
Abstract
Field epidemiology has become a major principle in public health and animal health service. Field epidemiologists are the primary group of professionals responding to outbreaks and other health emergencies who provide evidence-based recommendations for decision makers. In outbreak investigations, their duties are to identify the disease etiology, risk factors or source of an outbreak, and to contain the spread of the disease. Field epidemiology training programs (FETP) recruit professionals with training in medical, veterinary medical and other related health sciences to deal with real-life outbreaks and health problems. Joint training in surveillance and outbreak investigation has led to improved surveillance and control of zoonotic diseases by young professionals from human health and animal health sectors. Field epidemiology training programs for veterinarians (FETPV) is a living branch of a mature FETP which could support the development of wildlife and ecosystem needs under a broad One Health canopy. FETP can be a practical means of actualizing the One Health approach based upon shared needs and mutual benefit. One such model for sustainable, joint capacity development in field epidemiology under a One Health approach has been initiated in Thailand and is being adopted in other Asian countries. The Field Epidemiology Training Network of FETP in Southeast Asia is a useful platform for further strengthening regional disease surveillance and improving response to both public and animal health problems of international concern.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
1 Needs for Field Epidemiologists and Field Epidemiology Training
1.1 Function and Role of the Field Epidemiologist
In many public health emergencies, effective prevention and control of health threats requires appropriate response by health professionals who have been trained in field epidemiology. Prompt investigation and proper response to major disease outbreaks by a team of field epidemiologists can minimize negative impacts on the health and economies of affected populations. Outbreak investigation is commonly recognized as an important function of field epidemiologists who work in a variety of field settings in different countries. Outbreaks of communicable and non-communicable diseases can occur in various settings ranging from a big city or rural town to a sophisticated healthcare facility (Ungchusak and Iamsirithaworn 2009). During outbreak events, field epidemiologists work closely with health professionals from different disciplines to gather relevant information from patients, family members, close contacts and residents of the affected area. Common challenges to field epidemiologists include working with data sources that are incomplete and using investigation protocols that are not well planned (Goodman and Buehler 2008). The nature of the work of field epidemiologists demands a timely response and travel to the field site which can sometimes require difficult access to remote areas, in order to solve the problem. The extent of the investigation is often limited because of the need for timely intervention as well as situational constraints on study methods.
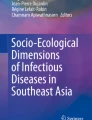
During public health crises (e.g., major outbreaks or events of illness with unexpected deaths), field epidemiologists are usually the first group of professionals deployed to investigate the outbreaks and initiate control measures to protect at-risk populations. The primary function of field epidemiologists is to use findings obtained from an investigation to define the disease etiology, to identify the possible source(s) of an outbreak, and risk factors in order to contain its spread, and to implement prevention and control measures. Key objectives of the investigation generally include creating a case definition, implementing methods for case-finding, and establishing the occurrence of cases by time, place, and attributes of the affected population including, gender and age. The data generated are used to formulate hypotheses regarding etiology, mode of transmission, and other key facets of the disease. An important aspect of the investigation is the collection of samples from patients, the environment, and other sources for diagnostic tests and other laboratory investigations. An investigation of a foodborne Streptococcal suis outbreak attributable to consumption of fresh pig blood is an example of field epidemiologists identifying an implicated food item in this zoonotic disease outbreak (Khadthasrima et al 2008). The associated epidemic curve shows a pattern of common point source outbreak following a funeral banquet in Thailand in 2007 (Fig. 9.1). Roughly 75 % of recently emerging diseases and 60 % of human pathogens are zoonoses, outbreak response required coordinated and field investigations (U.S. CDC 2013). Therefore harmonized, yet adapted approaches for field investigation are essential components of a holistic approach to understand, prevent and control zoonoses in a comprehensive manner.

Epidemic curve of of S. suis infections (N = 49*) in Phu Sang District, Phayao Province, Thailand, April to May 2007
Surveillance is a major epidemiological intelligence tool and serves as the brain of health authorities and workers. Effective surveillance systems provide timely information to guide appropriate interventions for solving health problems. Field epidemiologists are often the key persons in establishing and maintaining surveillance systems since they design the system as well as collecting, analyzing, interpreting and sharing surveillance information with stakeholders for necessary action. Regular evaluations of surveillance systems by epidemiologists are necessary for quality improvement and ensuring utilization of the surveillance information.
In recent decades, the principle of field epidemiology has become increasingly applied to studying and solving complex chronic health threats, e.g., cancer in humans as well as both animal production (health) and disease. Field epidemiologists play a role in conducting field studies to identify causes and risk factors for the diseases, then select, design and implement appropriate intervention(s) to tackle the problems. Furthermore, field epidemiologists get involved with many interventional studies that are often carried out in the field setting to test the effectiveness of health interventions.
