
Abstract
Despite the incessant efforts to decrease exorbitant number of daily deaths, malaria remains a major threat to the public health in many countries. Transmitted by Anopheles mosquitoes, it is caused by infection with Plasmodium parasites that have become resistant to many antimalarial drugs. In this context, series of metal-based compounds have been screened for optimal activity against different Plasmodium species and strains. This chapter briefly reviews current and potential uses of metal complexes (such as iron, cobalt, nickel, gallium, copper, gold, and silver), metal chelators, and organometallic compounds, as interesting medicinal agents that greatly benefits the fight against malaria.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others
Keywords
1 Introduction
Malaria is a neglected tropical disease caused by the protozoan of the genus Plasmodium and transmitted by the female Anopheles (Culicidae) mosquitoes (França et al. 2008). Probably originated in Africa, malaria has been plaguing the humanity for millennia, which can be inferred from documents of ancient civilizations that preceded the Christian era (Egyptians, Chinese, Mesopotamian, Hindus, Greeks, and Romans). Important figures in the human history, such as Pharaoh Tutankhamun and his family (1324 BC), Saint Augustine (579 BC), Dante Alighieri (1321 AD), and Charles V of the Holy Roman Germanic Empire (1558 AD), were affected by severe intermittent fevers (Celli 1925; Bruce-Chwatt 1988; Hawass et al. 2010; Fiocruz 2017).
The great navigations and the consequent territorial conquests were the perfect opportunity for malaria to spread to other regions of the planet, being considered one of the most devastating diseases of North American colonies between the XVI and the XVIII centuries (Duffy 1953; Ackerknecht 1966; Russell 1968). At the XVIII century, Italians thought that the symptoms of intermittent fever were due to unhealthy air—“mal aire”—and that expression gave rise to the current name of the disease, malaria. In South America, this disease arrived through the ships that brought the slaves to work mainly in Brazil (Yalcindag et al. 2012). At the XVII century, as the mortality increased, South American, Indians, and Jesuit priests started using teas and beverages prepared with Cinchona sp. as treatment (Lee 2002; Ockenhouse et al. 2005). In 1820, Pierre Pelletier and Joseph Caventau isolated quinine from Cinchona sp., proved its antimalarial effect, and in the next year, quinine and quinine sulfate were commercially available as the first antimalarial drugs (Cunico et al. 2008). Despite the discovery of an effective active principle, it took some decades to elucidate the causes of malaria. It was in 1880 that the French physician Charles Alphonse Laveran observed the malaria-causing protozoa in red blood cells of one of his patients. Between 1897 and 1899, Italian researchers Amico Bignami, Giuseppe Bastianelli, Battista Grassi, and the English physician Ronald Ross identified the female of the Anopheles mosquito as the transmitter of Plasmodium protozoan to the mammals and defined its life cycle, for which he was awarded Nobel Prizes in 1902 and 1907 (Keeble 1997; Despomnier et al. 2006; FioCruz 2017).
Up to the I World War, quinine was the only drug used to treat malaria. The difficulty to obtain the bark of Cinchona motivated the Germans to develop, in 1920, a synthetic molecule, 9-aminoacridine, that has been marketed since 1930 by the trade name Atabrine (Wallace 1989). Despite the advances, the countries involved in the I World War reported large decrease in their populations due to malaria. In the XI Pan American Sanitary Conference in 1942, malaria was identified as the continent’s most devastating disease (Rocha et al. 2006).
In the II World War, also driven by the inherent difficulties for the extraction of quinine from the bark of Cinchona, the United States started working in 1942 on an alternative synthetic drug, Atabrine (Curico et al. 2008). A couple of years later, american researchers in collaboration with pharmaceutical industries attempted to produce a synthetic quinine, but technical drawbacks and the large-scale production costs made this attempt impossible (Lee 2002).
The failures in the laboratory synthesis of quinine greatly motivated researches for the prospection of new antimalarial drugs such as Amodiaquine, Primaquine, Proguanil, Pyrimethamine, and Chloroquine (Boss et al. 2003; Ockenhouse et al. 2005; Silva et al. 2005). Chloroquine has been highlighted among these drugs due to its efficiency, low production costs, low toxicity, and the possibility of being consumed by pregnant women. These advantages made chloroquine the first choice in the treatment of malaria (Robert et al. 2001; Silva et al. 2005).
