
Abstract
Vitamin D was discovered as a result of its ability to cure rickets, but recently a wide range of other functions for it in the human body has been suggested. Vitamin D is not a vitamin in the strict sense as it can be synthesised in the human body following exposure of the skin to ultraviolet radiation. Provitamin D (7-dehydrocholesterol) is converted to previtamin D which is further modified by a series of reactions to the active form, 1,25-dihydroxyvitamin D. This Chapter summarises the discovery of vitamin D and reviews the chemistry and photochemistry of its precursors, transformations and metabolites. The production of vitamin D in various human populations is described, and how to assess vitamin D status. The skeletal and non-skeletal effects of vitamin D are discussed, particularly its role in immunomodulation with consequences for protection against a variety of human diseases. The Chapter concludes with evolutionary aspects, the occurrence and role of vitamin D in the plant kingdom, biogeographical considerations, and the nonphotochemical production of vitamin D in certain plants.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
23.1 Introduction
Some of us remember how we were forced to swallow a spoonful of cod liver oil every day and were told that it contained vitamin D and that we had to eat it to get good bones. At that time, we did not wonder why it was in the cod or how it got there.
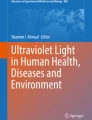
The early research history relating to vitamin D has been recounted many times, for instance, by DeLuca (1997), and only a short summary will be given here. Rickets was first described in England by Whistler (1645) and Glisson (1650). In the next century, Sniadecki established a connection between skeleton malformation and lack of sunlight among children in Warsaw (Mozolowski 1939). The disease became known as the English disease in many countries. Mellanby (1918) demonstrated that rickets (Fig. 23.1) could be prevented in dogs by supplementing their diet with cod liver oil, and Hess and Unger (1921) showed that rickets could be cured by sunlight. Hess and Weinstock (1924) and Steenbock and Black (1924) showed that the exposure of lettuce and several other foodstuffs to radiation from a mercury vapour lamp would render them antirachitic.

X-ray plates showing signs of vitamin D deficiency (rickets): incomplete bone formation in the wrist and knee and malformed legs in a child (Courtesy Dr. Michael L. Richardson, University of Washington Department of Radiology)
Several treatises on medical aspects of vitamin D are available, e.g. DeLuca (1997), Feldman, Glorieux and Pike (2005), Holick (2010), Bouillon et al. (2004), Lips (2006), and Norman (2006). Many later reviews deal with various special aspects of vitamin D, such as the molecular mechanisms of action (Haussler et al. 2013). Here vitamin D will be considered broadly covering not only medical aspects but also photochemistry, its role in non-human organisms, and evolutionary, ecological, and biogeographical aspects.
23.2 Chemistry and Photochemistry of Provitamin and Vitamin D
There are at least two kinds of vitamin D (also called calciferol), i.e. vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol), with slightly different structures (Fig. 23.2). The reason that there is no vitamin D1 is that the product first given this name turned out not to be a single compound but a mixture. In some non-mammal vertebrates, other compounds act in a similar way as vitamins D2 and D3 (Holick 1989), but they have not been chemically defined. In most organisms, the synthesis of vitamin D requires UV-B radiation. Exceptions to this rule will be described later. Vitamin D is formed from the provitamins (provitamin D2, also called ergosterol, and provitamin D3, also called 7-dehydrocholesterol). UV-B radiation can photoisomerise the provitamins to the corresponding previtamins, either in vivo without the mediation of any enzyme or in solution. The previtamins are slowly converted by a nonenzymatic and non-photochemical reaction to the vitamins (Fig. 23.2).

The structure of the two types of provitamin D: the reversible photoconversion of provitamin D3 to previtamin D3 and the reversible thermochemical conversion of previtamin D3 to vitamin D3
Provitamin D3 is synthesised in the upper layers of the human skin. Exposure to sunlight converts it to previtamin D3, which is in turn converted to vitamin D3. Since a vitamin is defined as a substance necessary for health which cannot be synthesised by the body and must be ingested with the food, vitamin D is, strictly speaking, not a vitamin. Since, however, exposure to sunlight can be insufficient for maintaining health and deficiency can be prevented by vitamin D in food, the vitamin status is defendable.
The recommended daily intake of vitamin D has been gradually raised, for instance, during 2013 in Sweden from 7.5 to 10 μg/day (and from 10 to 20 μg/day for the elderly). This is insufficient for prevention of deficiency if exposure to UV-B radiation does not supplement the intake. It was found, e.g. that Moslems in Denmark were still deficient after taking 15 μg/day (Glerup et al. 2000). Attempts to avoid the need for UV exposure by high daily intake (over 50 μg daily) cannot be recommended, as this can lead to vitamin D intoxication. Exposure even to high daily fluence of UV-B radiation can never lead to vitamin D overdosage, as will be explained below.
As mentioned, the vitamin D precursor previtamin D is formed from provitamin D by a photochemical reaction (Figs. 23.2 and 23.3) driven by UV radiation (UV-B in the natural condition, but UV-C can also be used artificially). But this is far from the only UV-driven reaction in the vitamin D context. The basic photochemistry of the vitamin D system was summarised by Havinga (1973). Previtamin D is also sensitive to UV radiation and can undergo three different photoreversible photochemical reactions. It can be either reconverted to provitamin D or converted to lumisterol or tachysterol and further irreversibly to products known under the common name of toxisterols (Boomsma et al. 1975). Vitamin D is sensitive to UV radiation and can be photoconverted to three compounds: 5,6-trans-vitamin D3, suprasterol 1, and suprasterol 2 (Webb et al. 1989).

The reversible conversions of previtamin D with quantum yields of the photochemical reactions. Previtamin D can also be photochemically converted to various compounds termed toxisterols (not shown) (From Havinga (1973), modified)
Havinga (1973) states that the quantum yields are independent of wavelength or at least have the same values at 254 and 313 nm. There is, however, as will be detailed below, an important exception to this rule. Although some literature sources give values slightly different from those of Fig. 23.3, there is no indication of differences in quantum yield between the D2 and D3 series.
Provitamin D3 is present in mammalian skin not only in free form but also esterified with fatty acids, and the esterified provitamin is transformed to esterified vitamin D3 upon exposure to UV radiation (Takada 1983). In fact, most of the provitamin and vitamin D in rat skin is in the esterified form.
A number of authors (reviewed by Dmitrenko et al. 2001) have found curious behaviour for the quantum yield of the photochemical ring closure of previtamin D (ring closure results in either conversion back to provitamin D or to formation of lumisterol, which has the same structure as provitamin D except for the direction of a methyl group, which is up for previtamin D in Fig. 23.2, down for lumisterol). This quantum yield increases slowly with wavelength from 295 to 302 nm but then doubles from 0.08 at 302 nm to 0.16 at 305 nm and then increases steadily to 0.29 at 325 nm. The quantum yield of cis-trans isomerisation to tachysterol decreases correspondingly over the same wavelength range. Various explanations for this behaviour have been advanced (see Dmitrenko et al. 2001 for further literature).
There are more complications to this photochemical system, which at first glance looks rather simple. It was found that the thermochemical step forming vitamin D, following the photochemical conversion of provitamin D, takes place more quickly in cells than in solutions (Tian et al. 1993; Holick et al. 1995). The reason for this is the existence of the conformer of previtamin D (lower right, Fig. 23.3 Dmitrenko et al. 2001). In solution, this is the preferred conformer, and it cannot be converted directly to vitamin D. In membranes, both natural and artificial liposome membranes (Tian and Holick 1999), the previtamin is held in the active, vitamin-producing conformer (cf. Saltiel et al. 2003). The same effect can be achieved by complexing the previtamin with β-cyclodextrin (Tian and Holick 1995).
Provitamins, previtamins, and vitamin D occur not only in free form but as glycosides in plants and in mammal skin also as fatty acid esters (Takada 1983). In rat skin, at least 80 % of the provitamin D3 is esterified, and upon exposure of the skin to UV radiation, the provitamin D3 ester is converted to vitamin D3 ester.
The action spectrum for conversion of provitamin D3 to previtamin D3 in human skin has been determined by MacLaughlin et al. (1982). It has a single peak at about 297 nm that roughly corresponds to the long-wavelength absorption band of provitamin D3 dissolved in n-hexane (Fig. 23.4). A digitised version with a long-wavelength extrapolation to 329.5 nm, having a maximum value at 297.5 nm (Bouillon et al. 2006), has been adopted by CIE (Comité International de l’Éclairage) as an official reference spectrum. This spectrum should be regarded as tentative, and there is reason to use it with caution (Norval et al. 2010). The absorption spectrum for provitamin D3 is three-peaked, but the two short-wave absorption bands are lacking in the action spectrum. Two circumstances could contribute to this lack: (1) the stratum corneum of the skin could filter the shorter wavelength components, and (2) since at the shorter wavelengths both provitamin and previtamin absorb but at the longer wavelengths (around 295 nm) only provitamin and tachysterol, the conversion of provitamin to previtamin is favoured at long wavelengths, while at shorter wavelengths the back and side reactions of previtamin are important competitors. Probably, under the conditions in which the action spectrum was determined, the first reason is more important.

