
Abstract
Both of the two most common neurodegenerative disorders, namely Alzheimer’s disease (AD) and Parkinson’s disease (PD), have multiple lines of evidence, from molecular and cellular to epidemiological, that nicotinic transmission is implicated in those pathogenesis. This review presents evidences of nicotinic acetylcholine receptor (nAChR)-mediated protection against neurotoxicity induced by β amyloid (Aβ), glutamate, rotenone, and 6-hydroxydopamine (6-OHDA) and the signal transduction involved in this mechanism. Our studies clarified that survival signal transduction, α7 nAChR-Src family-PI3K-AKT pathway and subsequent upregulation of Bcl-2 and Bcl-x, would lead to neuroprotection. Recently analyzing the properties of galantamine, we clarified the neuroprotective pathway, which is mediated by enhancement of microglial α7 nAChR resulting in upregulation of Aβ phagocytosis. Galantamine sensitizes microglial α7 nAChRs to choline and induce Ca2+ influx into microglia. The Ca2+-induced intracellular signaling cascades may then stimulate Aβ phagocytosis through the actin reorganization. This discovery would facilitate further investigation of possible nAChRs enhancing drugs targeting not only neuronal but also microglial nAChRs.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
8.1 Introduction
Alzheimer’s disease (AD) pathology is characterized by the presence of two hallmarks, senile plaques (SP) and neurofibrillary tangles (NFT), and by extensive neuronal loss (Giannakopoulos et al. 1996). β amyloid (Aβ) is a major element of SP and one of the candidates for the cause of the neurodegeneration found in AD. It has been shown that the accumulation of Aβ precedes other pathological changes and causes neurodegeneration and neuronal death in vivo (Yankner et al. 1990). Several mutations of the Aβ precursor protein (APP) are found in familial AD, and these mutations are involved in amyloidogenesis (Citron et al. 1992). Also, familial AD mutations of presenilin 1 (PS-1) enhance the generation of Aβ 1-42 (Tomita et al. 1997). The cerebral cortex contains a dense plexus of cholinergic axon terminals that arise from the cells of the basal forebrain including the nucleus basalis of Meynert (Bigl et al. 1982; Mesulam et al. 1983). Degeneration of this cholinergic projection is recognized as one of the most prominent pathological changes in AD brain (Whitehouse et al. 1981; Rosser et al. 1982). In AD, the cholinergic system is affected, and a reduction in the number of nicotinic acetylcholine receptor (nAChR) has been reported (Shimohama et al. 1986; Whitehouse and Kalaria 1995). ACh receptors are classified into two groups; nAChRs and muscarinic ACh receptors (mAChRs). In the brain, nAChRs show additional complexity, as there are multiple receptor subtypes with differing properties and functions (Clarke et al. 1985; Lindstrom et al. 1995). At least nine α subunits (α2–α7, α9, and α10 in mammals; α8 in chicks) and three β subunits (β2–β4) have been identified in the brain. Both α and β subunits are required to form functional heteropentametric receptors, with the exception of α7–10 subunits, which apparently form functional homopentameric receptors. In the brain, α7 homometric and α4β2 heterometric nAChRs are the two major subtypes. Both α4β2 and α7 subtypes have been implicated in the mechanism of neuroprotection provided by nicotine (Kihara et al. 1998, 2001). It is also known that Aβ binds very strongly to α7 nicotinic acetylcholine receptor (nAChR) (Wang et al. 2000) and up-regulation of α7 nAChR is observed in transgenic mice co-expressing mutant (A246E) human presenilin 1 and (K670N/M671L) APP (Dineley et al. 2002). Multiple lines of evidence show that neuronal nAChRs are involved in synaptic plasticity as well as in neuronal survival and neuroprotection. Moreover, presynaptic nAChRs can modulate the release of many neurotransmitters, including dopamine (DA), noradrenaline, serotonin, ACh, γ-aminobutyric acid (GABA), and glutamate. These neurotransmitter systems play an important role in cognitive and non-cognitive functions such as learning, memory, attention, locomotion, motivation, reward, reinforcement, and anxiety. Thus, nAChRs are considered promising therapeutic targets for new treatments of neurodegenerative disorders. It is also known that α4 and β2 nAChR genes, CHRNA4 and CHRNB2, are causative genes of autosomal dominant nocturnal frontal lobe epilepsy (ADNFLE) (Steinlein et al. 1995; De Fusco et al. 2000). Analyzing the polymorphism of the nAChRs genes in AD patients and controls, we showed that genetic polymorphisms of the neuronal nAChR genes might be related to the pathogenesis of sporadic AD (Kawamata and Shimohama 2002). This, in conjunction with the memory-enhancing activity of nicotine and selective nAChR agonists such as the α7 nAChR agonist, 3-(2,4)- dimethoxybenzylidene anabaseine (DMXBA) (Meyer et al. 1997), suggests a significant role of nAChRs in learning and memory. Therefore, it is generally recognized that the down-regulation of nAChRs is involved in the intellectual dysfunction in AD. Our studies showed that nAChR stimulation protected neurons from Aβ- and glutamate-induced neurotoxicity. This allowed us to hypothesize that nAChRs are involved in a neuroprotective cascade (Kihara et al. 1997, 1998, 2001; Akaike et al. 1994) as described in the following sections.
Parkinson’s disease (PD) is the second most common progressive neurodegenerative disorder next to AD. It is characterized by relatively selective degeneration of dopaminergic neurons in the substantia nigra and loss of dopamine in the striatum resulting in resting tremor, rigidity, bradykinesia and postural instability (Shimohama et al. 2003; Obeso et al. 2010). Although the pathogenesis of PD is still unclear, it is thought that the interaction of gene and the environment plays roles in causing the multi-factorial disease. Rural residency, pesticides and intrinsic toxic agents were reported as environmental risk factors for sporadic PD. Recent studies revealed several mutations in familial PD genes such as α-synuclein, parkin, PINK1, LRRK2, DJ-1, UCHL1, ATP13A2 and GBA (glucocerebrocidase) (Hardy 2010; Sidransky et al. 2009). The most reproducible epidemiological relevant factor against Parkinson’s disease (PD) is cigarette smoking habits (Dorn 1959; Quik 2004). Epidemiological studies suggest that the use of pesticides increases the risk of PD, possibly via reduced activity of complex I in the mitochondrial respiratory chain in the substantia nigra (Parker et al. 1989; Mann et al. 1992; Mizuno et al. 1998). Grady et al. examined mouse brain using in situ hybridization to characterize the mRNA expression pattern of nAChRs. The ventral tegmental area (VTA) and substantia nigra expressed high concentrations of α4 and α6 and β2, and β3 mRNAs, intermediate levels of α5 mRNA, and low levels of the α3 and α7 mRNAs. No signal for α2 and β4 mRNA was detected (Le Novère et al. 1996; Grady et al. 2007). They reviewed the subtypes of nAChRs on dopaminergic terminals of mouse striatum reporting five nAChR subtypes that expressed on dopaminergic nerve terminals, three of which are α6 containing subunits, namely α4α6β2β3, α6β2β3, and α6β2. The remaining two subtypes, α4β2, α4α5β2, are more numerous than the α6-containg subtypes. The α6 containing nAChRs, which do not contribute to dopamine release induced by nicotine, are mainly located on dopaminergic neuronal terminals and probably mediating the endogenous cholinergic modulation of dopamine release at the terminal level. In contrast, α4β2 nAChR represent the majority of functional heteromeric nAChRs on dopaminergic neuronal soma. α7 nAChRs are present on dopaminergic neuronal soma, contributing to nicotine reinforcement (Champtiaux et al. 2003). There are several studies analyzing the decline of specific nAChRs in PD patients. Court et al. reported the decline of α3 subunits and no change of α7 subunits. Gotti et al. and Court et al. reported decreased level of α4 subunits but Guan et al. reported not (Court et al. 2000; Gotti et al. 1997; Guan et al. 2002). Bordia et al. reported the decline of α6 subunits in caudate and putamen. They further specified that the most vulnerable subtype in striatum of MPTP-treated mice and monkeys is α6α4β2β3 rather than α6β2β3 and further identified the specific loss of α6α4β2β3 subtype in PD brains (Bordia et al. 2007). These results seem to indicate that the decline of nigrostriatal specific α6 subtypes is highly specific and relevant to the PD pathogenesis but not is α7 subtype. Functional studies on α6 nAChRs should be undertaken to confirm its pathological importance in PD. For this purpose, Drenan et al. (2008) generated the gain-of-function α6 nAChR transgenic mouse, which turned to present locomotive hyperactivity. With low dose of nicotine by the way of stimulating dopamine but not GABA, its phenotype was exaggerated and hyperdopaminergic state in vivo was observed. Current drug therapy against PD is limited to supplementing DA or enhancing dopaminergic effect. Some may have neuroprotective effects, but their effects remain controversial (Quik 2004; Du et al. 2005; Iravani et al. 2006). It has also been reported that smokers have a lower risk for PD (De Reuck et al. 2005; Wirdefeldt et al. 2005), and nAChRs were decreased in the brains of PD patients (Fujita et al. 2006) and model animals (Quik et al. 2006a). Nicotine may upregulate DA release at striatum from nigral dopaminergic neurons (Morens et al. 1995), followed by stimulation of α4β2 nAChRs (Champtiaux et al. 2003). Furthermore, nicotine could protect mitochondria and had protective effect from oxidative stress (Cormier et al. 2003; Xie et al. 2005). In studies made in vivo, stimulation of nAChRs resulted in neuroprotection in PD model animals (Parain et al. 2003). Although several clinical trials to evaluate possible therapeutic effect of nicotine to PD patients have been conducted, whether nicotine has therapeutic effects on PD is still controversial. The relatively high dose transdermal nicotine administration might have therapeutic effect on PD patients (Villafane et al. 2007). In the following we present evidence for nAChR-mediated neuroproptection in PD models based mainly on our studies.