During the Korean (1950–1953) and Vietnam (1950–1957) wars, the US Army observed that some malaria patients did not respond to chloroquine. Again, a new drug prospection program was conducted, in which Dapsone, Pyrimethamine, Sulfadoxine, Sulfalene, Mefloquine, and Halofantrine were developed (Boss et al. 2003; Foley et al. 2005; Ockenhouse et al. 2005; Nzila et al. 2006).
More recently, it was observed that the number of Plasmodium strains resistant to the drugs available on the market has increased dramatically, and researches for the discovery of new antimalarial drugs have become increasingly necessary. Some emerging countries like Brazil, India, and China have invested extensively in researches for the treatment of neglected tropical diseases, especially malaria. In the 1970s, Chinese researchers presented artemisinin and its semisynthetic derivatives (Artemether, Arteether, Artesunate, Artemisinic acid, and Dihydroartemisin) as potential antimalarial drugs (Li et al. 1998; Prince 2000; Haynes 2001). The success of these drugs in the treatment of malaria is due to the fact that the Plasmodium strains have still little or no resistance to them.
Currently, statistics related to the number of malaria deaths are lower than in previous decades, with a decrease of approximately 52% in the last 15 years (Fig. 8.1). However, malaria is still present in 108 countries, and in 2015, it was estimated that 212 million people were affected by the disease, with most of the cases concentrated in Southeast Asia, sub-Saharan Africa, and Amazon due to their tropical or subtropical climates that favor the survival and reproduction of Anopheles mosquitoes. Also, countries with the highest number of malaria cases are in regions with poor sanitary conditions that also favor the reproduction and development of the malaria vector.

Number of malaria deaths in the world in the last 15 years (Source World Health Organization 2017)
Projects such as the “Roll Back Malaria Partnership” (RBM) must invest approximately 93 billion euros until 2030 (www.rollbackmalaria.org) for the treatment and total eradication of malaria. However, the success of such initiatives can be compromised once again by problems caused by the resistance of Plasmodium lineages. For this reason, research for the development of new antimalarial drugs must be constant. Recently, metal-based drugs have been actively explored for the treatment of a variety of parasites, with an important effect in the treatment of malaria. The following paragraphs aim to present the state-of-the-art of such strategy.
2 General Aspects of Malaria: The Mechanisms of Action of Classic Drugs and the Resistance of the Protozoan
Malaria is a protozoan infection caused by Plasmodium (P. falciparum, P. vivax, P. ovale and P. malariae), with P. falciparum being the most dangerous form of the disease due to the related highest rates of complications and mortality. The main vector to humans and other mammals is mosquitoes of the genus Anopheles, which comprises more than 400 species, with only a few epidemiologically important. These mosquitoes have nocturnal habits, and only females feed on blood and are responsible for the transmission of the Plasmodium (Rabinovitch et al.1998; FioCruz 2017).
The life cycle of the protozoan is divided between a host and an insect vector, as briefly described below and illustrated schematically in Fig. 8.2. (I) By stinging the host, the sporozoite form of Plasmodium, lodged in the mosquito’s salivary glands, is injected into the bloodstream until it reaches the liver. (II) In hepatic cells, the sporozoites reproduce asexually generating other cells called merozoite (not all merozoites reproduce asexually, some develop sexually). (III) The merozoites destroy the erythrocytes, causing anemia in the host and initiating a series of reproductive cycles. (IV) Some merozoites will become immature gametocytes, precursors of male and female gametes. (V) By re-stinging the host, the gametocytes will be collected and matured in the mosquito’s digestive system. (VI) The fusion of gametocytes will result in zygotes (also named as ookinetes) that will subsequently be converted into sporozoites, which migrate to the salivary glands of the mosquito, thus initiating a new infectious cycle (Rabinovitch et al. 1998; Cunico et al. 2008; FioCruz 2017).

Plasmodium life cycle. The stages I–IV occur in the host cells and stages V and VI occur in the Anopheles mosquito
The knowledge of the Plasmodium life cycle is of fundamental interest in the selection and administration of drugs for the treatment of the infected host. According to Korolkovas and Burckhalter (1982), the antimalarials commonly used act on the evolutionary stage of the parasite and can be classified as follows:
-
(I)
Blood schizonticides or suppressive agents: drugs that act on the asexual forms of the parasite found in the bloodstream;
-
(II)
Tissue schizonticides: drugs that act on the asexual forms of the parasite found in the tissues;
-
(III)
Gametocytes: drugs that act on the sexual forms of the parasites;
-
(IV)
Sporonticides: drugs that act indirectly on the vegetative forms found in the mosquito vector through gametocytes;
-
(V)
Sporozoiticides: drugs that act on the forms of the parasite infecting the host.