Lehmann et al. (2001) measured the action spectra for formation of vitamin D3 as well as 1,25(OH)2D3 (1α,25-dihydroxyvitamin D3) from provitamin D3 in “artificial skin” containing cultured human keratinocytes. Remarkably, this action spectrum is displaced about 5 nm towards longer wavelength (peaking at about 302 nm) compared to the spectrum determined by MacLaughlin et al. (1982). Although no wavelength below 285 nm was tested, the spectrum indicates a rise from 293 nm towards shorter wavelengths. The minimum at approximately 293 nm is deeper than would be expected from the provitamin D3 absorption spectrum. Takada et al. (1979) investigated the spectral dependence of vitamin D3 formation in shaved cat skin. They found a maximum at 303 nm, similar to Lehmann et al. (2001). Their long-wavelength tail extends all the way to 340 nm. However, their spectrum must be regarded as very approximate, since it is plotted as effect at constant fluence, and the spectral bandwidth of the radiation is not stated. As the spectra of MacLaughlin et al. (1982) and Lehmann et al. (2001), it is plotted on an energy rather than photon basis and, therefore, not expected to match an absorption spectrum exactly. Knudson and Benford (1938) compared the effectiveness of different UV wavebands in preventing rickets in shaved rats. They found a peak at approximately the same wavelength as MacLaughlin et al. (1982) but also a (higher) peak at about 280 nm.
23.3 Production of the Active Form of Vitamin D in Humans
Exposure to the UV-B component in sunlight induces the production of previtamin D3 from 7-dehydrocholesterol in the membranes of keratinocytes in the epidermis (Fig. 23.5). Vitamin D3 (cholecalciferol) is then formed by a thermochemical reaction. Vitamin D3 attaches to the vitamin D-binding protein (Gc-globulin) and enters the blood stream. In the liver it undergoes hydroxylation by the 25-hydroxylase enzyme, CYP27A1, to produce 25-hydroxyvitamin D3 [25(OH)D3] (calcidiol). A second hydroxylation step takes place in the kidney by the enzyme 1α-hydroxylase enzyme, CYP27B1, to form 1,25(OH)2D3 (calcitriol) which is the active form of vitamin D. 1,25(OH)2D3 can interact with the nuclear vitamin D receptor (VDR) present in many cell types in the body, thus affecting the transcription of more than 2,000 genes. 1,25(OH)2D3 also induces rapid response signalling through a specific membrane receptor, recently identified as a protein disulfide isomerase, Pdia3 (Doroudi et al. 2014). The amount of circulating 1,25(OH)2D3 is tightly regulated by negative feedback control through induction by the hormone of 24-hydroxylase which catabolises both 25(OH)D3 and 1,25(OH)2D3 into various calcitonic acid products. There is limited evidence that 1,25(OH)2D3 can be formed entirely in the epidermis following exposure to UV-B radiation.

Metabolic pathway leading to the synthesis of the active form of vitamin D3, 1,25-dihydroxyvitamin D3, following solar UV-B irradiation of the skin
The quantity of solar UV-B radiation reaching the Earth’s surface varies hugely depending on many factors including the solar zenith angle. This is highest in the summer months and decreases to 5 % of this value at mid-latitudes in the winter and is zero at higher latitudes. One recent study illustrates clearly how the solar UV-B irradiation affects the vitamin D status of a population. In the USA, the peak in vitamin D levels was found in August and the trough in February, a lag of 8 weeks after the peak and trough respectively in ambient UV-B (Kasahara et al. 2013). The solar zenith angle also explains why at least 50 % of the daily UV radiation is found in the 4 h period around local noon. Other environmental variables are ozone, cloud cover, air pollution, altitude, and surface reflection, such as from snow or choppy water. There are also large differences between individuals in their ability to produce active vitamin D following a given dose of solar UV-B. These include skin type, age, amount of clothing worn and head cover, use of sunscreen, body mass index, serum cholesterol level, polymorphisms in VDR and enzymes of the vitamin D pathway, and baseline 25(OH)D. For example, to synthesise the same amount of previtamin D3, about a sixfold higher dose of UV-B is required for black skin compared with fair skin (due to absorption by melanin) (Clemens et al. 1982), and a twofold higher dose is required for an 80-year-old compared with a 20-year-old (due to the reduction in 7-dehydrocholesterol in older skin) (MacLaughlin and Holick 1985).
23.4 Vitamin D Status and Optimal Levels for Sufficiency
The assessment of vitamin D status is routinely carried out by measurement of the concentration of 25(OH)D in serum or plasma. The methods include chemiluminescence and radioimmunoassay, but these are recognised to lack accuracy, reproducibility, and sensitivity (Lai et al. 2012). Liquid chromatograph-tandem mass spectroscopy (LC-MS/MS) can distinguish between 25(OH)D2 (produced after consuming plants and vitamin D2 supplements) and 25(OH)D3 and is rapidly becoming the method of choice. A vitamin D standardisation programme is underway using LC-MS/MS to ensure consistency in the measurements of 25(OH)D globally.
There is no consensus at present on the reference values that define a “satisfactory” vitamin D status, and indeed, the optimal range may differ between the skeletal and nonskeletal functions of vitamin D and between one individual and another. In the 1990s, the threshold for deficiency was frequently defined as <25 nmol/L 25(OH)D. In 2010, the US Institute of Medicine defined sufficiency as a serum concentration of 50 nmol/L or above for both adults and children (Institute of Medicine 2011). Others working in the area recommend much higher levels. For example, the Vitamin D Council advocates at least 125 nmol/L 25(OH)D (www.vitamindcouncil.org/about-vitamin-d/vitamin-d-deficiency/). Concentrations higher than 250 nmol/L may be harmful.
Some surveys suggest that there has been a decline in vitamin D status in populations in recent years. Thus there was a reduction from 75 nmol/L in 1988–1994 to 60 nmol/L in 2001–2004 in the large National Health and Nutritional Examination Survey in the USA (Ginde et al. 2009a). Epidemiological studies in several parts of the world indicate that an insufficient vitamin D status may be widespread, even in sunny countries. For example, 31 % of a large representative adult population in Australia, 21.4 % of women of child-bearing age in Oman, and 57 % of women and 49 % of men, aged 65 and above, in England all had 25(OH)D levels <50 nmol/L. Efforts have been made to construct models using the action spectrum from the conversion of 7-dehydrocholesterol to previtamin D3 in the human skin to predict how much sun exposure an individual requires under different climate conditions to ensure a satisfactory vitamin D status (McKenzie et al. 2009, 2011; Diffey 2010). This approach has been supplemented by actual measurement of 25(OH)D levels in volunteers with different skin types, exposed to the simulated sunlight present at particular latitudes at different times of the year (Rhodes et al. 2010).
23.5 Vitamin D and Bone Health
Vitamin D deficiency has been known for many years to lead to abnormal skeletal development in utero and in children and to poor bone health in adults. The disease that results from the deficiency in children is called rickets in which bone deformities are found due to chondrocyte disaggregation and skeletal mineralisation defects. It is estimated that 25(OH)D levels lower than about 20 nmol/L can lead to rickets. Supplementation with vitamin D is recommended for infants aged 0–12 months. In adults, osteomalacia can result from vitamin D deficiency, with defective mineralisation of the collagen matrix and hence reduced structural support and increased risk of fracture. Osteoporosis can also occur in the elderly with an increased risk of fracture. Osteoblast activity is reduced and bone mineralisation is defective. Although various studies have not produced consistent results, they suggest that 25(OH)D levels above 75 nmol/L are required for protection against osteomalacia and osteoporosis (reviewed in Wacker and Holick 2013).
Vitamin D has a critical role in calcium and phosphorus metabolism, ensuring adequate levels of both for various metabolic functions and bone mineralisation. 1,25(OH)2D significantly increases the absorption of both calcium and phosphorus from the intestine, the former by increasing the expression of an epithelial calcium channel and a calcium-binding protein. Vitamin D also acts indirectly on calcium and phosphorus levels via the regulation of parathyroid hormone (PTH). Low levels of 25(OH)D are associated with low levels of serum-ionised calcium, a situation which leads to increased PTH levels. Higher 25(OH)D levels with associated higher calcium levels have the reverse effects on PTH. Both PTH and 1,25(OH)2D stimulate osteoblasts to mobilise calcium stores. Further details can be found in Lips and van Schoor (2011) and Sai et al. (2011).
23.6 Nonskeletal Effects of Vitamin D and Potential Protection Against a Variety of Human Diseases
23.6.1 Immunomodulation Induced by Vitamin D
Increasing evidence has been obtained in recent years that vitamin D has multiple effects on the immune system, some stimulatory and some inhibitory. These could have relevance for the control of several human diseases and have been the subject of intense investigations in recent years.
