101] the prevalence of AMD was also similar between those who took vitamin E supplement for >2 years and those who never took vitamin E supplements. The results of three double-masked, placebo-controlled primary prevention studies involving high doses of vitamin E and AMD found that there was no association of treatment group with any sign of AMD [102–104]. The Alpha-Tocopherol, Beta-Carotene trial evaluated the effect of nutritional antioxidants on AMD. Overall there were 728 people randomized to any antioxidant (alpha-tocopherol and/or β-carotene) and 213 to placebo. The results of this study found that there was no association of treatment group with any sign of maculopathy. There were 216 cases of the disease in the antioxidant groups and 53 in the placebo group. The majority of these cases were early age-related maculopathy. There was no association with the treatment group and development of early stages of the disease. The findings are similar when each of the antioxidant groups—alpha-tocopherol, beta-carotene, alpha-tocopherol + beta-carotene—are compared with placebo. Although this was a large, high quality study there were few cases of late AMD (14 cases in total) which means that the study had limited power to address the question as to whether supplementation prevents late AMD. Furthermore, the 5–8-year intervention with alpha-tocopherol and/or beta-carotene may not have been a long enough intervention period to assess a difference in the prevalence of late AMD. This study was conducted in Finnish male smokers and caution must be taken when extrapolating the findings to other geographical areas, to people in other age-groups, to women, and to nonsmokers. However, the incidence of AMD, particularly neovascular disease, is likely to be higher in smokers [105], which means that they provide a good population to demonstrate any potential protective effects of antioxidant supplementation.
As mentioned above, The AREDS 2 trial found that lutein and zeaxanthin supplements lowered the progression to advanced AMD in persons with low dietary lutein and zeaxanthin.
Zinc supplementation (100 mg zinc sulfate for 12–24 months) given to elderly people with early stages of AMD resulted in better maintenance of visual acuity than in those receiving placebo [86]. A more recent randomized, placebo-controlled study showed supplementation with 50 mg/day for 6 months of zinc monocysteine significantly improved macular function in persons with dry AMD [106]. However, patients with wet AMD in one eye had no positive effect on the other eye diagnosed with drusen after 200 mg/day zinc supplementation for 2 years [107].
In summary, of the studies that have examined nutrient supplement use vs. the risk of eye disease, it is difficult to determine if supplements provide any added protection against eye disease. The number of studies reporting a positive outcome, i.e., a decreased risk, was about the same as the number of null outcomes. Further, in a recent meta-analysis it was concluded that there is insufficient evidence to support the role of dietary antioxidants including the use of dietary antioxidant supplements for the primary prevention of AMD [108]. However, AREDS 1 and 2 strongly support the beneficial effects of supplementation with a combination of antioxidants on delaying the progression from intermediate to late AMD.
Clinical Recommendations/Treatment Guidelines
The inconsistencies among studies in terms of the amount of nutrient required for protection against eye disease makes it difficult to make specific recommendations for dietary intakes of these antioxidants. Therefore, it may be more practical to recommend specific food choices rich in vitamins C and E, lutein and zeaxanthin, omega-3 fatty acids and zinc, thereby benefiting from possible effects of the components in food that may also be important. This necessitates an awareness of dietary sources of nutritional antioxidants for both the patient and clinician. Good sources of vitamin C include citrus fruit, berries, tomatoes, and broccoli (Table 4.13). Good sources of vitamin E are vegetable oils, wheat germ, whole grain cereals, nuts, and legumes (Table 4.14). The two foods that were found to have the highest amount of lutein and zeaxanthin are kale and spinach (Table 4.15). Other major sources include broccoli, peas, and brussels sprouts. Fish oils are the primary source of omega-3 fatty acids (Table 4.16)
A healthy diet including a variety of fresh fruit and vegetables, legumes, fish, and nuts, will have many benefits, will not do any harm, and will be a good source of the antioxidant vitamins and minerals implicated (but not proven) in the etiology of cataract and age-related macular degeneration. There is no evidence that nutrient-dense diets high in these foods, which provide known and unknown antioxidant components, are harmful. In fact, intake of fruits and vegetables is associated with reduced risk of death due to cancer, cardiovascular disease, and all causes [109]. Thus, recommendations such as consuming a more nutrient-dense diet, i.e., lower in sweets and fats, and increasing levels of fruit and vegetable intake do not appear to be harmful and may have other benefits despite their unproven efficacy in preventing or slowing disease. Until the efficacy and safety of taking supplements containing nutrients can be determined, current dietary recommendations [110] are advised.
