
Abstract
The lungs are a frequent site of infectious diseases. Pleuropulmonary infections include bronchitis and bronchiolitis, pneumonia, lung abscess, cavity formation, allergic bronchopulmonary reaction, as well as pleural effusion and empyema. An accurate diagnosis of infection by means of cytology can be lifesaving. Sputum, lung FNA, bronchoscopic brushing, washing, and BAL are useful procedures that can help provide a fast, cost-effective, and noninvasive diagnosis of pulmonary infection. This chapter covers a wide variety of viral, bacterial, fungal, and parasitic infections that involve the lower respiratory system.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Respiratory Syncytial Virus
- Diffuse Alveolar Damage
- Ancillary Study
- Fungal Organism
- Allergic Bronchopulmonary Aspergillosis
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
The lungs are a frequent site of infectious diseases. An accurate diagnosis of infection by means of cytology can be lifesaving. Sputum, lung FNA, bronchoscopic brushing, washing, and BAL are useful procedures that can help provide a fast, cost-effective, and noninvasive diagnosis of pulmonary infection. Pleuropulmonary infections include bronchitis and bronchiolitis, pneumonia (inflammation of the lung parenchyma), lung abscess, cavity formation, allergic bronchopulmonary reaction, as well as pleural effusion and empyema (pus in the pleural cavity).
A variety of microorganisms can infect the lungs including viruses, bacteria, fungi, and parasites. The implicated pathogen depends in part on the clinical setting. For example, microorganisms responsible for community-acquired pneumonia include Streptococcus pneumoniae, Haemophilus influenzae, and Staphylococcus aureus. Atypical community-acquired pneumonia is caused by Mycoplasma pneumoniae, Chlamydia spp. and several viruses including respiratory syncytial virus (RSV) and parainfluenza virus in children and influenza A and B in adults. Nosocomial infections may be caused by Klebsiella spp., Escherichia coli, Pseudomonas spp., and penicillin resistant S. aureus. Finally, there are certain pathogens responsible for infections in the immunocompromised host like cytomegalovirus (CMV), Pneumocystis jirovecii, and Mycobacterium avium-intracellulare (MAI). This chapter discusses the cytologic features of a variety of pathogens that infect the respiratory tract.
The optimal diagnostic method depends on the location of the lesion and radiologic findings. Sputum samples, and bronchial brushings and washings yield diagnostic material for centrally located lesions that involve major airways, while a BAL is useful for assessing inflammatory and infectious processes in the peripheral regions of the lung. Transbronchial or ultrasound guided FNA permits endobronchial lesions or hilar lymph nodes to be sampled, and radiologically guided FNA is used when subpleural regions need to be aspirated that cannot be assessed by bronchoscopy. Given that cytologic examination of the respiratory tract is less invasive compared to open surgical biopsies, cytology is often the initial and only means by which patients are evaluated for infectious diseases. This is especially true in immunocompromised patients who need to be followed over a given period of time to rule out opportunistic infections. In fact, BAL remains the diagnostic procedure of choice for detecting opportunistic infections in immunocompromised hosts.
Viral Infections
Viruses are one of the most common causes of infection of the respiratory tract. Not all viral infections have cytopathic changes (e.g., influenza, swine flu, severe acute respiratory syndrome/SARS, EBV). However, in many cases the cytologic features of viral infection are fairly specific as to the etiology (Table 6.1). Ancillary studies such as immunohistochemistry, viral culture, and molecular tests are often necessary to accurately identify the cause of certain infections.
Herpes Simplex Virus (HSV)

BAL specimen from a patient with a history of colon adenocarcinoma who presented with respiratory distress. The left photos show characteristic of Cowdry type B herpes inclusions. The right photo shows accompanying reactive reparative change with prominent and multiple nucleoli that mimics malignancy in this case (Pap stain, high magnification).
Microbiology
-
Herpesvirus types 1 and 2 (HSV 1 and 2) can both infect the lungs.
Clinical Features
-
HSV infection of the upper respiratory tract can lead to pharyngitis, laryngotracheitis, and pneumonia. HSV infection of the lung may cause a necrotizing pneumonia or diffuse interstitial pneumonia.
-
HSV commonly infects neonates and immunocompromised patients.
Cytomorphologic Features
-
Herpetic inclusions can be found within metaplastic squamous cells when the inflammation is centered around airways or in multinucleated giant cells within necroinflammatory debris in the interstitial form of disease.
-
Infected cells often display prominent nuclear molding.
-
Two forms of characteristic herpes inclusions may be seen, including Cowdry type A inclusions (distinct eosinophilic intranuclear inclusions surrounded by a clear halo due to margination of chromatin material) and Cowdry type B inclusions (eosinophilic ground glass “smudge nuclei” with margination of the chromatin material) (Fig. 6.1).
-
The background may have associated acute inflammatory cells and necrosis.
Differential Diagnosis
-
Nonspecific reactive bronchial cells and alveolar macrophages (multinucleated bronchial cells and cells with clearing/washed out nuclei).
-
Squamous dysplasia in metaplastic cells or in a squamous papilloma lesion.
-
The cytopathic features are identical to those of herpes zoster (clinical history and/or ancillary studies are required to resolve this differential diagnosis).
-
CMV infection (rarely causes multinucleation, see Fig. 6.2 (see next page)).
Fig. 6.4. 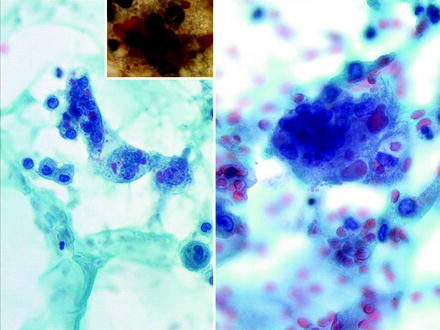
Measles pneumonia in a 42-year-old woman showing giant cell pneumonia with enormous multinucleated giant cells that have cytoplasmic and intranuclear inclusions (Pap stain, high magnification). The inset shows a cell stained with Phloxine Tartrazine that highlights the bright red cytoplasmic inclusions (images courtesy of Dr. Pawel Schubert, South Africa).