1.2 Concept of Field Epidemiology Training
In 1951, a pioneer training program for field epidemiology was first established in the USA (Gregg 2008). The U.S. Centers for Disease Control and Prevention (CDC) program, Epidemic Intelligence Service or EIS, is the first model that has been progressively adopted by many countries around the world. The EIS program aims to produce competent epidemiologists to combat infectious diseases and to mitigate the non-communicable disease burden in communities. The program has trained nearly 3,000 professionals in this discipline and assisted other nations to establish a number of field-based training programs. Since its onset, the US CDC’s EIS program included primarily physicians but also recruited a variety of other health professionals such as statisticians, sanitary engineers, microbiologists, and veterinarians.
The term “Field Epidemiology Training Program: FETP” was first used by the Thai FETP at the time of its establishment in 1980. In the first two decades of the program, only young medical doctors (physicians) who were dedicated and enthusiastic to pursue their career in public health and epidemiology service were enrolled into the field-based training program. Beginning in 2005, veterinarians were regularly recruited through close collaboration between human health and animal health sectors including a formal memorandum of understanding signed by both the Ministries of Public Health and of Agriculture and Cooperatives in 2008.
In most countries, field epidemiology training courses are specifically designed for health professionals as applied post-graduation education. Graduates with a background in medicine, veterinary medicine or other health sciences are recruited and enrolled into a 2-year, non-degree program. Some programs closely collaborate with universities or academic institutes as a part of a joint diploma-degree program. In Thailand, the curriculum of FETP is incorporated as a part of the 3-year residency training for human medical doctors who aim to build their expertise in preventive medicine and epidemiology. As a second component of the residency training, physicians pursue a Master’s of Public Health (MPH) degree in universities of their choice. This 1-year graduate degree provides broad knowledge for working in public health. On-the-job, in-service training in applied epidemiology provides trainees opportunities to learn from actual disease outbreaks and direct experience in responding to important health problems. Close supervision by mentors and learning through providing service are essential features and important challenges of delivering field epidemiology training.
FETP has a unique curriculum that intends to provide opportunities for trainees to learn epidemiology while they provide public health services. Transferable skills and competencies are built which improve the level of government services required to meet the challenges of emerging infectious diseases (EID) (TEPHINET 2013). Trainees learn how to conduct an outbreak investigation starting from verifying its existence, then organizing and traveling to the field to collect, manage and analyze data and interpret the findings in order to provide relevant recommendations. Most FETP curricula are designed for 2-year training though some are shorter (6 months to 1 year) and are referred to as field epidemiology training (FET). Trainees learn basic concepts of epidemiology and biostatistics and how to conduct field surveys and surveillance. In addition they also develop basic skills related to laboratory diagnosis, communication and outbreak management. Major requirements for graduation in most FETPs include an evaluation of a surveillance system, conducting outbreak investigations and epidemiologic field research.
In general, FETPs are based in ministries of health where trainees can legally access surveillance data and participate in outbreak response with no delay and with full legal authority. It should be noted that formal education in epidemiology has existed in a variety of Master’s degree programs for decades but field-based practice involving real-life outbreak investigation is less emphasized in the universities due to time constraints, difficult field management and a limited mandate to deliver public health service. In contrast, the on-the-job epidemiology training provides trainees opportunities to learn from field practice. During the 2-year, in-service training in field epidemiology, the trainees’ time spent conducting field work activities is placed at the highest priority and accounts for 70 % or more of their time. The remaining time allocation is for non-field activities, such as didactic teaching and workshops. This training strategy has proven to be successful in producing competent field epidemiologists for effective response to disease outbreaks and other public health challenges.
As of June 2013, 55 training programs in field epidemiology have been developed around the world (TEPHINET 2013) and the FETPs can address the needs for capable epidemiologists in health service and to meet a requirement of the International Health Regulations 2005 by building surveillance and response capacity in the country.
1.3 Development of Field Epidemiology Training in Thailand and Southeast Asia
The Field Epidemiology Training Program (FETP) in Thailand was initiated following a demand by health authorities for competent field epidemiologists who can effectively respond to acute health problems in a timely manner. The Thai program is the first field-based epidemiology training outside the American continent that was modelled after the EIS in the U.S. (Malison et al 1989). The curriculum of the Thai FETP was jointly developed by a collaborative effort of the Thai Ministry of Public Health (MoPH), the World Health Organization (WHO) and the U.S. CDC. The first cohort of trainees consisted of five medical doctors who began on-the-job training in June 1980. The label “FETP” has been recognized as applied epidemiology training that is directly linked to providing public health services including the surveillance and outbreak investigation mandates of the MoPH. An international training course was established in 1998 under FETP-Thailand with the goal of addressing needs for capable field epidemiologists in controlling public health problems in Asian countries that include Bhutan, Cambodia, China, Lao PDR, Malaysia, Myanmar and Vietnam.
