
Abstract
Intestinal transplantation (ITx) represents the physiologic alternative to total parenteral nutrition (TPN) for patients suffering from life-threatening complications of irreversible intestinal failure. The number of transplants performed worldwide has been increasing for several years until recently. ITx has recently become a valid therapeutic option with a graft survival rate between 80 % and 90 % at 1 year, in experienced centers. These results have been achieved due to a combination of several factors: better understanding of the pathophysiology of intestinal graft, improved immunosuppression techniques, more efficient strategies for the monitoring of the bowel graft, as well as control of infectious complications and posttransplant lymphoproliferative disease (PTLD). In fact, this procedure is associated with a relatively high rate of complications, such as infections, acute rejection, graft versus host disease (GVHD), and PTLD, if compared to the transplantation of other organs. These complications may be, at least in part, the consequence of the peculiarity of this graft, which contains gut-associated lymphoid tissue and potentially pathogenic enteric flora. Furthermore, in these patients, the existing disease and the relative malnutrition could predispose them to infectious complications. Additionally, other factors associated with the procedure, such as laparotomy, preservation injury, abnormal motility, and lymphatic disruption, could all be implicated in the development of complications.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Intestinal transplantation
- Total parenteral nutrition
- Living donor intestinal transplantation
- Donor selection
- Recipient selection
- Posttransplant lymphoproliferative disease
- Surgical technique
- Ethical considerations
Introduction
Intestinal transplantation (ITx) represents the physiologic alternative to total parenteral nutrition (TPN) for patients suffering from life-threatening complications of irreversible intestinal failure. The number of transplants performed worldwide has been increasing for several years until recently (Fig. 4.1) [1]. ITx has recently become a valid therapeutic option with a graft survival rate between 80 % and 90 % at 1 year, in experienced centers [1]. These results have been achieved due to a combination of several factors: better understanding of the pathophysiology of intestinal graft, improved immunosuppression techniques, more efficient strategies for the monitoring of the bowel graft, as well as control of infectious complications and posttransplant lymphoproliferative disease (PTLD) . In fact, this procedure is associated with a relatively high rate of complications, such as infections, acute rejection, graft versus host disease (GVHD), and PTLD, if compared to the transplantation of other organs [2–5]. These complications may be, at least in part, the consequence of the peculiarity of this graft, which contains gut-associated lymphoid tissue and potentially pathogenic enteric flora. Furthermore, in these patients, the existing disease and the relative malnutrition could predispose them to infectious complications. Additionally, other factors associated with the procedure, such as laparotomy, preservation injury, abnormal motility, and lymphatic disruption, could all be implicated in the development of complications.

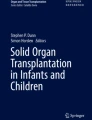
Intestine transplant performed worldwide since 1985
Data from the Scientific Registry of Transplant Recipients (SRTR) show that most of the intestinal transplants have been performed in the US using intestinal graft obtained from cadaver donors (Fig. 4.2) [6]. Differently to what occurred in liver and kidney transplantation , the use of living donors for ITx has been limited mostly because deceased intestinal donors are available. However, optimal deceased intestinal donors are not common either. In fact, despite the fact that the number of patients waiting for ITx is limited, the time spent on the waiting list increased compared to previous years for all candidates on the waiting list. In 2011, 41.7 % of patients listed waited less than 1 year for ITx, while 25.1 % waited between 1 and 2 years, and 33.2 % waited for more than 2 years [6]. Despite the fact that mortality on the waiting list has decreased in the US in recent years compared to the past, it is still reported to be up to 20 % per year on the waiting list [6, 7]. All this suggests that despite the fact that many cadaver donors are available, they are often not utilized because they are not adequate to satisfy the need of patients waiting for ITx.

Growth of living donor and deceased donor intestinal transplantation worldwide by era. LV living donors, DD deceased donors
Intestinal Transplant Registry data show that patient and graft survival rates after living donor ITx (LD-ITx) are similar to those obtained with cadaver organs [1, 7–10]. However, it is important considering that most of the LD-ITx surgeries were performed in low-volume centers (often as isolated cases in low-experience centers), while the best results obtained with ITx from cadaver donors are obtained in high-volume centers, suggesting that increasing the use of LD-ITx could further improve outcome. In fact, the use of intestinal grafts from living donors, when compared to cadaver donors, offers important advantages with low risks, and these are summarized in Table 4.1.
As mentioned above, LD-ITx virtually eliminates waiting time and could further decrease morbidity and mortality on the waiting list compared to the activity seen on the deceased donor list. LD-ITx also would allow transplantation in developing countries where TPN and deceased donor are not easily available. Furthermore, because LD-ITx is an elective procedure, it can be performed when the donor and the recipient conditions are optimal, and the donor bowel preparation can be easily performed, leading to a decreased risk of infectious complications. In an analysis of 50 pediatric ITx recipients, it has been shown that the length of graft preservation was the most significant factor in inducing bacterial translocation [11, 12]. This phenomenon can contribute to the high rate of infections seen during the early posttransplant period also considering that this coincides with the timing of maximum amount of immunosuppression given to the patient.
The Achilles’ heel of bowel transplantation remains its extreme sensitivity to preservation injury. Deceased donors are often subject to either cardiac arrest or resuscitation, to prolonged periods of hypotension, or use of vasopressors. All these could result in splanchnic hypoperfusion, which can trigger ischemia/reperfusion injury even before the intestine is procured from the donor. Cold preservation of the graft can be also extended due to the distance between procurement and transplant centers. This can further increase such injury considering that specific preservation solutions designed for intestinal grafts are not yet available. The use of living donors can obviate these problems, since the donor is a healthy individual, hemodynamically stable, and with consequent normal intestinal perfusion. Furthermore, the short cold ischemic time prior to revascularization also improves graft quality, virtually eliminating ischemia/reperfusion injury, and may reduce the rate of posttransplant infections [12].
Another not negligible benefit of LD-ITx is immunologic [8, 9]. A living donor is often a relative of the recipient due to the strong emotional involvement that justifies the donation. Living related donors have a closer distribution of human leukocyte antigens (HLAs) with the recipient that could contribute to an immunologic advantage. This is supported by the experience of HLA-matched transplants performed between homozygote twins [13]. This point might be challenged since in recent times, a significant decreased rate of rejection has been also observed using HLA-unmatched deceased donors [1, 14]. However, this improvement has been accomplished using more potent immunosuppression and induction therapy with polyclonal antibodies. However, a similarly low rate of rejection is seen using living related HLA-matched donors using a less potent immunosuppressive regimen [8, 9, 15]. An additional benefit can be offered performing LD-ITx at an earlier stage of the disease, since long-term TPN and indwelling venous catheters can be associated with priming of the immune system, as recently suggested [16–18].
Naturally, potential disadvantages are also associated with the use of living donors. The main disadvantage remains the risk for the donor, which includes early surgical complications of bowel resection as well as potential long-term impairment of intestinal absorption. The procedure-specific risks for the live intestinal donor are given in Table 4.2. Specific data on living intestinal donors are limited at this time, and no serious complications have been reported. The potential risk can be hypothetically calculated, using a parallelism with general surgery-related data of small bowel resection; about 3–5 % of the donors could develop a small bowel obstruction [19–24]. In large series, the mortality rate for patients with small bowel obstruction is approximately 2 % for the lifetime of the patient [25]. A brief and self-limited period of diarrhea has been reported after intestinal donation for LD-ITx [15]. Although weight loss and dysvitaminosis are not reported, they represent potential risks of this procedure.
Another disadvantage is associated with the increased risk of vascular thrombosis, related to the smaller vascular pedicle used compared to grafts obtained from cadaver donors. Nevertheless, these risks can be reduced with a careful and appropriate surgical technique [26, 27].
Donor Selection and Evaluation
General Considerations
The potential donor should be an individual in good health with no history of previous intestinal or abdominal surgery, and with no underlying chronic medical illnesses that would increase the surgical operative risk.
Once a potential donor is identified, the initial step should consist of a meeting with the surgeon to describe the procedure, as well as risks and benefits and the steps involved in the workup. During this initial visit, the potential donor can be screened with an ABO blood type determination. If this is compatible and the candidate is willing to continue the workup, an HLA test and histocompatibility testing by T-cell crossmatch should be performed. Crossmatch should be negative, and among multiple donor candidates, the one with the best HLA match should be preferred and should be directed to continue the workup. The cornerstone of success is the identical or compatible HLA. For this reason, it is preferred that living donors be relatives of the recipients. The donor can also be unrelated to the recipient but should have a compatible HLA and close emotional relationship. This condition and the absence of any financial interest or coercion for donation are of paramount importance in LD-ITx, just like any other type of live organ donation. The screening process should exclude active or uncontrolled psychiatric disorders, and ensure the altruistic nature of the donation. The institution’s ethical committee should separately evaluate the donor to ensure that there is full understanding of the limited information regarding the short- and long-term risks associated with intestinal donation.
Full Evaluation
Once the potential donor has completed these initial steps, a series of tests are mandatory for the live donor evaluation (Table 4.3). Based on the available clinical experience with LD-ITx, a limit of 60 years of age is advisable. The minimal age is only determined by legal ability to consent to the procedure. High body mass index (> 30) may not affect graft quality and does not constitute, per se, an absolute contraindication to live donation, though general surgical experience indicates that a high body mass index (> 30 kg/m2) may increase the risk of surgical complications after intestinal resection.
A comprehensive metabolic panel should be obtained. Blood test results that confirm donor infection with HIV, HCV, or HBV are contraindications for living intestine donation.
Specific considerations must be used for genetically related donors of potential recipients who have a genetic or familial intestinal disease. Despite the fact that no data are available at this time, it is possible that the related donor might develop the same condition later in life. At the present time, it is advisable not to consider these donors and eventually to screen them to rule out the same genetic disorder.
Imaging studies are performed to rule out underlying or occult pathology and to specifically delineate the intestinal vascular anatomy. A computed tomography (CT) or magnetic resonance (MR) angiography is performed, possibly with computerized three-dimensional (3D) reconstruction, if available. In case, these techniques are not available or are inadequate, a traditional angiogram can be also performed. Angiography is performed to evaluate the superior mesenteric artery (SMA) anatomy, to ensure a normal vascular distribution to the small bowel with particular attention to the right colic and ileocolic arteries and the terminal branches of the SMA, and to exclude the presence of atherosclerotic disease and abnormal anatomy. If more than one donor is available, patients with a single distal arterial pedicle should be preferred to patients with multiple vessels. These vessels usually originate caudal to the takeoff of the right colic artery and must be spared during procurement to provide adequate blood supply to the cecum, terminal ileum, and ileocecal valve (Fig. 4.3).