Ancillary Studies
-
Most cases do not need ancillary studies to confirm the diagnosis.
-
Immunostains are available for HSV infection and can be performed on cell block material or smears.
-
Viral culture.
-
HSV DNA detection by in situ hybridization or PCR.
-
Serology (type-specific assays).
-
Electron microscopy.
Cytomegalovirus (CMV)

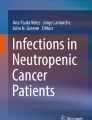
Co-infection with CMV and P. jirovecii is shown in this BAL specimen from an immunocompromised patient. Characteristic “owl eye” inclusions are seen. Multinucleation is rare in CMV infection, but can occur (see inset). Pneumocystis infection resulted in the cast of frothy material; each circlet with a central dot is an organism (Pap stain, intermediate magnification left and high magnification right).
Microbiology
-
CMV is one of the most common causes of opportunistic infections involving the respiratory tract. In the respiratory tract, CMV mainly targets pulmonary macrophages, endothelial cells and fibroblasts, but virtually any cell can be infected by this virus.
Clinical Features
-
CMV pneumonia is frequently seen in patients with HIV/AIDS, those receiving organ transplants, or individuals at the extremes of age.
Cytomorphologic Features
-
The diagnostic features of CMV infection include cytomegaly, large amphophilic intranuclear inclusions with perinuclear halos and chromatin margination (“owl eye” inclusion), and small basophilic cytoplasmic inclusions.
-
The number of cells showing cytopathic changes varies with the severity of infection or as a result of patients receiving prophylactic antiviral therapy.
-
As CMV is frequently found in immunosuppressed patients, it may be seen together with other opportunistic pathogens such as fungi including P. jirovecii (Fig. 6.2).
Differential Diagnosis
-
Herpes simplex infection.
-
Neoplastic cells.
-
Reactive epithelial cells or macrophages with karyomegaly.
-
Other viral infections including adenovirus and RSV infection.
Ancillary Studies
-
Most cases do not need ancillary studies to confirm the diagnosis.
-
Immunocytochemistry or in situ hybridization for CMV.
-
Molecular testing (PCR).
-
Viral culture.
Adenovirus