Innate immunity involves a range of mechanisms that are often of most benefit at the initiation of a disease. Several innate immune responses are stimulated by 1,25(OH)2D. One important effect is to promote the expression of the cathelicidin gene in macrophages which leads to the production of cathelicidin (Liu et al. 2007). This peptide has antimicrobial activity against intracellular bacteria. 1,25(OH)2D induces autophagy in monocytes and macrophages via the induction of cathelicidin which then activates transcription of the autophagy-related genes (Yuk et al. 2009). Autophagy is the process whereby a cell self-digests through the action of enzymes within the same cell, thus preventing the survival of intracellular bacteria and viruses. Low levels of vitamin D result in impaired development of invariant natural killer T cells, a consequence that is particularly apparent if the deficiency occurs in utero (Cantorna et al. 2012). The invariant natural killer T cells are involved in many immunological processes; they recognise lipids and glycolipids rather than the peptide-MHC complexes recognised by other T cell subsets, and, on activation, produce a range of immunostimulatory mediators including interferon (IFN)-γ, interleukin (IL)-2, and tumour necrosis factor (TNF)-α.
In contrast to the mainly positive effects of vitamin D on innate immune responses, the majority of adaptive immune responses are downregulated by 1,25(OH)2D. It inhibits the number and function of T regulatory cells, promotes the production of immunosuppressive cytokines such as IL-4 and IL-10 while having the reverse effect on the immunostimulatory cytokines such as IL-2, suppresses the differentiation and maturation of dendritic cells and their ability to present antigens, and inhibits the differentiation and maturation of B cells and their production of immunoglobulins (reviewed in Van Etten and Mattieu 2005).
Due to these varying responses, elucidating the role of vitamin D in the immune control of various diseases in humans is not an easy task, particularly when further complexities are considered, such as various VDR polymorphisms which might confer additional susceptibility and the independent immune function of the vitamin D-binding protein. Several disease categories in which vitamin D may play an important role by modulating the immune response have been described. These cover a wide range of common conditions. The evidence frequently relies on the group of patients with the disease having a lower 25(OH)D level than the group of controls. However, few of these studies are prospective and therefore cannot distinguish whether the low status is a consequence of the disease or is a significant risk factor. Clinical trials using vitamin D supplements to prevent the disease or, more commonly, as a treatment have yielded inconsistent results thus far. In addition, it is difficult and frequently impossible to separate the effects of solar UV radiation from the effects of vitamin D in human subjects (Hart and Gorman 2013). Therefore this area is one of uncertainty at present in which there is vigorous research interest and activity.
Diseases where vitamin D may be protective include various microbial infections, autoimmune diseases, internal cancers, mental disorders, cardiovascular diseases, all-cause mortality, and asthma. As examples, information relating to the role of vitamin D in infectious and autoimmune diseases is outlined in Sects. 23.6.2 and 23.6.3, respectively.
23.6.2 Vitamin D and Risk of Infectious Diseases
Many infectious diseases, especially those caused by viruses infecting the respiratory tract (e.g. respiratory syncytial virus, rhinovirus, coronavirus, influenza, and parainfluenza), have a seasonal incidence with a peak in the winter months. Although there could be several explanations for this, including increased survival and transmission of viruses at low temperature and humidity, one suggestion, first made more than 30 years ago (Hope-Simpson 1981), attributed the pattern to the lower level of vitamin D in the winter months as the solar UV-B radiation declines. As outlined in Sect. 23.6.1, many aspects of innate immunity which are important in protection against viral infection of the respiratory tract are diminished by insufficient vitamin D. In particular, the reduced production of antimicrobial peptides by neutrophils, macrophages, and natural killer cells of the respiratory tract and by epithelial cells may be important as well as the lack of autophagy in macrophages. In addition, the action of vitamin D in suppressing the cytokine “storm” that is a feature of many respiratory infections may be vital (de Jong et al. 2006).
Observational evidence has been obtained from a variety of settings and countries in which 25(OH)D levels have been correlated with the occurrence of respiratory viral infections. In most cases, the lower the concentration of 25(OH)D, the higher the risk of respiratory infection (Ginde et al. 2009b; Sabetta et al. 2010; Berry et al. 2011). However, it should be noted that in almost all of these studies, the population already had symptoms of the infection at the time of the 25(OH)D assessment. Thus whether a low vitamin D status contributes to the risk of a symptomatic infection or is a consequence of the infection cannot be distinguished. About eight prospective randomised double-blind trials have taken place which examined whether vitamin D3 supplements can prevent respiratory infections. No consistent difference in the risk of respiratory infection between those taking the supplement and those given a placebo was found (reviewed in Bergman et al. 2013). However, one study reported that a benefit was apparent if the starting level of 25(OH)D was deficient (Camargo et al. 2012). Further trials are underway currently.
In tuberculosis, the causative bacterium, Mycobacterium tuberculosis, persists in macrophages, and therefore, the promotion of antimicrobial peptides and autophagy by 1,25(OH)2D may represent important factors in protection against persistence of the organism or its activation. In the nineteenth century, cod liver oil, which contains the highest level of vitamin D3 of any food, was used in Europe to prevent childhood diseases such as tuberculosis. It was superseded by heliotherapy (sun exposure) and phototherapy (exposure to artificial light sources) before the development of antibiotics in the second half of the twentieth century. Thus a possible link between vitamin D deficiency and susceptibility to tuberculosis or disease progression has a long history. More recent studies consistently report that subjects with tuberculosis have insufficient 25(OH)D levels or lower levels than control subjects (reviewed in Ralph et al. 2013). It is clearly difficult to investigate whether vitamin D status influences susceptibility to infection with M. tuberculosis and development of active disease from latency or response to treatment. In particular, whether a low 25(OH)D level is a consequence of the disease or a risk factor for, it needs to be distinguished. This can only be examined in prospective studies. Clinical trials using vitamin D supplements to prevent progression from latent to active tuberculosis have not been undertaken as yet, but other trials in which the supplements were administered to treat active disease have yielded predominantly negative results. The reasons that these trials do not support the observational findings include the possibilities that suboptimal doses of the supplement were used or that they did not lead to a sufficient increase in 1,25(OH)2D or that host determinants were not taken into account such as expression of the hydroxylases and the vitamin D-binding protein and polymorphisms in the VDR (Ralph et al. 2013).
23.6.3 Vitamin D and Risk of Autoimmune Diseases
It has been recognised for many years that the frequency of several autoimmune diseases is associated with latitude so that the further from the Equator, the higher the prevalence. Such a gradient has been shown most convincingly for multiple sclerosis (MS) but is also found to a lesser degree for type 1 diabetes mellitus, rheumatoid arthritis, and Crohn’s disease. Although the aetiology of these diseases is multifactorial with a clear genetic susceptibility, there is evidence that one environmental risk factor might be low exposure to solar UV radiation leading to insufficient vitamin D. As outlined in Sect. 23.6.1 above, 1,25(OH)2D has effects on the immune system that could help to prevent autoimmunity. In brief, it can counteract autoimmune inflammation, induce the differentiation of T regulatory cells that promote self-tolerance, inhibit the differentiation of dendritic cells and their ability to present antigen, and increase the production of immunosuppressive cytokines.
Of the autoimmune diseases and their possible link with vitamin D, most information has been published for MS. In MS, there is immune-mediated destruction of myelin-producing cells and axonal loss in the central nervous system, and it is the most frequent disabling neurological disorder of young adults. The latitudinal gradient for MS was first noted more than 50 years ago (Acheson and Bachrach 1960) and has been validated in more recent reports, including a comprehensive meta-analysis of global data in 2011 (Simpson et al. 2011). A similar latitudinal variation in the incidence of the common precursor of MS, called first central nervous system demyelinating events, has also been found (Taylor et al. 2010). Low ambient UV radiation or low sun exposure in childhood may be particularly significant in increasing the risk of MS in later life. Also, the month of birth has an important effect on the risk of MS development in the offspring; an increased risk for those born in the spring when maternal 25(OH)D levels are likely to be low and a decreased risk for those born in the late autumn/early winter when maternal 25(OH)D levels are likely to be higher (Dobson et al. 2013). In two large cohort studies in the USA, a higher vitamin D intake in the form of supplements and higher serum 25(OH)D levels were both linked to a decreased risk of MS (Munger et al. 2004; Munger et al. 2006). There was a particularly strong inverse relationship if the higher 25(OH)D level occurred before the age of 20 years. Furthermore the relapse rates for MS correlate inversely with serum 25(OH)D levels.
With regard to treatment of MS, several clinical trials have assessed vitamin D3 as a supplement, sometimes in association with IFN-β. The results thus far have been inconsistent (Soilu-Hanninen et al. 2012; Kampman et al. 2012; James et al. 2013), but none have shown more than a very modest benefit. Such studies are difficult and costly to undertake due to the low incidence of MS, the length of follow-up that is required, the need for a placebo group and for monitoring radiological, clinical, and immunological parameters, and uncertainties regarding the optimal dose of the supplement and how frequently it should be taken. However, there remains the intriguing possibility of using vitamin D supplements as an inexpensive, safe, and easy to administer treatment to improve current therapies in MS.