In addition to antioxidant vitamins, patients ask about a wide variety of unproven and often untested nutritional supplements. These include bilberries, shark cartilage, and Ginko biloba extract. Unfortunately, little is known about the effect of these products on cataract or AMD: no clinical trials have been conducted. Patients with eye disease who are offered these often expensive and sometimes risky treatments are given little information as to their benefit or risk. Patients should be advised to avoid unproven treatments.
Conclusion
The hypothesis that antioxidant nutrients may protect against the cataract and AMD is a plausable one given the role of oxidative damage in the etiology of these diseases. It is not known at what stage the protective effect may be important. The question that needs to be addressed is whether people who begin to consume antioxidant vitamins in their 60s and 70s alter their risk of age-related macular degeneration. Although data regarding the use of nutrient supplements suggest protection in cataract, the data are less convincing for AMD. The research to date has not sufficiently evaluated the effectiveness vs. safety of nutrient supplements. But advocating the use of nutrient supplementation must be done with a cautionary note given that there have been trials which have suggested that supplementation with beta-carotene may have an adverse effect on the incidence of lung cancer in smokers and workers exposed to asbestos [111, 112]. Clearly further trials are warranted to address the usefulness of nutrient supplementation in eye disease prevention.
It is likely that cataract and AMD develops over many years and the etiology of these diseases is due to many factors. There are likely to be differences in the potential protective effect of antioxidant supplementation depending on the stage of the disease. Future research needs to take into account the stage at which oxidative damage, and therefore antioxidant supplementation, may be important.
References
Congdon N, O’Colmain B, Klaver CCW, Klein R, Munoz B, Friedman DS, et al. Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol. 2004;122(4):477–85.
World Health Organization. Use of intraocular lenses in cataract surgery in developing countries. Bull World Health Organ. 1991;69:657–66.
Thylefors B, Negrel AD, Pararajasegaram R, Dadzie KY. Global data on blindness. Bull World Health Organ. 1995;69:115–21.
Prevalence of Blindness Data Tables (NEI Statistics and Data). National Eye Institute, National Institute of Health. 2004 [cited 7 June 2012]. Available from: http://www.nei.nih.gov/eyedata/
Javitt JC. Who does cataract surgery in the United States? Arch Ophthalmol. 1993;111:1329.
Steinberg EP, Javitt JC, Sharkey PD, Zuckerman A, Legro MW, Anderson GF, et al. The content and cost of cataract surgery. Arch Ophthalmol. 1993;111:1041–9.
Snodderly DM. Evidence for protection against age-related macular degeneration by carotenoids and antioxidant vitamins. Am J Clin Nutr. 1995;62(6 Suppl):1448S–61.
Taylor HR. Epidemiology of age-related cataract. Eye. 1999;13:445–8.
Taylor A, Jacques PF, Nadler S, Morrow F, Sulsky SI, Shepard D. Relationship in humans between ascorbic acid consumption and levels of total and reduced ascorbic acid in lens, aqueous humor and plasma. Curr Eye Res. 1991;10:751–9.
Yeum KJ, Taylor A, Tang G, Russell RM. Measurement of carotenoids, retinoids, and tocopherols in human lenses. Invest Ophthalmol Vis Sci. 1995;36:2756–61.