Adenovirus pneumonia. The images on the left are of a smear prepared from sputum showing an infected cell (circled) with a degenerated nucleus (top left, Pap stain, intermediate magnification) and a detached ciliary tuft (bottom left, Pap stain, high magnification). The images on the right are of a BAL from a child with adenovirus pneumonia showing a smudgy appearing nucleus of an infected cell (top right, Pap stain, cytospin, high magnification) with positive immunocytochemistry confirming this is due to adenovirus infection (bottom right, high magnification) (BAL images courtesy of Dr. S. Ranganathan, Pittsburgh Children’s Hospital, USA).
Microbiology
-
Adenovirus is a DNA virus that can cause ulcerative bronchiolitis, acute pneumonia, or diffuse alveolar damage (DAD).
Clinical Features
-
Pulmonary adenovirus infections may occur in healthy subjects living in close quarters (e.g., military recruits), but can also cause severe and potentially fatal infections in immunocompromised patients.
Cytomorphologic Features
-
Infected cells exhibit two types of nuclear inclusions: amphophilic intranuclear inclusions with perinuclear clearing that mimic herpes simplex infection, or “smudge cells” where large basophilic inclusions fill the entire nucleus and obscure the chromatin detail (Fig. 6.3).
-
Another finding is the presence of decapitated ciliated respiratory epithelial cells, so-called ciliocytophthoria.
-
There may be an associated neutrophilic pneumonia, marked hemorrhage, or evidence of necrosis.
Differential Diagnosis
-
Other viral infections such as herpes infection.
-
Reactive epithelial cells.
-
Cytotoxic drug injury.
Ancillary Studies
-
Immunocytochemistry for adenovirus.
-
Monoclonal antibody-based enzyme immunoassay can be performed on a fresh specimen.
-
Immunofluorescence assay.
-
Microbiology tissue culture.
-
PCR.
-
Electron microscopy.
Respiratory Syncytial Virus (RSV)
Microbiology
-
RSV is an RNA virus (a member of the paramyxovidae subfamily Pneumovirinae) that targets the respiratory lining epithelium.
-
Infection produces syncytial giant cells with inconspicuous eosinophilic cytoplasmic inclusions.
Clinical Features
-
RSV is a major cause of lower respiratory tract infection (bronchiolitis and pneumonia) during infancy and childhood.
-
RSV causes benign respiratory infections in older children and has been linked to more severe adult community-acquired pneumonia, acute bronchiolitis, and diffuse alveolar disease (DAD) in the immunocompromised host or in lung allograft recipients.
Cytomorphologic Features
-
Syncytial giant cells with cytoplasmic inclusions surrounded by clear halos.
Differential Diagnosis
-
Other viral infections such as human metapneumonia virus and measles.
-
Benign noninfectious entities with giant cells.
Ancillary Studies
-
Binax NOW® RSV (BN) used on cytology specimens.
-
Microbiology tissue culture.
-
Shell vial culture.
-
PCR.
Parainfluenza
Microbiology
-
Human parainfluenza viruses are RNA viruses belonging to the paramyxovidae family that cause upper respiratory tract infections.
Clinical Features
-
In children, upper respiratory tract infections (e.g., croup) usually follow a benign course.
-
Severe disease may occur in immunocompromised patients.
Cytomorphologic Features
-
As with RSV, this infection is associated with syncytial giant cells and epithelial cells with intracytoplasmic inclusions. However, these inclusions tend to be more frequent and larger than those seen with RSV.
-
Ciliocytophthoria may be prominent.
Differential Diagnosis
-
Other viral infections such as RSV.
-
Benign noninfectious entities with giant cells (e.g., hard metal pneumoconiosis).
Ancillary Studies
-
Immunocytochemistry for parainfluenza virus.
-
Rapid real-time multiplex PCR assay.
-
Multiplex nucleic acid sequence-based amplification (NASBA) assay.
-
Viral culture.
Measles
Microbiology
-
Measles (also known as rubeola) is an infection of the respiratory system caused by the RNA rubeola virus of the genus Morbillivirus.
-
Measles pneumonia is a rare and serious complication of the viral exanthem, especially in immunocompromised patients.
Clinical Features
-
Measles pneumonia can range from mild (bronchiolitis) to severe (DAD) disease.
Cytomorphologic Features
-
Cytology specimens show large multinucleated giant cells with cytoplasmic and intranuclear inclusions. The intranuclear inclusion has a glassy, eosinophilic appearance reminiscent of Cowdry types A inclusions (Fig. 6.4).
-
There may be associated acute inflammation.
Differential Diagnosis
-
Other viral infections such as RSV.
-
Benign noninfectious entities with giant cells morphology (e.g., hard metal pneumoconiosis).
Ancillary Studies
-
Phloxine tartrazine special stain, which stains viral inclusions bright red.
-
Serology: IgM (acute infection); IgG (immunity).
-
PCR (from a swab).
-
Viral culture.
Bacterial Infections
Bacterial pneumonia may be lobar, lobular, or present in an atypical manner (e.g., mass-like or interstitial appearance). Gram-positive and negative-bacteria are a common cause of pulmonary infection. Most bacteria cause a nonspecific acute necroinflammatory reaction associated with a variable fibrohistiocytic response (organization). Necrotizing pyogenic infections may result in abscess formation. Mycobacteria may evoke a granulomatous process. The etiology of infectious pneumonia is best established by correlating clinical and radiologic findings with microbiology studies.
Actinomyces
Microbiology
-
Actinomyces are Gram-positive filamentous bacteria that cause suppurative and granulomatous inflammation. Infections may also result in bronchiectasis and abscesses containing sulfur granules.
-
Pulmonary infections occur via aspiration of oral organisms and are seen most often in persons with poor oral hygiene, immunocompromised patients, or from direct extension of cervicofacial or subdiaphragmatic infection.
-
Secondary actinomycotic infection can involve devitalized lung tissue damaged by other infections.
Clinical Features
-
The clinical manifestations of pulmonary actinomycosis are fever, productive cough, and hemoptysis. Chronic infection may cause sinus tracts.
-
Lung imaging findings may include consolidation, necrosis, abscess, or an aspirated broncholith.
Cytomorphologic Features
-
Specimens contain acute inflammation and bacterial colonies composed of thin beaded and delicate branching filaments that are cyanophilic with a Pap stain (so-called “cotton ball” appearance).
-
Some cases may have sulfur granules which are colonies of tangled Gram-positive bacilli, often coated with an eosinophilic matrix of exudate plasma proteins (Splendore-Hoeppli reaction).
Differential Diagnosis
-
Actinomyces are commonly found in tonsillar crypts, and therefore may be seen (associated with squamous cells) contaminating sputum and bronchial specimens. Their presence on FNA is unlikely to be due to contamination. True infection is associated with abundant neutrophils.
-
Nocardia (less beading, no sulfur granules).
-
Botryomycosis (may also form sulfur granules, but contains cocci).
-
Mycobacteria.
-
Fungal infection.
Ancillary Studies
-
Special stains (Actinomyces are positive with Gram and GMS stains, but negative with an AFB/Fite stain).
-
Microbiology culture.
Nocardia

FNA of Nocardia pneumonia with numerous PMNs and necrotic material (left image Pap stain, high magnification) associated with thin filamentous branching bacteria (middle image Gram stain and right image AFB stain, both high magnification).
Microbiology
-
Nocardia are weakly staining Gram-positive, partially acid-fast, rod-shaped, aerobic bacteria. They form beaded branching filaments. The majority of infections (80%) are due to Nocardia asteroides.
-
Pulmonary infection occurs via inhalation. Pre-existing pulmonary disease, particularly pulmonary alveolar protienosis, increases the risk of contracting Nocardia pneumonia.
Clinical Features
-
Patients commonly present with slowly progressive pneumonia. In immuncompromised patients, infection may be associated with cavitary lung nodules. Infection can also spread to the pleura or to chest wall.
Cytomorphologic Features
-
Cytology findings include those of acute pneumonia (numerous neutrophils and necrotic material) together with the presence of thin filamentous, beaded bacteria with right angle branching that resembles Chinese letters (Fig. 6.5).
Differential Diagnosis
-
Actinomyces (more beading and more commonly have sulfur granules).
-
Mycobacteria.
Ancillary Studies
-
Special stains (Nocardia are positive with Gram and GMS stains, and weakly positive with an AFB/Fite stain).
-
Microbiology culture.
Tuberculosis

Necrotizing granulomatous pneumonia caused by M. tuberculosis shown on Pap stained smears at high magnification (left and middle images) and cell block (H&E stain, high magnification). Rare mycobacteria are seen with an AFB stain (upper right image and inset, high magnification).

