
Abstract
In every epidemic season, viral infections affect the general population, including children, which is an underestimated issue. The present study demonstrates the results of examination of 802 clinical samples obtained from pediatric patients aged 0–14 years during the 2014/2015 epidemic season in Poland. The study was part of the virological surveillance systems – SENTINEL and NON-SENTINEL. A positive result for virological infection was obtained in 50.9 % of samples tested. The distribution of positive results by the age-groups was as follows: 38.2 % in 0–4 years old, 8.5 % in 5–9 years old, and 4.2 % in 10–14 years old children. Influenza viruses accounted for 48.0 % and influenza-like viruses for 52.0 % of all positive samples. Concerning the influenza virus, molecular biology-based techniques confirmed the infection caused by influenza type A in 63.3 % of samples, consisting of unsubtyped A virus detected in 65.3 % of cases of this sample group, subtype A/H1N1/pdm09 in 28.2 %, and subtype A/H3N2/ in 6.5 %. Genetic material of influenza B was detected in 36.7 % of samples. In a group of influenza-like viruses, the predominant virus was respiratory syncytial virus (RSV) in as many as 96.2 % of samples, followed by parainfluenza viruses: PIV3 – 1.4 % and PIV1 – 1.0 %. Attention should be paid to the coinfection of respiratory viruses. There were six possible coinfection combinations reported in Poland, with four of them related to children up to 14 years old.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Influenza, a commonly occurring infectious disease, is caused by a capsular RNA virus. Influenza virus is an important cause of respiratory diseases among children. Young children do not have a well-formed immune system and 30 % of influenza infections occur in the first year of life. Studies also show that children younger than 2 years of age have a high rate of hospitalization attributable to influenza; the rates is comparable to that attributable to influenza among older adults (Izurieta et al. 2000; Neuzil et al. 2000). Healthy children are included in the high-risk group and should be vaccinated against influenza from the age of 6 months (Grohskopf et al. 2014). Unfortunately, the percentage of vaccinated children has been remaining at a very low level, namely 0.6–1.4 %, throughout many epidemic seasons. The annualized level of vaccinated children in Poland in the years 2010–2014, stratified by the age-groups, was as follows: 0.6–0.9 % in 0–4 years old and 1.1–1.5 % in 5–14 years old children (NIPH-NIH 2015). These low estimates are in stark contrast with the verified effectiveness of the trivalent vaccine in healthy children at the level of 59–65 % (Jefferson et al. 2008; Nichol 2008), which decisively points to the highly protective value of influenza vaccination in children. The objective of the present study was to examine clinical samples obtained from pediatric patients aged 0–14 years in one recent epidemic season in Poland to estimate the frequency and type of influenza and influenza-like infections.
2 Methods
2.1 Study Design
The study was approved by an institutional Ethics Committee and was conducted in comport with the principles for biomedical human research as set by the Declaration of Helsinki.
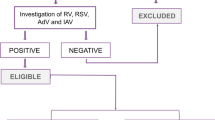
In the 2014/2015 epidemic season, i.e., during the period dating from the 40th week of 2014 to the 28th week of 2015, virological data were collected within the framework of SENTINEL and NON-SENTINEL surveillance programs. The programs are thought to represent a population sample of the country and form a basis for dealing with influenza infection in a subsequent epidemic season. Eight hundred and two clinical specimens from patients aged 0–14 years were tested in 16 Voivodeship Sanitary Epidemiological Stations and in the National Influenza Center of the National Institute of Public Health – National Institute of Hygiene (NIPH-NIH) in Poland. The specimens consisted of nasal swabs, throat swabs, and bronchoalveolar lavage fluid. The patients were stratified by age-groups into: 0–4 years old, 5–9 years old, and 10–14 years old. Epidemiologic data collected from the SENTINEL influenza surveillance concerned only the 0–4 years old and 5–14 years old children.
2.2 Diagnostic Methods
Extraction of Viral RNA
The viral RNA was extracted using a QIAamp Viral RNA Mini Kit (Qiagen; Hilden, Germany) from 140 μl of clinical samples in viral transport medium consisting of phosphate-buffered saline, according to the manufacturer’s instructions. The RNA was eluted with 50 μl of RNase-free water.
Conventional Multiplex Reverse Transcription Polymerase Chain Reaction (RT-PCR)
Multiplex RT-PCR was conducted with an RV12 ACE Detection Kit (Seegene; Seul, South Korea). The assays of the diagnostic panel enabled to detect respiratory viruses, such as influenza A virus, influenza B virus, human respiratory syncytial virus A, human respiratory syncytial virus B, human adenovirus, human metapneumovirus, human coronavirus 229E/NL63, human coronavirus OC43, human parainfluenza viruses 1, 2, and 3, and human rhinovirus A/B. Products of a random hexamer-primed cDNA synthesis were generated using the First Strand cDNA Synthesis Kit (Fermentas; York, UK), according to the manufacturer’s instructions, and were stored at −20 °C until use.