8.2 Alzheimer’s Disease and nAChRs
8.2.1 nAChR Enhancement Shows Neuroprotection Against Glutamate Toxicity
Glutamate cytotoxicity is one of the most suspected causative pathways in neurodegenerative process, namely in AD and PD. To give examples, it is also assumed that glutamate plays an important role in the neurodegeneration observed in hypoxic-ischemic brain injury (Choi 1988; Meldrum and Garthwaite 1990). Several investigators have also suggested that cortical neurodegeneration in AD is attributable to glutamate (Maragos et al. 1986; Mattson 1988). Moreover, brief glutamate exposure induces delayed cell death in cultured neurons from certain brain regions, such as the cerebral cortex and hippocampus. In these brain regions, the N-methyl-D-aspartate (NMDA) glutamate receptor subtype plays a crucial role in glutamate neurotoxicity. Several studies have indicated the existence of nitric oxide (NO) synthase in the CNS, including the cerebral cortex. NMDA receptor stimulation induces Ca2+ influx into cells through ligand-gated ion channels, thereby triggering NO formation. NO is also thought to diffuse to the adjacent cells, resulting in the appropriate physiological response and/or glutamate-related cell death (Choi 1988; Hartley and Choi 1989; Dawson et al. 1991).
We examined the effects of nicotine on glutamate-induced neurotoxicity using primary cultures of rat cortical neurons. Cell viability was decreased by treatment with 1 mM glutamate for 10 min followed by incubation in glutamate-free medium for 1 h. Incubating the cultures with 10 μM nicotine for 24 h prior to glutamate exposure significantly reduced glutamate cytotoxicity. To investigate whether nicotine-induced neuroprotection is due to a specific effect mediated by nAChRs, the effects of cholinergic antagonists were examined. An addition of dihydro-β-erythroidine (DHβE), an α4β2 nAChR antagonist, or α-BTX, an α7 nAChR antagonist, to the medium containing nicotine reduced the protective effect of nicotine. We also examined the protection of nicotine against the effects of ionomycin, a calcium ionophore, and SNOC, an NO-generating agent. Incubating the cultures for 10 min in either 3 μM ionomycin- or 300 μM SNOC-containing medium markedly reduced cell viability. A 24-h pretreatment with nicotine significantly attenuated the ionomycin cytotoxicity, but did not affect the SNOC cytotoxicity (Akaike et al. 1994; Shimohama et al. 1996; Kaneko et al. 1997) (Fig. 8.1).

Proposed hypothesis for the mechanism of nAChR-mediated survival signal transduction against glutamate-Iinduced necrosis. The NMDA glutamate receptor subtype plays a crucial role in glutamate neurotoxicity. NMDA receptor stimulation induces Ca2+ influx into cells through ligand-gated ion channels, thereby triggering NO formation. NO would diffuse to the adjacent cells, resulting in the appropriate physiological response and/or glutamate-related cell death
We have also shown that nicotinic α7 nAChRs protect against glutamate neurotoxicity and neuronal ischemic damage in vivo. The α7 nAChR agonist, dimethoxybenzylidene anabaseine (DMXBA), protected rat neocortical neurons against excitotoxicity administered 24 h before, but not concomitantly with, NMDA. This action was blocked by nicotinic but not muscarinic antagonists. DMXBA (1 mg/kg i.p.) also reduced infarct size in rats when injected 24 h before, but not during, focal ischemic insults. In a mecamylamine-sensitive manner, α7 nAChRs appear neuroprotective in non-apoptotic model (Shimohama et al. 1998).
8.2.2 Nicotine Protects Neurons Against Aβ Toxicity In Vitro
A 48-h exposure to 20 μM neurotoxic Aβ25–35 caused a significant reduction in the neuronal cells of rat fetal primary culture. Simultaneous incubation of the cultures with nicotine and Aβ significantly reduced the Aβ-induced cytotoxicity. The protective effect of nicotine was reduced by both DHβE and α-BTX. The effect of a selective α4β2 nAChR agonist, cytisine, and a selective α7 nAChR agonist, DMXBA (Hunter et al. 1994), on Aβ cytotoxicity was examined. Aβ cytotoxicity was significantly reduced when 10 μM cytisine or 1 μM DMXB was co-administered. These findings suggest that both α4β2 and α7 nAChR stimulation is protective against Aβ cytotoxicity. In addition, MK-801, an NMDA receptor antagonist, inhibited Aβ cytotoxicity when administrated simultaneously with Aβ, suggesting that Aβ cytotoxicity is mediated via the NMDA receptor, or via glutamate in cultured cortical neurons (Kihara et al. 1997, 1998, 2001).
Although it is regarded that PS-1 mutations enhance the generation of Aβ1–42, it is controversial whether Aβ is directly toxic to neurons. We found that Aβ25–35-induced neurotoxicity was inhibited by MK801. It can therefore be hypothesized that Aβ might modulate or enhance glutamate-induced cytotoxicity. Indeed, Aβ causes a reduction in glutamate uptake in cultured astrocytes (Harris et al. 1996), indicating that, to some extent, Aβ-induced cytotoxicity might be mediated via glutamate cytotoxicity.
In our study (Kihara et al. 2000), incubation of the cortical neurons with both Aβ1–40 (1 nM) and Aβ1–42 (100 pM) for 7 days did not induce cell death. These are the concentrations of Aβ in the cerebrospinal fluid (CSF) of AD patients (Jensen et al. 1999). Although 20 μM glutamate alone did not significantly induce cell death, exposure to 20 μM glutamate for 24 h caused a significant reduction in the neuronal cells in the Aβ-treated group, showing that Aβ itself is not toxic at low concentrations, but makes neurons vulnerable to glutamate. Conversely, co-incubation of the cultures with nicotine (50 μM for 7 days) and Aβ significantly reduced Aβ-enhanced glutamate cytotoxicity (Akaike et al. 1994; Shimohama et al. 1996; Kaneko et al. 1997).
To investigate the mechanism of the protective effect of nicotine, we focused on the phosphatidylinositol 3-kinase (PI3K) pathway because PI3K had been shown to protect cells from apoptosis (del Peso et al. 1997). Long exposure to low concentrations of glutamate (50 μM for 24 h) induced cytotoxicity. Incubating the cultures with nicotine (10 μM for 24 h) prior to glutamate exposure significantly suppressed glutamate cytotoxicity. Simultaneous application of LY294002, a PI3K inhibitor, with nicotine cancelled the protective effect of nicotine. α-BTX blocked the protection provided by nicotine and DMXB. Furthermore, this DMXBA-induced protection was also reduced by LY294002. Although α4β2 nAChR stimulation also had a protective effect on Aβ- and glutamate-induced cytotoxicity, this effect was not inhibited by LY294002, suggesting PI3K system is not directly involved in α4β2 nAChR-mediated neuroprotection. PD98059, a mitogen-activated protein (MAP) kinase kinase (MEK) inhibitor, did not reduce the protective effect of nicotine, also suggesting that the MEK/ERK pathway is not directly involved in the protective effect of nicotine. A non-receptor tyrosine kinase inhibitor, PP2, did reduce the protective effect of nicotine, suggesting that Src is involved in the mechanism of the protective effect. Cycloheximide also inhibited the protection, implying that some protein synthesis is necessary for this effect.