The philosophy of Thai FETP is “Learning through Providing Services”. The Thai FETP recruits young medical doctors with high interest in public health into the 2-year in-service training at the Bureau of Epidemiology in the MoPH. Trainees develop competence in operating surveillance systems by analyzing and interpreting the data and disseminating key information to support policy decisions. They also have opportunities to conduct a surveillance system evaluation or become involved with establishment of a new surveillance system. Each trainee investigates at least three outbreaks as a principal investigator and reports major findings and recommendations to local authorities and relevant policy makers. One of the requirements, an epidemiologic study, is carefully carried out to understand priority health issues and disease epidemiology, and to solve those health problems. In situations of health emergencies, FETP trainees are the front line investigators in the field. Close supervision by well-trained mentors, the majority of whom are FETP graduates, is a vital component of the successful field training.
As of June 2013, the program has graduated over 200 field epidemiologists to serve in various public health programs. Approximately 70 % of graduates have served in the MoPH by providing epidemiological services at national and local levels. Others graduates work in universities, military service and international organizations including WHO, US CDC and United Nations Populations Fund (UNFPA).
During the first decade of FETP-Thailand in 1980s, infectious diseases were major health challenges. Trainees and mentors worked with responsible agencies to control the public health problems through outbreak investigation and providing recommendations for improving vaccination strategies in the Expanded Program on Immunization. In the early 1990s, the Human immunodeficiency virus infection/acquired immunodeficiency syndrome (HIV/AIDS) epidemic provided another opportunity for the Thai FETP to demonstrate its usefulness. Trainees and graduates from FETP assisted in investigating the first 100 AIDS cases in the country and revealed epidemics among drug users and sex workers. The FETP graduates played a key role in establishing a sentinel surveillance system to monitor the HIV prevalence and risk behaviours among target populations (Weniger et al 1991). A famous intervention called “100 % Condom Use Program” was initiated and advocated and implemented by a program graduate. This program resulted in slowing down the HIV epidemic in Thailand (Rojanapithayakorn and Hanenberg 1996).
With a demonstration of the prominent 2-year field epidemiology training, a policy to establish and train 1,030 “Surveillance and Rapid Response Teams”, so called SRRTs to cover all districts in Thailand was initiated following the emergence of the global severe acute respiratory syndrome (SARS) epidemic and outbreaks of Highly Pathogenic Avian Influenza (HPAI) H5N1 in Southeast Asia including Thailand in the early 2000s. SRRTs provide timely surveillance and are an effective response mechanism for containment of the epidemics. Thai FETP was asked to design a curriculum and training materials for medical doctors and other health professionals working at the district level. Each SRRT has approximately five members each of whom was trained for 6 months in surveillance and outbreak investigation, under supervision of more experienced epidemiology officers at the provincial level (Fig. 9.2). In recent years, a short course for basic epidemiology and event-based surveillance was developed for training personnel in communities including public health and animal health volunteers under the One Health approach.

Target of Field Epidemiology Training in Thailand
In 1998, a new track for training of international participants was established under FETP-Thailand. On average, two to three trainees from Southeast Asian nations are enrolled into the 2-year program. After an 8-week introductory training module of basic epidemiology and biostatistics in classroom and field studies, the trainees perform actual surveillance studies and outbreak investigations in their home countries under the supervision of a local advisor. Every 6-months, they return to the training center in Thailand to work with their program advisor to share their work and experiences with colleagues from other countries. By 2013, the cumulative number of international graduates was 39. In late 2011, a network of field epidemiology training programs, “ASEAN+3 Field Epidemiology Training Network: ASEAN+3 FETN” was formed to strengthen field epidemiology training capacity in ten Asian countries plus China, Japan and Republic of Korea.
2 Establishment of FETPV in Thailand: A Collaboration Between Human and Animal Health Sections Through an Applied Field-Based Training Model
2.1 The Demand for Joint Field Epidemiology Capacity in Thailand
In Thailand, animal zoonoses control and prevention is mainly the responsibility of the Department of Livestock Development (DLD), Ministry of Agriculture and Cooperatives while the human zoonoses control and prevention task is under the authority of the Department of Disease Control (DDC), Ministry of Public Health. Effective response to zoonoses needs close collaboration, at least, between these two organizations. Many zoonotic diseases are notifiable diseases required for the surveillance system under the responsibility of DDC, i.e., rabies, leptospirosis, anthrax, influenza, trichinosis, Japanese encephalitis and streptococcosis caused by Streptococcus suis. However, the most effective approach to fight against these zoonoses is timely control at their origin. Thus, DLD and DDC have worked collaboratively to tackle those important zoonoses for decades.