23.7 Evolutionary Aspects
Why has nature chosen, for the hormonal regulation of calcium metabolism and other bodily functions, a substance requiring the uncertain exposure to UV radiation for its synthesis? The answer to this question is not obvious and requires probing into several evolutionary aspects.
One explanation, proposed by Chevalier et al. (1997), is that the formation of 1,25(OH)2D from 7-dehydrocholesterol was originally a catabolic pathway, which then became regulatory. Arguments for this are, first, that vitamin D and related substances are rather toxic, and, secondly, that P450-type enzymes are involved both in hydroxylations that lead to detoxification and solubilisation of known toxins and in several hydroxylation steps of vitamin D and its analogues (see reviews of the vitamin D-related hydroxylations by Jones (1999) and Okuda and Ohyama (1999)).
One way of probing into the past is to compare amino acid sequences in proteins of living organisms. It is believed that the VDR belongs to a class of nuclear receptors of very ancient origin. The nuclear receptor class can be divided into several subclasses, and the divergence into these subclasses occurred at least 600 Ma ago (Bertrand et al. 2004). The closest known relative to the VDR is the ecdysone receptor in insects. One way of tracing the origin of the vitamin D regulation system would be to track the evolution of the VDR more in detail, but such a study has not been undertaken thus far.
In terrestrial vertebrates, i.e. birds, reptiles, and amphibians, the role of vitamin D is similar to that in mammals, although birds are not able to use vitamin D2 efficiently and other provitamins and vitamin D than D2 and D3 may exist in lizards and frogs (Holick 1989) (see Sect. 23.10 below for the relative efficiency of vitamin D3 and vitamin D2 in humans). Further back in evolutionary history, the evidence starts to become more “fishy”.
Several investigations show that various saltwater fish can thrive without vitamin D, and this is true also for at least one freshwater fish species (Ashok et al. 1998, 1999). There are, however, an even larger number of studies that indicate a function for vitamin D in other fish species (Barnett et al. 1979; Brown and Robinson 1992; Larsson 1999 and sources cited therein). It is also not clear why regulation would be unnecessary as a mechanism to avoid too high a calcium concentration in the cytosol is required.
The first vertebrates were the jawless Heterostraci and Osteostrachi, whose bodies were covered by bony plates. They were followed in evolution by the first true fishes, the shark-like Placodermi. These, belonging to the Elasmobranchiomorphi (cartilaginous fishes), had no bones inside their bodies, but they were also covered with a bony armour. Is it possible that the deposition of calcium phosphate and calcium carbonate early in evolution served as a protection against UV radiation, and that its deposition was regulated by radiation? This suggestion could be tested by finding out if the thickness of the armour varied with latitude (and thus with UV-B exposure) while taking continental drift and polar migration into account.
Even the earliest vertebrates mentioned lived less than 550 million years ago, at a time when the protecting ozone shield is thought to have afforded almost the same protection as today (see Chap. 16). The nuclear VDR has been found in a jawless fish (Whitfield et al. 2003), but could the regulation of calcium metabolism by vitamin D be of even more ancient origin than the vertebrates? Several investigations point in this direction.
In one type of coral (incidentally a relative of the red coral used for gems), UV radiation favours the development of normal spicules, structures containing collagen and calcium carbonate. The animal also produces 1,25(OH)2D in a UV-dependent manner (Kingsley et al. 2001).
The most compelling evidence, however, for the ancient origin of vitamin D as a calcium regulator comes from experiments with snails. In these animals, certain vitamin D-like compounds elevate intracellular exchangeable calcium and suppress alkaline phosphatase activity, leading to the conclusion that snails adapt to light conditions via the vitamin D endocrine system (Kriajev and Edelstein 1994, 1995; Kriajev et al. 1994). The evolutionary lines leading to molluscs and to vertebrates are estimated, with some uncertainty, to have diverged about 720 million years ago. If further evidence of vitamin D regulation in copepods, corals, and coccolithophorids is found, a much older age for the regulation system would have credence. If it is assumed that the vitamin effects in plants (see Sect. 23.11.) have an evolutionary origin in common with the regulation of calcium metabolism in animals, then this origin lies more than a one and a half billion years ago (Nei et al. 2001).
There remains the unlikely possibility of convergent evolution that distantly related organisms have independently selected vitamin D as their calcium regulator. If this is the case, why is vitamin D the best choice?
Calcium carbonate itself is a poor absorber of UV radiation, and therefore, it is not efficient as a radiation shield. Even a cm-thick layer absorbs only half of the incident radiation at the DNA absorption maximum (260 nm), as calculated from data for clear calcite crystals (Washburn et al. 1929). However, the scattering effect of calcium carbonate needs to be added and, most importantly, the absorption by proteins and other substances always associated with calcium carbonate shells and other calcified structures.
If the reason for the choice of the UV-sensitive vitamin D system is not regulation of UV shielding, what could it be? The human immune system is altered by UV radiation (see Chap. 24), but the evolutionary pressure that has selected for this modulation is obscure. It is likely to be relevant, since it occurs through different mechanisms, among others UV absorption in urocanic acid and absorption in DNA. Could it be that the original function of the vitamin D system was to modulate the immune defence, a function that to some extent seems still to exist?
23.8 Vitamin D2 Compared with Vitamin D3
The form of vitamin D used in major preparations of prescriptions in North America was for a long time vitamin D2 (Houghton and Vieth 2006), probably because it can be produced at a lower cost, and the process was patented early. This is now changing. Recently, there has been much interest in comparing the effects of vitamin D2 and vitamin D3 in human nutrition (Horst et al. 2000). When administered over a prolonged time, both are equally well taken up and converted to 25(OH)D circulating in the blood stream and also hydroxylated a second time to 1,25(OH)2D. Tsugawa et al. (1999) found that the D2 form of 1,25(OH)2D binds equally well as the D3 form to the VDR. However, this experiment used calf VDR, and the results may not apply to the polymorphic forms of the human receptor. The D2 forms are not converted to the corresponding D3 forms (Holick et al. 2008; Biancuzzo et al. 2013). Some of the vitamin D, D2, as well as D3 is also converted to 1,24,25-hydroxylated forms. While 1,24,25(OH)3D3 can bind to the VDR and exert biological activity, 1,24,25(OH)3D2 is inactive (see Houghton and Vieth 2006 for this and related topics), and this results in vitamin D2 having less overall activity than vitamin D3. It should be noted that differences in effects between D2 and D3 forms are not as large in humans as in rats and birds.
When vitamin D is given as a single large dose, the increase in circulating 25(OH)D2 initially rises in the same way as does the D3 form, but after 3 weeks, the level starts to fall in the case of hydroxyvitamin D2 but continues to rise and only falls after 15 weeks in the case of hydroxyvitamin D3 (Armas et al. 2004).
23.9 Distribution of Provitamin and Vitamin D in the Plant Kingdom
Among microalgae, several (but not all) species of the green algae Chlorella (Patterson 1971) and Chlamydomonas reinhardtii (Patterson 1974) contain ergosterol. This provitamin has also been found in the diatom Skeletonema menzelii, the coccolithophorid Emaliana huxleyi (Holick 1989), and the chrysophycean Ochromonas danica (Gershengorn et al. 1968). In addition, there have been numerous investigations on phytoplankton of mixed composition. In one instance, a correlation with the probable UV exposure was established, using season as a proxy for irradiation (Takeuchi et al. 1991; see also Tables 1a and 1b in Björn and Wang 2001). Among macroalgae, not only ergosterol but also provitamin D2 and vitamins D2 and D3 have been found in the brown alga Fucus vesiculosus grown under natural conditions with a higher content of the vitamins at a lower (southern Sweden) than at a higher (northern Norway) latitude. Provitamin D3 is present in the gametophyte of the red alga Chondrus crispus, while the sporophyte of the same species contains the isomer 22-dehydrocholesterol.
Higher plants generally contain provitamins and vitamins D2 and D3 in their leaves (Napoli et al. 1977; Rambeck et al. 1981; Horst et al. 1984; Prema and Raghuramulu 1996; Boland et al. 2003). In general, vitamins are present only after exposure to UV radiation (Hess and Weinstock 1924; Skliar et al. 2000; Björn and Wang 2001 and references cited therein) although there are exceptions (see Sect. 23.13). Some plants even form the hydroxylated forms of vitamin D (Napoli et al. 1977; Skliar et al. 2000; Gil et al. 2007).
23.10 Physiological Effects of Provitamin and Vitamin D in Plants and Algae
Fries (1984) showed that growth of the green macroalga Enteromorpha compressa, the red alga Nemalion helminthoides, and the brown alga Fucus spiralis is stimulated by vitamins and provitamin D. Vitamin D3 applied to herbaceous and woody plants stimulates initiation of adventitious roots (Buchala and Schmid 1979; Jarvis and Booth 1981; Moncousin and Gaspar 1983). Vitamin D at a nanomolar concentration inhibits root elongation in Phaseolus vulgaris and promotes germination of light-sensitive lettuce seed in darkness (Buchala and Pythoud 1988). Vitamin D3 induces the synthesis of the calcium-binding signalling protein calmodulin in bean roots (Vega and Boland 1986).