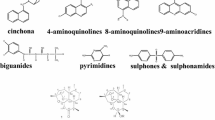
The effects of the above antimalarial drugs on parasite cells are variable according to the infecting species; however, these drugs may act as hemozoin production inhibitors, folic acid synthesis inhibitors, transcription inhibitors or inhibitors of the mitochondrial respiratory chain, transport proteins inhibitors, and genetic material modifiers (Cunico et al. 2008; Rai et al. 2017). Table 8.1 shows the main classes of antimalarial used, their molecular structures, and their effects on the parasite.
The importance of drugs with the quinoline group (highlighted in bold in the structural formulas of Table 8.1) is highlighted in several drugs, especially synthetic quinine derivatives that in the last century have achieved significant space in the pharmaceutical market. In addition to the antimalarial effect, recent studies have shown that the active ingredients quinolinics and derivatives presented antiviral activity (antiviral) (Achan et al. 2011; www.cureffi.org).
Despite a variety of drugs used in the treatment of malaria, Plasmodium species have become resistant to many compounds. Sibley and Ringwald (2007) reported that the emergence of resistance to antimalarial drugs is directly related to an enormous amount of pathogenic populations and the short time of reproduction of the parasite. In addition, the indiscriminate and extensive use of antimalarial drugs also contributes to the process of resistance.
Trying to solve this issue, the World Health Organization (WHO) recommends the use of combinations of antimalaria drugs instead of monotherapy, mainly Artemether/Lumefantrine, Artesunate/Amodiaquine, Artesunate/Mefloquine, Artesunate/Sulfadoxine, and Artesunate/Pyrimethamine (WHO 2007; Cunico et al. 2008). Some in vitro studies demonstrated that the compounds verapamil, desipramine, and promethazine may reverse the resistance of P. falciparum to chloroquine; however, the mechanisms of this reversal are not yet known (Van Schalkuyk et al. 2001; Ridley 2002; Cunico et al. 2008).
The resistance of the parasites to the classic antimalarial drugs has enormously motivated the prospection of new drugs, and metal-based compounds play an important role in this context. Strategies for the discovery and development of metal-based drugs are driven by the elucidation of the biological profile of the parasite and by the identification of therapeutic targets. Metalloantimalarials are considered very attractive new antimalaria agents as we will see in the following topics.
3 Metalloantimalarials
3.1 Metal Complexes
The use of metals for therapeutic purposes has following advantages: the possibility of preparing stable complexes with predictable structures, the selective choice of ligands according to their affinity, and the increasing know-how on the metal complexes behavior in biological environments (Allesio 2011). The antimalarial activities of several metal complexes were already demonstrated, proving their high potential as alternative treatment against resistant Plasmodium species (Biot et al. 2012; Salas et al. 2013; Wani et al. 2015).
3.2 Metal Complexes of Quinoline
The attachment of a metal atom to an already existent antimalarial drug is an interesting strategy used to enhance its efficacy (Navarro 2009). Quinoline-containing antimalarial drugs are widely used in malaria therapy, as mentioned in Table 8.1 (Salas et al. 2013).
Chloroquine (CQ) and aminoquinoline were extensively used for many years (Sharma 2005; Navarro et al. 2010). Ruthenium complexes, widely investigated for many applications in medicine, exhibit anticancer, anti-allergic, and antiparasitic potential, as they correspond to nitric oxide donors for vascular relaxation induction (Donnici et al. 2009; Levina et al. 2009; Gambino and Otero 2012; Lima et al. 2014; Seuanes et al. 2015; Correa et al. 2016; Furrer et al. 2016; Mazuryk et al. 2016; Zhang et al. 2016). The synthesis of ruthenium complexes containing CQ as ligands is an interesting strategy to improve the effectiveness of antimalarial drugs (Sanchez-Delgado et al. 1996; Biot et al. 2011; Martínez et al. 2011).
Historically, ruthenium CQ complexes were the first class of compounds investigated for this purpose. According to the literature, the binuclear complex of Ru(II) chloroquine [RuCQCl2]2 (complex 1, Fig. 8.3) was five times more potent than standard chloroquine against P. berghei and P. falciparum strains. The mechanism of action of complex 1 was described as the posthydrolytic binding to hematin in solution inhibiting its aggregation to β-hematin. Results show that the presence of the metal resulted in significantly enhanced activity against CQ-resistant strains (Sanchez-Delgado et al. 1996; Martínez et al. 2008; Salas et al. 2013).