Mesenteric angiography
Indications and Recipient Selection
The indications for ITx are identical using either a living or a deceased donor. This transplant should be considered for patients with irreversible intestinal failure requiring TPN. This can be caused by short gut syndrome (Figs. 4.4 and 4.5) related to the loss of over 70 % of the native small bowel length (< 100 cm of residual intestine), defective gastrointestinal (GI) motility, impaired enterocyte absorptive capacity, genetic malformations of the GI tract or abdominal wall, or neoplastic disease [1]. The irreversibility of intestinal failure is based on the length and function of the remaining native bowel and its inability to provide sufficient fluid and nutritional support. Intestinal rehabilitation can correct this condition in up to 50 % of patients requiring chronic TPN, and should be always attempted before considering transplantation [28, 29].

Indications for intestinal transplantation in adults

Indications for intestinal transplantation in children
Inclusion Criteria
A patient diagnosed with intestinal failure is not automatically considered an ITx candidate. Usually, these patients are considered transplant candidates only when TPN-related complications arise. These criteria are summarized in Table 4.4.
Impending Liver Failure Due to TPN-Induced Cholestasis
TPN-induced cholestasis is a condition of impaired canalicular secretion of bile, characterized by bile duct regeneration, portal inflammation, and fibrosis. It is diagnosed in patients receiving TPN who develop cholestasis not due to other liver diseases or biliary obstruction. The clinical manifestations include elevated serum bilirubin and/or liver enzymes, splenomegaly, thrombocytopenia, gastroesophageal varices, coagulopathy, stomal bleeding, or hepatic fibrosis/cirrhosis. Its progression could be very rapid, and in some patients, liver cirrhosis may develop in a few months [30].
Vascular Access
This can be consequent to the thrombosis of the major central venous system, such as jugular, subclavian, and femoral veins. Thrombosis of two or more of these vessels is considered a life-threatening complication and a failure of TPN therapy. The sequelae of central venous thrombosis are the lack of access for TPN infusion, fatal sepsis secondary to infected thrombi, pulmonary embolism, superior vena cava syndrome, or chronic venous insufficiency.
Frequent Line Infections and Sepsis
The development of two or more episodes per year of systemic sepsis, secondary to line infection that requires hospitalization, also indicates failure of TPN therapy. A single episode of line-related fungemia, septic shock, and/or acute respiratory disease syndrome (ARDS) is considered TPN failure.
Frequent Episodes of Severe Dehydration Despite Intravenous Fluid Supplement in Addition to TPN
Under certain medical conditions, such as secretory diarrhea, in GI tract that cannot be reconstructed, the loss of the GI and pancreatobiliary secretions exceed the maximum intravenous infusion rates that can be tolerated by the cardiopulmonary system.
Exclusion Criteria
Several conditions also preclude intestinal transplant. The exclusion criteria are summarized in Table 4.5.
Preoperative Workup
Once a patient with intestinal failure is considered for a transplant, a specific evaluation is performed. The purpose of the evaluation is to determine if the patient would benefit from ITx; to rule out contraindications; and to improve, if possible, the current medical management of these patients. The workup performed in the recipient is similar for either a deceased donor or a live donor (see Table 4.3). The workup is performed by a multidisciplinary team consisting of a transplant surgeon, gastroenterologist, nutrition specialist, cardiologist, anesthesiologist, infectious disease specialist, psychiatrist, and social worker. A multidisciplinary committee discussion and presentation of each case are advisable.
Radiographic Imaging Studies
It is imperative to know the anatomy of the recipient pretransplant. If numerous intestinal resections have been performed over a long period of time, often previous medical records are not available or are inaccurate in recording the remaining portion of the intestine and its length after each surgery. In addition, intraoperative evaluation of the anatomy is often difficult due to the scarring and adhesions found. Upper and lower GI series with contrast will allow one to visualize the portion of residual gut, its position in the abdominal cavity, and its length. It is not uncommon that during a workup, a longer-than-expected segment of small or large intestine is identified, and this might allow different strategies than transplantation, such as surgical recanalization of the residual intestine, intestinal rehabilitation, or other surgical elongation procedures. Abdominal CT scan (or MR imaging) with contrast is also used to rule out malignancies or other undiagnosed diseases.
Patency of the upper and lower body veins must be established by venogram, since duplex scan might not be sufficiently sensitive for this purpose. Thrombosis of these vessels is not uncommon in patients receiving TPN. Thrombosis can cause inability to cannulate the vessels, and can cause superior vena cava syndrome when the inferior vena cava (IVC) is clamped. The patient may have patency only of the femoral veins. Complete lack of venous access could be a contraindication for ITx.
Electrocardiography and echocardiogram are used to determine the cardiac function and any valvular lesions, and should be accompanied by a cardiologic evaluation and clearance for surgery. Stress test or cardiac catheterization may also be performed, if indicated.
Additional Diagnostic Procedures
Liver biopsy may be indicated in patients with intestinal failure and hepatic dysfunction. TPN-induced cholestatic liver injury can be reversed by isolated intestinal transplant or by restoring intestinal integrity [31]. However, in the presence of liver cirrhosis or portal hypertension, a patient with intestinal failure requires a combined liver–ITx. This can be performed using a deceased donor. However, as an option, liver transplant from a deceased donor can be followed by intestinal transplant from a living donor, if an intestinal graft is not attainable from the same donor at the same time. In addition, in pediatric patients, combined liver–ITx from a living donor has been recently reported [10].
Further assessment of associated liver disease (portal hypertension, coagulopathy, ascites, hyperdynamic circulation, hepatopulmonary syndrome, and hepatic encephalopathy) should be done, if indicated.
Patients with familial polyposis should be evaluated for the presence of polyps in the remaining portion of the Gl tract. Patients with dysmotility disorders may require an assessment of the stomach to evaluate functional abnormalities. Children with pseudo-obstruction may require urologic assessment because as many as a third may have a dysfunctional urinary tract. Children with necrotizing enterocolitis may require a full neurologic and pulmonary workup to exclude the possibility of associated intraventricular hemorrhage and bronchopulmonary dysplasia.
Surgical Technique
Background
The transplantation of an intestinal graft from a live donor, by definition, involves the transplantation of a segment of the small intestine. Central caveat of the donor operation is to provide adequate length of intestine to the recipient to ensure enteral autonomy, while preserving enough small bowel length in the donor. The appropriate length and the anatomic origin of the segmental graft to harvest is the cornerstone of a successful transplant.
Anatomical Considerations
The arterial blood supply to the small intestine is from the superior mesenteric artery (SMA) . The basic pattern of distribution of the intestinal arteries generally includes 5 arteries arising on the left of the SMA above the origin of the ileocolic artery and 11 below that level. Eight additional arteries usually originate from the ileal branch of the ileocolic artery [32]. These intestinal vessels branch a few centimeters from the border of the intestine to form arterial arcades connecting the intestinal arteries with one another. Proximally, a single set of arcades is present; distally, there are usually several sets of arcades. These arches form the primary interconnections of the arterial supply. From arches and arcades, the vasa recta arise and pass without cross-communication to enter the intestinal wall. A complete channel may also exist from the posteroinferior pancreaticoduodenal artery that is parallel to the intestine and joins the marginal artery of Drummond of the colon. The terminal ileum, ileocecal valve, and right colon receive blood supply also from the right colic artery and ileocolic artery, often sharing a common origin, connected by the marginal artery of Drummond to the terminal branches of the SMA (Fig. 4.6). In 5 % of the population, blood supply to these structures is guaranteed only by the ileocolic artery, as the marginal artery is incomplete (Fig. 4.7). The venous drainage of the small intestine is less complex than the arterial vessels, merging in the jejunal and ileal veins, and into the superior mesenteric vein and portal vein.