Human resource development, especially capacity building for field epidemiologists, is an essential component of preparedness and response for emerging, re-emerging and endemic infectious zoonotic diseases under the concept of “One Health”. In Thailand, the evidence shows that animal health and human health sectors working closely together can effectively control many important zoonotic diseases. For example, during the avian Influenza crisis in Thailand between 2004 and 2006, staff from DLD and DDC joined hands to fight against this emerging disease and successfully controlled its spread in the country.
Considering differences in human resources, infrastructure, expertise and mandate, collaboration in the area of joint human capacity development has begun in 2005. The Ministry of Public Health FETP recruited two veterinarians from DLD into the 2-year training program at the Bureau of Epidemiology, DDC, Ministry of Public Health. Since then, FETP has recruited one to two veterinarians annually to participate in the FETP. It has been demonstrated that the collaboration results in improved response to zoonoses as well as creating a working network between public health and animal health sectors. Thus, DLD and DDC agreed to strengthen the collaboration by the signing of a Memorandum of Understanding in January 2008 with the goal to produce 30 veterinary epidemiologists for DLD within the next 10 years. Graduate veterinary epidemiologists are now core persons responsible for human capacity development in DLD and strengthening networks from central to local levels.
2.2 Development of FETPV
The Field Epidemiology Training Program for Veterinarians (FETPV) curriculum was developed under close consultation with FETP faculty and veterinary experts from DLD, universities and FAO for the most effective application of the FETP concept, “Learning through Providing Services”. Thai veterinarians and physicians are trained and work together to respond to any possible zoonotic disease outbreaks, thereby contributing to the public health sector mandate. The program aims not only to strengthen capacity of animal health personnel but also to promote self-sufficiency and multi-disciplinary response capacity for animal diseases that improves technical services for DLD.
In the first year of the training program, FETPV trainees are assigned for health situation analysis and outbreak investigation and they are focused equally on exclusive animal diseases and zoonotic diseases. This approach ensures that the animal health situation will be analyzed and critiqued for a better understanding it and improvement of the surveillance system. Trainees are expected to generate hypotheses and research questions to identify gaps in the response system through health situation analysis and outbreak investigation assignments in the first year of the program. A field epidemiological study is developed during the second year of the training program to further assess and provide recommendations to fill gaps identified previously.
The program shares financial and technical resources among partners, particularly DLD and DDC in order to train veterinarians. Trainees spend 30 % of the time in formal classroom training and 70 % of the time conducting field work to fulfil the requirements for graduation. During the 2-year training program, veterinarians participate in various short training courses and workshops such as basic epidemiology and biostatistics, field surveillance and outbreak demonstration and basic computer software and laboratory workshops to ensure that trainees are competent to carry out field epidemiological activities. Some of these short training courses and workshops are organized in conjunction with the regional aspect of FETPV and the animal health professional development programs of DLD. A summary of the FETPV curriculum is shown in Table 9.1.
During the training course, veterinarians and physicians have a chance to share their experiences and expertise and work collaboratively to solve animal and human health problems. Veterinarians and physicians in the program are trained to understand both animal and public health service systems. Since the beginning of FETPV, a number of collaborative health situation analyses, outbreak responses and field epidemiological studies of both human and animal health problems have been conducted. These include human leptospirosis, human streptococcosis caused by S. suis type 2 from pigs, human and animal brucellosis caused by Brucella melitensis and B. suis, human and animal rabies, Porcine Reproductive and Respiratory Syndrome (PRRS) in pigs, zoonotic Influenza A in humans and animals, and Methicillin-resistant Staphylococcus aureus (MRSA) in pigs and farm workers.
It has been 8 years since veterinarians joined the FETP—tangible proof of the program sustainability and commitment from both DLD and DDC. As of June 2013, a total of 13 Thai veterinarians graduated from the program. Further, as trainees have graduated and returned to their own organizations, several animal and public health collaboration activities have been initiated by an alumni network at the local and central level. These include joint field investigations, and joint surveillance database programs for avian influenza and rabies. Our experience with FETPV development reinforces the concept that effective response to zoonoses and emerging animal-health related problems requires a broad range of competencies from various disciplines.
3 Collaboration Between Human and Animal Health Sectors at Regional Level
3.1 The Challenge
The emergence and spread of Nipah virus, SARS and highly pathogenic avian influenza (HPAI) H5N1 subtype in Asia since 2004 provided a stress test of both country and regional capacity to deal with emerging infectious diseases (EIDs) and transboundary animal diseases (TADs). Common constraints were identified in addressing an emerging zoonosis including the lack of resources and the difficulties in establishing a seamless interaction among human health, animal health and environmental health agencies (Schelling et al. 2005). In order to fully support a One Health approach to zoonoses, it was evident that the veterinary health infrastructure needed to be strengthened in order to deal with EIDs which will continue to pose a significant threat to human, animal and environmental health, food security, livelihoods, sustainability of food production systems and the economies of developing countries (FAO 2011).