23.11 Roles of Provitamin and Vitamin D in Plants
Solanum glaucophyllum, the waxy leaf nightshade, endemic in several South American countries, forms such large amounts of the active vertebrate hormone form, 1,25(OH)2D3, that grazing animals develop calcinosis and can die (see Curino et al. 1998; Boland et al. 2003 for literature). In this case, a protective function of vitamin D for the plant is assumed.
There are some indications that vitamin D and its hydroxylated forms are involved in calcium metabolism in plants. Thus Aburjai et al. (1997) found that calcium deprivation increased the concentrations of vitamin D and 25(OH)D in cell cultures of Solanum malacoxylon, while results for 1,25(OH)2D3 were not clear due to analytical difficulties. Burlini et al. (2002) showed that the concentration of 1,25(OH)2D3 increased when calcium ions were removed from the medium. Conversely, Habib and Donnelly (2005) claimed that the calcium content of potato plants (Solanum tuberosum) was increased by either exposure to UV radiation or administration of vitamin D. This finding needs confirmation by independent investigators. Vega and Boland (1988, 1989) and Milanesi and Boland (2006) have pointed to the similarity between the vertebrate VDR and proteins present in Phaseolus vulgaris and Solanum glaucophyllum.
23.12 Biogeographical Aspects
Human complexion tends to be darker the higher the UV radiation in the environment. This is an inherited (“racial”) trait that has evolved independently in Europe and Asia (Norton et al. 2007), but many individuals can acclimatise phenotypically to some extent (i.e. the skin forms pigment in response to UV radiation; see Chap. 24 and Cui et al. 2007). UV radiation can cause skin cancer and other problems, and these effects are particularly frequent for people poorly adapted for the high environmental radiation they are exposed to, such as people of European origin living in South Africa and Australia. Thus, clearly, the pigment works as protection against high radiation. It has been proposed (Branda and Eaton 1978; Jablonski and Chaplin 2000) that pigmentation is important for photoprotection of folic acid, but in vivo, this substance is photoprotected in another way (Vorobey et al. 2006). Although vitamin D is toxic at too high a concentration, it has been shown by Holick et al. (1981) that skin pigment is not necessary to prevent its overaccumulation; the photochemical system is self-regulating. The reason for this is the low rate of conversion of previtamin to vitamin, in combination with the photochemical side and back reactions of previtamin D. Thus, toxicity can occur only following excessive intake (e.g. Koutkia et al. 2001).
There is, however, another connection between skin type and vitamin D. All humans are thought to originate from Africa and presumably are all descendants of black-skinned people, although at a prehuman furred stage, lighter skin is possible as found in chimpanzees (Jablonski and Chaplin 2000). But with migration to higher and higher latitudes, the skin colour became paler (Fig. 23.6). The selection pressure for this is clear: avoidance of vitamin D deficiency (Clemens et al. 1982). African people who have emigrated north in historic time are known to suffer from just such a deficiency (Shewakramani et al. 2001). Inuits may have more pigment than would be predicted from their northern habitat; their traditional food is from the sea and mostly rich in vitamin D (because the sea currents bring vitamin D from lower and more sunny latitudes), so they have not been exposed to the same selection pressure as people with more terrestrial habits.

The relation between skin colour (reflectance at 685 nm) and latitude for 85 samples of “indigenous populations” from different parts of the world. Darker skin colour is lower in the diagram, and on the abscissa, 0 stands for the equator. In the regression equation at the bottom of the graph, y stands for reflectance in percent and x for latitude in degrees. There is a clear trend of darker skin colour towards the equator. The great variation around the regression curve has several causes. Even “indigenous populations” have migrated and settled in their present regions within a time span which is often too short to allow complete adaptation to the environment. The way of life also modulates the need for sunlight. Thus, the square at the highest latitude (a little above 60°) lies far below the regression curve. It represents Inuits in southern Greenland. It is thought that they, due to their vitamin D-rich food from the sea, have a lesser need for vitamin D from photochemical conversion in the skin than most other populations (Data adapted from those compiled by Jablonski and Chaplin (2000))
Jablonski and Chaplin (2000) found that in all human populations where data were available, the complexion of women is lighter than that of men. It may be difficult to separate out the acclimation component due to different lifestyles, but the authors believe that it could be an adaptation to the greater need for calcium and vitamin D during pregnancy and lactation.
The question remains: How do non-human terrestrial vertebrates manage at high latitudes? As they are often covered with hair or plumage or are “cold-blooded” (poikilothermic), they would have difficulties in producing their own vitamin D by having either inefficient photochemical conversion of pro- to previtamin or inefficient thermochemical conversion of previtamin to vitamin. In fact, amphibians, and reptiles in particular, decline in frequency with increasing latitude. The arctic dinosaurs may, in fact, have been homeothermic (thermoregulating).
According to an old and abandoned theory, birds produce provitamin D in their uropygial gland and distribute it over their plumage when preening. This converts to vitamin D on exposure to sunlight and is ingested at the next preening. Later investigations with more modern methods of analysis have failed to establish with certainty that provitamin D is in the uropygial secretion. There is a single study, using the best analytical methods available at the time, which demonstrated the presence of provitamin D3 in the uropygial gland of domestic fowl (Gallus) (Uva et al. 1978). Such an investigation needs to be repeated using high-performance liquid chromatography, nuclear magnetic resonance, and absorption spectroscopy, since the identification of provitamin D3 among all the steroids present in uropygial secretion is not straightforward. If its presence can be established, the analysis could be extended to other kinds of birds. It should also be mentioned that Holick (1989; referring to unpublished observations by himself and M.A. St. Lezin) found no provitamin D3 in chicken feathers. On the other hand, it is well established that fowl can use UV absorbed by the head and legs to improve their vitamin D and calcium status and egg production. It is assumed that birds like arctic owls and ptarmigans are totally dependent on vitamin D in the food for covering their requirements. Birds cannot efficiently use vitamin D2 only D3.
For arctic mammals, like reindeer, the situation is critical. Reindeer need large quantities of calcium, not only for the skeleton but also for the yearly production of antlers. They are covered with hair and do not have a uropygial gland, so they rely heavily on food for their vitamin D. The critical time is the dark winter, and the most important winter food is reindeer lichen. We (Wang et al. 2001) investigated one species of reindeer lichen from different latitudes (Fig. 23.7) and found that it contained both vitamins D2 and D3, in a strongly latitude-dependent manner, with the lowest values in northern Scandinavia even by the end of the summer. Still, 10 g of the lichen from northern Scandinavia would provide a human with the necessary daily amount, but would humans eat lichen? Wild reindeer survive, even on Spitsbergen island at 78°N, where the vitamin D content in their food must be lower than this. Could there be another source? It would perhaps be worth looking at what the rumen bacteria can produce.

Vitamins D2 and D3 contents in the reindeer lichen Cladina arbuscula at different latitudes (northern Finland, 67°N, to Greece, 40°N) (From Wang et al. (2001))
23.13 Non-photochemical Production of Vitamin D
Vitamin D can be produced non-photochemically. Curino et al. (1998, 2001) have shown that cells of Solanum glaucophyllum grown in culture in darkness form 1,25(OH)2D3, albeit at lower concentrations than the plant under sun-exposed field conditions. The mechanism is not known, but one has been proposed by Norman and Norman (1993) to explain how animals like subterranean mole rats, living in darkness, can obtain their requirement from underground plant parts. It is, however, (1) doubtful whether these animals need vitamin D (Pitcher and Buffenstein 1995 and literature cited there) and (2) unlikely that their diet is really completely vitamin D-free, as we have found small amounts of vitamins D2 and D3 in carrot roots not exposed to UV radiation (Wang and Björn, unpublished). The same holds for nocturnal animals (Opperman and Ross 1990; Kwiecinski et al. 2001). Larsson (1999) has erroneously claimed that Opperman and Ross (1990) found that the nocturnal fruit-eating bat Rousettus aegyptiacus can form 7-dehydrocholesterol from mevalonate.