Gold and ruthenium complexes of chloroquine
Sanches-Delgado et al. (1996) synthesized the first class of ruthenium complexes containing CQ as ligand. In vitro experiments showed that arena ruthenium complexes were more effective than CQ against resistant strains of P. falciparum. Arene-Ru(II)-chloroquine (complexes 2–4, Fig. 8.3) demonstrated appreciable antimalarial activity. Additionally, the interaction between these ruthenium derivatives and target biomolecules was investigated (Martínez et al. 2011).
Another promising class of chloroquine complexes for the development of therapeutic agents are gold complexes (Navarro 2009; Navarro et al. 2010). These compounds exhibit antiparasitic potential for the treatment of leishmaniasis, trypanosomiasis, schistosomiasis, and malaria (Fricker et al. 2008; Navarro 2009; Vieites et al. 2009; Navarro et al. 2010; Biot et al. 2012).
The antiplasmodial potential of gold complexes was investigated, with a high number of possible ligands that can be coordinated to CQ or chloroquine diphosphate (CQDP), allowing the investigation of antimalarial properties of the several complexes (Navarro 2009).
In vitro tests showed that the gold complex [Au(PPh3)(CQ)]PF6 (complex 5, Fig. 8.3) caused inhibition of two resistant strains of P. falciparum, with IC50 values of 5 and 23 nM, and against a P. berghei strain. Studies on the elucidation of the possible mechanism of action of this complex include two targets, i.e., the inhibition of hemozoin (malarial pigment) and DNA interaction. Experiments with mice showed that treatment 1 mg/kg of AuCQ, and parallely with equivalent concentrations of CQDP, induced a reduction in parasite cells of 84 and 44%, respectively, when compared to the untreated control. These results suggest that the complexation of gold to CQ increased the in vivo susceptibility of P. berghei to CQ (Navarro et al. 1997, 2011) and lead to the search for novel gold–CQ complexes, which were synthesized, characterized, and evaluated against CQ-sentitive and CQ-resistant strains of P. falciparum. In this perspective, changes in the molecular structure of the [Au(PPh3)(CQ)]PF6 complex were performed, such as variation in the counter anion (complex 6, Fig. 8.3), in the phosphine ligand (complex 7, Fig. 8.3), and in gold oxidation state (Au (I) and Au (III)) (Navarro et al. 1997, 2004).
The literature also reported the antimalarial activities of iron, cobalt, and nickel complexes containing chloroquine (CQ) and Mefloquine (Mef) as ligands. The complexes of general formula [M(II)L1L2Cl2] and [M(III)(Mef)(CQ)Cl3)], where L1 = Mefloquine, L2 = chloroquine, M = Co2+, Ni2+, and Fe3+, were synthesized, characterized, and evaluated. The in vivo tests revealed that the mixed metal complexes of Mefloquine and chloroquine [Co(Mef)(CQ)Cl2] and [Fe(Mef)(CQ)Cl3)] exhibited higher antimalarial potential. Furthermore, toxicity studies showed that these complexes demonstrated less toxicity than the Ni(II) analogue (Adediji et al. 2009). Other quinoline derivatives, Amodiaquine and primaquine, were complexed to several metal ions. The complexes of general formula [M2+(Amodiaquine)(Cl)2] and [Mn+(primaquine)2(X)n(H2O)y], where M= VO(II), Cr(III), Fe(III), Cu(II), Co(II), Ni(II), Zn(II), Cd(II), Hg(II), Rh(III), Pd(II), Au(III), Ag(I), Mn(II), Sn(II), and Pt(II), were prepared and studied as potential antimalarial agents (Wasi et al. 1987). The antimalarial activity of platinum (II) complexes containing 4-aminoquinoline analogues was also considered (Souza et al. 2011). All these results indicated that metal complexation to traditional antimalarial quinolones represents an attractive alternative to the development of new antimalarials agents.