Yeum KJ, Shang F, Schalch W, Russell RM, Taylor A. Fat-soluble nutrient concentrations in different layers of human cataractous lens. Curr Eye Res. 1999;19:502–5.
Newsome DA, Oliver PD, Deupree DM, Miceli MV, Diamond JO. Zinc uptake by primate retinal pigment epithelium and choroid. Curr Eye Res. 1992;11:213–7.
SanGiovanni JP, Chew EY. The role of omega-3 long-chain polyunsaturated fatty acids in health and disease of the retina. Prog Retin Eye Res. 2005;24:87–138.
Lengyel I, Flinn JM, Peto T, Linkous DH, Cano K, Bird AC, et al. High concentration of zinc in sub-retinal pigment epithelial deposits. Exp Eye Res. 2007;84(4):772–80.
Bone RA, Landrum JT. Macular pigment in Henle fiber membranes: a model for Haidinger’s brushes. Vision Res. 1984;24:103–8.
Parker RS. Bioavailability of carotenoids. Eur J Clin Nutr. 1997;51:S86–90.
Bone RA, Landrum JT, Tarsis SL. Preliminary identification of the human macular pigment. Vision Res. 1985;25(11):1531–5.
Johnson EJ. Obesity, lutein metabolism, and age-related macular degeneration: a web of connections. Nutr Rev. 2005;63(1):9–15.
Hodge WG, Whitcher JP, Satariano W. Risk factors for age-related cataracts. Epidemiol Rev. 1995;17(2):336–46.
Sarks SH, Sarks JP. Age-related macular degeneration: atrophic form. In: Ryan SJ, Schachat SP, Murphy RM, editors. Retina. St. Louis: Mosby, Inc.; 1994. p. 149–73.
Fliesler SJ, Anderson RE. Chemistry and metabolism of lipids in the vertebrate retina. Prog Lipid Res. 1983;22(2):79–131.
Bazan NG, Reddy TS, Bazan HEP, Birkle DL. Metabolism of arachidonic and docosahexaenoic acids in the retina. Prog Lipid Res. 1986;25:595–606.
Benedek GB. Theory of transparency of the eye. Appl Opt. 1971;10:459–73.
Asbell PA, Dualan I, Mindel J, Brocks D, Ahmad M, Epstein S. Age-related cataract. Lancet. 2005;365(9459):599–609.
Facts about Age-Related Macular Degeneration. 2009 [cited 22 November 2011]. Available from: http://www.nei.nih.gov/health/maculardegen/armd_facts.asp#1
Mares-Perlman JA, Brady WE, Klein BE, Klein R, Haus GJ, Palta M, et al. Diet and nuclear lens opacities. Am J Epidemiol. 1995;141(4):322–34.
Jacques PF, Chylack Jr LT. Epidemiologic evidence of a role for the antioxidant vitamins and carotenoids in cataract prevention. Am J Clin Nutr. 1991;53:353S–5.
The Italian-American Cataract Study Group. Risk factors for age-related cortical, nuclear, and posterior subcapsular cataracts. Am J Epidemiol. 1991;133:541–53.
Hankinson SE, Stampfer MJ, Seddon JM, Colditz GA, Rosner B, Speizer FE, et al. Nutrient intake and cataract extraction in women: a prospective study. BMJ. 1992;305:244–51.
Vitale S, West S, Hallfrisch J, Alston CM, Wang F, Moorman C, et al. Plasma antioxidants and risk of cortical and nuclear cataract. Epidemiology. 1993;4:195–203.
Tavani A, Negri E, LaVeccia C. Food and nutrient intake and risk of cataract. Ann Epidemiol. 1996;6:41–6.
Tan AG, Mitchell P, Flood VM, Burlutsky G, Rochtchina E, Cumming RG, et al. Antioxidant nutrient intake and the long-term incidence of age-related cataract: the Blue Mountains eye study. Am J Clin Nutr. 2008;87(6):1899–905.