Tuberculosis pneumonia with numerous mycobacteria seen as negative images on Diff-Quik stain (high magnification).
Microbiology
-
Pulmonary tuberculosis (TB) is caused by the bacterium Mycobacterium tuberculosis. Pulmonary TB may be due to primary or reactivation (chronic) infection. Pulmonary manifestations of TB include bronchopneumonia, caseating pneumonia, nodular disease (tuberculoma), tracheobronchitis, milliary disease, hilar lymphadenopathy, and pleural disease.
-
Individuals at risk for infection are those who are immunosuppressed, the elderly, and infants.
-
Nontuberculous mycobacteria (NTM), such as Mycobacterium avium complex (MAC) and Mycobacterium kansasii, may also cause pulmonary infections.
-
Infections are often associated with granulomatous inflammation. In NTM infection, particularly in immunocompromised patients, granulomas tend to be nonnecrotizing and incompletely formed.
Clinical Features
-
Patients usually present with night sweats, fever, weight loss, fatigue, chronic cough, chest pain, hemoptysis, and possibly extrapulmonary TB that may involve the pleura and mediastinal lymph nodes.
-
Thoracic imaging studies may show infiltrates or cavities (especially of the upper lobes), solitary or milliary nodules, pleural effusion, pneumothorax, and/or hilar lymphadenopathy.
Cytomorphologic Features
-
The main finding is granulomas that show clusters of epithelioid histiocytes that may be mixed with lymphocytes, Langhans, and/or foreign body-type multinucleated giant cells with/without a necrotic background (Fig. 6.6).
-
In NTM infections, macrophages laden with abundant mycobacteria may show abundant foamy cytoplasm (referred to as pseudo-Gaucher cells).
-
A negative image of extracellular mycobacteria may be notable with Diff-Quik, Giemsa, or other Romanowsky-type stains (Fig. 6.7). In NTM infection, these unstained mycobacteria (especially within macrophages) are usually more numerous.
Differential Diagnosis
-
Other microorganisms that cause necrotizing granulomatous inflammation and are AFB positive (Nocardia, Rhodococcus, and Legionella micdadei).
-
Noninfectious causes of granulomatous lung disease (e.g., sarcoidosis).
Ancillary Studies
-
Acid-fast stains (Ziehl-Neelsen or Kinyoun stains). The diagnosis of mycobacterial infection can be on the basis of the identification of microorganisms with acid-fast (AFB) stains. Mycobacteria with M. tuberculosis compared to NTM may be rare and require careful and lengthy scrutiny of slides. Some mycobacteria have a distinct morphology; for example M. kansasii resembles a shepherd’s crook or candy cane and Mycobacterium fortuitum closely resembles Nocardia spp.
-
Mycobacteria may be weakly Gram-positive and will stain with GMS.
-
Fluorescence microscopy with fluorochrome dyes such as auramine O or auramine–rhodamine are more sensitive and specific than AFB stains.
-
Autofluorescence.
-
PCR for diagnosis and subclassification (can be done on cell block material).
-
Culture for diagnosis and subclassification, although mycobacteria are slow growing and culture can take weeks (6–8 weeks with conventional Lowenstein-Jensen medium and 3 weeks with Middlebrook liquid and solid media).
Legionella
-
Pneumonia is the predominant manifestation of Legionella infection (Legionnaire’s disease).
-
Bacteria (Gram-negative coccobacilli) can be identified with silver stains (Steiner, Warthin-Starry, or Diertrle stains), and are often abundant prior to therapy. Legionella micdadei stains with modified Ziehl-Neelsen stains.
-
Immunocytochemistry (for Legionella pneumophilia) can be performed if needed.
Fungal Infections
Pulmonary fungal infections can be readily diagnosed by means of exfoliative cytology or FNA. Infections are often associated with a granulomatous or necroinflammatory reaction. Fungal morphology varies with the stage of the disease and fungal organism. Table 6.2 summarizes the cytologic features of common fungal pathogens that infect the respiratory tract.
Candidiasis

Candidiasis in a BAL specimen with pseudohyphae (elongated yeast joined together) and budding yeast (left Pap stain and right GMS stain, high magnification).
Microbiology
-
Candidiasis, infection caused by Candida spp., can involve the lungs. Candida albicans is the primary causative agent. They are yeast-like fungi that can form true hyphae and pseudohyphae.
-
Most cases of candida pneumonia are secondary to hematological dissemination of organisms from a distant mucocutaneous site.
-
The respiratory tract is often colonized with Candida spp., especially in hospitalized patients. Patients at particular risk of acquiring a candida lung infection include those with impaired immunity (e.g., transplant recipients, HIV positive individuals, those using corticosteroids, burn victims, and patients with a hematologic neoplasm).
Clinical Features
-
Infection of the airways (laryngeal candidiasis and tracheobronchitis) may present with a sore throat, hoarseness, fever, productive cough, and possibly dyspnea. Candida pneumonia is usually associated with disseminated candidiasis. The most common form of infection is multiple lung abscesses.
Cytomorphologic Features
-
Specimens containing candida elements may contain pseudohyphae (elongated yeast joined together), true hyphae, and/or budding yeast (blastoconidia) with/without background inflammatory cells (Fig. 6.8).
Differential Diagnosis
-
Contamination from oropharyngeal sites (e.g., oral thrush)
-
Other fungal organisms (e.g., Aspergillus, cryptococcus)
-
Fungal mimics (e.g., synthetic fibers, pollen grains, etc.)
Ancillary Studies
-
Fungal stains (GMS and PAS are positive)
-
Gram stain: Positive
-
Fungal culture
Histoplasmosis