Vascular supply to the small intestine from SMA. The terminal ileum, ileocecal valve, and right colon receive blood supply also from the right colic and ileocolic arteries, and are connected by the marginal artery of Drummond. CB colic branches, ICA ileocolic artery, MCA middle colic artery, RCA right colic artery, SMA superior mesenteric artery. (From Tan HP, Marcos A, Shapiro R, Living donor organ transplantation, 1st edition, copyright © 2007, Informa Healthcare. Reproduced with permission of Informa)

Vascular supply to the small intestine from SMA. The marginal artery is incomplete in 5 % of the population. IMA incomplete marginal artery, ICA ileocolic artery, MCA middle colic artery, RCA right colic artery, SMA superior mesenteric artery. (From Tan HP, Marcos A, Shapiro R, Living donor organ transplantation, 1st edition, copyright © 2007, Informa Healthcare. Reproduced with permission of Informa)
From a technical standpoint, the ileum offers the advantage of a larger vascular pedicle if the distal portion of the SMA is used. This vessel can be transected below the takeoff of the right colic artery to avoid hypoperfusion of the terminal ileum, and the preservation of the ileocecal valve in the donor (Fig. 4.8). At this level, this artery is commonly single, but could also consist of two or more branches. Additionally, despite the fact that both jejunum and ileum have the ability to adapt following intestinal resection, the ileum has the advantage of allowing structural and functional adaptation [33, 34].

From a technical standpoint, the ileum offers the advantage of a larger pedicle if the distal portion of the superior mesenteric artery is used. This vessel can be transected below the takeoff of the right colic artery to avoid hypoperfusion of the terminal ileum and ileocecal valve, which are always preserved in the donor. CB colic branches, ICA ileocolic artery, MCA middle colic artery, RCA right colic artery, SMA superior mesenteric artery. (From Tan HP, Marcos A, Shapiro R, Living donor organ transplantation, 1st edition, copyright © 2007, Informa Healthcare. Reproduced with permission of Informa)
Despite these advantages, the jejunum has been also used in early experience for the possible immunologic advantages, since it has been reported, from small-animal studies, that acute rejection is less severe in the jejunum [35, 36]. However, the vascular distribution to the jejunum makes the operation more complex, as the segmental graft obtained has numerous arterial branches needing multiple anastomoses in the recipient to obtain adequate revascularization for the graft (Fig. 4.9). Jaffe et al. reported attempts at proximal small bowel transplantation involving complex vascular reconstruction that resulted in vascular complications [35]. In addition, the early clinical experience from the same group did not show a clear immunologic advantage with the use of jejunal segmental grafts.

The vascular distribution to the jejunum makes the operation more complex as the segmental graft obtained has numerous arterial branches needing multiple anastomoses in the recipient to obtain adequate revascularization of the graft. CB colic branches, ICA ileocolic artery, MCA middle colic artery, RCA right colic artery, SMA, superior mesenteric artery. (From Tan HP, Marcos A, Shapiro R, Living donor organ transplantation, 1st edition, copyright © 2007, Informa Healthcare. Reproduced with permission of Informa)
Optimal Length of the Segmental Graft
The appropriate length of the human alimentary tract to be resected has proven to be surprisingly difficult to measure. The length of the small intestine in deceased donors was reported to be from 10 to 40 feet, with an average of 20.5 feet or 624.8 cm [37]. In vivo measurements using an intraluminal method provided an average of 8.5 feet or 258 cm [38]. This discrepancy is attributed to the postmortem loss of longitudinal muscle tune of the small intestine that can lead to an increase in length, up to 135 % in a few hours, as shown in animal studies [39]. For the purpose of ITx, intestinal measurements are performed in a live subject, but being under general anesthesia, the effect of the pharmacologic agents used might affect the intestinal distension, motility, and length [40–43].
For these reasons, the calculation of a generic optimal length of small bowel graft to resect can be difficult. In each individual case, the entire small bowel should be measured from the ligament of Treitz to the ileocecal valve, using a sterile surgical tape. Once the length of the entire small bowel is determined in a particular patient under a specific anesthetic agent, a final determination of the segment to be removed is made. Although it is relatively easy to determine when an intestinal segment is too short, the long-term impact to the donor of the resection of a longer segment is unknown. Deltz reported a transplant of a 60-cm segment of distal jejunum and proximal ileum, whereas, Morris used a similarly long segment of distal ileum, ileocecal valve, and a portion of the cecum [44, 45]. Despite these early successes, a length of 60-cm small bowel has been generally inadequate to provide a TPN-free condition [44], and resection of the ileum, ileocecal valve, and cecum can have a negative impact on the function of the remaining donor bowel (e.g., increased transit time and vitamin B12 deficiency) [45].
From the short-bowel syndrome literature, a segment of approximately 1 m has been reported to be sufficient to ensure adequate absorption [29]. However, this depends on the presence of the ileocecal valve or part of the colon. Considerations in the recipient anatomy also play an important role in determining the length of the intestinal segment to remove in the donor. A recipient with no colon or ileocecal valve, for example, will require a longer segment compared with a patient where these structures are present.
Donor safety is, of course, paramount, and this will determine the upper limit of the length of resection. The resection of a long segment might induce malabsorption and weight loss, and the removal of terminal ileum might induce the malabsorption of bile salts, vitamin B12, and chronic diarrhea. It is clear that the ileocecal valve and terminal ileum should be preserved in the donor, and that the segment of intestine to be removed should be the ileum. Only 20–30 % of the total length of the small intestine should be resected to minimize risk to the donor, as no data are available to determine the ideal length of the intestine to preserve. The successful use of ileal segments between 150 and up to 200 cm of length has been reported, with no sign of long-term complications in the donors [15]. Generally, the expectation is that the adaptation of the residual intestine will take place, compensating for the segment removed, and reestablishing a completely normal functional condition. However, although data exist about posttransplant adaptation in the recipient, such evidence is not yet available in the donor [26, 27].
Pollard was the first to report the use of a segment of ileum with the distal mesenteric artery and vein for an LD-ITx; however, no information was given regarding the distal terminal ileum and blood supply to the remaining cecum and ileocecal valve [46]. Subsequently, Gruessner reported a case describing the surgical technique utilized to preserve these structures [47].
Donor
Preoperative Orders
Preoperative orders are individualized by each transplant center. A mechanical bowel preparation and preoperative intestinal decontamination are preferred. A final crossmatch should be performed and stool cultures obtained. An example of these orders is shown in Table 4.6.
Surgical Procedure
A schematic illustration of the donor operation is shown in Fig. 4.10. The donor operation is performed with the patient in a supine position, using a midline incision from approximately 4 cm above the umbilicus to 2 cm above the pubis. The small intestine is inspected and measured from the ligament of Treitz to the ileocecal valve. The terminal ileum is identified, and a mark is placed at 15–20 cm from the ileocecal valve using a silk stitch in the serosal layer. This segment of terminal ileum is preserved and its blood supply maintained by the ileal branches of the ileocolic artery, usually originating from the right colic artery. The total length of the intestinal segment to be removed is based on the recipient anatomic characteristics and donor total intestinal length. This measurement starts at the previously placed mark proceeding cranially in the ileum, and is marked with another silk stitch in the serosal layer. At this point, the segment of ileum to be removed is identified, and is included between the two marks. Different marks should be used proximally and distally to identify later the orientation of the intestinal graft. The terminal branches of the SMA and vein are identified and dissected from the surrounding tissue, and identified with vessel loops near the origin of the right colic artery (Fig. 4.11). The origin of the right colic artery is also identified with a vessel loop. The line of transection of the SMA will be below this point to preserve the right colic artery in order to provide blood supply to the terminal ileum, ileocolic valve, and cecum with its ileocolic branches.