Simon JA, Hudes ES. Serum ascorbic acid and other correlates of self-reported cataract among older Americans. J Clin Epidemiol. 1999;52:1207–11.
Valero MP, Fletcher AE, DeStavola BL, Vioque J, Alepuz VC. Vitamin C is associated with reduced risk of cataract in a Mediterranean population. J Nutr. 2002;132:1299–306.
Dherani M, Murthy GVS, Gupta SK, Young IS, Maraini G, Camparini M, et al. Blood levels of vitamin C, carotenoids and retinol are inversely associated with cataract in a North Indian population. Invest Ophthalmol Vis Sci. 2008;49(8):3328–35.
Jalal D, Koorosh F, Fereidoun H. Comparative study of plasma ascorbic acid levels in senile cataract patients and in normal individuals. Curr Eye Res. 2009;34(2):118–22.
Ferrigno L, Aldigeri R, Rosmini F, Sperduto RD, Maraini G, Italian-American Cataract Study Group. Associations between plasma levels of vitamins and cataract in the Italian-american clinical trial of nutritional supplements and age-related cataract (CTNS): CTNS Report #2. Ophthalmic Epidemiol. 2005;12(2):71–80.
Mohan M, Sperduto RD, Angra SK, Milton RC, Mather RL, Underwood BA, et al. Indian-US case-control study of age-related cataracts. India-US case-control Study Group. Arch Ophthalmol. 1989;107:670–6.
Leske MC, Chylack Jr LT, Wu SY. The lens opacities case-control study. Risk factors for cataract. Arch Ophthalmol. 1991;109(2):244–51.
Knekt P, Heliovaara M, Rissenen A, Aronaa A, Aaran R. Serum antioxidant vitamins and risk of cataract. BMJ. 1992;304:1392–4.
Leske MC, Wu SY, Hyman L, Sperduto R, Underwood BA, Chylack LT, et al. Biochemical factors in the lens opacities case-control study. Arch Ophthalmol. 1995;113:1113–9.
Rouhiainen P, Rouhiainen H, Saloneen JT. Association between low plasma vitamin E concentrations and progression of early cortical lens opacities. Am J Epidemiol. 1996;114:496–500.
Leske MC, Chylack LT, He Q, Wu SY, Schofield F, Friend J, et al. Antioxidant vitamins and nuclear opacities: the longitudinal study of cataract. Ophthalmology. 1998;105:831–6.
Mares-Perlman JA, Brady WE, Klein R, Klein BE, Bowen P, Stacewicz-Sapuntzakis M, et al. Serum antioxidants and age-related macular degeneration in a population-based case-control study. Arch Ophthalmol. 1995;113(12):1518–23.
Vu HTV, Robman L, Hodge A, McCarty CA, Taylor HR. Lutein and zeaxanthin and the risk of cataract: the Melbourne visual impairment project. Invest Ophthalmol Vis Sci. 2006;47(9):3783–6.
Chasen-Taber L, Willett WC, Seddon JM, Stamper MJ, Rosner B, Colditz GA, et al. A prospective study of carotenoid and vitamin A intakes and risk of cataract extraction in US women. Am J Clin Nutr. 1999;70:517–24.
Brown L, Rimm EB, Seddon JM, Giovanucci EL, Chasen-Taber L, Speigelman D, et al. A prospective study of carotenoid intake and risk of cataract extraction in US men. Am J Clin Nutr. 1999;70:517–24.
Lyle BJ, Mares-Perlman JA, Klein BE, Klein R, Greger JL. Antioxidant intake and risk of incident age-related nuclear cataracts in the Beaver Dam eye study. Am J Epidemiol. 1999;149(9):801–9.
Gale CR, Hall NF, Phillips DIK, Martyn CN. Plasma antioxidant vitamins and carotenoids and age-related cataract. Ophthalmology. 2001;108:1992–8.