Histoplasmosis. (Left images) Macrophages are shown in this ThinPrep specimen of a bronchoalveolar lavage specimen from an AIDS patient with multiple intracellular yeast (Pap stain, top image intermediate and bottom image high magnification). (Right images). Macrophages containing H. capsulatum microorganisms are shown at high magnification in these direct smears from lung specimens (Diff-Quik stain).
Microbiology
-
Histoplasmosis, caused by the dimorphic fungus Histoplasma capsulatum, infection is acquired through inhalation of infective spores (microconidia), which primarily target macrophages in the respiratory system.
-
Pulmonary infection may be acute or chronic and present with localized or diffuse pulmonary disease.
Clinical Features
-
Pulmonary histoplasmosis can present clinically with pneumonia, lung nodule, cavitary lung disease, mediastinal or hilar lymphadenopathy, and even superior vena cava syndrome or obstruction of other mediastinal structures.
-
It is not uncommon for localized infections to mimic cancer.
Cytomorphologic Features
-
There are numerous intracellular yeasts measuring 3–5 μm, with narrow based budding, within macrophages. When cells are disrupted they may also be extracellularly located (Fig. 6.9).
Differential Diagnosis
-
Candida
-
Cryptococcus neoformans (microform)
-
Blastomyces dermatitidis
-
P. jiroveci
-
Microcalcifications (especially in the cell block)
-
Platelets (extracellular only)
Ancillary Studies
-
Special stains (GMS and PAS stains are positive)
-
Fungal culture
-
Antigen detection (enzyme immunoassay using urine, blood, or bronchoalveolar lavage fluid).
-
Serology
Blastomycosis
Microbiology
-
This is a systemic infection caused by inhaling the conidia of the dimorphic fungus B. dermatitidis.
-
Infections primarily involve the lung, usually associated with the formation of microabscesses, but may disseminate to cause extrapulmonary disease.
Clinical Features
-
Blastomycosis of the lung can be asymptomatic or manifest as acute or chronic pneumonia. In the lungs, this organism usually infects the upper lobes.
Cytomorphologic Features
-
One finds round large yeast (5–15 μm) that have a characteristic double contoured thick cell wall, and show broad-base budding.
-
There is often associated granulomatous inflammation present.
Differential Diagnosis
-
Other fungal organisms (e.g., the microform of H. capsulatum and giant form of Coccidioides immitis).
Ancillary Studies
-
Fungal stains (GMS and PAS are positive)
-
Mucicarmine stain (negative, to exclude cryptococcus)
-
Immunocytochemistry
-
Fungal culture
Cryptococcosis

Cryptococcus pneumonia. Yeasts are round to oval and have narrow-based buds (Pap stain left image, high magnification). Yeasts may resemble pneumocystis cysts, but tend to be more variable and often larger in size (left inset, DQ stain, high magnification). Encapsulated cryptococcal organisms are surrounded by a thick capsule that stains with GMS (top right), PAS (middle right), and mucicarmine (bottom right) stains (high magnification).

In cryptococcus pneumonia, organisms may be intracellular. The halo around the organism indicates the presence of a thick capsule (Pap stain, high magnification).
Microbiology
-
Humans are infected with cryptococcus by inhaling basidiospores or yeast. The important human pathogens are Cryptococcus neoformans and Cryptococcus gattii.
-
The course of disease depends on whether yeast are encapsulated (encapsulated yeast may cause a granulomatous reaction) and the patient’s immune status. Invasive cryptococcus has become increasingly common among HIV positive and transplant patients.
Clinical Features
-
Cryptococcal pulmonary disease varies from asymptomatic airway colonization to a slowly progressive lung mass (cryptococcoma), pneumonia, acute respiratory distress syndrome (ARDS), and pleural effusion.
Cytomorphologic Features
-
Round to oval yeasts measuring 5–20 μm are seen with narrow-based buds.
-
Yeasts are surrounded by thick capsules that are positive with mucicarmine, alcian blue, and colloidal iron stains (Figs. 6.10 and 6.11).
Differential Diagnosis
-
Other fungal organisms (e.g., candida, blastomycosis)
-
Fungal mimics
Ancillary Studies
-
Fungal stains (GMS and PAS are positive)
-
Mucicarmine stain is positive in encapsulated forms
-
Fontana-Masson stain may stain the yeast wall
-
India ink (requires live organisms)
-
Immunocytochemistry
-
Serum cryptococcal antigen
-
Fungal culture
Coccidioidomycosis

Coccidioidomycosis. (Left images) The images shown on the left are from a patient who presented with a lung mass that was thought to be a malignancy. An intraoperative touch preparation (top left) revealed a spherule with endospores (H&E stain, high magnification). The lung resection in this case confirmed an infection due to Coccidioidomycosis. A spherule is shown (bottom left) surrounded by granulomatous inflammation and eosinophils (H&E stain, high magnification). (Right images) The images on the right are from a lung FNA of a 33-year-old nonsmoking man who presented with a 3 cm lung nodule. Present among the necrotic acellular material were many large round spherules, some of which were empty (top right) as they were disrupted after being smeared on the slide (DQ stain, high magnification). A GMS stain in this case shows a spherule filled with endospores and many dispersed free spores in the background (high magnification).
Microbiology
-
C. immitis infection typically causes a necrotizing granulomatous inflammation. The major pulmonary manifestations include pulmonary nodules, cavities, diffuse reticulonodular pneumonia, and rarely pleural disease.
-
Fungemia can also produce multiple septic pulmonary emboli, especially in patients with immune deficiency.
Clinical Features
-
Most people are asymptomatic following initial respiratory exposure to arthroconidia. Those who become ill typically develop respiratory symptoms, such as cough, pleurisy, fever, and weight loss.
Cytomorphologic Features
-
The common morphologic forms of C. immitis seen in cytology specimens are thick walled spherules (measuring 10–80 μm) that contain endospores (measuring 2–5 μm). There are generally very few spherules present in most specimens (Fig. 6.12).
-
Sometimes the spherules may be collapsed and appear as empty structures, surrounded by scattered endospores all over the slide.
-
Mycelial elements may rarely be present, but these have no distinguishing morphologic characteristics.
-
An inflammatory background with/without granulomas may be present.
Differential Diagnosis
-
Other large fungal organisms (e.g., Rhinosporidium and Prototheca wickerhamii).
-
Fungal mimics.
Ancillary Studies
-
Fungal stains (GMS, PAS).
-
Gram stain is negative.
-
Mucicarmine stain is positive.
-
Wet preparation of fresh samples using saline or potassium hydroxide solution can be utilized to demonstrate spherules.
-
Calcofluor staining is positive.
-
Immunocytochemistry using a specific fungal antibody
-
Serology and antigen tests
-
Skin test
-
Fungal culture
Aspergillosis