A schematic illustration of the donor operation is shown. (From Tan HP, Marcos A, Shapiro R, Living donor organ transplantation, 1st edition, copyright © 2007, Informa Healthcare. Reproduced with permission of Informa)

The terminal branches of the superior mesenteric artery and vein are identified and dissected from the surrounding tissue and identified with vessel loops near the origin of the right colic artery. SMV superior mesenteric vein, RCA right colic artery, SMA superior mesenteric artery
Careful inspection by transillumination of the vascular arcades is performed (Fig. 4.12). The peritoneum of the mesentery is initially scored with electrocautery, and the mesenteric tissue is dissected; the vascular arcades encountered are ligated and divided between silk ties. The line of dissection of the mesentery starts from the marks on the ileum and is directed toward the previously dissected and looped blood vessels. Once all the dissection is performed, the intestinal segment is still vascularized through a triangle of mesentery containing the distal superior mesenteric vessels (Fig. 4.13). Once the recipient is ready in the adjacent operating room, the intestine is transacted using a gastrointestinal anastomosis (GIA) stapler. Adequate blood supply to the proximal and the distal stumps of the ileum is confirmed when it is transected by GIA stapler (Fig. 4.14). The ileocolic vessels are clamped and transacted, and the vasculature of the intestinal segment is flushed using 4℃ cold preservation solution on the back table. As the graft is transported to the recipient operating room for transplantation, the vascular stumps in the donor are ligated using nonabsorbable monofilament stick ties. The proximal and distal segments of the ileum are re-anastomosed primarily using either a GIA or a manual technique. To avoid intraperitoneal spillage of intestinal content, the intestine is clamped using linen-shod noncrushing Doyen clamps closed at one to two clicks. If the manual technique is used, our preference is to use an absorbable monofilament for the mucosal layer and a nonabsorbable monofilament for the sero-muscular layer using Lambert or Cushing stitches. A side-to-side technique is preferred to minimize the risk of stenosis. The mesenteric defect should be closed carefully. The abdomen is then closed using absorbable monofilament for the fascia and subcuticular for skin closure; the surgical drain is not necessary.

Careful inspection by transillumination of the vascular arcades is performed. (From Tan HP, Marcos A, Shapiro R, Living donor organ transplantation, 1st edition, copyright © 2007, Informa Healthcare. Reproduced with permission of Informa)

Once the dissection is completed, the intestinal segment is still vascularized through a triangle of mesentery containing the distal superior mesenteric vessels. (From Tan HP, Marcos A, Shapiro R, Living donor organ transplantation, 1st edition, copyright © 2007, Informa Healthcare. Reproduced with permission of Informa)

The picture shows adequate blood supply to the proximal and distal stumps of the graft. (From Tan HP, Marcos A, Shapiro R, Living donor organ transplantation, 1st edition, copyright © 2007, Informa Healthcare. Reproduced with permission of Informa)
Postoperative Management and Follow-Up
Postoperative orders are substantially similar to the orders used for a general surgical patient undergoing small intestinal resection.
The recommended minimum follow-up includes postoperative visits for the first 4 weeks. There are several risks potentially associated with the donor operation that could occur early in the postoperative period, such as diarrhea, weight loss, dysvitaminosis, and small bowel obstruction, whereas the long-term risk of small bowel resection primarily involves small bowel obstruction. Donors should be followed until all procedure-related symptoms have been resolved. B12 deficiency can be monitored by performing serum levels at 6 months and annually for 3 years. Donor data should be collected and submitted to the intestinal transplant registry.
Recipient
Preoperative Orders
Preoperative orders are, again, individualized by each transplant center. An example of our preference is shown in the preoperative orders exhibited in Table 4.7.
Surgical Procedure
A schematic illustration of the recipient operation is shown in Fig. 4.15. The recipient operations for isolated ITx from living or deceased donors are not different, except for the length of the intestinal graft and the vascular pedicle. These patients can present with a variety of anatomic differences in their native intestine. These can go from the presence of the entire dysfunctional intestine in patients with pseudo-obstruction, to the ultra-short gut syndrome with only a portion of the duodenum intact. In all cases, the anatomy should be well identified pretransplantation to plan the best surgical approach. The goal of the operation is to reestablish intestinal continuity by transplanting the segment of ileum recovered from the donor. The proximal and distal (if present) segments of intestine in the recipient should be always preserved and used for the anastomosis. The presence of a segment of colon or ileocecal valve in these patients would decrease the transit time and increase absorption and would allow a shorter ileal graft to be transplanted.

The picture shows a schematic illustration of the recipient operation. (From Tan HP, Marcos A, Shapiro R, Living donor organ transplantation, 1st edition, copyright © 2007, Informa Healthcare. Reproduced with permission of Informa)
Often, these patients develop short bowel syndrome as a consequence of multiple surgical resections. In this case, the presence of diffuse intra-abdominal adhesions requires a long and careful dissection to identify vascular and intestinal structures and anomalies. For this reason, we start the recipient operation first and initiate the procedure in the donor in the adjacent operating room only when the recipient anatomy is identified. A midline incision from the xiphoid process to the pubis is used. The operation is carried out to identify the aorta, vena cava, and the proximal and distal intestinal stumps. Once this is accomplished, the graft is removed from the donor and is transported in the recipient operating room. The previously dissected aorta and vena cava are used for the anastomoses. The vena cava is clamped in its infrarenal portion with a Satinsky vascular clamp. The ileocolic vein is anastomosed end to side with running nonabsorbable monofilament. The mesenteric artery is anastomosed end to side to the aorta after this vessel is also clamped using a vascular clamp. In this case, a running or interrupted anastomosis is performed, depending on the size of the vessel using nonabsorbable monofilament. If the vascular pedicle consists of multiple arteries, these are anastomosed individually. Once the vascular anastomoses have been completed, the intestinal graft is reperfused (Fig. 4.16). The proximity of the vena cava and aorta allows anastomosis without tension, as the vascular pedicle of the graft can be short. However, an alternative vascular approach, for example, using the portal vein, could also be utilized.