Abbreviations
- 1,25(OH)2D:
-
1,25-dihydroxyvitamin D
- 25(OH)D:
-
25-hydroxyvitamin D
- IFN:
-
Interferon
- IL:
-
Interleukin
- LC-MS/MS:
-
Liquid chromatography-tandem mass spectroscopy
- MS:
-
Multiple sclerosis
- PTH:
-
Parathyroid hormone
- TNF:
-
Tumour necrosis factor
- UV:
-
Ultraviolet
- VDR:
-
Vitamin D receptor
References
Aburjai T, Bernasconi S, Manzocchi LA, Pelizzoni F (1997) Effect of calcium and cell immobilization on the production of cholecalciferol and its derivatives by Solanum malacoxylon cell cultures. Phytochemistry 46:1015–1018
Acheson ED, Bachrach CA (1960) The distribution of multiple sclerosis in U.S. veterans by birthplace. Am J Hyg 72:77–88
Armas LAG, Hollis BW, Heaney RP (2004) Vitamin D2 is much less effective than vitamin D3 in humans. J Clin Endocrinol Metab 89:5387–5391
Ashok A, Rao DS, Raghuramulu N (1998) Vitamin D is not an essential nutrient for rora (Labeo rohita) as a representative of freshwater fish. J Nutr Sci Vitaminol 44:195–205
Ashok A, Rao DS, Chennaiah S, Raghuramulu N (1999) Vitamin D2 is not biologically active for rora (Labeo rohita) as vitamin D3. J Nutr Sci Vitaminol 45:21–30
Barnett BJ, Cho CY, Slinger SJ (1979) The essentiality of cholecalciferol in the diets of rainbow trout (Salmo gairdneri). Comp Biochem Physiol 63A:291–297
Bergman P, Lindh AU, Bjorkhem-Bergman L, Lindh JD (2013) Vitamin D and respiratory tract infections: a systematic review and meta-analysis of randomized controlled trials. PLoS One 8:e65835
Berry DJ, Hesketh K, Power C, Hypponen E (2011) Vitamin D status has a linear association with seasonal infections and lung function in British adults. Br J Nutr 106:1433–1440
Bertrand W, Brunet FG, Escriva H, Parmentier G, Laudet V, Robinson-Rechavi M (2004) Evolutionary genomics of nuclear receptors: From twenty-five ancestral genes to derived endocrine systems. Mol Biol Evol 21:1923–1937
Biancuzzo RM, Clarke N, Reitz RE, Travison TG, Holick MF (2013) Serum concentrations of 1,25-dihydroxyvitamin D2 and 1,25-dihydroxyvitamin D3 in response to vitamin D2 and Vitamin D3 supplementation. J Clinic Endocrinol Metab 98:973–979
Björn LO, Wang T (2001) Is provitamin D a UV-B receptor in plants? Plant Ecol 154:3–8
Boland R, Skliar M, Curino A, Milanesi L (2003) Vitamin D compounds in plants. Plant Sci 164:357–369
Boomsma F, Jacobs HJC, Havinga E, van der Gen A (1975) Studies of vitamin D and related compounds, part 24. New irradiation products of pre-vitamin D3. Tetrahedron Lett 7:427–430
Bouillon R, Eisman J, Garabedian M, Holick MF, Kleinschmidt J, Suda T, Terenetskaya I, Webb A (2006) Action spectrum for production of previtamin D3 in human skin, CIE Technical Report 174, Commission Internationale de l’Éclairage (CIE) Central Bureau, Vienna, Austria.
Bouillon R, Norman AW, Pasqualini JR (eds) (2004) Vitamin D: proceedings of the 12th workshop on vitamin D, July 6–10, 2003. Maastricht, the Netherlands. Elsevier, Amsterdam. (Reprinted from J. Steroid Biochem Mol Biol 89–90)
Branda RF, Eaton JW (1978) Skin color and nutrient photolysis: an evolutionary hypothesis. Science 201:625–626
Brown PB, Robinson EH (1992) Vitamin D studies with channel catfish (Ictalurus punctuatus) reared in calcium-free water. Comp Biochem Physiol 103A:213–219
Buchala AJ, Pythoud F (1988) Vitamin D and related compounds as plant growth substances. Physiol Plant 74:391–396
Buchala AJ, Schmid A (1979) Vitamin D and its analogues as a new class of plant growth substances affecting rhizogenesis. Nature 280:230–231
Burlini N, Bernasconi S, Manzocchi LA (2002) Effects of elicitors and Ca2+ deprivation on the levels of sterols and 1,25-dihydroxy vitamin D-3 in cell cultures of Solanum malacoxylon. Funct Plant Biol 29:527–533
Camargo CA Jr, Ganmaa D, Frazier AL, Kirchberg FF, Stuart JJ, Kleinman K, Sumberzul N, Rich-Edwards JW (2012) Randomized trial of vitamin D supplementation and risk of acute respiratory infection in Mongolia. Pediatrics 130:e561–e567
Cantorna MT, Zhao J, Yang L (2012) Vitamin D, invariant natural killer T-cells and experimental autoimmune disease. Proc Nutr Soc 71:62–66
Chevalier G, Baudet C, AvenelAudran M, Furman I, Wion D (1997) Was the formation of 1,25-dihydroxyvitamin D initially a catabolic pathway? Med Hypotheses 48:325–329
Clemens TL, Adams JS, Henderson SL, Holick MF (1982) Increased skin pigment reduces the capacity of skin to synthesise vitamin D3. Lancet 319:74–76
Cui R, Widlund HR, Feige E, Lin JY, Wilensky DL, Igras VE, D’Orazio J, Fung CY, Schanbacher CF, Granter SR, Fisher DE (2007) Central role of p53 in the suntan response and pathologic hyperpigmentation. Cell 128:853–864
Curino A, Skliar M, Boland R (1998) Identification of 7-dehydrocholesterol, vitamin D3, 25(OH)-vitamin D3 and 1,25(OH)2-vitamin D3 in Solanum glaucophyllum cultures grown in absence of light. Biochim Biophys Acta 1425:485–492
Curino A, Milanesi L, Benassati S, Skliar M, Boland R (2001) Effect of culture conditions on the synthesis of vitamin D3 metabolites in Solanum glaucophyllum grown in vitro. Phytochemistry 58:81–89
De Jong MD, Simmons CP, Thanh TT et al (2006) Fatal outcome of human influenza A (H5N1) is associated with high viral load and hypercytokinemia. Nat Med 12:1203–1207
DeLuca (1997) Historical overview. In: Feldman D, Glorieux FH, Pike JW (eds) Vitamin D. Academic, New York, pp 3–12
Diffey DL (2010) Is casual exposure to summer sunlight effective at maintaining adequate vitamin D status? Photodermatol Photoimmunol Photomed 26:172–176
Dmitrenko O, Frederick JH, Reischl W (2001) Previtamin D conformations and the wavelength-dependent photoconversions of previtamin D. J Photochem Photobiol A: Chemistry 139:125–131
Dobson R, Giovannoni G, Ramagopalan S (2013) The month of birth effect in multiple sclerosis: systematic review, meta-analysis and effect of latitude. J Neurol Neurosurg Psychiatry 84:427–432
Doroudi M, Chen J, Boyan BD, Schwartz Z (2014) New insights on membrane mediated effects of 1α,25-dihydroxy vitamin D3 signaling in the musculoskeletal system. Steroids 81:81–87
Feldman D, Glorieux FH, Pike JW (eds) (2005) Vitamin D. 2nd ed. Academic Press, New York
Fries L (1984) D-vitamins and their precursors as growth regulators in axenically cultivated marine macroalgae. J Phycol 20:62–66
Gershengorn MC, Smith ARH, Goulston G, Goad LJ, Goodwon TW, Haines TH (1968) The sterols of Ochromonas danica and Ochromonas malhamensis. Biochemistry 7:1698–1706
Gil S, Dallorso M, Horst R (2007) Screening of vitamin D activity (VDA) of Solanum glaucophyllum leaves measured by radioimmunoassay (RIA). J Steroid Biochem Mol Biol. doi:10.1016/j.jsbmb.2006.11.008
Ginde AA, Lui MC, Camargo CA Jr (2009a) Demographic differences and trends of vitamin D insufficiency in the US population, 1988–2004. Arch Intern Med 169:626–632
Ginde AA, Mansbach JM, Camargo CA Jr (2009b) Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health Nutrition Examination Survey. Arch Intern Med 169:384–390
Glerup H, Mikkelsen K, Poulsen L, Hass E, Overbeck S, Thomsen J, Charles P, Eriksen EF (2000) Commonly recommended daily intake of vitamin D is not sufficient if sunlight exposure is limited. J Intern Med 247:260–268
Glisson F (1650) De Rachitide sive morbo puerili, qui vulgo The Rickets diciteur http://books.google.se/books?id=mtOLP7AI8v4C&printsec=frontcover&hl=sv#v=onepage&q&f=false
Habib A, Donnelly DJ (2005) Stimulation of Ca2+ uptake into micropropagated potato plantlets by UV light and vitamin D3. Am J Potato Res 82:191–196
Hart PH, Gorman S (2013) Exposure to UV wavelengths in sunlight suppresses immunity. To what extent is UV-induced vitamin D3 the mediator responsible? Clin Biochem Rev 34:3–13
Haussler MR, Whitfield GK, Kaneko I, Haussler CA, Hsieh D, Hsieh J-C, Jurutka PW (2013) Molecular mechanisms of vitamin D action. Calcif Tissue Int 92:77–98
Havinga E (1973) Vitamin D, example and challenge. Experientia 29:1181–1193
Hess AF, Unger LG (1921) Cure of infantile rickets by sunlight. JAMA 77:39
Hess AF, Weinstock M (1924) Antirachitic properties imparted to inert fluids and green vegetables by ultraviolet irradiation. J Biol Chem 62:301–313
Holick MF (1989) Phylogenetic and evolutionary aspects of vitamin D from phytoplankton to humans. In: Pang PKT, Schreibman MP (eds) Vertebrate endocrinology: fundamentals and biomedical implications, vol 3. Academic, Orlando, pp 7–43
Holick MF (1999) Evolution, biologic functions, and recommended dietary allowances for vitamin D. In: Holick MF (ed.) Vitamin D: Physiology, molecular biology, and clinical applications. Humana Press, Totowa, pp. 1–16.