Christen WG, Liu S, Glynn RJ, Gaziano JM, Buring JE. Dietary carotenoids, vitamins C and E, and risk of cataract in women: a prospective study. Arch Ophthalmol. 2008;126(1):102–9.
Delcourt C, Carriere I, Delage M, Barberger-Gateau P, Schalch W, POLA Study Group. Plasma lutein and zeaxanthin and other carotenoids as modifiable risk factors for age-related maculopathy and cataract: the POLA Study. Invest Ophthalmol Vis Sci. 2006;47(6):2329–35.
Kistler J, Bullivant S. Structural and molecular biology of the eye lens membranes. Crit Rev Biochem Mol Biol. 1989;24:151–81.
Borchman D, Cenedella RJ, Lamba OP. Role of cholesterol in the structural order of lens membrane lipids. Exp Eye Res. 1996;62:191–7.
Simonelli F, Libondi T, Romano N, Nunziata G, D’Aloia A, Rinaldi E. Fatty acid composition of membrane phospholipids of cataractous human lenses. Ophthalmic Res. 1996;28:101–4.
Rosenfeld L, Spector A. Comparison of polyunsaturated fatty acid levels in normal and mature cataractous human lenses. Exp Eye Res. 1982;35:69–75.
Hatcher H, Andrews JS. Changes in lens fatty acid composition during galactose cataract formation. Invest Ophthalmol. 1970;9:801–6.
Hutton JC, Schofield PH, Williams JF, Regtop HL, Hollows FC. The effect of an unsaturated-fat diet on cataract formation in streptozotocin-induced diabetic rats. Br J Nutr. 1976;36:161–7.
Townend BS, Townend ME, Flood V, Burlutsky G, Rochtchina E, Wang JJ, et al. Dietary macronutrient intake and five-year incident cataract: the Blue Mountains eye study. Am J Ophthalmol. 2007;143(6):932–9.
Lu M, Cho E, Taylor A, Hankinson SE, Willett WC, Jacques PF. Prospective study of dietary fat and risk of cataract extraction among US women. Am J Epidemiol. 2005;161(10):948–59.
Arnarsson A, Jonasson F, Sasaki H, Ono M, Jonsson V, Kojima M, et al. Risk factors for nuclear lens opacification: the Reykjavik eye study. Dev Ophthalmol. 2002;35:12–20.
Cumming RG, Mitchell P, Smith W. Diet and cataract: the Blue Mountains eye study. Ophthalmology. 2000;107(3):450–6.
Seddon JM, Ajani UA, Sperduto RD, Hiller R, Blair N, Burton TC, et al. Dietary carotenoids, vitamins A, C, and E, and advanced age-related macular degeneration. Eye Disease Case-Control Study Group. JAMA. 1994;272(18):1413–20.
Age-Related Eye Disease Study Research Group, SanGiovanni JP, Chew EY, Clemons TE, Ferris III FL, Gensler G, et al. The relationship of dietary carotenoid and vitamin A, E, and C intake with age-related macular degeneration in a case-control study: AREDS Report No. 22. [see comment]. Arch Ophthalmol. 2007;125(9):1225–32.
West S, Vitale S, Hallfrisch J, Munoz B, Muller D, Bressler S, et al. Are antioxidants or supplements protective for age-related macular degeneration? Arch Ophthalmol. 1994;112(2):222–7.
Eye Disease Case-Control Study Group, (EDCCSG). Antioxidant status and neovascular age-related macular degeneration. Arch Ophthalmol. 1993;111:104–9.
Sanders TAB, Haines AP, Wormald R, Wright LA, Obeid O. Essential fatty acids, plasma cholesterol, and fat-soluble vitamins in subjects with age-related maculopathy and matched control subjects. Am J Clin Nutr. 1993;57:428–33.
Snellen EL, Verbeek AL, Van Den Hoogen GW, Cruysberg JR, Hoyng CB. Neovascular age-related macular degeneration and its relationship to antioxidant intake. Acta Ophthalmol Scand. 2002;80(4):368–71.