3.2 The Response
A regional needs assessment was conducted in nine countries from Southeast Asia between May and August 2008 to establish a baseline measurement of veterinary epidemiology capacity. It included a semi-structured interview and questionnaire and a gap analysis of 32 skills related to field epidemiology for veterinarians (FAO 2008b). Stakeholders from animal health and public health sectors at national, regional and international agencies in each country were interviewed over several days to assess capacity development needs for veterinarians working to fulfil the mandates to address TADs and zoonotic diseases in the region.
The needs assessment revealed that the level of cooperation between animal and human health sectors among countries in the region varied greatly and was generally limited. In 2008, eight of nine countries surveyed had established cooperative relationships in dealing with zoonotic diseases, however in 2013 all countries have established cooperative relationships related to zoonoses. In general, the lead agency for H5N1 was designated according to the species first affected, related to whether the index species was human or animal. The needs assessment in 2008 also revealed that joint surveillance rapid response teams (SRRTs) existed only in Thailand. Similar efforts to build SRRTs in China and Bangladesh as well as several other countries in the region are now underway.
Most notably, epidemiologists from both human and animal health agencies favored joint training of human medical and veterinary medical staff in applied field epidemiology training programs such as FETP and FETPV. Joint training was considered as a practical way to establish trust and working relationships among local stakeholders for zoonotic diseases. However the needs assessment concluded that institutional barriers prevent greater linkage among human and animal health sectors. Removal of institutional barriers at middle and upper management levels of human and animal health agencies remains an essential target to address in order to promote integration of joint training and implementation of functional SRRT in the region for zoonotic diseases.
4 Regional Application of the Field Epidemiology Training Program for Veterinarians (FETPV)
4.1 The Need for Veterinary Field Epidemiologists
Veterinary infrastructure will require improvement to support a successful One Health approach. The 79th General Session of the World Assembly of the World Organization for Animal Health (OIE) cited that more than half the countries of the world have fewer than 35 public sector veterinarians per million inhabitants and with a median number of 5.4 veterinarians per million with an animal health mandate (including zoonotic and animal specific diseases (Bonnet et al. 2011)). In addition, over half the countries of the world invest less than US$ 2 per capita per year of public investment on veterinary services. The functional state of animal health surveillance systems is limited since even though 86 % of countries reported having the capacity for early detection by the animal health sector, 30 % of them had not reported suspected disease events during the previous 5 years (Bonnet et al. 2011). However diagnostic capacity has greatly improved since the advent of avian influenza H5N1 subtype through the creation of an active regional laboratory network which is increasingly capable of detecting a wider array of zoonotic diseases, in partnership with public health laboratories and enabled through donor support. “Two-way linking” of field and laboratory services within the animal health sector is being strengthened with the aim of enabling the eventual “four-way linking” between laboratory and field services of animal health and public health services.
Veterinarians have been engaged in public health training and service in the U. S. through the epidemiology intelligence service (EIS) since 1951 (Pappaioanou et al. 2003). Engagement of veterinarians in field epidemiology training and service has evolved more recently in Asia. Its development is also coincident with wider recognition of the general need for field training in veterinary epidemiology (Salman 2009). In 2008, three strategic areas were identified for the development of FETPV, which include establishing partnerships, designing a programmatic framework and developing a relevant curriculum to meet country needs within the region.
4.2 Assessing Veterinary Epidemiology Capacity Development in Asia
Prior to the development of FETPV, FAO conducted an inventory of training related to epidemiology for veterinarians in the Region of Asia and the Pacific in 2008 for training conducted in the region that was largely supply-driven. The training included an 30-month period between January 2006 and June 2008 associated with efforts to prevent and control the panzootic of HPAI H5N1 in Asia. The review included 356 training courses in 10 countries, which assessed the quantity and quality of efforts at country level (FAO 2008a). A summary of these parameters and findings is presented in Table 9.2.
It was necessary to adjust capacity development to provide demand-driven training and to address country and regional ownership and stakeholder needs. From its inception, FETPV was envisioned as a model that addresses both public health and animal health sector needs for both zoonotic and animal-specific diseases in order to be relevant and sustainable.
FETPV is a living branch of a mature FETP which has been developed in many countries in the region. This joint collaboration can also support the development of wildlife and ecosystem needs under a broad One Health canopy.
4.3 Regional Needs Assessment for Veterinary Field Epidemiology Training
Vision and mission statements, six core competencies and 32 skills were defined through a consultative workshop facilitated by FAO that included technical inputs from Thailand MoPH, Thailand DLD and university representatives (FAO 2008c). A list of skills and competencies for FETPV is presented in Table 9.3.
The stated objective of FETPV was “training through providing services” as with FETP. The required skills, competencies and concepts from the Training Programs in Epidemiology and Public Health Interventions Network (TEPHINET) were adapted for veterinarians based on the public health needs as well as the nature of the animal health work and services provided (Traicoff et al. 2008) (U.S. CDC 2006).