AKT is a serine/threonine protein kinase and a putative effector of PI3K. To investigate the activation of AKT by nicotine through PI3K, we examined the level of phosphorylated AKT using an anti-phospho-specific AKT antibody. The phosphorylated form of AKT appeared immediately after the application of nicotine. Nicotine-induced AKT phosphorylation was blocked by simultaneous application of LY294002, but not of PD98059, indicating that PI3K, but not MAPK is involved. The AKT phosphorylation is blocked by α-BTX, but not by DHβE, implying that nicotine-induced AKT phosphorylation is mediated by α7 but not by α4β2 nAChRs. PP2 also blocked AKT phosphorylation, which suggests the involvement of tyrosine kinase. The level of total AKT protein which was detected with anti-AKT antibody remained unchanged.
Bcl-2 and Bcl-x proteins are anti-apoptotic proteins that can prevent cell death induced by a variety of toxic attacks (Zhong et al. 1993). It has been reported that AKT activation leads to the overexpression of Bcl-2 (Matsuzaki et al. 1999). Because nicotine can activate AKT via PI3K, we examined the protein levels of Bcl-2 and Bcl-x. We found that treatment with nicotine for 24 h increased the levels of Bcl-2 and Bcl-x, and this was inhibited by LY294002, which indicates the involvement of the PI3K pathway in nicotine-induced Bcl-2 and Bcl-x upregulation. These results suggest that nAChR stimulation protects neurons from glutamate-induced cytotoxicity by activating PI3K, which in turn activates AKT and upregulates Bcl-2 and Bcl-x (Kihara et al. 2001) (Fig. 8.2).

Proposed hyposis for the mechanism of nAChR-mediated survival signal transduction against Aβ-induced apoptosis. Nicotine-induced neuroprotection is mediated via nAChRs, especially through α7 and α4β2 receptors, and inhibited by a PI3K inhibitor and an Akt/PKB inhibitor. This means that nicotine activates the PI3K-Akt/PKB pathways and increase survival of neurons. JAK2 and Fyn are key molecules trigger activation of the PI3K-Akt/PKB pathways which lead to subsequent upregulation of Bcl-2 and neuroprotection
8.2.3 Galantamine Acts As an Allosteric Potentiating Ligand (APL) of nAChRs and Blocks Aβ-Enhanced Glutamate Toxicity In Vitro
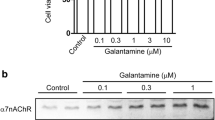
Galantamine is an acetylcholinesterase inhibitor (AChEI) that is currently used for the treatment of AD. Although its AChEI activity appears to be much weaker than other clinically available AChEIs, its therapeutic effects on cognitive function in AD are comparable with the other agents. Furthermore, the long term extension clinical trial of galantamine suggested that the cognitive benefits of galantamine are sustained for at least 36 months (Raskind et al. 2004). In addition to the inhibition of AChE, galantamine binds to nAChRs and allosterically potentiates their synaptic transmission. Consequently, galantamine is called an allosteric potentiating ligand (APL) of nAChRs. This APL effect is present on both α7 and α4β2 nAChRs (Maelicke et al. 2001). Thus, galantamine could stimulate cholinergic transmission in two ways: (1) by inhibiting AChE and increasing AChs, and (2) by potentiating cholinergic transmission through the APL effect. We demonstrated that galantamine protected cortical neurons against Aβ-enhanced glutamate toxicity by, at least partially, the α7 nAChR-PI3K-AKT pathway (Kihara et al. 2004).
8.2.4 Galantamine-Induced Aβ Clearance Mediated via Stimulation of Microglial nAChRs
We found that in human AD brain, microglia accumulates on Aβ deposits and expresses α7 nAChRs including the APL-binding site, which is recognized specifically with FK1 antibody. Treatment of rat microglia with galantamine significantly enhanced microglial Aβ phagocytosis, and acetylcholine competitive angatonists as well as FK1 antibody inhibited the enhancement.
We further demonstrated that galantamine treatment facilitated Aβ clearance in brains of rodent AD models. We investigate effect of daily intraperitoneal galantamine (1 or 5 mg/kg) administration on Aβ clearance in rat that had received intrahippocampal Aβ42 (1 μg) injection. The amount of Aβ was significantly reduced by galantamine in a dose-dependent manner, compared with the vehicle-treated rats. This result suggests that galantamine may enhance microglial Aβ phagocytosis and promote the Aβ clearance from the Aβ-injected rat brain.
Hemizygous APdE9 mice is expressing chimeric mouse/human amyloid precursor protein APPswe (mouse APP695 harboring a human Aβ domain and mutations K594N and M595L linked to Swedish familial AD pedigrees) and human mutated presenilin 1-dE9 (deletion of exon 9), and present a weak decline in spatial learning and memory at 9 months of age. We had administrated the mice galantamine (1 or 5 mg/kg) from 9 months of age for 7 weeks and evaluated spatial learning and memory using water maze testing at 11 months of age. Both low and high dose galantamine significantly improved the performance in the 11 months old APdE9 mice. Pathological evaluation also revealed that the Aβ burden in the brains of APdE9 mice treated with galantamine show less Aβ plaque. The measurement of amount of insoluble Aβ40 and Aβ42 in formic acid-extracted fraction of the brain revealed a significant decrease in galantamine-treated mice compared to sham treated mice.
Using primary-cultured rat microglia, we evaluated the microglial Aβ phagocytosis. We treated rat microglia with 1 μM Aβ42 in the presence or absence of galantamine or nicotine. Galantamine enhanced microglial Aβ phagocytosis in a concentration-dependent manner and phagocytosis reached the peak at 1 μM galantamine. Nicotine also increased Aβ phagocytosis at the concentration of 1000 μM. These effects were inhibited by pretreatment with the blockage of APL-binding site by FK1 antibody as well as with nAChR antagonists. Although galantamine-enhanced microglial Aβ phagocytosis was significantly inhibited by FK1 antibody, Fk1 antibody alone did not influence the magnitude of Aβ phagocytosis in the absence of galantamine. From these findings, we can assume that the galantamine-enhanced microglial Aβ phagocytosis requires the combined actions of an acetylcholine competitive agonist and the APL for nAChRs. In fact, depletion of choline, an acetylcholine-competitive α7 nAChR agonist, from the culture medium impedes the enhancement.
We investigated whether the Ca2+ influx correlates with enhanced microglial Aβ phagocytosis. In the absence of galantamine or nicotine, the levels of microglial Aβ phagocytosis were almost the same in Ca2+ (−) or Ca2+ (+) DMEM. Galantamine and nicotine significantly enhanced microglial Aβ phagocytosis in Ca2+ (+) DMEM, but not in Ca2+ (−) condition. Similarly, inhibition of the calmodulin-dependent pathways for the actin reorganization by 20 μM W-7, an inhibitor of calmodulin, or 10 μM KN93, an inhibitor of Ca2+/CaM-dependent protein kinase II (CaMKII), abolished the enhancement. We evaluated other signaling cascades including JAK2-PI3K-AKT cascade, Fyn-PI3K-AKT cascade, MAPKK (MEK) cascade, using each inhibitor and concluded that they are not involved in galantamine enhanced microglial Aβ phagocytosis. These results suggest that Ca2+ influx through nAChRs and subsequent activation of CaM-CaMKII signaling cascade were involved in enhanced microglial Aβ phagocytosis through the actin reorganization (Takata et al. 2010) (Fig. 8.3).

Proposed pathway for microglial CaM/CaMKII/Aβ phagocytosis. Ca2+ influx through nAChRs and subsequent activation of CaM-CaMKII signaling cascade are involved in enhanced microglial Aβ phagocytosis through the actin reorganization
8.2.5 Donepezil Promotes Internalization of NMDA Receptors by Stimulating α7 nAChRs and Attenuates Glutamate Cytotoxicity
Donepezil is one of the most widely prescribed AChEI for the treatment of AD and related dementias. Our group reported that in addition to up-regulating the PI3K-AKT pathway, there is another mechanism underlying neuroprotection by donepezil, showing decreases glutamate toxicity through down-regulation of NMDA receptors, following stimulation of α7 nAChRs in primary rat neuron cultures (Shen et al. 2010).
8.2.6 Donepezil Directly Acts on Microglia to Inhibit Its Inflammatory Activation
Hwang et al. reported that 5–20 μM donepezil attenuates microglial production of nitric oxide and tumor necrosis factor (TNF)-α, and suppressed the gene expression of inducible nitric oxide synthase, inteleukin-1β, and TNF-α in the microglia cultures. They also confirmed donepezil inhibit inflammatory NF-kB signaling in microglial cell line (Hwang et al. 2010).