Moeller SM, Parekh N, Tinker L, Ritenbaugh C, Blodi B, Wallace RB, et al. Associations between intermediate age-related macular degeneration and lutein and zeaxanthin in the carotenoids in age-related Eye disease study (CAREDS): ancillary study of the Women’s health initiative. Arch Ophthalmol. 2006;124(8):1151–62.
Tan JSL, Wang JJ, Flood V, Rochtchina E, Smith W, Mitchell P. Dietary antioxidants and the long-term incidence of age-related macular degeneration: the Blue Mountains eye study. Ophthalmology. 2008;115(2):334–41.
Bone RA, Landrum JT, Mayne ST, Gomez CM, Tibor SE, Twaroska EE. Macular pigment in donor eyes with and without AMD: a case-control study. Invest Ophthalmol Vis Sci. 2001;42(1):235–40 [Erratum appears in Invest Ophthalmol Vis Sci. 2001;42(3):548].
Wooten BR, Hammond BR, Land RI, Snodderly DM. A practical method for measuring macular pigment optical density. Invest Ophthalmol Vis Sci. 1999;40:2481–9.
Beatty S, Murray IJ, Henson DB, Carden D, Koh H, Boulton ME. Macular pigment and risk for age-related macular degeneration in subjects from a Northern European population. Invest Ophthalmol Vis Sci. 2001;42(2):439–46.
Bernstein PS, Shao D-Y, Wintch SW. Resonance Raman measurement of macular carotenoids in normal subjects and in age-related macular degeneration patients. Ophthalmology. 2002;109:1780–7.
Schweitzer D, Lang GE, Remsch H, Beuerman B, Hammer M, Thamm E, et al. Age-related maculopathy. Comparative studies of patients, their children and healthy controls. (German). Ophthalmologe. 2000;97:84–90.
LaRowe TL, Mares JA, Snodderly DM, Klein ML, Wooten BR, Chappell R, et al. Macular pigment density and age-related maculopathy in the carotenoids in age-related eye disease study. An ancillary study of the women’s health initiative. Ophthalmology. 2008;115(5):876–83.e1.
Chong EWT, Kreis AJ, Wong TY, Simpson JA, Guymer RH. Dietary omega-3 fatty acid and fish intake in the primary prevention of age-related macular degeneration. Arch Ophthalmol. 2008;126(6):826–33.
Cho E, Hung S, Willett WC, Spiegelman D, Rimm EB, Seddon JM, et al. Prospective study of dietary fat and the risk of age-related macular degeneration. Am J Clin Nutr. 2001;73:209–18.
Seddon JM, Rosner B, Sperduto RD, Yannuzzi L, Haller JA, Blair NP, et al. Dietary fat and risk for advanced age-related macular degeneration. Arch Ophthalmol. 2001;119:1191–9.
Seddon JM, Cote J, Rosner B. Progression of age-related macular degeneration. Association with dietary fat, trans unsaturated fat, nuts and fish intake. Arch Ophthalmol. 2003;121:1728–37.
Tan JSL, Wang JJ, Flood V, Mitchell P. Dietary fatty acids and the 10-year incidence of age-related macular degeneration: the Blue Mountains eye study. Arch Ophthalmol. 2009;127(5):656–65.
Smith W, Mitchell P, Leeder SR. Dietary fish and fish intake and age-related maculopathy. Arch Ophthalmol. 2000;118:401–4.
Sangiovanni JP, Agron E, Meleth AD, Reed GF, Sperduto RD, Clemons TE, et al. {omega}-3 Long-chain polyunsaturated fatty acid intake and 12-y incidence of neovascular age-related macular degeneration and central geographic atrophy: AREDS report 30, a prospective cohort study from the age-related eye disease study. Am J Clin Nutr. 2009;90(6):1601–7.
Mares-Perlman JA, Brady WE, Klein R, VandenLangenberg GM, Klein BE, Palta M. Dietary fat and age-related maculopathy. Arch Ophthalmol. 1995;113:743–8.
