
Abstract
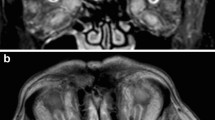
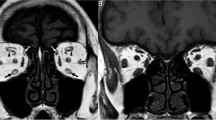
JC is a 32-year-old woman who noted increasing prominence of her right eye over several months. She presented to her primary care doctor, who ordered thyroid tests (TSH and T4) that were normal. He then ordered a CT scan that was interpreted as normal by the radiologist with no mass lesions detected and extraocular muscle thickness “within normal limits.” She was referred to an ophthalmologist who documented possible lid lag on the right side and exophthalmometry readings of 19 mm OD and 16 mm OS. She was referred for echography. A-scan revealed several muscles in both orbits that were greater than upper limits of normal for muscle thickness. The internal reflectivity pattern of these muscles was heterogeneous and consistent with Graves’ disease (Fig. 1). Thyroid antibody testing was performed and was moderately positive. She was instructed about her disease and how to manage any symptoms that may occur, such as puffy lids and dry, scratchy eyes. She was scheduled for a follow-up examination in 6 months and warned about symptoms of optic nerve compression and was specifically told to check her color sensitivity to a red object at home.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
JC is a 32-year-old woman who noted increasing prominence of her right eye over several months. She presented to her primary care doctor, who ordered thyroid tests (TSH and T4) that were normal. He then ordered a CT scan that was interpreted as normal by the radiologist with no mass lesions detected and extraocular muscle thickness “within normal limits.” She was referred to an ophthalmologist who documented possible lid lag on the right side and exophthalmometry readings of 19 mm OD and 16 mm OS. She was referred for echography. A-scan revealed several muscles in both orbits that were greater than upper limits of normal for muscle thickness. The internal reflectivity pattern of these muscles was heterogeneous and consistent with Graves’ disease (Fig. 1). Thyroid antibody testing was performed and was moderately positive. She was instructed about her disease and how to manage any symptoms that may occur, such as puffy lids and dry, scratchy eyes. She was scheduled for a follow-up examination in 6 months and warned about symptoms of optic nerve compression and was specifically told to check her color sensitivity to a red object at home.

A-scan of extraocular muscle involved by Graves’ disease (vertical arrows)
The extraocular muscles may also be thickened in cases of orbital myositis, but the A-scan is quite helpful in viewing the internal structure, which can clarify the differential diagnosis of the enlarged muscle. This capability of internal analysis is especially valuable in cases where the muscle is not abnormally enlarged.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Harrie, R.P., Kendall, C.J. (2014). Case Study 15 Extraocular Muscles in Graves’ Disease. In: Clinical Ophthalmic Echography. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-7082-3_15
Download citation
DOI: https://doi.org/10.1007/978-1-4614-7082-3_15
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-7081-6
Online ISBN: 978-1-4614-7082-3
eBook Packages: MedicineMedicine (R0)