8.2.7 Temporal Changes of CD68 and α7nAChR Expression in Microglia in AD-Like Mouse Models
As shown above, activated microglia are involved in Aβ clearance and that stimulation of α7nAChR in microglia enhances Aβ clearance. Nevertheless, how microglia and α7 nAChR in microglia are affected in AD remains unknown. The study aimed to collect fundamental data for considering whether microglia are potential targets for AD treatment and the appropriate timing of therapeutic intervention, by evaluating the temporal changes of Aβ, microglia, neurons, presynapses, and α7 nAChR by immunohistochemical studies in mouse models of AD. In an Aβ-injected AD mouse model, we observed early accumulation of CD68-positive microglia at Aβ deposition sites and gradual reduction of Aβ. Microglia were closely associated with Aβ deposits, and were confirmed to participate in clearing Aβ. In a transgenic mouse model of AD, we observed an increase in Aβ deposition from 6 months of age, followed by a gradual increase in microglial accumulation at Aβ deposit sites. Activated microglia in APdE9 mice showed two-step transition: a CD68-negative activated form at 6–9 months and a CD68-positive form from 12 months of age. In addition, α7 nAChR in microglia increased markedly at 6 months of age when activated microglia appeared for the first time, and decreased gradually coinciding with the increase of Aβ deposition. These findings suggest that early microglial activation is associated with α7 nAChR upregulation in microglia in APdE9 mice. These novel findings are important for the development of new therapeutic strategy for AD (Matsumura et al. 2015).
8.3 Parkinson’s Disease and nAChRs
8.3.1 nAChR Enhancement Shows Dopaminergic Neuronal Protection Against Rotenone Cytotoxicity
Rotenone is a naturally occurring complex ketone pesticide derived from the roots of Lonchocarpus species. It can rapidly cross over cellular membranes without the aid of transporters, including the blood brain barrier (BBB). Rotenone is a strong inhibitor of complex I, which is located at the inner mitochondrial membrane and protrudes into the matrix. In 2000, Betarbet et al. (2000) demonstrated with rat model that chronic systemic exposure to rotenone causes many features of PD, including slow-progressive dopamine neuronal loss in nigrostriatal dopaminergic system, and Lewy body-like particles, which are primarily aggregations of α-synuclein (Mizuno et al. 1998; Inden et al. 2007). Rotenone works as a mitochondrial complex I inhibitor. Acute lethal doses of rotenone eliminate the mitochondrial respiratory system of the cell, resulting in an anoxic status that immediately causes cell death. At sub-lethal doses it causes partial inhibition of mitochondrial complex I, and in this situation mitochondrial dysfunction leads to increased oxidative stress, decreased ATP production, increased aggregation of unfolded proteins, and then activated apoptotic pathway(s) that result in neuronal cell death (Betarbet et al. 2000), resembling dopaminergic neurodegeneration in PD.
In cultures of rat fetus mesencephalic neurons, 48 h exposure to rotenone caused dose-dependent neurotoxicity, more evident in dopaminergic neurons than in other neuronal cells. This result showed that dopaminergic neurons were more vulnerable to rotenone-induced neurotoxicity. Simultaneous administration of nicotine resulted in a dose-dependent increase of the viability of dopaminergic neurons. This neuroprotective effect was inhibited by 100 μM mecamylamine, a broad-spectrum nAChR antagonist, 100 nM αBuTx and 1 μM DHβE. Nicotine-induced neuroprotection was therefore shown to occur via nAChRs, especially through α7 and α4β2 receptors. Furthermore, nicotinic neuroprotection is inhibited by LY294002, a PI3K inhibitor, and triciribine, an AKT/PKB inhibitor. This means that nicotine could activate the PI3K-AKT/PKB pathways and increase the survival of mesencephalic dopaminergic cells against rotenone-induced cell death (Takeuchi et al. 2009). From our previous studies, it is known that the PI3K-AKT/PKB pathways would lead to subsequent upregulation of Bcl-2 and neuroprotection (Akaike et al. 2010; Shimohama 2009).
We confirmed that orally rotenone (30 mg/kg for 28 days)-treated mouse model showed motor deficits, dopaminergic cell death in the substantia nigra, and nerve terminal/axonal loss in the striatum. These findings are relevant to some previous reports on rotenone PD models (Schmidt and Alam 2006; Ravenstijn et al. 2008). Simultaneous subcutaneous administration of nicotine (0.21 mg/kg/day) prevented both motor deficits and dopaminergic neuronal cell loss in the substantia nigra of rotenone-treated mice.
8.3.2 nAChR Enhancement Show Dopaminergic Neuronal Protection Against 6-OHDA- Induced Hemiparkinsonian Rodent Model
6-hydroxydopamine (6-OHDA)’s strong neurotoxic effects were described by Ungerstedt in 1971, in a study presenting the first example of using a chemical agent to produce an animal model of PD (Ungerstedt 1971). Since 6-OHDA cannot cross over the BBB, systemic administration fails to induce parkinsonism. This induction model requires 6-OHDA to be injected into the SN, medial forebrain bundle, and striatum. The intrastriatal injection of 6-OHDA causes progressive retrograde neuronal degeneration in the VTA and substantia nigra.
Costa et al. evaluated the neuroprotection of nicotine in 6-OHDA-induced hemiparkinsonian rat model. They injected 6 μg 6-OHDA in the SN, and confirmed that the dopamine level in the corpus striatum was decreased nearly by half. Repeated subcutaneous nicotine administration at 4 h before and 20, 44 and 68 h after 6-OHDA injection significantly prevented the striatal dopamine loss and the protection reverted by nAChR antagonist. The protective effect was not achieved by one-off administration of nicotine before or after 6-OHDA injection (Costa et al. 2001).
Using rat 6-OHDA-induced hemiparkinsonian model, the neuroprotective effects of galantamine and nicotine were evaluated. 32 nmol 6-OHDA with or without 4–120 nmol galantamine and/or 120 nmol nicotine were injected into unilateral SN of rats. Although methamphetamine-stimulated rotational behavior and dopaminergic neuronal loss induced by 6-OHDA were not inhibited by galantamine alone, those were moderately inhibited by nicotine alone. In addition, 6-OHDA-induced neuronal loss and rotational behavior were synergistically inhibited by co-injection of galantamine and nicotine. These protective effects were abolished by mecamylamine, a nAChR antagonist. α7nAChR was expressed on both dopaminergic and non-dopaminergic neurons in the rat substantia nigra pars compacta (SNpc). A combination of galantamine and nicotine greatly suppressed 6-OHDA-induced reduction of α7nAChR- immunopositive dopaminergic neurons. These results suggest that galantamine synergistically enhances the neuroprotective effect of nicotine against 6-OHDA-induced dopaminergic neuronal loss through an allosteric modulation of α7nAChR activation (Yanagida et al. 2008).
To explore a novel therapy against PD through enhancement of α7 nAChR, we evaluated the neuroprotective effects of DMXBA in a rat 6-OHDA-induced hemiparkinsonian model. Microinjection of 6-OHDA into the nigrostriatal pathway of rats destroys dopaminergic neurons selectively. DMXBA dose-dependently inhibited methamphetamine-stimulated rotational behavior and dopaminergic neuronal loss induced by 6-OHDA. The protective effects were abolished by methyllycaconitine citrate salt hydrate, an α7 nAChR antagonist. Immunohistochemical study confirmed abundant α7 nAChR expression in the cytoplasm of dopaminergic neurons. These results indicate that DMXBA prevented 6-OHDA-induced dopaminergic neuronal loss through stimulating α7 nAChR in dopaminergic neurons. Injection of 6-OHDA elevated immunoreactivities to glial markers such as ionized calcium binding adaptor molecule 1, CD68, and glial fibrillary acidic protein in the substantia nigra pars compacta of rats. In contrast, these immunoreactivities were markedly inhibited by comicroinjection of DMXBA. Microglia also expressed α7 nAChR in both resting and activated states. Hence, we hypothesize that DMXBA simultaneously affects microglia and dopaminergic neurons and that both actions lead to dopaminergic neuroprotection. The findings that DMXBA attenuates 6-OHDA-induced dopaminergic neurodegeneration and glial activation in a rat model of PD raise the possibility that DMXBA could be a novel therapeutic compound to prevent PD development (Suzuki et al. 2013) (Fig. 8.4).