Heuberger RA, Mares-Perlman JA, Klein R, Klein BE, Millen AE, Palta M. Relationship of dietary fat to age-related maculopathy in the Third National Health and Nutrition Examination Survey. Arch Ophthalmol. 2001;119(12):1833–8.
Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the age-related eye disease study 2 (AREDS2) randomized clinical trial. JAMA. 2013;309(19):2005–15.
Newsome DA, Swartz M, Leone NC, Elston RC, Miller E. Oral zinc in macular degeneration. Arch Ophthalmol. 1988;106(2):192–8.
Erie JC, Good JA, Butz JA, Pulido JS. Reduced zinc and copper in the retinal pigment epithelium and choroid in age-related macular degeneration. Am J Ophthalmol. 2009;147(2):276–82.e1.
Cho E, Stampfer MJ, Seddon JM, Hung S, Spiegelman D, Rimm EB, et al. Prospective study of zinc intake and the risk of age-related macular degeneration. Ann Epidemiol. 2001;11:328–36.
Morris MS, Jacques PF, Chylack LT, Hankinson SE, Willett WC, Hubbard LD, et al. Intake of zinc and antioxidant micronutrients and early age-related maculopathy lesions. Ophthalmic Epidemiol. 2007;14(5):288–98.
Jacques PF, Taylor A, Hankinson SE, Lahav M, Mahnken B, Lee Y, et al. Long-term vitamin C supplement and prevalence of age-related opacities. Am J Clin Nutr. 1997;66:911–6.
Robertson JM, Donner AP, Trevithick JR. Vitamin E intake and risk of cataracts in humans. Ann N Y Acad Sci. 1989;570:372–82.
Chasan-Taber L, Willett WC, Seddon JM, Stamper MJ, Rosner B, Colditz GA. A prospective study on vitamin supplement intake and cataract extraction among US women. Epidemiology. 1999;10:679–84.
Gritz DC, Srinivasan M, Smith SD, Kim U, Lietman TM, Wilkins JH, et al. The antioxidants in prevention of cataracts study: effects of antioxidant supplements on cataract progression in South India. Br J Ophthalmol. 2006;90(7):847–51.
Rautiainen S, Lindblad BE, Morgenstern R, Wolk A. Vitamin C supplements and the risk of age-related cataract: a population-based prospective cohort study in women. Am J Clin Nutr. 2010;91(2):487–93.
Nadalin G, Robman LD, McCarty CA, Garrett SK, McNeil JJ, Taylor HR. The role of past intake of vitamin E in early cataract changes. Ophthalmic Epidemiol. 1999;6:105–12.
McNeil JJ, Robman L, Tikellis G, Sinclair MI, McCarty CA, Taylor HR. Vitamin E supplementation and cataract: randomized controlled trial. Ophthalmology. 2004;111(1):75–84.
Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001;119(10):1417–36 [Erratum appears in Arch Ophthalmol. 2008;126(9):1251].
Sperduto RD, Hu TS, Milton RC, Zhao JL, Everett DF, Cheng QF, et al. The Linzian cataract studies. Two nutrition intervention trials. Arch Ophthalmol. 1993;111:1246–53.
Chylack LTJ, Brown NB, Bron A, Hurst M, Kopcke W, Thien U, et al. The Roche European American cataract trial (REACT): a randomized clinical trial to investigate the efficiency of a antioxidant micronutrient mixture to slow progression of age-related cataract. Ophthalmic Epidemiol. 2002;9:49–80.
Age-Related Eye Disease Study 2 (AREDS2). [cited 9 May 2013]. Available from: www.nei.nih.gov/areds2
Seddon JM, Christen WG, Manson JE, LaMotte FS, Glynn RJ, Buring JE, et al. The use of vitamin supplements and the risk of cataract among US male physicians. Am J Public Health. 1994;84(5):788–92.