Aspergillosis shown in a ThinPrep preparation of a bronchial washing. Hyphae have relatively straight walls with 45° (dichotomous) branching. The hyphal form of the organism is also septated, best seen with the GMS stain (right image, high magnification). A conidial form (fruiting body) was observed in this specimen (left image, Pap stain, high magnification), as well as calcium oxalate crystals (lower part of the middle image, Pap stain, high magnification).
Microbiology
-
Aspergillosis is caused by the fungus Aspergillus. Transmission occurs via inhalation of airborne conidial forms.
-
Although most people are exposed to this fungus, infections mainly occur in individuals with underlying lung disease (e.g., cystic fibrosis) or impaired immunity (e.g., transplant or AIDS patients).
-
There are four types of lung disease caused by Aspergillus:
-
Allergic bronchopulmonary aspergillosis.
-
Aspergilloma (fungus ball or mycetoma), which develops in a preexisting lung cavity.
-
Chronic necrotizing pneumonia.
-
Invasive pulmonary aspergillosis, which may cause lung infarction and dissemination to other organs.
-
Clinical Features
-
Symptoms depend on the type of infection, and range from cough to hemoptysis or manifestations from extrapulmonary infection.
-
Chest imaging findings are also variable and may include pulmonary infiltrates or a lung cavity with a fungus ball.
Cytomorphologic Features
-
Usually only the hyphal form is seen, characterized by septate hyphae with relatively straight walls and 45° (dichotomous) branching (Fig. 6.13).
-
Conidial forms of this organism (fruiting bodies) are seen when this organism is exposed to air (e.g., abscess cavity or involvement of large airways).
-
A necroinflammatory background is often present.
-
Calcium oxalate crystals, which are strongly birefringent under polarized light, may be seen and are highly suggestive of aspergillosis (Fig. 6.13).
Fig. 6.17. 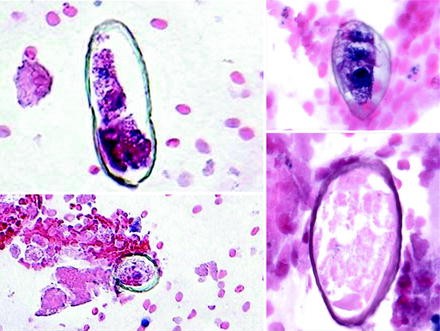
Paragonimus eggs identified in this FNA cell block from a lung nodule. The eggs have a thick, double contour shell (H&E stain, low and high magnification, left and right respectively).

Differential Diagnosis
-
Other fungal organisms (e.g., mucormycosis, candida, blastomycosis).
-
Fungal mimics.
Ancillary Studies
-
Fungal stains (GMS and PAS are positive).
-
Mucicarmine stain is positive.
-
Immunocytochemistry using an immunostain specific to the Aspergillus genus (but not species specific).
Fig. 6.18. 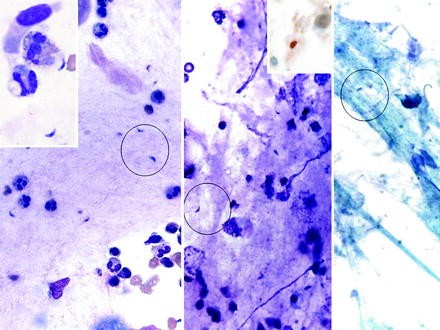
Toxoplasmosis in a BAL specimen from a transplant patient. The extracellular trophozoites caught up in the mucus are banana-shaped organisms with a prominent central nucleus (Giemsa stain, high magnification). The parasites are barely visible with a Pap stain (right image, high magnification). The inset in the middle shows an immunoreactive parasite (immunocytochemical stain, high magnification).
-
Aspergillosis antibody test.
-
Galactomannan (a molecule from the fungus sometimes found in blood).
-
Fungal culture.

Mucormycosis (Zygomycosis)

Pulmonary mucormycosis (zygomycosis). Sputum showing terminal chlamydoconidia that are spherical and have thick walls (Pap stain, intermediate magnification on the left, and high magnification for right images).
Microbiology
-
This invasive fungal infection is caused by mycelia-forming fungi of the Mucorales (e.g., Rhizopus, Mucor spp.) and Entomophthorales (e.g., Conidiobolus and Basidiobolus spp.) orders.
-
Primary pulmonary zygomycosis tends to occur in patients with immunosuppression such as patients with neutropenia, transplant recipients, and in those persons receiving high-dose corticosteroid therapy (Fig. 6.14).
Clinical Features
-
Patients with pulmonary infection typically present with respiratory symptoms like cough, hemoptysis, chest pain, and dyspnea.
Cytomorphologic Features
-
Specimens contain broad, ribbon-like, nonseptate, irregularly shaped hyphae with right-angle branching.
-
One may only find a terminal chlamydoconidium that is spherical with thick walls.
Fig. 6.19. 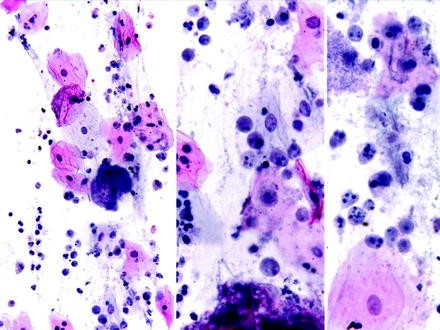
A sputum specimen from a 32-year-old man is shown with E. gingivalis. The amebae are larger than histocytes, have amphophilic bubbly cytoplasm, and a sharply defined nuclear karyosome (Pap stains, intermediate magnification on the left, high magnification middle and right).
-
A necroinflammatory background is often present.