Proposed pathway for nAChR-mediated neuronal protection: direct effect to neurons and indirect effect to microglia against 6-OHDA-induced hemiparkinsonian rodent model. We hypothesize that DMXBA simultaneously affects microglia and dopaminergic neurons and that both actions lead to dopaminergic neuroprotection
8.3.3 α4 nAChR Modulated by Galantamine on Nigrostriatal Terminals Regulates Dopamine Receptor-Mediated Rotational Behavior
This study was designed to evaluate the allosteric effect of galantamine on nAChR regulation of nigrostrial dopaminergic neuronal function in the hemiparkinsonian rat model established by unilateral nigral 6-OHDA injection. Methamphetamine, a dopamine releaser, induced ipsilateral rotation, whereas dopamine agonists apomorphine (a non-selective dopamine receptor agonist), SKF38393 (a selective dopamine D1 receptor agonist), and quinpirole (a selective dopamine D2 receptor agonist) induced contralateral rotation. When 6-OHDA-injected rats were co-treated with nomifensine, a dopamine transporter inhibitor, a more pronounced and a remarkable effect of nicotine and galantamine was observed. Under these conditions, the combination of nomifensine with nicotine or galantamine induced the ipsilateral rotation similar to the methamphetamine-induced rotational behavior, indicating that nicotine and galantamine also induce dopamine release from striatal terminals. Both nicotine- and galantamine-induced rotations were significantly blocked by flupenthixol (an antagonist of both D1 and D2 dopamine receptors) and mecamylamine (an antagonist of nAChRs), suggesting that galantamine modulation of nAChRs on striatal dopaminergic terminals regulates dopamine receptor-mediated movement. Immunohistochemical staining showed that α4 nAChRs were highly expressed on striatal dopaminergic terminals, while no α7 nAChRs were detected. Pretreatment with DHβE significantly inhibited nicotine- and galantamine-induced rotational behaviors, whereas pretreatment with methyllycaconitine was ineffective. Moreover, the α4 nAChR agonist ABT-418 induced ipsilateral rotation, while the α7nAChR agonist PNU282987 had no significant effect on rotational behavior. These results suggest that galantamine can enhance striatal dopamine release through allosteric modulation of α4 nAChRs on nigrostriatal dopaminergic terminals (Inden et al. 2016).
8.3.4 Neuroprotective Effect of Nicotine in MPTP-Induced Parkinsonian Model
In 1979 and 1983, MPTP was initially identified as a strong neurotoxin when heroin addicts accidentally self-administered MPTP and developed an acute form of parkinsonism that was indistinguishable from idiopathic PD (Davis et al. 1979; Langston et al. 1983). The tragic results of MPTP poisoning in the heroin addicts led to the development of MPTP-induced rodent and non-human primate animal models of PD. Jeyarasasingam et al. reported exposure of rat primary mesencephalic cultures to 10−7 and 10−4 M nicotine partially protect against dopaminergic neurotoxicity induced by 1-methyl-4-phenylpyridinium (MPP+). The optimal protective effect was observed when pre-exposure to nicotine for 24 h before administration of MPP+. They also showed the nicotine protection was mediated by non-α7 nAChR stimulation but not through α7 nAChR stimulation (Jeyarasasingam et al. 2002). Junyent et al. reported comparison of two prosurvival pathways, AKT pathway and JAK2/STAT3 pathway, in MPP+ treated cerebellar granule cell culture. Their data indicated that the treatment of cerebellar granule cell with MPP+ decreased both survival pathways. Loss of STAT3 could be a signal pathway involved in neuroprotection against the MPP+, whereas AKT activation, using a PTEN inhibitor, did not play a prominent role in neuroprotection (Junyent et al. 2010).
In MPTP-induced animal model, the neuroprotective effect of nicotine is not consistent probably due to different experimental methods. Besides small number of negative reports (Behmand and Harik 1992), several independent groups confirmed the neuroprotective effects of nicotine against MPTP in rodents. The pretreatment of nicotine is essential and post treatment did not show any neuroprotective effect in MPTP-induced rat as well as in primate models. There are many reports attributing the neuroprotective effect of cigarette smoking against MPTP cytotoxicity to inhibition of monoamine oxidase B (MAO-B), which converts MPTP to active MPP+. But because of the fact that nicotine does not inhibit brain MAO-B, the nicotinic neuroprotection against MPTP cytotoxicity is not mediated through MAO-B inhibition. A blockade of MPP+ uptake into the dopaminergic cells via increased dopamine release may be the reason of the protective effect. Jasons et al. (1992) reported the chronic infusion of nicotine via minipumps produced a dose-related enhancement of MPTP-induced dopaminergic neurotoxicity in mouse, which might be caused by a failure of nAChRs to desensitized to the chronic nicotine exposure (Parain et al. 2001, 2003). Regarding to primate model, there have been only several papers from one group examining the nicotine-induced neuronal protection in MPTP-induced primate PD motor deficit model (Quik et al. 2006a, b; Bordia et al. 2006; Huang et al. 2009). In their reports, neuroprotection was observed only when nicotine is given orally before the MPTP exposure. Decamp and Schneider established stable cognitive deficit primate model injecting low dose of MPTP (0.025–0.10 mg/kg) over a period ranging from 98 to 158 days, without the confounding effect of significant motor impairment. They examined the effect of nicotine, l-dopa, and SIB-1553A, α4β4 nAChR agonist, on spatial delayed response task performance and reported that nicotine and SIB-1153A improved performance whereas l-dopa impaired (Decamp and Schneider 2009).
8.4 Neuroprotective Enhancement of nAChRs Through Four Pathways (Kawamata and Shimohama 2011)
-
1.
PI3K/AKT pathway
Our studies showed that nAChR stimulation protected neurons from Aβ-, glutamate-, rotenone-, and 6-OHDA-induced neurotoxicity. From the experimental data, our hypothesis for the mechanism of nAChR-mediated survival signal transduction is as follows: activation of α7 nAChRs stimulates the Src family, which in turn activates PI3K. PI3K phosphorylates AKT, which causes upregulation of Bcl-2 and Bcl-x. α4β2 nAChR stimulation also causes neuroprotection cascade without direct involvement of PI3K system.
-
2.
JAK2/STAT3 pathway
Other properties of nicotine proposed by other groups are anti-inflammatory potentials and modulating innate immune pathways mainly via α7 nAChR. Nicotine exerts its anti-inflammatory effect in activated immune cells, macrophages and microglia as well as neurons, by interacting α7 nAChR. Activated α7 nAChR binds directory to JAK2 and triggers the JAK2/STAT3 pathway to interfere with the activation of TLR-induced NF-κB, which is responsible for pro-inflammatory cytokine transcription (Cui and Li 2010).
-
3.
MEK/ERK pathway
Importance of the MEK/ERK pathway in nicotinic neuroprotection has also been emphasized by several groups (Buckingham et al. 2009; Wang et al. 2003). Dajas-Bailador et al. reported nicotine stimulation leads to PKA activation through α7 nAChR and further Raf-1/MEK/ERK signaling pathway (Dajas-Bailador et al. 2002). Other group showed that stepwise activation of Ras/Raf-1/MEK/ERK cascade provides for an increased cytoplasmic concentration of STAT3 due to an up-regulated expression (Arredondo et al. 2006) activating the JAK2/STAT3 pathway in human oral keratonocytes.
-
4.
Microglial CaM/CaMKII/Aβ phagocytosis pathway
In addition to known three neuroprotective pathways in neurons, we showed microglial Aβ clearance effect mediated through nAChRs enhancement should have special importance especially in AD therapy (Takata et al. 2010).
8.5 Conclusion
Targeting enhancement of nAChRs is one of the most practical therapeutic alternatives against AD to date. Based on epidemiological and experimental findings, clinical application of nicotinic enhancement against PD is also believed to be promising strategy different from ongoing dopamine replenish therapies. The underlying mechanisms of the neuroprotective effect induced by nicotinic stimulation were studied vigorously and three neuronal survival signal transductions have been elucidated as reviewed here. Recently microglial CaM/CaMKII/Aβ phagocytosis pathway is proved to be additional important neuroprotective pathway in AD models. Combined with other therapeutic methods under development, the enhancement of nAChRs would keep its position as safe and practical therapeutic alternatives against the progress of neurodegenerative disorders such as AD and PD.