Once the vascular anastomoses have been completed, the intestinal graft is reperfused. (From Tan HP, Marcos A, Shapiro R, Living donor organ transplantation, 1st edition, copyright © 2007, Informa Healthcare. Reproduced with permission of Informa)
Intestinal continuity is immediately reestablished anastomosing the proximal end of the graft, previously marked in the donor, to the proximal intestinal stump available in the recipient. Often, this is the duodenum or the proximal jejunum. Care should be taken not to shorten the native intestine unless pseudo-obstruction or motility disorder is present. The intestine is anastomosed using a hand-sewn technique side to side along its anti-mesenteric border. Our preference is to use absorbable monofilament for the mucosal layer and a nonabsorbable monofilament for the seromuscular layer using Lambert or Cushing stitches. The same is done for the distal portion of the graft if a segment of colon is available. To avoid intraperitoneal spillage of the intestinal content, the intestine is clamped using linen-shod noncrushing Doyen clamps closed at one to two clicks. A temporary loop ileostomy is constructed and is maintained for 6 months. This is used for endoscopy, feces sample collection, and the evaluation of the graft mucosa visible in the stoma. Construction of the loop ileostomy is performed after the intestinal anastomoses have been completed, and intestinal continuity is reestablished. At this point, a site in the lower quadrant is identified to perform the ileostomy without tension, depending on the length of the mesenteric vessels, the anatomy of the recipient, and the intestinal reconstruction performed. This is performed excising a 2-cm diameter circle of skin followed by a 2-cm incision of the fascia. The muscle fibers are spread and the tips of two fingers should be easily introduced into the opening. The loop should be gently exteriorized using a Babcock clamp, and a rod is introduced in a small opening of the mesentery to keep the loop in position. The anterior wall of the ileum is opened slightly more than 50 % of its circumference. The proximal stoma is larger and is kept cephalad. The ileostomy is matured with mucocutaneous fixation using interrupted sutures. Sutures are also used to secure the graft to the peritoneum to prevent herniation, and to help in identifying the proximal and distal end of the ileostomy for future endoscopy.
If no colon is available, a permanent end ileostomy is constructed. If possible, this is performed approximately 5 cm to the right of the midline incision and about 4 cm below the umbilicus. The presence of scar from previous surgeries might mandate a different location. The end ileostomy is performed excising a 2-cm diameter circle of skin followed by a 2-cm incision of the fascia. After spreading the muscle, two fingers should be easily introduced into the opening. The distal end of the graft should be gently exteriorized using a Babcock clamp, preserving the marginal artery and with the mesentery cephalad. The end ileostomy is matured with mucocutaneous fixation using interrupted sutures. Intraperitoneal sutures are used to secure the graft to prevent herniation or prolapse of the stoma.
Abdominal closure is performed in two layers using nonabsorbable monofilament for the fascia and surgical staples for the skin. If tension exists on the fascia at the time of closure, this should not be attempted to reduce the risk of thrombosis. The skin can be approximated leaving the fascia open. This approach may require a complex plastic reconstruction later [48]. The abdominal wall fascia can be alternatively closed without tension using a biological acellular dermal matrix that has been previously described to be safe in this setting [49].
Postoperative Orders
Postoperative orders are individualized by each transplant center. Several protocols of immunosuppression can be used. Our preference is shown in the postoperative and transfer orders shown (Table 4.8).
Current Outcome of ITx and LD-ITx
Intestinal transplant outcome drastically improved over time, and 1-year graft survival in the US now exceeds 80 % [1]. Unfortunately, longer-term outcomes have failed to improve over time and the 5-year patient survival rates for all types of ITx are approximately 50 %. Graft rejection and/or infection are still the most common causes of early and late deaths. The inability to completely control rejection has resulted in heavier immunosuppression; consequently, infectious complication and malignancy were the cause of death in a substantial percentage of patients. LD-ITx offers theoretical advantages that could help to address these problems [8–10].
In fact, even among the early attempts made to transplant the intestine in the 1960s and early 1970s in the pre-cyclosporine era, the longest survivor (76 days after transplantation) received an HLA-identical ileal segment from her sister [50]. However, of 2,611 ITxs performed worldwide until 2009, only 66 (2.5 %) were performed from living donors [1, 6]. Indeed, the potential benefits of live donation must be weighed against the potential disadvantages of LD-ITx, which include risk to the donor, shorter segment of the intestinal graft, and the limited experience available [51, 52].
Donors
At this time, no donor deaths or long-term morbid complications in intestinal donors have been reported. Only a 1-–2-week period of postoperative diarrhea has been described [15]. However, this is usually self-limited and does not require aggressive therapy. In our experience, donors maintain their presurgical weight and, in some instances, tend not to gain weight even after increasing their caloric intake during the first few months. This is probably because of an adaptation of the remaining shorter segment of ileum left in the donor. No studies have been published at this time regarding bowel adaptation or absorption in donors following the donor enterectomy, probably a function of lack of symptoms and an understandable desire to minimize postoperative visits in these otherwise healthy individuals. Additionally, no data have been collected on vitamin absorption. However, even if the distal ileum has been utilized, most of the LD-ITx performed in recent years have been performed with careful preservation of the terminal ileum, which should prevent these problems.
Unfortunately, these patients are followed only for a limited period of time. It has been recently recommended that data on long-term follow-up of these donors should be collected. For example, vitamin B12 should be monitored with serum levels at 6 months, and annually for 3 years. In addition, recent recommendations have been developed to create a donor registry in conjunction with the existing International Intestinal Transplant Registry to evaluate the long-term risk of the procedure to the donor [53].
Recipient Outcomes
LD-ITx is not routinely performed; therefore, few reports of short- and long-term outcomes exist. The largest series, reported by the University of Illinois at Chicago, included 13 patients who underwent transplantation of 150–200 cm of terminal ileum proximal to the ileocecal valve [10]. Five of them had a combined liver–ITx. The 1- and 3- year actuarial patient and graft survival rates in patients with LD-ITx only were 60 and 50 %, respectively. In combined liver–LD-ITx recipients the patient survival rates at 1 and 2 years were 100 %; the liver graft survival rate was 100 %, and the bowel graft survival 80 %. Three LD-ITx recipients developed acute rejection, and another recipient developed chronic rejection 3.5 years after the original transplant and died after re-transplantation [46, 47].
Intestinal graft survival has steadily improved over time. Close to half of the patients who have undergone LD-ITx are currently alive today [9, 10]. This is probably an underestimated survival, considering the high rate of failure of the early attempts (historical data). Causes of death included sepsis (29 %), liver failure (5 %), rejection (5 %), and other causes (10 %). Only one patient lost the intestinal graft to vascular thrombosis (2.5 %). This suggests that the small vascular pedicle in LD-ITx is not a significant risk factor for graft loss when compared with deceased donor grafts, as the technical results are at least comparable with those seen with deceased donors (2.5 % vs. 15–20 % graft loss, respectively). In previous reports, center volume had no effect on graft survival, but this may reflect the small number of procedures performed worldwide. There was no difference in graft survival or patient survival when comparing LD-ITx and ITx. However, with increased center experience in LD-ITx, it is possible that an improved survival might be obtained, like it is observed in large centers performing ITx from cadaver donors.
Rejection and Immunosuppression
The rate of rejection in ITx from deceased donors has been higher than that observed with other organs, and possible benefits may exist with HLA-matched live donors.