Each cDNA preparation was subjected to the RV12 PCR procedure (Seegene; Seoul, South Korea). The RV12 system enables to simultaneously detect 12 respiratory viruses in two reactions per sample. Amplicons were detected by gel electrophoresis. Briefly, reverse transcription and PCR amplification were performed on the Applied Biosystems Veriti 96-Well Thermal Cycler (Applied Biosystems; Foster City, CA), according to the manufacturer’s instructions.
3 Results
3.1 Epidemiology
In the 2014/2015 epidemic season, a total of 1,580,420 influenza and influenza-like illness cases were reported in children aged 0–14 years in Poland. The incidence of infections was 27,333 per 100,000 children. The distribution by age-groups was as follows: 775,100 cases at 0–4 years of age, with incidence of 38,312 per 100 000, and 805,320 cases at 5–14 years of age, with incidence of 21,424 per 100,000 (Figs. 1 and 2).

Total number of influenza and influenza-like illness reported in children, stratified by age-groups, during the 2014/2015 epidemic season in Poland

Incidence of influenza and influenza-like illness per 100,000 children, stratified by age-groups, during the 2014/2015 epidemic season in Poland
For comparison, in the preceding epidemic season, there were a total of 1,193,511 cases, with incidence of 20,641 per 100,000 children.
3.2 Virology
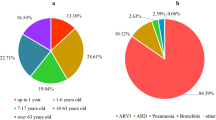
Out of the 802 clinical samples examined in the present study, a positive virology result was obtained in 50.9 % of samples tested. Of those samples with positive virology, 75.0 % was found in the group of 0–4 years of age, 16.7 % in the group of 5–9 years of age, and 8.3 % in the group of 10–14 years of age (Fig. 3). Influenza viruses accounted for 48.0 % of confirmations and influenza-like viruses were detected in 52.0 % of all positive samples. Molecular biology-based techniques confirmed the infections caused by influenza type A in 63.3 % of samples, including influenza virus unsubtyped A which was detected in 65.3 % of cases, subtype A/H1N1/pdm09 in 28.2 %, and subtype A/H3N2/ in 6.5 % of cases. Further, genetic material of influenza B was detected in 36.7 % of samples. With respect to the confirmation of influenza-like viruses, the predominant virus was RSV in as many as 96.2 % of samples, a lower percentage of detected viruses accounted for the family of parainfluenza: PIV3 – 1.4 % and PIV1 – 1.0 %. In addition, the presence of rotavirus was found in 1.4 %. In all three age-groups in the 2014/2015 epidemic season, the predominant influenza infection was with the A/H1N1/pdm09 subtype and as for other viral respiratory infections it was with RSV virus. Data on the diagnostic confirmations in each age-group are tallied in Table 1.

Percentage distribution of positively diagnosed cases of influenza and influenza-like illness combined in children during the 2014/2015 epidemic season in Poland
Attention should be paid to the coinfection with respiratory viruses. There were six possible coinfection combinations reported in Poland, with four of them related to children up to 14 years of age (Table 2).
4 Discussion
Overall, there were more reported cases of influenza and influenza-like illness in children aged 0–14 years in the 2014/2015 epidemic season in Poland than in the preceding 2013/2014 season; a total 1,580,420 with incidence of 27,333 per 100,000 vs. 1,193,511 with incidence of 20,641 per 100,000 children, respectively.
The findings of this study demonstrate that the most frequent incidences of influenza and influenza-like illness concerned children aged 0–4 years in the 2014/2015 epidemic season. The predominant type of influenza virus in this season was A/H1N1/pdm09 virus – 28.2 %, while in the preceding season it was A/H3N2/ virus – 38.3 %. Among influenza-like viruses, in both seasons, the predominant virus was the RSV: this influenza season – 96.2 % and the preceding season – 87.8 %. Of note is a sharp increase in the prevalence of influenza type B virus as a casual factor of infection, which accounted for 36.7 % of positively identified cases in the presently investigated samples of the 2014/2015 season compared with the meager 1.2 % in the preceding 2013/2014 season. Interestingly, the number of confirmations of influenza type B virus increased with increasing age of children, the largest proportion of type B virus was noted in the group of 10–14 years of age (Fig. 4).