References
Akaike A, Tamura Y, Yokota T, Shimohama S, Kimura J (1994) Nicotine-induced protection of cultured cortical neurons against N-methyl-D-aspartate receptor-mediated glutamate cytotoxicity. Brain Res 644:181–187
Akaike A, Takada-Takatori Y, Kume T, Izumi Y (2010) Mechanisms of neuroprotective effects of nicotine and acetylcholinesterase inhibitors: role of α4 and α7 receptors in neuroprotection. J Mol Neurosci 40:211–216
Arredondo J, Chernyavsky AI, Jolkovsky DL, Pinkerton KE, Grando SA (2006) Receptor-mediated tobacco toxicity: cooperation of the Ras/Raf-1/MEK1/ERK and JAK-2/STAT-3 pathways downstream of alpha7 nicotinic receptor in oral keratinocytes. FASEB J 20:2093–2101
Behmand RA, Harik SI (1992) Nicotine enhances 1-methyl-4-phenyl- 1,2,3,6- tetrahydropyridine neurotoxicity. J Neurochem 58:776–779
Betarbet R, Sherer TB, MacKenzie G, Garcia-Osuna M, Panov AV, Greenamyre JT (2000) Chronic systemic pesticide exposure reproduces features of Parkinson’s disease. Nat Neurosci 3:1301–1306
Bigl V, Woolf NJ, Butcher LL (1982) Cholinergic projections from the basal forebrain to frontal, parietal, temporal, occipital, and cingulate cortices: a combined fluorescent tracer and acetylcholinesterase analysis. Brain Res Bull 8:205–211
Bordia T, Parameswaran N, Fan H, Langston JW, McIntosh JM, Quik M (2006) Partial recovery of striatal nicotinic receptors in 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP)-lesioned monkeys with chronic oral nicotine. J Pharmacol Exp Ther 319:285–292
Bordia T, Grady SR, McIntosh JM, Quik M (2007) Nigrostriatal damage preferentially decreases a subpopulation of α6β2* nAChRs in mouse, monkey, and Parkinson’s disease striatum. Mol Pharmacol 72:52–61
Buckingham SD, Jones AK, Brown LA, Sattelle DB (2009) Nicotinic acetylcholine receptor signalling: roles in Alzheimer’s disease and amyloid neuroprotection. Pharmacol Rev 61:39–61
Champtiaux N, Gotti C, Cordero-Erausquin M, David DJ, Przybylski C, Léna C, Clementi F, Moretti M, Rossi FM, Le Novère N, McIntosh JM, Gardier AM, Changeux JP (2003) Subunit composition of functional nicotinic receptors in dopaminergic neurons investigated with knock-out mice. J Neurosci 23:7820–7829
Choi DW (1988) Calcium-mediated neurotoxicity: relationship to specific channel types and role in ischemic damage. Trends Neurosci 11:465–469
Citron M, Oltersdorf T, Haass C, McConlogue L, Hung AY, Seubert P, Vigo-Pelfrey C, Lieberburg I, Selkoe DJ (1992) Mutation of the β-amyloid precursor protein in familial Alzheimer’s disease increases β-protein production. Nature 360:672–674
Clarke PB, Schwartz RD, Paul SM, Pert CB, Pert A (1985) Nicotinic binding in rat brain: autoradiographic comparison of [3H]acetylcholine, [3H]nicotine, and [125I]-α-bungarotoxin. J Neurosci 5:1307–1315
Cormier A, Morin C, Zini R, Tillement J, Lagrue G (2003) Nicotine protects rat brain mitochondria against experimental injuries. Neuropharmacology 44:642–652
Costa G, Abin-Carriquiry JA, Dajas F (2001) Nicotine prevents striatal dopamine loss produced by 6-hydroxydopamine lesion in the substantia nigra. Brain Res 888:336–342
Court JA, Martin-Ruiz C, Graham A, Perry E (2000) Nicotinic receptors in human brain: topography and pathology. J Chem Neuroanat 20:281–298
Cui WY, Li MD (2010) Nicotinic modulation of innate immune pathways via α7 nicotinic acetylcholine receptor. J Neuroimmune Pharmacol 5:479–488
Dajas-Bailador FA, Soliakov L, Wonnacott S (2002) Nicotine activates the extracellular signal-regulated kinase 1/2 via the alpha7 nicotinic acetylcholine receptor and protein kinase A, in SH-SY5Y cells and hippocampal neurones. J Neurochem 80:520–530
Davis GC, Williams AC, Markey SP, Ebert MH, Caine ED, Reichert CM, Kopin IJ (1979) Chronic Parkinsonism secondary to intravenous injection of meperidine analogues. Psychiatry Res 1:249–254
Dawson VL, Dawson TM, London ED, Bredt DS, Snyder SH (1991) Nitric oxide mediates glutamate neurotoxicity in primary cortical cultures. Proc Natl Acad Sci U S A 88:6368–6371
De Fusco M, Becchetti A, Patrignani A, Annesi G, Gambardella A, Quattrone A, Ballabio A, Wanke E, Casari G (2000) The nicotinic receptor β2 subunit is mutant in nocturnal frontal lobe epilepsy. Nat Genet 26:275–276
De Reuck J, De Weweire M, Van Maele G, Santens P (2005) Comparison of age of onset and development of motor complications between smokers and non-smokers in Parkinson’s disease. J Neurol Sci 231:35–39
Decamp E, Schneider JS (2009) Interaction between nicotinic and dopaminergic therapies on cognition in a chronic Parkinson model. Brain Res 1262:109–114
del Peso L, Gonzalez-Garcia M, Page C, Herrera R, Nunez G (1997) Interleukin-3-induced phosphorylation of BAD through the protein kinase Akt. Science 278:687–689
Dineley KT, Xia X, Bui D, Sweatt JD, Zheng H (2002) Accelerated plaque accumulation, associative learning deficits, and up-regulation of α7 nicotinic receptor protein in transgenic mice co-expressing mutant human presenilin 1 and amyloid precursor proteins. J Biol Chem 277:22768–22780
Dorn HF (1959) Tobacco consumption and mortality from cancer and other diseases. Public Health Rep 74:581–593
Drenan RM, Grady SR, Whiteaker P, McClure-Begley T, McKinney S, Miwa JM, Bupp S, Heintz N, McIntosh JM, Bencherif M, Marks MJ, Lester HA (2008) In vivo activation of midbrain dopamine neurons via sensitized, high-affinity α6 nicotinic acetylcholine receptors. Neuron 60:123–136
Du F, Li R, Huang Y, Li X, Le W (2005) Dopamine D3 receptor-preferring agonists induce neurotrophic effects on mesencephalic dopamine neurons. Eur J Neurosci 22:2422–2430
Fujita M, Ichise M, Zoghbi SS, Liow JS, Ghose S, Vines DC, Sangare J, Lu JQ, Cropley VL, Iida H, Kim KM, Cohen RM, Bara-Jimenez W, Ravina B, Innis RB (2006) Widespread decrease of nicotinic acetylcholine receptors in Parkinson’s disease. Ann Neurol 59:174–177
Giannakopoulos P, Hof PR, Kövari E, Vallet PG, Herrmann FR, Bouras C (1996) Distinct patterns of neuronal loss and Alzheimer’s disease lesion distribution in elderly individuals older than 90 years. J Neuropathol Exp Neurol 55:1210–1220
Gotti C, Fornasari D, Clementi F (1997) Human neuronal nicotinic receptors. Prog Neurobiol 53:199–237
Grady SR, Salminen O, Laverty DC, Whiteaker P, McIntosh JM, Collins AC, Marks MJ (2007) The subtypes of nicotinic acetylcholine receptors on dopaminergic terminals of mouse striatum. Biochem Pharmacol 74:1235–1246
Guan ZZ, Nordberg A, Mousavi M, Rinne JO, Hellström-Lindahl E (2002) Selective changes in the levels of nicotinic acetylcholine receptor protein and of corresponding mRNA species in the brains of patients with Parkinson’s disease. Brain Res 956:358–366
Hardy J (2010) Genetic analysis of pathways to Parkinson disease. Neuron 68:201–206
Harris ME, Wang Y, Pedigo NWJ, Hensley K, Butterfield DA, Carney JM (1996) Amyloid β peptide (25–35) inhibits Na+-dependent glutamate uptake in rat hippocampal astrocyte cultures. J Neurochem 67:277–286
Hartley DM, Choi DW (1989) Delayed rescue of N-methyl-D-aspartate receptor-mediated neuronal injury in cortical culture. J Pharmacol Exp Ther 250:752–758
Huang LZ, Parameswaran N, Bordia T, Michael McIntosh J, Quik M (2009) Nicotine is neuroprotective when administered before but not after nigrostriatal damage in rats and monkeys. J Neurochem 109:826–837
Hunter BE, de Fiebre CM, Papke RL, Kem WR, Meyer EM (1994) A novel nicotinic agonist facilitates induction of long-term potentiation in the rat hippocampus. Neurosci Lett 168:130–134