The output from this consultative workshop provided the basis for a needs assessment tool including a gap analysis in nine member countries of the Region of Asia and the Pacific including Cambodia, China, Indonesia, Lao PDR, Malaysia, Mongolia, Myanmar, Thailand and Viet Nam (FAO 2008b). The needs assessment included a semi-structured questionnaire using a Delphi approach which created a profile of country level animal health services and their relationship with public health services and needs. An analysis of skills identified for veterinary field epidemiologists was produced for zoonotic and animal specific disease priorities at the country level. The gap analysis and country profiles served as the basis for the development for the FETPV pre-requisite short course and for the 2-year modular curriculum. The process of conducting a needs assessment promoted trust and ownership for countries that continue to support FETPV. Key outcomes of the 2008 regional needs assessment are listed in Table 9.4.
The assessments uncovered the need to develop short, medium and long-term approaches for capacity development at local, subnational and national levels that include vocational, in-service and academic training models.
In 2010, seeing the potential use of field epidemiology to solve animal disease problems in their country the China Ministry of Agriculture (MoA) requested FAO to assist in developing a roadmap to develop a 2 year national FETPV that would complement the China FETP that which was established in 2003. After 2 years, China MoA now provides the majority of funding to support China FETPV (Fusheng 2012, personal communication). Further, coordination between the Thailand based FETPV and China FETPV includes sharing lessons learned, resource persons and training materials.
4.4 Application of FETPV in the Region
Demand for veterinary field epidemiology training at the country and sub-regional level has grown since 2010 through application of the pre-requisite short course including 1 week of field activities based on country needs assessment profiles. The FETPV pre-requisite course has been adapted for country level and regional contexts including China, Lao PDR, Cambodia, India and the eight member countries of the South Asian Association for Regional Cooperation (SAARC). The Food Agricultural Organization (FAO) has developed working partnerships with national, international and other public health agencies to provide joint training under a One Health umbrella through memoranda of understanding that include country FETP, the World Health Organization and the U.S. CDC.
To further create an enabling environment for field epidemiology training in the region, strategic planning and regional institutionalization are required to sustain FETPV. FAO has conducted advocacy with country Chief Veterinary Officers (CVO) to raise awareness of the need for epidemiology and related institutional changes required to enable and support field epidemiologists following their return to the workplace (FAO 2010). In 2011 and 2012, member country representatives from the Association of South East Asian Nations (ASEAN) developed a strategic framework and plan for epidemiology capacity development (FAO 2012a). As of May 2013 both FETPV and the strategic plan are now formally recognized by ASEAN as regional platforms. There is similar potential to support the needs of the SAARC member countries.
Since 2008, FETPV training has expanded to include both ASEAN and SAARC member countries with 2-year programs established in Thailand and China. In addition, a total of 12 FETPV pre-requisite short courses have been conducted in six countries since January 2009 in Thailand (4), China (2), Lao PDR (2), Cambodia (1), India (2) and Nepal (1). In consultation with country decision makers, trainees attend the FETPV short course in order to prepare in-country field studies upon their return from the training. Fifty field studies have been conducted for seven of the 12 short courses conducted since 2009 despite limitations in funding and mentoring. Constraints related to travel, laboratory testing and mentoring limit the number of eligible field surveys that can be implemented by FETPV short course participants. Follow up workshops to report results are held in Thailand and are currently under development in Cambodia and Nepal.
Veterinary participants in the FETPV short course demonstrate a strong interest in conducting surveys for zoonotic diseases in their countries. Fifty-four percent (27/50) of all field surveys conducted by FETPV short course participants involve zoonotic diseases including brucellosis, rabies, anthrax, leptospirosis, and Japanese encephalitis.
Institutional barriers such as lack of regional enabling mechanisms, lack of funding and the limited availability of resource persons restrict input from national and international public health experts for veterinary field epidemiology training programs. However, well-established FETPs have provided significant inputs in three of the six training centers. Training contributions from national health agencies occurred at three of five training centers noted above and one of five training centers received training inputs from international health agencies for FETPV short course training across the region. Resource constraints limit input from some public health agencies in addition to existing institutional barriers in some countries or sub-regions.
4.5 Visible Implementation of One Health
FETP and FETPV are practical means of actualizing the One Health approach based upon shared needs and mutual benefit. Integration of One Health through joint training is progressing, however institutional barriers and financial constraints must be overcome to increase the benefits of training investments in some countries. Mechanisms are needed to transfer One Health knowledge and approaches beyond the conceptual stage within the existing institutional frameworks of each country in order to conduct field studies that are trans-sectoral. The development of joint surveillance and rapid response teams is limited and incipient in most countries in the region with some exceptions including Thailand, Bangladesh and Cambodia.