Percentage of confirmations of influenza type B in children, stratified by age-groups, during the 2014/2015 epidemic season in Poland
The best protection against influenza for children is immunization. However, there is a mistaken view making the rounds that young children should not be vaccinated. The American Academy of Pediatrics and the U.S. Centers for Disease Control and Prevention Advisory Committee on Immunization Practices recommend routine influenza immunization for healthy children aged 6–23 months, with the aim of reducing influenza incidence and mortality of elderly people living in families along with children (Fiore et al. 2008; American Academy of Pediatrics Committee on Infectious Diseases 2004). The WHO recommends vaccination against influenza from 6 months of age. Negri et al. (2005) have shown that the average efficacy of vaccines for children aged 6 months to 16 years is 65 %. The efficacy of influenza vaccine is affected by the antigenic relationship between strains included in the vaccine and those circulating in a given epidemic season. A study conducted by Joshi et al. (2009) has shown that when there is a good antigenic match of circulating and those included in the vaccine viruses, the effectiveness of vaccination in children below 5 years of age is within 60–85 %. Vaccination of children signifies a reduction in treatment costs for influenza. It has been shown that the cost of treating influenza in children under 2 years of age is higher than that in children aged 2–5 years. The higher cost is associated with parental childcare and related absenteeism at work (Esposito et al. 2011).
In conclusion, influenza is an important clinical, epidemiological, and economic problem, not only in the adult population but also in children. Influenza infection in children remains an undervalued issue.
References
American Academy of Pediatrics Committee on Infectious Diseases (2004) Recommendations for influenza immunization of children. Pediatrics 113:1441–1447
Esposito S, Cantarutti L, Molteni CG, Daleno C, Scala A, Tagliabue C, Pelucchi C, Giaquinto C, Principi N (2011) Clinical manifestations and socio-economic impact of influenza among healthy children in the community. J Infect 62(5):379–387
Fiore AE, Shay DK, Broder K, Iskander JK, Uyeki TM, Mootrey G, Bresee JS, Cox NS, Centers for Disease Control and Prevention (CDC), Advisory Committee on Immunization Practices (ACIP) (2008) Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 57(RR-7):1–60. Available from http://europepmc.org/abstract/med/18685555. Accessed 12 Dec 2015
Grohskopf LA, Olsen SJ, Sokolow LZ, Bresee JS, Cox NJ, Broder KR, Karron RA, Walter EB, Centers for Disease Control and Prevention (CDC), Advisory Committee on Immunization Practices (ACIP) (2014) Prevention and control of influenza: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 63(32):691–697. Available from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6332a3.htm. Accessed 28 Sept 2015
Izurieta HS, Thompson WW, Kramarz P, Shay DK, Davis RL, DeStefano F, Black S, Shinefield H, Fukuda K (2000) Influenza and the rates of hospitalization for respiratory disease among infants and young children. N Engl J Med 342:232–239
Jefferson T, Rivetti A, Harnden A, Di Pietrantonj C, Demicheli V (2008) Vaccines for preventing influenza in healthy children. Cochrane Database Syst Rev (2):CD004879. doi:10.1002/14651858.CD004879.pub32, CD004879
Joshi AY, Iyer VN, St Sauver JL, Jacobson RM, Boyce TG (2009) Effectiveness of inactivated influenza vaccine in children less than 5 years of age over multiple influenza seasons: a case-control study. Vaccine 27(33):4457–4461
NIPH-NIH (2015) National Influenza Center of the National Institute of Public Health – National Institute of Hygiene. Available from http://www.pzh.gov.pl/meldunki-epidemiologiczne/. Accessed 29 Sept 2015
Negri E, Colombo C, Giordano L, Groth N, Apolone G, La Vecchia C (2005) Influenza vaccine in healthy children: a meta-analysis. Vaccine 23(22):2851–2861
Neuzil KM, Mellen BG, Wright PF, Mitchel EF Jr, Griffin MR (2000) The effect of influenza on hospitalizations, outpatient visits, and courses of antibiotics in children. N Engl J Med 342:225–231
Nichol K (2008) Efficacy and effectiveness of influenza vaccination. Vaccine 26(4):D17–D22
Acknowledgements
This work was funded in part by grants 2011/01/B/NZ7/06188 and NIPH-NIH 5/EM.1. We would like to thank physicians and employees of VSESs participating in SENTINEL program for their input into the influenza surveillance in Poland.
Conflicts of Interest
The authors declare no conflicts of interest in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Hallmann-Szelińska, E., Bednarska, K., Kondratiuk, K., Rabczenko, D., Brydak, L.B. (2016). Viral Infections in Children in the 2014/2015 Epidemic Season in Poland. In: Pokorski, M. (eds) Prospect in Pediatric Diseases Medicine. Advances in Experimental Medicine and Biology(), vol 912. Springer, Cham. https://doi.org/10.1007/5584_2016_209
Download citation
DOI: https://doi.org/10.1007/5584_2016_209
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-35103-2
Online ISBN: 978-3-319-35104-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)