Differential Diagnosis
-
Other fungal organisms (e.g., candida, blastomycosis).
-
Fungal mimics.
Ancillary Studies
-
Fungal stains (GMS and PAS are positive).
-
Mucicarmine stain is positive.
-
Immunocytochemistry using a specific fungal antibody.
-
Direct immunofluorescence.
-
No serologic tests are available.
-
Fungal culture (3–5 days).
Pneumocystis

P. jirovecii (carinii) seen in BAL ThinPrep specimens. Foamy casts are shown containing “empty spaces” that represent cysts entrapped in alveolar exudates (Pap stain, top left intermediate magnification, bottom left high magnification). Numerous alveolar casts are also present in the cell block (top right, H&E stain, intermediate magnification). The cysts tend to aggregate together (bottom middle, GMS stain, high magnification), and often have a central dot-like area in the cyst (right lower, GMS stain, high magnification).
Microbiology
-
Pneumocystis pneumonia (or pneumocystosis) is caused by the yeast-like fungus P. jirovecii (formerly called Pneumocystis carinii).
-
Infection typically involves the distal airspaces and is associated with a foamy or frothy exudate.
-
Immunocompromised patients including persons with AIDS and those receiving immunosuppressive therapy are at increased risk of infection.
Clinical Features
-
Symptoms include fever, nonproductive cough, shortness of breath, weight loss, and night sweats.
-
Complications may include pneumothorax and extrapulmonary disease. Pleural effusion and intrathoracic adenopathy are rare.
-
Specimens used to diagnose pulmonary infection include sputum (induced sputum is more sensitive than expectorated samples), BAL (more invasive but has a greater diagnostic yield), and for intubated patients tracheal aspirates.
Cytomorphologic Features
-
The typical finding is circumscribed foamy alveolar foamy casts that contain cysts. In some cases, casts may be absent, with organisms present only within macrophages.
-
The background inflammatory infiltrate is variable, and may rarely include granulomas.
-
Organisms are not well stained but are still visible with a Papanicolaou stain, seen mainly as multiple clear spaces within casts. Cysts are best visualized with silver stains (e.g., GMS).
-
Cysts measure 4–8 μm, resemble crushed ping-pong balls (cup-shaped), and with a GMS stain a central dot-like area may be seen representing a focus of cell membrane condensation (Fig. 6.15).
-
Cysts tend to be present in aggregates of 2–8, and should not be confused with Histoplasma or Cryptococcus which typically do not aggregate.
-
Budding does not occur. However, adjacent or overlapping cysts may mimic budding organisms.
Differential Diagnosis
-
Other fungal organisms (e.g., Candida, cryptococcus, blastomycosis).
-
Alveolar proteinosis.
-
Amyloidosis.
-
Lysed red blood cells.
-
Other potential mimics including mucus, lubricant, bacterial clumps, talc, neutrophils, hemosiderin filled macrophages, and epithelial cells.
Ancillary Studies
-
Cyst wall stains with GMS, PAS, and mucicarmine stains.
-
Intracystic or free sporozoites (not cyst walls) stain with Giemsa.
-
Immunocytochemistry using a specific Pneumocystis immunostain.
-
Calcofluor white.
-
Direct immunofluorescence.
-
PCR.
Parasitic Infections
Parasites are rare in most developed countries, but may be endemic in other parts of the world. Pulmonary involvement often occurs because the lungs represent a site of infection during the life cycle of some parasites. Infection is often associated with eosinophilia in the blood and pulmonary tissue. Table 6.3 lists parasitic organisms likely to infect the respiratory tract.
Dirofilariasis
-
Humans may acquire Dirofilaria immitis (dog heartworm) through insect vectors (mosquitoes) from dogs. Parasites that become entrapped within pulmonary vessels may result in pulmonary infarction.
-
FNA of infarcted nodules demonstrate worm fragments mixed with necrotic lung tissue and an inflammatory and granulomatous response.
-
Worms measure 120–310 mm in length depending on the sex (females are larger than males). Dirofilaria are distinguished from other nematodes by their prominent muscular lateral cords and striated cuticle.
Strongyloidiasis