Holick MF (ed) (2010) Vitamin D: physiology, molecular biology, and clinical applications, 2nd edn. Humana Press, Totowa. ISBN 978-1-60327-303-9; e-ISBN 978-1-60327-303-9’; doi:10.1007/978-1-60327-303-9
Holick MF, MacLaughlin JA, Doppelt SH (1981) Regulation of cutaneous previtamin D3 photosynthesis in man: skin pigment is not an essential regulator. Science 211:590–592
Holick MF, Tian XQ, Allen M (1995) Evolutionary importance for the membrane enhancement of the production of vitamin D3 in the skin of poikilothermic animals. Proc Natl Acad Sci U S A 98:3124–3126
Holick MF, Biancuzzo RM, Chen TC, Klein EK, Young A, Bibuld D, Reitz R, Salameh W, Ameri A, Tannenbaum AD (2008) Maintaining circulating concentrations of 25-hydroxyvitamin D. J Clin Endocrinol Metab 93:677–681
Hope-Simpson RE (1981) The role of season in the epidemiology of influenza. J Hyg (Lond) 86:35–47
Horst RL, Reinhardt TA, Russell JR, Napoli JL (1984) The isolation and identification of vitamin D2 and vitamin D3 from Medicago sativa (alfalfa plant). Arch Biochem Biophys 231:67–71
Horst RL, Prapong S, Reinhardt TA, Koszewski NJ, Knutson J, Bishop C (2000) Comparison of the relative effects of 1,24-dihydroxyvitamin D2, [1,24-(OH)2D2], 1,24-dihydroxyvitamin D3 [1,24-(OH)2D3], and 1,25-dihydroxyvitamin D3 [1,25-(OH)2D3] on selected vitamin D-regulated events in the rat. Biochem Pharmacol 60:701–708
Hossein-nezhad A (2013) Vitamin D for health: a global perspective. Mayo Clin Proc 88:720–755
Houghton LA, Vieth R (2006) The case against ergocaciferol (vitamin D2) as a vitamin supplement. Am J Clin Nutr 84:694–697
Institute of Medicine (US) committee to review dietary reference intakes for vitamin D and calcium (2011) Ross AC, Taylor CL, Yaktine AL, Del Valle HB (eds) Dietary reference intakes for calcium and vitamin D. National Academies Press, Washington DC
Jablonski NG, Chaplin G (2000) The evolution of human skin coloration. J Hum Evol 39:57–106
James E, Dobson R, Kuhle J, Baker D, Giovannoni G, Ramagopalan SV (2013) The effect of vitamin D-related interventions on multiple sclerosis relapses: a meta-analysis. Mult Scler J 19:1571–1579
Jarvis BC, Booth A (1981) Influence of indole-butyric acid, boron, myo-inositol, vitamin D2 and seedling age on adventitious root development in cuttings of Phaseolus aureus. Physiol Plant 53:213–218
Jones G (1999) Metabolism and catabolism of vitamin D, its metabolites and clinically relevant analogs. In: Holick MF (ed) Vitamin D: physiology, molecular biology, and clinical applications. Humana Press, Totowa, pp 57–84
Kampman MT, Steffensen LH, Mellgren SI, Jorgensen L (2012) Effect of vitamin D3 supplementation on relapses, disease progression, and measures of function in persons with multiple sclerosis: exploratory outcomes from a double-blind randomised controlled trial. Mult Scler 18:21144–21151
Kasahara AK, Sungh RJ, Noymer A (2013) Vitamin D (25OHD) serum seasonality in the United States. PLoS One 8:e65785
Kingsley RJ, Corcoran ML, Krider KL, Kriechbaum KL (2001) Thyroxine and vitamin D in the gorgonian Leptogorgia virgulata. Comp Biochem Physiol A 129:897–907
Knudson A, Benford F (1938) Quantitative studies of the effectiveness of ultraviolet radiation of various wave-lengths in rickets. J Biol Chem 124:287–299
Koutkia P, Chen TC, Holick MF (2001) Vitamin D intoxication associated with an over-the-counter supplement. N Engl J Med 345:66–67
Kriajev L, Edelstein S (1994) Vitamin D metabolites and extracellular calcium currents in hemocytes of land snails. Biochem Biophys Res Commun 204:1096–1101
Kriajev L, Edelstein S (1995) Effect of light and nutrient restriction on the metabolism of calcium and vitamin D in land snails. J Exp Zool 272:153–158
Kriajev L, Otremski I, Edelstein S (1994) Calcium shells from snails: response to vitamin D metabolites. Calcified Tissue Int 55:204–207
Kwiecinski GG, Lu ZR, Chen TC, Holick MF (2001) Observations on serum 25-hydroxyvitamin D and calcium concentrations from wild-caught and captive neotropical bats, Artibeus jamaicensis. Gen Comp Endocrinol 122:225–231
Lai JK, Lucas RM, Banks E, Ponsonby AL (2012) Variability in vitamin D assays impairs clinical assessment of vitamin D status. Intern Med J 42:43–50
Larsson D (1999) Vitamin D in teleost fish: non-genomic regulation of intestinal calcium transport. Diss. Göteborg Univ., Dept of Zoophysiology Göteborg, Sweden. ISBN 91-628-3681-1
Lehmann B, Genehr T, Pietzsch J, Meurer M (2001) UVB-induced conversion of 7-dehydrocholesterol to 1α,25-dihydroxyvitamin D3 in an in vitro human skin equivalent model. J Invest Dermatol 117:1179–1185
Lips P (2006) Vitamin D physiology. Prog Biophys Mol Biol 92:4–8
Lips P, van Schoor NM (2011) The effects of vitamin D on bone and osteoporosis. Best Pract Res Clin Endocrinol Metab 25:585–591
Liu PT, Stenger S, Tang DH, Modlin RL (2007) Cutting edge: vitamin D-mediated human antimicrobial activity against Mycobacterium tuberculosis is dependent on the induction of cathelicidin. J Immunol 179:2060–2063
MacLaughlin J, Holick MF (1985) Aging decreases the capacity of human skin to produce vitamin D3. J Clin Invest 76:1536–1538
MacLaughlin JA, Anderson RR, Holick MF (1982) Spectral character of sunlight modulates photosynthesis of previtamin D3 and its photoisomers in human skin. Science 216:1001–1003
McKenzie RL, Aucamp PJ, Bais AF, Bjorn LO, Ilyas M, Madronich S (2011) Ozone depletion and climate change: impacts on UV radiation. Photochem Photobiol Sci 10:182–198
McKenzie RL, Liley JB, Björn LO (2009) UV radiation: Balancing risks and benefits. Photochem Photobiol 85:88–98.