Christen WG, Glynn RJ, Chew EY, Buring JE. Vitamin E and age-related macular degeneration in a randomized trial of women. Ophthalmology. 2010;117(6):1163–8.
Taylor HR, Tikellis G, Robman LD, McCarty CA, McNeil JJ. Vitamin E supplementation and macular degeneration: randomised controlled trial. BMJ. 2002;325(7354):11.
Teikari JM, Laatikaineen L, Virtamo J, Haukka J, Rautalahti M, Liesto K, et al. Six-year supplementation with alpha-tocopherol and beta-carotene and age-related maculopathy. Acta Ophthalmol Scand. 1998;76:224–9.
Solberg Y, Posner M, Belkin M. The association between cigarette smoking and ocular diseases (review). Surv Ophthalmol. 1998;42:535–47.
Newsome DA. A randomized, prospective, placebo-controlled clinical trial of a novel zinc-monocysteine compound in age-related macular degeneration. Curr Eye Res. 2008;33(7):591–8.
Stur M, Tittl M, Reitner A, Meisinger V. Oral zinc and the second eye in age-related macular degeneration. Invest Ophthalmol Vis Sci. 1996;37(7):1225–35.
Chong EWT, Wong TY, Kreis AJ, Simpson JA, Guymer RH. Dietary antioxidants and primary prevention of age related macular degeneration: systematic review and meta-analysis. [see comment]. BMJ. 2007;335(7623):755.
Kris-Etherton PM, Hecker KD, Bonanome A, Coval SM, Binkoski AE, Hilpert KF, et al. Bioactive compounds in foods: their role in the prevention of cardiovascular disease and cancer. Am J Med. 2002;113(Suppl 9B):71S–88.
USDA. Dietary Guidelines for Americans 2005. http://www.health.gov/dietaryguidelines/dga2005/document/
The Alpha-Tocopherol Beta-Carotene Cancer Prevention Study Group. The effect of vitamin E and beta-carotene on the incidence of lung cancer and other cancers in male smokers. N Engl J Med. 1994;330:1029–35.
Omenn GS, Goodman GE, Thornquist MD, Balmes J, Cullen MR, Glass A, et al. Risk factors for lung cancer and for intervention effects in CARET, the beta-carotene and retinol efficiency trial. J Natl Cancer Inst. 1996;88:1550–9.
Nourmohammadi I, Modarress M, Khanaki K, Shaabani M. Association of serum alpha-tocopherol, retinol and ascorbic acid with the risk of cataract development. Ann Nutr Metab. 2008;52(4):296–8.
Lyle BJ, Mares-Perlman JA, Klein BE, Klein R, Palta M, Bowen PE, et al. Serum carotenoids and tocopherols and incidence of age-related nuclear cataract. Am J Clin Nutr. 1999;69(2):272–7.
USDA ARS Nutrient Data Laboratory. National Nutrient Database for Standard Reference. 2010 [cited 1 November 2010]. Available from: www.nal.usda.gov/fnic/foodcomp/search/
US Department of Agriculture. USDA-NCC Carotenoid Database for US Foods—1 Nov 1998. 2012. Available from: www.ars.usda.gov/SP2UserFiles/Place/12354500/Data/SR25/nutrlist/sr25a338.pdf
Kris-Etherton PM, Taylor DS, Yu-Poth S, Huth P, Moriarty K, Fishell V, et al. Polyunsaturated fatty acids in the food chain in the United States. Am J Clin Nutr. 2000;71:179S–88.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Johnson, E.J. (2015). Nutrition and the Aging Eye. In: Bales, C., Locher, J., Saltzman, E. (eds) Handbook of Clinical Nutrition and Aging. Nutrition and Health. Humana Press, New York, NY. https://doi.org/10.1007/978-1-4939-1929-1_4
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1929-1_4
Published:
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-4939-1928-4
Online ISBN: 978-1-4939-1929-1
eBook Packages: MedicineMedicine (R0)