Strongyloides stercoralis in a BAL specimen from an HIV positive patient. The specimen shows many filariform larvae with rounded ends and notched (coiled) tails (Pap stain, intermediate magnification left, high magnification right).
-
Strongyloides stercoralis involves the respiratory tract via hematogenous spread of the infective form (filariform larvae), especially in those who are immunosuppressed.
-
Sputum, tracheal aspirates, and BAL samples are all useful for establishing the diagnosis.
-
Filariform larvae are large (400–500 μm), and possess notched tails and a short buccal cavity. They need to be distinguished from the larval forms of Ascaris lumbricoides and hookworms (Fig. 6.16).
Paragonimiasis
-
The species that commonly causes human infection is Paragonimus westermani.
-
Mature worms in the lung shed eggs that may be visible in exfoliated samples (sputum or bronchial washings) or FNA specimens.
-
Eggs have a thick, double contour shell with an operculated end that has a flattened appearance, and, depending upon the species, measure approximately 80–118 μm (Fig. 6.17).
Toxoplasma gondii
-
Lung involvement occurs with severe disseminated infection (toxoplasmosis), especially in neonates (via congenital transplacental infection) and immunocompromised patients.
-
Respiratory specimens like BAL require close inspection for crescent or arc-shaped free (extracellular) trophozoites, as they measure only around 5–7 μm in length. Macrophages may be seen containing several parasites. Parasites contain a prominent central nucleus, and need to be distinguished from similar sized Histoplasma (which exhibit narrow-neck budding) and Leishmania (which also contain a kinetoplast).
-
Parasitic organisms are best identified using a Giemsa-stained preparation.
-
An immunohistochemical stain for Toxoplasma is available (Fig. 6.18).
Entamoeba
-
With Entamoeba histolytica infection, the lungs may be involved by extension from an amebic liver abscess or via hematogenous spread.
-
E. gingivalis is a parasitic protozoan of the oral cavity. In patients with poor oral hygiene, aspiration can result in a lung infection.
-
Amebae have a histiocyte-like morphology and typically contain ingested RBCs in their cytoplasm. Trophozoites are, however, slightly larger than macrophages and have smaller nuclei with coarser chromatin than histiocytes.
-
The morphologic appearances of E. histolytica and E. gingivalis are quite similar, although the trophozoites of E. gingivalis tend to be comparably larger (10–35 vs. 15–20 μm) and, unlike with E. histolytica, there is no associated cyst stage. E. gingivalis is also the only species of amebae that can phagocytose white and red blood cells as well as ingest bacteria (Fig. 6.19).
Echinococcosis (Hydatid Disease)

Echinococcosis (hydatid disease of the lung). This lung FNA from a 38-year-old woman yielded 20 mL of clear fluid that contained numerous intact protoscoleces containing radially arranged hooklets shown with a DQ stain (left, intermediate magnification) and Pap stain (upper right, intermediate magnification). Detached hooklets resembling shark’s teeth are also seen (DQ stain, lower right, high magnification) (images courtesy of Dr. Pawel Schubert, South Africa).
-
The most common cestode pathologic to the lung is Echinococcus granulosus, which manifests as an echinococcal (hydatid) cyst.
-
Patients may be asymptomatic for many years. A primary hydatid cyst of the chest may mimic a neoplasm.
-
FNA usually contains hydatid sand consisting of variable numbers of intact protoscoleces containing radially arranged hooklets and detached (free) refractile hooklets (resembling shark’s teeth) present in a background of thick granular material (Fig. 6.20).
-
Cell blocks may contain portions of a cyst wall that consists of three layers: (1) host layer with giant cells, fibroblasts, and eosinophils; (2) middle acellular laminated membrane; and (3) inner germinal layer.
-
It is controversial whether suspected hydatid cysts should be aspirated as fluid leakage could result in anaphylaxis or disseminated disease.
Pleural Infections and Empyema
-
Pleural (parapneumonic) effusion occurs in 20–40% of hospitalized patients with bacterial pneumonia, and has three stages: exudative (early culture negative), fibrinopurulent (infected), and pleural rind stage. Empyema is defined as pus in the pleural space.
-
Pleural infection can also occur following trauma, surgery, esophageal rupture, or as a result of direct extension (from the lung or subdiaphragmatic disease).
-
Infectious causes of pleural disease include bacteria (e.g., Streptococcus, H. influenza, anaerobes, actinomycosis, Legionella), mycobacteria, fungi (Candida, Pneumocystis), and parasites (E. histolytica).
-
A predominance of neutrophils indicates an acute infection, while many mononuclear inflammatory cells usually indicate a more indolent process (e.g., TB or fungal infection).
-
Pleural fluid eosinophilia (>10%) may be caused by infection (fungal, parasitic) and noninfectious causes (e.g., air, blood, drugs).
Suggested Reading
Lemos LB, Baliga M, Taylor BD, Cason ZJ, Lucia HL. Bronchoalveolar lavage for diagnosis of fungal disease. Five years’ experience in a southern United States rural area with many blastomycosis cases. Acta Cytol. 1995;39:1101–11.
Moriarty AT, Darragh TM, Fatheree LA, Souers R, Wilbur DC. Performance of Candida – fungal-induced atypia and proficiency testing: observations from the College of American Pathologists proficiency testing program. Arch Pathol Lab Med. 2009;133:1272–5.
Naimey GL, Wuerker RB. Comparison of histologic stains in the diagnosis of Pneumocystis carinii. Acta Cytol. 1995;39:1124–7.
Pisani RJ, Wright AJ. Clinical utility of bronchoalveolar lavage in immunocompromised hosts. Mayo Clin Proc. 1992;67:221–7.
Raab SS, Cheville JC, Bottles K, Cohen MB. Utility of Gomori methenamine silver stains in bronchoalveolar lavage specimens. Mod Pathol. 1994;7:599–604.
Saad RS, Silverman JF. Respiratory cytology: differential diagnosis and pitfalls. Diagn Cytopathol. 2010;38:297–307.
Sheehan MM, Coker R, Coleman DV. Detection of cytomegalovirus (CMV) in HIV+ patients: comparison of cytomorphology, immunocytochemistry and in situ hybridization. Cytopathology. 1998;9:29–37.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2011 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Khalbuss, W.E., Laucirica, R., Pantanowitz, L. (2011). Pulmonary Infections. In: Cytopathology of Infectious Diseases. Essentials in Cytopathology, vol 17. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-0242-8_6
Download citation
DOI: https://doi.org/10.1007/978-1-4614-0242-8_6
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-0241-1
Online ISBN: 978-1-4614-0242-8
eBook Packages: MedicineMedicine (R0)