Inter-sectoral as well as inter-disciplinary efforts are essential components of FETPV that include training modules linking these various aspects. Inter-sectoral commitment includes joint classroom and field training by instructors and mentors to demonstrate disease relationships at the human-animal-environment interface. Similarly, FETPV trainees consider disease events at the social-economic-communications interface to broaden the scope and understanding of the role and inter-relationships of field epidemiology with other disciplines.
5 Opportunities for Collaboration and Future Challenges
Historically, the need for collaboration under a One Health approach has been forced upon the global community by biological and political imperatives (Zinsstag and Weiss 2001). The succession of large-scale disease events illustrates the need to develop common platforms such as field epidemiology capacity in order to respond to emerging zoonotic diseases and livestock diseases comprehensively. The collaboration between FETP and FETPV represents a practical vehicle for One Health in action through training, working and sustainably building together at individual, institutional and country levels.
5.1 Joint Training
Joint training and fieldwork raises awareness of the benefits of working together to overcome differing institutional cultures and mandates. Joint training creates a common language, culture and experience that can lead to operationalized responses to pathogens and disease agents that are not constrained within institutional walls.
Joint training through FETP and FETPV in Thailand fosters a culture of mutual respect and appreciation among countries, sectors and disciplines. Individuals in applied epidemiology training are exposed to a performance (student-centered) model as opposed to an acquisition (teacher-focused) model (Taylor 2009). This learning model builds critical thinking skills that are transferrable and can adjust to the demands of dealing with any emergent disease agent that encompasses multiple sectors, disciplines and geo-political boundaries. Joint training from a broad range of instructors further expands understanding about how to implement surveillance or outbreak investigation jointly where the disease agent interacts at the interface of humans, livestock, wildlife and the environment. Quality assurance, particularly in an operational sense, is essential for continual improvement and adaptation of training to meet evolving challenges (White et al. 2001).
The FETPV is complementary to other training models needed for training para-veterinarians as well as undergraduate and post-graduate academic training for veterinarians. Veterinary Public Health needs must also be addressed including meat inspection, food safety and zoonotic disease control in live animals (Zamri-Saad et al 2009). Joint training of participants from many countries raises awareness of transboundary and regional perspectives that affect prevention and control of diseases at the country level (White et al. 2001).
5.2 Working Together
Service delivery models for joint surveillance and investigation of zoonoses when present will be specific for each disease event and within each country (Schelling et al. 2005). The relative scarcity of human resources to conduct field assessment and response in most countries requires a clear strategic approach to optimize these scarce resources. The SRRTs model in Thailand reflects a technically sound and financially practical option for disease response and surveillance from local communities to the national level.
Field epidemiology training programs focus on producing high quality graduates through an in-service training model at similar cost to a conventional academic training program. Balancing this cost, it has been demonstrated that governments also directly benefit from the “training through services model” (U.S. CDC 2006). Funding and cost sharing for training and field investigation and research greatly leverages scarce funds available, particularly for animal health agencies. Cost sharing by the Thai national government and international development partners has been used to support field activities and international fellowships including sponsoring attendance at international conferences to present findings of field research.
The increasing demand for food will require the use of systems-based approaches in order to mitigate risks to human health (King 2008). The occurrence of H7N9 in China in 2013 illustrated the opportunity to combine value chain analysis with epidemiological information in order to characterize and mitigate risks within large systems related to human exposure. These integrated systems-based approaches are greatly needed as food systems become larger and more complex. There are opportunities to extend the FETPV to building linkages with animal industry that have been promoted in Indian veterinary curricula, (Rahman 2004).
5.3 Building Sustainably Together
At the country level, applied training through FETP has contributed greatly to designing and implementing health programs since their initiation (White et al. 2001) (Yin et al 2006) (Petersen et al. 2000). This need for applied field training is now being extended to support the inclusion of both veterinary and non-veterinary wildlife professionals through joint FETP and FETPV training such as the wildlife training module (WILD) (FAO 2012b). TEPHINET has included the participation of FETPV at regional and global meetings to discuss curriculum development, program assessment and to share findings of field studies at conferences.
Building functional regional networks of alumni and mentors is will ensure the sustainability of FETP, FETPV and Field Epidemiology Training Network (FETN), which is a regional platform, recognized by 10 ASEAN nations plus China, Japan and the Republic of Korea. These integrated networks will support effective front line capacity to meeting the ongoing challenge of controlling emerging infectious diseases.