Grafts obtained from deceased donors have not been HLA-matched, mostly because intestinal grafts have been at least initially transplanted in association with the liver. However, living-related donors often have a better HLA match. This benefit is supported by the experience of ITx performed between homozygous twins [54]. In addition, low or no rejection has been documented in living-donor HLA-matched intestinal grafts during the first year posttransplantation, and have had good long-term graft function [55].
Rejection was a cause of death in 3.8 % of the patients transplanted with deceased donor organs, and 4.8 % in patients transplanted with LD-ITx. However, graft loss was related to rejection in 56 % of the transplants performed from deceased donors and 30 % in patients transplanted from living donors.
To date, no additional data are available, as donor and recipient tissue typing information has not been collected and analyzed. A recent improvement in the rate of rejection has been reported in deceased donor transplants using antibody induction therapy with anti-interleukin-2 (IL-2) receptor blockers due to their powerful anti-rejection properties combined with the lack of side effects in terms of direct toxicity and development of infection or malignancy [56].
Posttransplant Lymphoproliferative disease
PTLD is a serious complication of intestinal transplantation , and is related to the heavy immunosuppression that is required to prevent rejection. Recent data show that the overall incidence of PTLD was 11.8 % with a median onset 21 months after transplantation. A total of 50 % of cases resulted in graft failure or death. In contrast, PTLD was never reported as the cause of death in LD-ITx recipients. In these patients, the ability to use a less aggressive immunosuppressive regimen could have a beneficial impact on the incidence of PTLD [57].
Graft Adaptation
Deltz et al. reported a successful transplant of a 60-cm segment of distal jejunum and proximal ileum, and Morris et al. successfully used a 60-cm segment of distal ileum, ileocecal valve, and a portion of the cecum [44, 45]. Despite these early successes, a length of 60 cm of the bowel is generally inadequate [45]. From the short bowel syndrome literature, a segment of approximately 1 m has been reported to be sufficient to ensure adequate absorption [58], depending on the presence of ileocecal valve or part of the colon. The successful use of ileal segments of length between 150 and 200 cm have been reported, with no sign of long-term complication for either the donors or the recipients [59]. Furthermore, adaptation of the remaining intestine occurs, compensating for the segment removed and reestablishing completely normal function.
Intestinal grafts show evidence of functional adaptation in recipients (see Table 4.3). This occurs because of a morphologic adaptation characterized by increased length and size of the villi (see Figs. 4.8 and 4.9) [26].
Given the experience reported thus far, it seems that ileal grafts measuring 150– 200 cm of the distal ileum (without the ileocecal valve) will provide sufficient nutrient absorption to achieve independence from TPN, once adaptation is complete approximately 6 months after LD-ITx .
Ischemic Injury
Intestinal grafts are extremely sensitive to preservation injury. In an analysis of 50 pediatric ITx recipients, it has been shown that the ischemia time was the most significant factor in inducing bacterial translocation [11]. This phenomenon can contribute to the high rate of infections seen during the early posttransplant period, and, of course, also coincides with the timing of the maximum amount of recipient immunosuppression. With living donation, this problem is obviated, if the donor is a healthy individual who is hemodynamically stable, and this minimizes pre-recovery gut hypoperfusion. Furthermore, the short cold ischemia time, limited to a few minutes’ transport of the graft between donor and recipient operating rooms, virtually eliminates ischemia/reperfusion injury. This is documented by the fact that mucosal biopsies and zoom-endoscopy evaluation performed early after LD-ITx show no evidence of ischemic injury [60].
Ileal Compared with Jejunal Segmental Graft
In the early clinical experience, both jejunum and ileum were used. Jaffe et al. [59] reported attempts at proximal small bowel transplantation involving complex vascular reconstruction that resulted in vascular complications. Furthermore, the early clinical experience from the same group did not show an immunologic advantage for jejunal grafts. Currently, most transplant surgeons today prefer using distal ileal grafts.
Cost-Effectiveness
A cost analysis in the US for TPN reveals that the cost per patient in 1992 was approximately US$ 150,000 per year only for supplies, not including the cost of frequent hospitalizations, medical equipment, and nursing care, and that the national cost of home TPN for Medicare was US$ 780 million in 1992 [61]. The cost of an intestinal transplantation performed from a deceased donor has been analyzed in the US and varies according to the type of transplant performed. This was estimated in 1994–1998 to average US$ 132,285 for isolated intestinal transplant, US$ 214,716 for combined liver–ITx, and US$219,098 for multivisceral transplants [62]. The cost of LD-ITx was estimated to be US$ 16,000 ± 2,000 for the donor workup and hospitalization, US$ 113,000 ± 26,000 for the recipient hospitalization, US$3,900 ± 750 for yearly routine follow-up, and US$ 20,000 for the first year, followed by US$ 3,000 per year thereafter for immunosuppression [22]. Compared with the cost of TPN, LD-ITx is cost-effective after the first year, and it is also less expensive than deceased donor-isolated ITx.
Quality of Life
The quality of life of recipients undergoing LD-ITx has been evaluated before the injury, while TPN-dependent, and following transplantation [63–68]. The premorbid period was defined as the patient’s normal state of health prior to becoming TPN-dependent. The morbid phase was the period when patients were TPN-dependent.
Quality of life was measured with the Quality of Life Inventory (QOLI), designed for transplant recipients, and previously validated in liver transplant patients and in ITx patients at the T.E. Starzl Translpant Institute at the University of Pittsburgh Medical Center [69, 70]. These patients, when comparing “before illness” with “during illness” (while on TPN), reported disruption in most areas of their lives, except for marital relationships, medical compliance, and medical satisfaction, which were unchanged from before illness. After transition from TPN dependence to posttransplant TPN independence, when comparing posttransplant status with that during illness (while on TPN), patients reported a significant improvement in most areas of quality of life: psychological (less anxiety, less depression, better mental status, increased stress experience, improved optimism, less impulsiveness and improved control, increased sexuality, and improved coping); physical (better mobility, better appearance, decreased gastrointestinal and genitourinary symptoms, improved sleep, and improved energy); and social (more ability to perform and enjoy recreation activities, improved quality of social support, and improved quality of relationships). The patients did not report worsened quality of life in any area. These patients reported that their posttransplant status compared favorably with their pre-illness condition. Of the 26 domains, only 5 areas of functioning were statistically worse than (pretransplant or TPN patients: loss of control, poorer sleep, increased pain and discomfort, poor quality of social supports, and difficulty in parenting. Regarding employment, all were working full time before becoming TPN-dependent. When they became TPN-dependent, none maintained their working status. All these patients recovered their working status, and one also achieved paternity 36 months after the LD-ITx.
Specific Ethical Considerations
When we are faced with a healthy person, invading a healthy body to obtain an organ for another, the ethical problem is most obvious. Certainly, removal of a kidney from a living person donor was partially justified by the fact that kidneys are paired organs, but what about intestine? To remove an organ from a living donor, as is the case in LD-ITx , ethical problems can arise; the first is the hurdle of the ancient medical maxim, “do not harm,” taking in account that “even identical twins do not require a living donor” [71]. Father Bert Cunningham anticipated its possibility with a thesis on the morality of organic transplantation. He considered the living donor a model of virtue for the reason that “there exist an ordination of men to one another and as a consequence, an order of their members to one another, thus we contend that men are ordinate to society as a part to the whole and, as such, are in some way ordinate to one another” [72]. Aquinas, too, had seen the sacrifice of one’s life for the good of another as an act of charity. Much more was the undertaking of a risk for a proportionate benefit to another [73].