Hwang J, Hwang H, Lee HW, Suk K (2010) Microglia signaling as a target of donepezil. Neuropharmacology 58:1122–1129
Inden M, Kitamura Y, Takeuchi H, Yanagida T, Takata K, Kobayashi Y, Taniguchi T, Yoshimoto K, Kaneko M, Okuma Y, Taira T, Ariga H, Shimohama S (2007) Neurodegeneration of mouse nigrostriatal dopaminergic system induced by repeated oral administration of rotenone is prevented by 4-phenylbutyrate, a chemical chaperone. J Neurochem 101:1491–1504
Inden M, Takata K, Yanagisawa D, Ashihara E, Tooyama I, Shimohama S, Kitamura Y (2016) α4 nicotinic acetylcholine receptor modulated by galantamine on nigrostriatal terminals regulates dopamine receptor-mediated rotational behavior. Neurochem Int 94:74–81
Iravani M, Haddon C, Cooper J, Jenner P, Schapira A (2006) Pramipexole protects against MPTP toxicity in non-human primates. J Neurochem 96:1315–1321
Janson AM, Fuxe K, Goldstein M (1992) Differential effects of acute and chronic nicotine treatment on MPTP-(1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) induced degeneration of nigrostriatal dopamine neurons in the black mouse. Clin Investig 70:232–238
Jensen M, Schröder J, Blomberg M, Engvall B, Pantel J, Ida N, Basun H, Wahlund LO, Werle E, Jauss M, Beyreuther K, Lannfelt L, Hartmann T (1999) Cerebrospinal fluid Aβ42 is increased early in sporadic Alzheimer’s disease and declines with disease progression. Ann Neurol 45:504–511
Jeyarasasingam G, Tompkins L, Quik M (2002) Stimulation of non-α7 nicotinic receptors partially protects dopaminergic neurons from 1-methyl-4-phenylpyridinium-induced toxicity in culture. Neuroscience 109:275–285
Junyent F, Alvira D, Yeste-Velasco M, de la Torre AV, Beas-Zarate C, Sureda FX, Folch J, Pallàs M, Camins A, Verdaguer E (2010) Prosurvival role of JAK/STAT and Akt signaling pathways in MPP+-induced apoptosis in neurons. Neurochem Int 57:774–782
Kaneko S, Maeda T, Kume T, Kochiyama H, Akaike A, Shimohama S, Kimura J (1997) Nicotine protects cultured cortical neurons against glutamate-induced cytotoxicity via α7-neuronal receptors and neuronal CNS receptors. Brain Res 765:135–140
Kawamata J, Shimohama S (2002) Association of novel and established polymorphisms in neuronal nicotinic acetylcholine receptors with sporadic Alzheimer’s disease. J Alzheimers Dis 4:71–76
Kawamata J, Shimohama S (2011) Stimulating nicotinic receptors trigger multiple pathways attenuating cytotoxicity in models of Alzheimer’s and Parkinson’s diseases. J Alzheimers Dis 24(Suppl 2):95–109
Kihara T, Shimohama S, Sawada H, Kimura J, Kume T, Kochiyama H, Maeda T, Akaike A (1997) Nicotinic receptor stimulation protects neurons against β-amyloid toxicity. Ann Neurol 42:159–163
Kihara T, Shimohama S, Urushitani M, Sawada H, Kimura J, Kume T, Maeda T, Akaike A (1998) Stimulation of α4β2 nicotinic acetylcholine receptors inhibits β-amyloid toxicity. Brain Res 792:331–334
Kihara T, Shimohama S, Honda K, Shibasaki H, Akaike A (2000) Neuroprotective effect of nicotinic agonists via PI3 kinase cascade against glutamate cytotoxicity enhanced by β amyloid. Neurology 54(Suppl 3):A367
Kihara T, Shimohama S, Sawada H, Honda K, Nakamizo T, Shibasaki H, Kume T, Akaike A (2001) α7 nicotinic receptor transduces signals to phosphatidylinositol 3-kinase to block A β-amyloid-induced neurotoxicity. J Biol Chem 276:13541–13546
Kihara T, Sawada H, Nakamizo T, Kanki R, Yamashita H, Maelicke A, Shimohama S (2004) Galantamine modulates nicotinic receptor and blocks Aβ-enhanced glutamate toxicity. Biochem Biophys Res Commun 325:976–982
Langston JW, Ballard P, Tetrud JW, Irwin I (1983) Chronic Parkinsonism in humans due to a product of meperidine-analog synthesis. Science 219:979–980
Le Novère N, Zoli M, Changeux JP (1996) Neuronal nicotinic receptor α 6 subunit mRNA is selectively concentrated in catecholaminergic nuclei of the rat brain. Eur J Neurosci 8:2428–2439
Lindstrom J, Anand R, Peng X, Gerzanich V, Wang F, Li Y (1995) Neuronal nicotinic receptor subtypes. Ann N Y Acad Sci 757:100–116
Maelicke A, Samochocki M, Jostock R, Fehrenbacher A, Ludwig J, Albuquerque EX, Zerlin M (2001) Allosteric sensitization of nicotinic receptors by galantamine, a new treatment strategy for Alzheimer’s disease. Biol Psychiatry 49:279–288
Mann V, Cooper J, Krige D, Daniel S, Schapira A, Marsden C (1992) Brain, skeletal muscle and platelet homogenate mitochondrial function in Parkinson’s disease. Brain 115(Pt. 2):333–342
Maragos WF, Greenamyre JT, Penney JB, Young AB (1986) Glutamate dysfunction in Alzheimer’s disease: an hypothesis. Trends Neurosci 10:65–68
Matsumura A, Suzuki S, Iwahara N, Hisahara S, Kawamata J, Suzuki H, Yamauchi A, Takata K, Kitamura Y, Shimohama S (2015) Temporal changes of CD68 and α7 nicotinic acetylcholine receptor expression in microglia in Alzheimer’s disease-like mouse models. J Alzheimers Dis 44:409–423
Matsuzaki H, Tamatani M, Mitsuda N, Namikawa K, Kiyama H, Miyake S, Tohyama M (1999) Activation of Akt kinase inhibits apoptosis and changes in Bcl-2 and Bax expression induced by nitric oxide in primary hippocampal neurons. J Neurochem 73:2037–2046
Mattson MP (1988) Neurotransmitters in the regulation of neuronal cytoarchitecture. Brain Res Rev 13:179–212
Meldrum B, Garthwaite J (1990) Excitatory amino acid neurotoxicity and neurodegenerative disease. Trends Pharmacol Sci 11:379–387
Mesulam MM, Mufson EJ, Levey AI, Wainer BH (1983) Cholinergic innervation of cortex by the basal forebrain: cytochemistry and cortical connections of the septal area, diagonal band nuclei, nucleus basalis (substantia innominata) and hypothalamus in the rhesus monkey. J Comp Neurol 214:170–197
Meyer EM, Tay ET, Papke RL, Meyers C, Huang GL, de Fiebre CM (1997) 3-[2,4-Dimethoxybenzylidene]anabaseine (DMXB) selectively activates rat α7 receptors and improves memory-related behaviors in a mecamylamine-sensitive manner. Brain Res 768:49–56
Mizuno Y, Yoshino H, Ikebe S, Hattori N, Kobayashi T, Shimoda-Matsubayashi S, Matsumine H, Kondo T (1998) Mitochondrial dysfunction in Parkinson’s disease. Ann Neurol 44(3 Suppl 1):S99–S109
Morens D, Grandinetti A, Reed D, White L, Ross G (1995) Cigarette smoking and protection from Parkinson’s disease: false association or etiologic clue? Neurology 45:1041–1051
Obeso JA, Rodriguez-Oroz MC, Goetz CG, Marin C, Kordower JH, Rodriguez M, Hirsch EC, Farrer M, Schapira AH, Halliday G (2010) Missing pieces in the Parkinson’s disease puzzle. Nat Med 16:653–661
Parain K, Marchand V, Dumery B, Hirsch E (2001) Nicotine, but not cotinine, partially protects dopaminergic neurons against MPTP-induced degeneration in mice. Brain Res 890:347–350
Parain K, Hapdey C, Rousselet E, Marchand V, Dumery B, Hirsch EC (2003) Cigarette smoke and nicotine protect dopaminergic neurons against the 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine Parkinsonian toxin. Brain Res 984:224–232
Parker W Jr, Boyson S, Parks J (1989) Abnormalities of the electron transport chain in idiopathic Parkinson’s disease. Ann Neurol 26:719–723
Quik M (2004) Smoking, nicotine and Parkinson’s disease. Trends Neurosci 27:561–568
Quik M, Chen L, Parameswaran N, Xie X, Langston J, McCallum SE (2006a) Chronic oral nicotine normalizes dopaminergic function and synaptic plasticity in 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine-lesioned primates. J Neurosci 26:4681–4689
Quik M, Parameswaran N, McCallum SE, Bordia T, Bao S, McCormack A, Kim A, Tyndale RF, Langston JW, Di Monte DA (2006b) Chronic oral nicotine treatment protects against striatal degeneration in MPTP-treated primates. J Neurochem 98:1866–1875