3.3 Metal Complexes of Other Ligands
In a very informative review on gallium(III) complexes as new promising metal-based drug candidates, Lessa et al. (2012) mentioned the complex of general formula [Ga-3-Madd]ClO4, where H2-3-Madd = 1,12 bis-(2-hydroxy-3-methoxybenzyl)-1,5,8,12-tetraazododecane, active against chloroquine-resistant FCR-3 and Indo-1 lineages at low micromolar concentrations. The complexes [Fe-3-Eadd]ClO4 (complex 8, Fig. 8.4) and [Ga-3-Eadd]ClO4 (complex 9, Fig. 8.4), where H2-3-Eadd = 1,12-bis-(2-hydroxy-3-ethyl-benzyl-1,5,8,12-tetraazadodecane, were investigated in respect to their antimalarials activities against HB3 (chloroquine-sensitive) and Dd2 (chloroquine-resistant) P. falciparum strains. The results revealed that both complexes were effective against the HB3 chloroquine-resistant strains, but were 10–30 times less potent against Dh2 chloroquine-resistant strains. In the case of HB3 strains, both complexes were good inhibitors of hemozoin formation and modest to Dh2 strain. According to the authors, these results suggested that due to the similar antimalarial activities of the complexes, gallium(III) can replace iron(III) in biological environments.

Chemical structure of some metal complexes with antimalarial activity
The structure–activity correlation of some metallic antimalarial complexes was studied. A series of copper (II) complexes containing naphthoquinone ligands were synthesized, characterized, and evaluated. All complexes exhibit enhanced antimalarial activity against 3D7 P. falciparum strains. Furthermore, correlations between the antimalarial activity and the metal redox couple indicate the component of the parasitic electron transport chain as a possible target of such compounds (Gokhale et al. 2006). Complexes containing buparvaquone of general formula [M(II)(L1)2(C2H5OH)2], where M(II) = Cu, Co, Ni, Mn, and Fe and L1 = buparvaquone ({3-trans-(4-tert-butylcyclohexyl) methyl-2-hydroxy-1,4-naphthoquinone}), were studied (Gokhale et al. 2003). The copper complex that showed better results demonstrated a thousand-fold enhancement in the antimalarial activity of parent quinone against 3D7 strain. Furthermore, this complex was three times more active against the chloroquine-resistant P. falciparum K1 strain when compared to the free ligand. Experiments with this strain cellular showed a 90% reduction in parasitemia at a dose of 15 mg/kg, which demonstrates the high potential of the copper complex as antimalarial agent (Gokhale et al. 2003). The antimalarial activity of gold(I) thiosemicarbazone complexes (complexes 10 and 11, Fig. 8.4) and platinum (II) and palladium(II) complexes with ligands derived from pyrazole (complexes 12–15, Fig. 8.4) was also investigated. These complexes exhibited better efficacy in comparison to their free ligands against D10, W2, and 3D7 strains of P. falciparum (Khanye et al. 2010; Quirante et al. 2011). Besides the enhancement of the efficacy of organic drugs, the metal complexes correspond to new alternatives for the treatment of malaria, such as the inhibition of the parasite establishment in the vector mosquito.
Recently, Tapanelli et al. (2017) showed that Cu(I), Au(I), and Ag(I) phosphene complexes exhibited notable activity against the Plasmodium early sporogonic stages. The results showed that the metal complexes of general formula [M(L)4]PF6 (M = Cu(I), Ag(I) and [Au(L)4]Cl with L = Thp (tris(hydroxymethyl) phosphene) or PTA (1,3,5-triaza-7-phosphaadamantane) interfere with the early sporogonic stage of Plasmodium, inhibiting the parasite establishment in the vector mosquito.
3.4 Metal Chelators
All microorganisms need iron for their growth and replication (Crumbliss 1990). Several metabolic processes of the erythrocytic malaria parasite are dependent on iron, such as heme synthesis, DNA synthesis, proteolysis of hemoglobin, glycolysis pentose phosphate shunt, mitochondrial electron transport, and CO2 fixation. It is therefore an indication that capturing iron from the parasite may interfere negatively on its metabolism (Sharma 2005).
This strategy corresponds to an interesting alternative for malaria treatment. Common iron-chelating compounds are siderophore, naturally produced by microorganisms to acquire iron from the environment. These compounds can also be administered in the form of free ligands to sequestrate iron, causing the death of the parasite due to deprivation, or in the form of toxic complexes with iron that inhibit parasite growth (Mabeza et al. 1999).