Mellanby E (1918) The part played by an “accessory factor”“in the production of experimental rickets. J Physiol (Lond) 52:11–14
Milanesi L, Boland R (2006) Presence of vitamin D-3 receptor (VDR)-like proteins in Solanum glaucophyllum. Physiol Plant 128:341–350
Moncousin C, Gaspar T (1983) Peroxidase as a marker for rooting improvement of Cynara scolymus L. cultured in vitro. Biochem Physiol Pflanzen 178:263–271
Mozolowski W (1939) Jedrzej Sniadecki (1768–1838) on the cure of rickets. Nature 143:121
Munger KL, Zhang SM, O’Reilly E, Hernan NS, Olek MJ, Willett WC, Ascherio A (2004) Vitamin D intake and incidence of multiple sclerosis. Neurology 62:60–65
Munger KL, Levin LI, Hollis BW, Howard NS, Ascherio A (2006) Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis. J Am Med Assoc 296:2832–2838
Napoli JL, Reeve LE, Eisman J, Schnoes HK, DeLuca HF (1977) Solanum glaucophyllum as source of 1,25-dihydroxyvitamin D3. J Biol Chem 252:2580–2583
Nei M, Xu P, Glazko G (2001) Estimation of divergence times from multiprotein sequences for a few mammalian species and several distantly related organisms. Proc Natl Acad Sci U S A 98:2497–2502
Norman AW (2006) Minireview: vitamin D receptor: new assignments for an already busy receptor. Endocrinology 147:5542–5548
Norman TC, Norman AW (1993) Consideration of chemical mechanisms for the nonphotochemical production of vitamin D3 in biological systems. Bioorg Med Chem Lett 3:1785–1788
Norton HL, Kittles RA, Parra E, McKeigue P, Mao X, Cheng K, Canfield VA, Bradley DG, McEvoy B, Shriver MD (2007) Genetic evidence for the convergent evolution of light skin in Europeans and East Asians. Mol Biol Evol 24:710–722
Norval M, Björn LO, de Gruijl FR (2010) Is the action spectrum for the UV-induced production of previtamin D3 in human skin correct? Photochem Photobiol Sci 9:11–17
Okuda K-I, Ohyama Y (1999) The enzymes responsible for metabolizing vitamin D. In: Holick MF (ed) Vitamin D: physiology, molecular biology, and clinical applications. Humana Press, Totowa, pp 85–107
Opperman LA, Ross FP (1990) The adult fruit bat (Rousettus aegypticus) expresses only calbindin-D9K (vitamin D-dependent calcium-binding protein) in its kidney. Comp Biochem Physiol B Biochem Mol Biol 97:295–299
Patterson GW (1971) The distribution of sterols in algae. Lipids 6:120–127
Patterson GW (1974) Sterols of some green algae. Comp Biochem Physiol B 47:453–457
Pitcher T, Buffenstein R (1995) Intestinal calcium-transport in mole rats (Cryptomys damarensis and Heterocephalus glaber) is independent of both genomic and non-genomic vitamin D mediation. Exp Physiol 80:597–608
Prema TP, Raghuramulu N (1996) Vitamin D3 and its metabolites in the tomato plant. Phytochemistry 42:617–620
Ralph AP, Lucas RM, Norval M (2013) Vitamin D and solar ultraviolet radiation in the risk and treatment of tuberculosis. Lancet Infect Dis 13:77–88
Rambeck WA, Kreutzberg O, Bruns-Droste C, Zucker H (1981) Vitamin D-like activity of Trisetum flavescens. Zschr Pflanzenphysiol 104:9–16
Rhodes LE, Webb AR, Fraser HI, Kift R, Durkin MT, Allan D, O’Brien SJ, Vail A, Berry JL (2010) Recommended summer sunlight exposure levels can produce sufficient (>or = 20 ng ml(-1)) but not the proposed optimal (>or = 32 ng ml(-1)) 25(OH)D levels at UK latitudes. J Invest Dermatol 130:1411–1418
Sabetta JR, DePetrillo P, Cipriano P, Smardin J, Burns LA, Landry ML (2010) Serum 25-hydroxyvitamin d and the incidence of acute viral respiratory tract infections in healthy adults. PLoS One 5:e11088
Sai AJ, Walters RW, Fang X, Gallagher JC (2011) Relationship between vitamin D, parathyroid hormone and bone health. J Clin Endocrinol Metab 96:E436–E446
Saltiel J, Cires L, Turek AM (2003) Conformer-specific photoconversion of 25- hydroxytachysterol to 25-hydroxyprevitamin D3: role in production of vitamin Ds. J Am Chem Soc 125:2866–2867
Schwartz GG, Skinner HG (2007) Vitamin D status and cancer: new insights. Curr Opin Clin Nutr Metab Care 10:6–11
Shewakramani S, Rakita D, Tangpricha V, Holick MF (2001) Vitamin D insufficiency is common and under-diagnosed among African American patients. J Bone Miner Res 16:S512
Simpson S Jr, Blizzard L, Otahal P, van der Mei I, Taylor B (2011) Latitude is significantly associated with the prevalence of multiple sclerosis: a meta-analysis. J Neurol Neurosurg Psychiatry 82:1132–1141
Skliar M, Curino A, Milanesi E, Benassati S, Boland R (2000) Nicotiana glauca: another plant species containing vitamin D3 metabolites. Plant Sci 156:193–199
Soilu-Hanninen M, Aivo J, Lindstrom BM, Elovaara I, Sumelahti ML, Farkkila M, Lienari P, Atula S, Sarasoja T, Herrala L, Keskinarkaus I, Kruger J, Kallio T, Rocca MA, Filippi M (2012) A randomised, double-blind, placebo controlled trial with vitamin D3 as an add on treatment to interferon β-1b in patients with multiple sclerosis. J Neurol Neurosurg Psychiatry 83:565–571
Steenbock H, Black A (1924) The induction of growth-promoting and calcifying properties in a ration by exposure to ultra-violet light. J Biol Chem 61:405–422
Takada K (1983) Formation of fatty acid esterified vitamin D3 in rat skin by exposure to ultraviolet radiation. J Lipid Res 24:441–448
Takada K, Okano T, Tamura Y (1979) A rapid and precise method for the determination of vitamin D3 in rat skin by high-performance liquid chromatography. J Nutr Sci Vitaminol 25:385–398
Takeuchi A, Okano T, Tanda M, Kobayashi T (1991) Possible origin of extremely high contents of vitamin D3 in some kinds of fish liver. Comp Biochem Physiol 100A:483–487
Taylor BV, Lucas RM, Dear K, Kilpatrick TJ, Pender MP, van der Mei IA, Chapman C, Coulthard A, Dwyer T, McMichael AJ, Valery PC, Williams D, Ponsonby AL, Lim L (2010) Latitudinal variation in the incidence and type of first central nervous system demyelinating events. Mult Scler 16:398–406
Tian WQ, Holick MF (1995) Catalyzed thermal isomerization between previtamin D3 and vitamin D3 via β-cyclodextrin complexation. J Biol Chem 270:8706–8711
Tian WQ, Holick MF (1999) A liposomal model that mimics the cutaneous production of vitamin D3. J Biol Chem 274:4174–4179
Tian XQ, Chen TC, Matsuoka LY, Wortsman J, Holick MF (1993) Kinetic and thermodynamic studies of the conversion of previtamin D3 to vitamin D3 in human skin. J Biol Chem 268:14888–14892
Tsugawa N, Nakagawa K, Kawamoto Y, Tachibana Y, Hayashi T, Ozono K, Okaono T (1999) Biological activity profiles of 1α,25-dihydroxyvitamin D2, D3, D4, D7, and 2-epi-1α,25-dihydroxyvitamin D2. Biol Pharm Bull 22:371–377
Uva BM, Ghiani P, Deplano S, Madich A, Vaccari M, Vallarino M (1978) Occurrence of 7-dehydrocholesterol in the uropygial gland of domestic fowls. Acta Histochem 62:237–243
Van de Peer Y, Baldauf SL, Doolittle WF, Meyer A (2000) An updated and comprehensive rRNA phylogeny of (crown) eukaryotes based on rate-calibrated evolutionary distances. J Mol Evol 51:565–576
Van Etten E, Mathieu C (2005) Immunoregulation by 1,25-dihydroxyvitamin D3: basic concepts. J Steroid Biochem Mol Biol 97:93–101
Vega MA, Boland RL (1986) Vitamin D-3 induces the novo synthesis of calmodulin in Phaseolus vulgaris root segments in vitro. Biochim Biophys Acta 881:364–374
Vega MA, Boland RL (1988) Presence of sterol-binding sites in the cytosol of French-bean (Phaseolus vulgaris) roots. Biochem J 250:565–569
Vega MA, Boland RL (1989) Partial characterization of the sterol binding macro-molecule of Phaseolus vulgaris roots. Biochim Biophys Acta 1012:10–15
Vorobey P, Steindal AE, Off MK, Vorobey A, Johan Moan J (2006) Influence of human serum albumin on photodegradation of folic acid in solution. Photochem Photobiol 82:817–822
Wacker M, Holick MF (2013) Sunlight and vitamin D: A global perspective for health. Dermato-Endocrin 5:51–108
Wang T, Bengtsson G, Kärnefelt I, Björn LO (2001) Provitamins and vitamins D2 and D3 in Cladina spp. over a latitudinal gradient: possible correlation with UV levels. J Photochem Photobiol B 62:118–122
Washburn EW, Washburn EW et al (eds) (1929) International critical tables of numerical data, physics chemistry and technology, vol 5. McGraw-Hill, New York, p 270
Webb AR, de Costa B, Holick MF (1989) Sunlight regulates the cutaneous production of vitamin D3 by causing its photodegradation. J Clin Endocrinol Metab 68:882–887
Whistler D (1645) Morbo puerili Anglorum, quem patrio idiomate indigenae vocant The Rickets. Lugduni Batavorum 1–13
Whitfield GK, Dang HTL, Schluter SF, Bernstein RM, Bnag T, Manzon LA, Hsieh G, Domnguez CE, Youson JH, Haussler MR, Marchalonis JJ (2003) Cloning of a functional vitamin D receptor from the lamprey (Petromyzon marinus), an ancient vertebrate lacking a calcified skeleton and teeth. Endocrinology 144(6):2704–2716
Wickelgren I (2007) A healthy tan? Science 315:1214–1216
Yuk JM, Shin DM, Lee HM, Yang CS, Jin HS, Kim KK, Lee ZW, Lee SH, Kim JM, Jo EK (2009) Vitamin D3 induces autophagy in human monocytes/macrophages via cathelicidin. Cell Host Microbe 6:231–243
Zarowitz BJ (2008) The value of vitamin D3 over vitamin D2 in older people. Geriatr Nurs 29:89–91
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Norval, M., Björn, L.O. (2015). Vitamin D: Photobiological and Ecological Aspects. In: Björn, L. (eds) Photobiology. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1468-5_23
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1468-5_23
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1467-8
Online ISBN: 978-1-4939-1468-5
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)