Raskind MA, Peskind ER, Truyen L, Kershaw P, Damaraju CV (2004) The cognitive benefits of galantamine are sustained for at least 36 months: a long-term extension trial. Arch Neurol 61:252–256
Ravenstijn PG, Merlini M, Hameetman M, Murray TK, Ward MA, Lewis H, Ball G, Mottart C, de Ville de Goyet C, Lemarchand T, van Belle K, O’Neill MJ, Danhof M, de Lange EC (2008) The exploration of rotenone as a toxin for inducing Parkinson’s disease in rats, for application in BBB transport and PK-PD experiments. J Pharmacol Toxicol Methods 57:114–130
Rosser MN, Svendsen C, Hunt SP, Mounjoy CQ, Roth M, Iversen LL (1982) The substantia innominata in Alzheimer’s disease: a histochemical and biochemical study of cholinergic marker enzymes. Neurosci Lett 28:217–222
Schmidt WJ, Alam M (2006) Controversies on new animal models of Parkinson’s disease pro and con: the rotenone model of Parkinson’s disease (PD). J Neural Transm Suppl 70:273–276
Shen H, Kihara T, Hongo H, Wu X, Kem WR, Shimohama S, Akaike A, Niidome T, Sugimoto H (2010) Neuroprotection by donepezil against glutamate excitotoxicity involves stimulation of α7 nicotinic receptors and internalization of NMDA receptors. Br J Pharmacol 161:127–139
Shimohama S (2009) Nicotinic receptor-mediated neuroprotection in neurodegenerative disease models. Biol Pharm Bull 32:332–336
Shimohama S, Taniguchi T, Fujiwara M, Kameyama M (1986) Changes in nicotinic and muscarinic cholinergic receptors in Alzheimer-type dementia. J Neurochem 46:288–293
Shimohama S, Akaike A, Kimura J (1996) Nicotine-induced protection against glutamate cytotoxicity. Nicotinic cholinergic receptor-mediated inhibition of nitric oxide formation. Ann N Y Acad Sci 777:356–361
Shimohama S, Greenwald DL, Shafron DH, Akaika A, Maeda T, Kaneko S, Kimura J, Simpkins CE, Day AL, Meyer EM (1998) Nicotinic α7 receptors protect against glutamate neurotoxicity and neuronal ischemic damage. Brain Res 779:359–363
Shimohama S, Sawada H, Kitamura Y, Taniguchi T (2003) Disease model: Parkinson’s disease. Trends Mol Med 9:360–365
Sidransky E, Nalls MA, Aasly JO, Aharon-Peretz J, Annesi G, Barbosa ER, Bar-Shira A, Berg D, Bras J, Brice A, Chen CM, Clark LN, Condroyer C, De Marco EV, Dürr A, Eblan MJ, Fahn S, Farrer MJ, Fung HC, Gan-Or Z, Gasser T, Gershoni-Baruch R, Giladi N, Griffith A, Gurevich T, Januario C, Kropp P, Lang AE, Lee-Chen GJ, Lesage S, Marder K, Mata IF, Mirelman A, Mitsui J, Mizuta I, Nicoletti G, Oliveira C, Ottman R, Orr-Urtreger A, Pereira LV, Quattrone A, Rogaeva E, Rolfs A, Rosenbaum H, Rozenberg R, Samii A, Samaddar T, Schulte C, Sharma M, Singleton A, Spitz M, Tan EK, Tayebi N, Toda T, Troiano AR, Tsuji S, Wittstock M, Wolfsberg TG, Wu YR, Zabetian CP, Zhao Y, Ziegler SG (2009) Multicenter analysis of glucocerebrosidase mutations in Parkinson’s disease. N Engl J Med 361:1651–1661
Steinlein OK, Mulley JC, Propping P, Wallace RH, Phillips HA, Sutherland GR, Scheffer IE, Berkovic SF (1995) A missense mutation in the neuronal nicotinic acetylcholine receptor α4 subunit is associated with autosomal dominant nocturnal frontal lobe epilepsy. Nat Genet 11:201–203
Suzuki S, Kawamata J, Matsushita T, Matsumura A, Hisahara S, Takata K, Kitamura Y, Kem W, Shimohama S (2013) 3-[(2,4-Dimethoxy)benzylidene]-anabaseine dihydrochloride protects against 6-hydroxydopamine-induced parkinsonian neurodegeneration through α7 nicotinic acetylcholine receptor stimulation in rats. J Neurosci Res 91:462–471
Takata K, Kitamura Y, Saeki M, Terada M, Kagitani S, Kitamura R, Fujikawa Y, Maelicke A, Tomimoto H, Taniguchi T, Shimohama S (2010) Galantamine-induced amyloid-β clearance mediated via stimulation of microglial nicotinic acetylcholine receptors. J Biol Chem 285:40180–40191
Takeuchi H, Yanagida T, Inden M, Takata K, Kitamura Y, Yamakawa K, Sawada H, Izumi Y, Yamamoto N, Kihara T, Uemura K, Inoue H, Taniguchi T, Akaike A, Takahashi R, Shimohama S (2009) Nicotinic receptor stimulation protects nigral dopaminergic neurons in rotenone-induced Parkinson’s disease models. J Neurosci Res 87:576–585
Tomita T, Maruyama K, Saido TC, Kume H, Shinozaki K, Tokuhiro S, Capell A, Walter J, Grünberg J, Haass C, Iwatsubo T, Obata K (1997) The presenilin 2 mutation (N141I) linked to familial Alzheimer disease (Volga German families) increases the secretion of amyloid β protein ending at the 42nd (or 43rd) residue. Proc Natl Acad Sci U S A 94:2025–2030
Ungerstedt U (1971) Postsynaptic supersensitivity after 6-hydroxy-dopamine induced degeneration of the nigro-striatal dopamine system. Acta Physiol Scand 367(Suppl):69–93
Villafane G, Cesaro P, Rialland A, Baloul S, Azimi S, Bourdet C, Le Houezec J, Macquin-Mavier I, Maison P (2007) Chronic high dose transdermal nicotine in Parkinson’s disease: an open trial. Eur J Neurol 12:1313–1316
Wang HY, Lee DH, D’Andrea MR, Peterson PA, Shank RP, Reitz AB (2000) β-Amyloid(1-42) binds to α7 nicotinic acetylcholine receptor with high affinity. Implications for Alzheimer’s disease pathology. J Biol Chem 275:5626–5632
Wang HY, Li W, Benedetti NJ, Lee DH (2003) α7 nicotinic acetylcholine receptors mediate β-amyloid peptide-induced tau protein phosphorylation. J Biol Chem 278:31547–31553
Whitehouse PJ, Kalaria RN (1995) Nicotinic receptors and neurodegenerative dementing diseases: basic research and clinical implications. Alzheimer Dis Assoc Disord 9:3–5
Whitehouse PJ, Price DL, Clark AW, Coyle TT, Delong M (1981) Alzheimer’s disease: evidence for a selective loss of cholinergic neurons in the nucleus basalis. Ann Neurol 10:122–126
Wirdefeldt K, Gatz M, Pawitan Y, Pedersen N (2005) Risk and protective factors for Parkinson’s disease: a study in Swedish twins. Ann Neurol 57:27–33
Xie Y, Bezard E, Zhao B (2005) Investigating the receptor-independent neuroprotective mechanisms of nicotine in mitochondria. J Biol Chem 280:32405–32412
Yanagida T, Takeuchi H, Kitamura Y, Takata K, Minamino H, Shibaike T, Tsushima J, Kishimoto K, Yasui H, Taniguchi T, Shimohama S (2008) Synergistic effect of galantamine on nicotine-induced neuroprotection in hemiparkinsonian rat model. Neurosci Res 62:254–261
Yankner BA, Duffy LK, Kirschner DA (1990) Neurotrophic and neurotoxic effects of amyloid β protein: reversal by tachykinin neuropeptides. Science 250:279–282
Zhong LT, Kane DJ, Bredesen DE (1993) BCL-2 blocks glutamate toxicity in neural cell lines. Mol Brain Res 19:353–355
Acknowledgements
This work was supported in part by the Japan Society for the Promotion of Science (JSPS) KAKENHI Grant Number 15K09840 (J.K.) and 16H05279 (S.S.), the Orange–MCI from the Japan Agency for Medical Research and Development (AMED)(S.S.), and the Smoking Research Foundation (No. 1503837, S.S.).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
This chapter is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
Copyright information
© 2018 The Author(s)
About this chapter

Cite this chapter
Shimohama, S., Kawamata, J. (2018). Roles of Nicotinic Acetylcholine Receptors in the Pathology and Treatment of Alzheimer’s and Parkinson’s Diseases. In: Akaike, A., Shimohama, S., Misu, Y. (eds) Nicotinic Acetylcholine Receptor Signaling in Neuroprotection. Springer, Singapore. https://doi.org/10.1007/978-981-10-8488-1_8
Download citation
DOI: https://doi.org/10.1007/978-981-10-8488-1_8
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-8487-4
Online ISBN: 978-981-10-8488-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)