Kidney transplantation became a routine operation, and we know that we can live well with one kidney; therefore, it does not raise particular ethical problems anymore. However, LD-ITx is a novelty in the field of transplant surgery. We believe that Daube gave a correct formulation of the ethical problem presented by LD-ITX. He suggested that more than consent is required. A medical judgment of relative risks to donor and recipient, a high degree of caution and concern for the donor, and the absence of alternatives “place on the transplanting surgeon a far greater responsibility” [74]. This is exactly what informed consent, or conscious consent, as we prefer to call it, means [75]. We must consider three actors involved in the setting: the doctor, the recipient, and the donor. The doctor has the technical knowledge, and then he can act in the way marked out by Daube. The recipient is at risk of dying if the donor does not give a segment of its gut. Therefore, the point of view of the recipient is completely in favor of transplant. Certainly, the long-term mortality among recipients is high, but the all or nothing perspectives compel us to do good for the patient. Therefore, the only perspective that can give rise to an ethical question is the particular condition of the donor. As the donor is a healthy person, the operation could represent a sort of mutilation. However, in the perspective given by Cunningham and considering the rule “do not harm” as a relativistic norm, where the imperative is beneficence, also for the others, we have the duty to consider living donor transplantation as an important tool in the field of surgery. All the existing data summarized in the chapter lean on the side of transplant. First of all, there are some problems, as the chapter pointed out, with deceased donors, taking into account that they are often subject to either cardiac arrest or resuscitation. Using living donors, we can obviate to these problems. Furthermore, LD-ITx can be performed and the recipient conditions are optimal and the donor bowel preparation can be easily performed, lessening the risk of infection complications. Not least, often a living donor is a relative of the recipient. This fact is not marginal, representing an unquestionable immunologic advantage. Furthermore, we have to consider that optimal deceased intestinal donors are not common, the waiting list is increasing, and the mortality for all candidates on the waiting list is reported to be up to 20 %. Besides, LD-ITx would improve the possibility to obtain transplant in developing countries, where TNP and deceased donors are not easily available. Considering that the principle of beneficence compels us to do what is best for the patient, LD-ITx represents the best treatment for patients. Finally, but not in order of importance, we must consider the risks to the donor, which include early surgical complications, such as small bowel obstruction, diarrhea, weight loss, and vascular thrombosis. These seem to be acceptable risks compared with the benefit to the recipient, which are going to be resolved in a short period of time. We must consider that with a careful and appropriate surgical technique , these risks can be still further reduced. Unfortunately, we do not have long-term follow-up of these patients. This fact could be a dilemma from an ethical point of view, but we have a lot of data from patients who opted for intestinal obstruction or abdominal infarction. Despite the fact that they had even wider resections, the long-term effects are acceptable. In light of these reasons, we believe that the LD-ITx represents a valid and ethical alternative to ITx from a deceased donor.
References
Intestinal TR, Toronto, ONT, Canada. Available at www.intestinaltransplant.org/itr Accessed March 2013.
Adam R, McMaster F, O’Grady JG, Castaing D, Klempnauer JL, Jamieson N, et al. European Liver Transplant Association. Evolution of liver transplantation in Europe: report of the European Liver Transplant Registry. Liver Transpl. 2003;9(l2):1231–43.
Dharnidharka VR, Sullivan EK, Stablein DM, Tejani AH, Harmon WE, et al. North American Pediatric Renal Transplant Cooperative Study (NAFRTCS). Risk factors for posttransplant lymphoproliferative disorder (PTLD) in pediatric kidney transplantation: a report of the North American Pediatric Renal Transplant Cooperative Study (NAPRTCS). Transplantation. 2001;71(8):1065–68.
Caillard S, Lachat V, Moulin B, et al. Posttransplant lymphoproliferative disorders in renal allograft recipients: report of 53 cases of a French multicenter study. PTLD French Working Group. Transplant Int. 2000;13 (suppl 1):S338–93.
Loinaz C, Kato T, Nishida S, Weppler D, Levi D, Dowdy L, et al. Bacterial infections after intestine and multivisceral transplantation. The experience of the University of Miami (1994–2001). Hepatogastroenterology. 2006;53(68):234–42.
Smith JM, Skeans MA, Thompson B, Horslen SP, Edwards EB, Harper AM, et al. OPTN/SRTR 2011 annual data report: intestine. Am J Transplant. 2013;13 Suppl 1:103–18.
Mazariegos GV, Steffick DE, Horslen S, Farmer D, Fryer J, Grant D, et al. Intestine transplantation in the United States, 1999–2008. Am J Transpl. 2010;10:1020–34.
Tzvetanov IG, Oberholzer J, Benedetti E, et al. Current status of living donor small bowel transplantation. Curr Opin Organ Transplant. 2010;15:346–8.
Benedetti E, Holterman M, Asolati M, Di Domenico S, Oberholzer J, Sankary H, et al. Living related segmental bowel transplantation. From experimental to standardized procedure. Ann Surg. 2006;244:694–9.
Testa C, Holterman M, John E, Kecskes S, Abcarian H, Benedetti E, et al. Combined living-donor liver/small bowel transplantation. Transplantation. 2005;79(10):1401–4.
Cicalese L, Sileri I, Green M, Abu-Elmagd K, Kocoshis S, Reyes J, et al. Bacterial translocation in clinical intestinal transplantation. Transplantation. 2001;71(11):1414–7.
Cicalese L, Sileri P. Asolati M, Rastellini C, Abcarian H, Benedetti E, et al. Low infectious complications in segmental living related small bowel transplantation in adults. Clin Transplant. 2000;14(6):567–71.
Berney T, Genton L, Buhler LH, Raguso CA, Charbonnet P, Pichard C, et al. Five-year follow-up after pediatric living-related small bowel transplantation between two monozygotic twins. Transplant Proc. 2004;36(2):316–8.
Grant D, Abu-Elmagd K, Reyes J, Tzakis A, Langnas A, Fishbein T, et al. 2003 report of the intestine transplant registry: a new era has dawned. Ann Surg. 2003;2005;241:607–13.
Cicalese L, Rastellini C, Sileri P, Abcarian H, Benedetti E, et al. Segnientii living-related small bowel transplantation in adults. J Gastrointest Surg. 2001;5(2):168–72.
Okada Y, Klein NJ, Van-Saene HK, Webb G, Holzel H, Pierro A, et al. Bactericidal activity against coagulasenegative staphylococci is impaired in infants receiving long-term parenteral nutrition. Ann Surg. 2000;231:276–31.
Okada Y, Papp E, Klein NJ, Pierro A, et al. Total parenteral nutrition directly impairs cytokine production after bacterial challenge. J Pediatr Surg. 1999;34:277–80.
Okada Y, Klein NJ, Pierro A, et al. Neutrophil dysfunction: the cellular mechanism of impaired immunity Turing total parenteral nutrition in infancy. J Pediatr Surg. 1999;34:242–5.
Ellozy SH, Harris MT, Bauer JJ, Gorfine SR, Kreel I, et al. Early postoperative small-bowel obstruction: a prospective evaluation in 242 Consecutive abdominal operations. Dis Colon Rectum. 2002;45(9):1214–7.
Fraser SA, Shrier I, Miller G, Gordon PH, et al. Immediate postlaparotomy small-bowel obstruction: a 16-year retrospective analysis. Am Surg. 2002;68(9):780–2.
Matter I, Khalemsky L, Abrahamson J, Nash E, Sabo E, Eldar S, et al. Does the index operation influence the course and outcome of adhesive intestinal obstruction? Eur J Surg. 1997;163(10):767–2.
Menzies D, Ellis H. Intestinal Obstruction from adhesions—how big is the problem? Ann R Coll Surg Engl. 1990;72(1):60–3.
Ellis H, Moran BJ, Thompson JN, Parker MC, Wilson MS, Menzies D et al. Adhesion-related hospital admission after abdominal and pelvic surgery: a retrospective cohort study. Lancet. 1999;353(9163):1476–80.
Fevang BT, Fevang J, Lie SA, Søreide O, Svanes K, Viste A, et al. Long-term prognosis after operation for adhesive small bowel obstruction. Ann Surg. 2004;240(2):193–201.
Miller G, Boman J, Shrier 1, Cordon PH. Natural history of patients with adhesive smalI bowel obstruction. Br J Surg. 2000;87(9):1240–7.
Benedetti B, Baum C, Cicalese I, Brown M, Raofi V, Massad MG, et al. Progressive functional adaptation of segmental bowel graft from living related donor. Transplantation. 2001;71(4):569–71.