References
Bonnet P, Lancelot R, Seegers H, Martinez D (2011) Contribution of veterinary activities to global food security for food derived from terrestrial and aquatic animals. In: 79th General Assembly of the World Organization for Animal Health, Paris, 22–27 May 2011
FAO (2008a) Assessment of epidemiology training in the region of Asia and the Pacific, January 2006 to June 2008, D Castellan internal FAO report
FAO (2008b) Needs assessment for the development of a field epidemiology training program for veterinarians (FETPV) in the region of Asia and the Pacific, D Castellan internal FAO report, August 2008
FAO (2008c) FETPV workshop to develop a vision, mission competencies and skills for the FETPV program and curriculum, April 2008, Bangkok
FAO (2010) Report of the regional advocacy meeting of chief veterinary officers, August 2010, Phuket
FAO (2011) Approaches to controlling, preventing and eliminating H5N1 Highly pathogenic avian influenza in endemic countries. Animal Production and Health Paper, No. 171. Rome, 2011
FAO (2012a) Report of the regional meeting to develop a strategic plan and framework for the development of epidemiology in Asia, August 2012, Chiang Mai
FAO (2012b) WILD training press release. http://www.fao.org/ag/againfo/programmes/en/empres/news_241012.html
Gregg M (ed) (2008) Field epidemiology, 3rd edn. Oxford University Press, New York, 572 pp
Goodman RA, Buehler JW (2008) In: Gregg MB (ed) Field epidemiology. Oxford University Press, New York, pp 1–5
Khadthasrima N, Hannwong T, Thammawitjaya P, Pingsusean D, Akkanij B, Jaikhar A et al (2008) Human streptococcus suis outbreak in Phayao province, Thailand. OSIR 1(1):4–7. http://www.osirjournal.net/issue.php?id=3
King L (2008) Collaboration in public health: a new global imperative. J Vet Med Educ 35(2):264–265
Malison MD, Dayrit MM, Limpakarnjanarat K (1989) The field epidemiology training programmes. Int J Epidemiol 18(4):995–996
Pappaioanou M, Garbe PL, Glynn MK, Thacker SB (2003) Veterinarians and public health: the epidemic intelligence service of the centers for disease control, 1951–2002. J Vet Med Educ 30(4):383–391
Petersen LR, Ammon A, Hamouda O, Breuer T, Keibling S, Bellach B, Nimer U, Bindert FJ, Ostroff S, Kurth R (2000) Developing national epidemiologic capacity to meet the challenges of emerging infections in Germany. Emerg Infect Dis 6(6):576–584
Rahman SA (2004) The history of veterinary education in India. J Vet Med Educ 33(2)
Rojanapithayakorn W, Hanenberg R (1996) The 100 % condom program in Thailand. AIDS 10(1):1–7
Salman MD (2009) The role of veterinary epidemiology in combating infectious animal diseases on a global scale: the impact of training and outreach programs. Prev Vet Med 92(2009):284–287
Schelling E, Wyss K, Bechir M, Doumagoum D, Zinsstag J (2005) Synergy between public health and veterinary services to deliver human and animal health interventions in rural low income settings. BMJ 331:1264–1267
Taylor RM (2009) Defining, constructing and assessing learning outcomes. Rev Sci Tech 28(2):779–788
TEPHINET (2013) Atlanta. http://www.tephinet.org/
Traicoff DA, Walke HT, Jones DS, Gogstead EK, Imtiaz R, White ME (2008) Replicating success: developing a standard FETP curriculum. Public Health Rep 123(Suppl 1):28–34
Ungchusak K, Iamsirithaworn S (2009) Principles of outbreak investigation. In: Detels R (ed) Oxford textbook of public health, 5th edn. Oxford University Press, New York, pp 484–497
U.S. CDC (2006) Field epidemiology training program development handbook. U.S. CDC, Atlanta
U.S. CDC (2013) http://www.cdc.gov/ncezid/
Weniger BG et al (1991) The epidemiology of HIV infection and AIDS in Thailand. AIDS 5(Suppl 2):S71–S85
White ME, McDonnell SM, Werker DH, Cardenas VM, Thacker SB (2001) Partnerships in international applied training and service, 1975–2001. Am J Epidemiol 154(11):993–999
Yin J, Li G, Ren X (2006) An overview of veterinary medical education in China: current status, deficiencies and strategy for improvement. J Vet Med Educ 33(2):238–243
Zamri-Saad M, Romziah S, Kunavongkrit A, Valdez CA (2009) Integrating the world of animal health and world public health into the veterinary curriculum: a southeast Asian perspective. Rev Sci Tech 28(2):719–725
Zinsstag J, Weiss WG (2001) Livestock diseases and human health. Science 294:477
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Japan
About this chapter
Cite this chapter
Iamsirithaworn, S., Chanachai, K., Castellan, D. (2014). Field Epidemiology and One Health: Thailand’s Experience. In: Yamada, A., Kahn, L., Kaplan, B., Monath, T., Woodall, J., Conti, L. (eds) Confronting Emerging Zoonoses. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55120-1_9
Download citation
DOI: https://doi.org/10.1007/978-4-431-55120-1_9
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-55119-5
Online ISBN: 978-4-431-55120-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)