Jao W, Sileri P, Holaysan J, Morini S, Chejfec G, Rastellini C, et al. Morphologic adaptation following segmental living related intestinal transplantation. Transplant Proc. 2002;34(3):924.
Fishbein TM, Matsumoto CS. Intestinal replacement therapy: timing and indications for referral of patients to an intestinal rehabilitation and transplant program. Gastroenterology. 2006;130 (2 suppl 1):S147–51.
DiBaise JK, Young RJ, Vanderhoof JA, et al. Intestinal rehabilitation and the short bowel syndrome part 1. Am J Gastroenterol. 2004;99(7):1386–1395; part 2, Am J Gastroenterol. 2004;99(9):1823–32.
Guglielmi FW, Regano N, Mazzuoli S, Fregnan S, Leogrande G, Guglielmi A, et al. Cholestasis induced by total parenteral nutrition. Clin Liver Dis. 2008;12:97–110.
Scolapio JS, Fleming CR, Kelly G, Wick DM, Zinsmeister AR, et al. Survival of home parenteral nutrition-treated patients: 20 years of experience at the Mayo Clinic. Mayo Clin Proc. 1999;74:217–22.
Michels N, Siddhart P, Kornblith L, Horslen SP, Edwards EB, Harper AM, et al. The variant blood supply to the small and large intestines: its import in regional resections. J Int Coll Surg. 1963;39:127.
Dowling RI-I, Booth C. Structural and functional changes following small bowel resection in the rat. Clin Sci. 1967;32:139–49.
Thompson JS, Ferguson DC. Effect of the distal remnant on ileal adaptation. J Gastrointest Surg. 2000;4:430–4.
Tesi R, Beckj R, Lamblase I, Haque S, Flint L, Jaffe B, et al. Living-related small bowel transplantation: donor evaluation and outcome. Transplant Proc. 1997;29:686–7.
Kimura K, Money S, Jaffe IT, et al. The effect of size and site of origin of intestinal grafts on small-bowel transplantation in the rat. Surgery. 1987;101:618–22.
Bryant J. Observations upon the growth and length of the human intestine. Am J Med Sci. 1924;167:499.
Blankehorn DH, Hirsch J, Ahrens EH, et al. Transintestinal intubation: technique to measure the gut length and physiologic sampling of known loci. Proc Soc Exp Biol Med. 1995;88:356.
Reis VderV, Schembra IW. Lange and Lage des Verdauungsrohres beim Lebenden. Z Ges Exp Med. 1924;43:94.
Reinelt II, Schirmer U, Marx T, Topalidis P, Schmidt M, et al. Diffusion of xenon and nitrous oxide into the bowel. Anesthesiology. 2001;94:475–7; discussion 6A.
Akca O, Lenhardt R, Fleischmann E, Treschan T, Greif R, Fleischhackl R, et al. Nitrous oxide increases the incidence of bowel distension in patients undergoing elective colon resection. Acta Anaesthesiol Scand. 2004;48:894–8.
Ogilvy Al SG. The gastrointestinal tract after anaesthesia. Eur J Anaesthesiol Suppl. 1995;111:35–42. Review.
Torjman MC, Joseph JI, Munsick C, Morishita M, Grunwald Z, et al. Effects of isoflurane on gastrointestinal motility after brief exposure in rats. Int J Pharm. 2005;294(1–2):65–71.
Deltz B, Schroeder F, Gehbardt H, et al. Successful clinical bowel transplantation. Clin Transplant. 1989;3:89.
Morris JA, Johnson DL, Rimmer JA, Kuo PC, Alfrey EJ, Bastidas JA, et al. Identical-twin small-bowel transplant or desmoid tumor. Lancet. 1995;345:1577–8.
Pollard SG, Lodge P, Selvakumar S, Heatley RV, Wyatt J, Wood R, et al. Living-related small bowel transplantation: the first United Kingdom case. Transplant Proc. 1996;28:2733.
Gruessner R, Sharp H. Living-related intestinal transplantation: first report of a standardized surgical technique. Transplantation. 1997;64:1605–7.
Tzoracoleftherakis E, Cohen M, Sileri P, Cicalese L, Benedetti E, et al. Small bowel transplantation and staged abdominal wall reconstruction after shotgun injury. J Trauma. 2002;53:770.
Asham F, Uknis M, Rastellini C, Elias G, Cicalese L, et al. Acellular dermal matrix provides a good option for abdominal wall closure following small bowel transplantation: a case report. Transplant Proc. 2006;38(6):1770–1.
Fortner JG, Sichuk G, Litwin SD, Beattie EJ Jr, et al. Immunological responses to an intestinal allograft with HL-A-identical donor-recipient. Transplantation. 1972;14:531–5.
Fishbein TM. Intestinal transplantation. N Engl J Med. 2009;361:998–1008.
Cicalese L, Sileri P, Gonzales O, Asolati M, Rastellini C, Abcarian H, et al. Cost-effectiveness of early living related segmental bowel transplantation as therapy for trauma-induced irreversible intestinal failure. Transplant Proc. 2001;33:3581–2.
Barr MI, Beighiti J, Villamii PC, Pomfret EA, Sutherland DS, Gruessner RW, et al. A report of the Vancouver forum on the care of the live organ donor: lung, liver, pancreas and intestine: data and medical guidelines. Transplantation. 2006;81:1373–85.
Abu-Elmagd K, Reyes J, Bond G, Mazariegos G, Wu T, Murase N, et al. Clinical intestinal transplantation: a decade of experience at a single center. Ann Surg. 2001;234:404–16.
Gangemi A, Tzvetanov IG, Beatty E, et al. Lessons learned in pediatric small bowel and liver transplantation from living-related donors. Transplantation. 2009;87:1027–30.
Pirenne J, Kawai M. Intestinal transplantation: evolution in immunosuppression protocols. Curr Opin Organ Transplant. 2009;14:250–55.
Quintini C, Kato T, Gaynor JJ, Ueno T, Selvaggi G, Gordon P, et al. Analysis of risk factors for the development of posttransplant lymphoprolipherative disorder among 119 children who received primary intestinal transplants at a single center. Transplant Proc. 2006;38:1755–8.
Calne R, Friend P. Middleton S, Jamieson NV, Watson CJ, Soin A, et al. Intestinal transplant between two of identical triplets. Lancet. 1997;350:1077–8.
Jaffe BM, Beck R, Flint L, Gutnisky G, Haque S, Lambiase L, et al. Living-related small bowel transplantation in adults: a report of two patients. Transplant Proc. 1997;29:1851–2.
Misra MV, Bhattacharya K, Nompleggi DJ, Uknis ME, Rastellini C, Cicalese L, et al. Magnification endoscopy as a reliable tool for the early diagnosis of rejection in living-related small bowel transplants: a case report. Transplant Proc. 2006;38:1738–9.
Howard L, Malone M. Current status of home parenteral nutrition in the United States. Transplant Proc. 1996;28:2691–5.
Abu-Elmagd KM, Reyes J, Fung JJ, Mazariegos G, Bueno J, Janov C et al Evolution of clinical intestinal transplantation: improved outcome and cost effectiveness. Transplant Proc. 1999;31:582 584.
O’Keefe SJ, Buchman AL, Fishbein TM, Jeejeebhoy KN, Jeppesen PB, Shaffer J, et al. Short bowel syndrome and intestinal failure: consensus definitions and overview. Clin Gastroenterol Hepatol. 2006;4:6–10.
Todo S, Reyes J, Furukawa H, Abu-Elmagd K, Lee RG, Tzakis A, et al. Outcome analysis of 71 clinical intestinal transplantations. Ann Surg. 1995;222:270–80.
Rovera GM, Sileri P, Rastellini C, Knight P, Benedetti E, Cicalese L, et al. Quality of life after living-related small bowel transplantation. Transplant Proc. 2002;34:967–8.
DiMartini A, Rovera GM, Graham TO, Furukawa H, Todo S, Funovits M, et al. Quality of life after small intestinal transplantation and among home parenteral nutrition patients. JPEN J Parenter Enteral Nutr. 1998;22:357–62.
Abu-Elmagd KM. Intestinal transplantation for short bowel syndrome and gastrointestinal failUIV current consensus, rewarding outcomes, and practical guidelines. Gastroenterology. 2006;130(2 suppl 1):S132–7.
Rovera GM, DiMartini A, Graham TO, Hutson WR, Furukawa H, Todo S, et al. Quality of life after intestinal transplantation and on toi, il parenteral nutrition. Transplant Proc. 1998;30:2513–4.
DiMartini A, Rovera GM, Graham TO, Furukawa H, Todo S, Funovits M, et al. Quality of life after small intestinal transplantation and among home parenteral nutrition patients. JPEN J Parenter Enteral Nutr. 1998;22:357–62.
Rovera GM, DiMartini A, Schoen RE, Rakela J, Abu-Elmagd K, Graham TO, et al. Quality of life of patienI after intestinal transplantation. Transplantation. 1998;66:1141–5.
Murray JE. Organ transplantation: the practical possibilities. In: Wostenholme GEW, O’Connors M, Editors. Law, ethics of transplantation. London:JA Churchill, Ltd; 1966.
Cunningham B. The morality of organic transplantation. Studies Sacred Theol. 1944;86:63.
Thomas Aquinas. III Sententiae, d. 29, a. 5, “when one gives one’s life for one’s friend, he does not love the friend more than himself, but rather prefers one’s own “good of virtue” to a physical good.”
Daube D. Transplantation: acceptability of procedures and the required legal sanctions. In: Wolsenholme GEW, O’Connors M, Editors. Ethics in Medical Progress. Boston: Little, Brown & Company; 1966.193.
Caocci G, La Nasa G, d’Aloja, Vacca A, Piras E, Pintor M, Demontis R, Pisu S, et al. Ethical issues of unrelated hematopoietic stem cell transplantation in adult thalassemia patients. BMC Medical Ethics. 2011;12: 4.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Tuveri, M., Pisu, S., Cicalese, L. (2014). Intestinal Transplantation from Living Donors. In: STEEL, J. (eds) Living Donor Advocacy. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-9143-9_4
Download citation
DOI: https://doi.org/10.1007/978-1-4614-9143-9_4
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-9142-2
Online ISBN: 978-1-4614-9143-9
eBook Packages: MedicineMedicine (R0)