Some characteristics are very important for effective iron-chelating, such as a hydrophilic–hydrophobic balance, the structure of the hex dentate ligand, a selectivity for iron(III), and high affinity for iron and for others cations. The affinity for iron is a main prerequisite for antimalarial activity of an iron-chelating drug, with values of affinity constants iron(III) chelators ranging from 1024 to 1038, according to the literature. The classic chelator desferrioxamine (DFO) (complex 16, Fig. 8.5), for example, presents an affinity constant value of 1031, forming a stable complex with iron and, therefore, a high antimalarial activity. The chelator must have additional affinity for other metals such as calcium, magnesium, and zinc, as their removal may be detrimental for the parasite (Goodwin and Whitten 1965; Albert 1981; Lytton et al. 1993; Ponka et al. 1994; Cabantchik et al. 1996).

Metal chelators used for malaria
The intensity of the antimalarial activity of iron chelators correlates with their hydrophilic/hydrophobic balance, as they can be capable of permeating cell membranes (Scheibel and Rodriguez 1989). Experimental studies with amino-terminal derivatives of desferrioxamine showed a preserved ability to bind to iron(III) species and a corresponding reduction to bind to iron(II) (Glickstein et al. 1996). Moreover, iron (III) forms stable complexes with coordination number equal six (Mabeza et al. 1999).
Desferrioxamine (DFO) is an important representative of iron-chelator and the first example of metal-based drug used to treat malaria. This siderophore occurs naturally in the form of trihydroxamic acid in Streptomyces pilosus and is used to treat hemochromatosis. However, the inherent slow permeation into infected cells and the restriction to advanced stages of P. falciparum are examples of drawbacks that limit its application (Modell and Berdoukas 1984; Brittenham 1988), and some structural modifications were conducted to produce more active and lipophilic derivatives, with broader efficiency for different stages of the infected cells.
As example of this strategy, a more lipophilic complex (MA-DFO, complex 17, Fig. 8.5) was synthesized by attaching N-methylanthranilic acid to the N-terminus, leading to a higher antimalarial activity. Zinc–desferrioxamine (Zn-DFO) complex exhibited increased permeability and improved antimalarial activity when compared to free DFO. A metal substitution reaction occurs inside the erythrocyte, forming the Fe(III)-DFO complex, which is more stable than the Zn-DFO complex (Loyevsky et al.1993; Chevion et al.1995).
During the last decades, the antimalarial activities of iron-chelating compounds have been investigated and metal chelators such as 1-(N-acetyl-6-aminohexyl)-3-hydroxy-2-methylpyridin-4-one demonstrated notable ability to inhibit the growth of P. falciparum in erythrocytes (Pangjit et al. 2015). Therefore, iron chelators correspond to a promising area to explore and obtain effective metal-based drugs for malaria.
3.5 Organometallic Compounds
In organometallic compounds , a metal–carbon bond (σ or π) provides special features to classic compounds. Many of these complexes have electronic structures based in 18 valence electrons (Miessler and Tarr 2004) and, due to their use in catalysis and other applications, are considerate potential therapy agents (Chavain and Biot 2010).
The first organometallic compounds for application in medicine, salvarsan (arsphenamine) and neosalvarsan, were based in arsenic and reported by Paul Ehrlich to treat syphilis and trypanosomiasis (Salas et al. 2013). Several organometallic complexes were prepared and valued as potential antimalarial agents, with ferrocene exhibiting the hightest antimalarial activity (Wani et al. 2015). Ferrocenes are highly liposoluble, stable, and nontoxic and have accessible redox potential, which make them very attractive to therapeutic applications (Van-Staveren and Metzler-Nolte 2004; Fouda et al. 2007), including malaria treatment. Inspired in ferrocene, several ferrocene-conjugated analogue structures were synthesized such as Mefloquine, artemisia, mepacrine, quinine, atovaquone, and other molecules (Biot et al. 2000; Blackie et al. 2003; Blackie and Chibale 2008).
Until the present moment, ferrochloroquine or ferroquine (FQ) (complex 18, Fig. 8.6) is the most successful metal-based drug for malaria therapy. This compound was described in 1997 as the first chloroquine derivative containing a ferrocene molecule, incorporating the ferrocene to the lateral side chain of chloroquine (Biot et al. 1997). Although there are structural similarities between chloroquine and FQ, the in vitro activities against P. falciparum of these compounds are distinct. FQ has high efficiency against chloroquine-sensitive and chloroquine-resistant P. falciparum parasite strains, reaching efficiencies 20 times higher than chloroquine. FQ exhibited high activity in vivo against P. yoeli, P. vinckei, and P. berghei strains (Biot et al. 1999, 2006).

Chemical structure of ferroquine (FQ)
Some evidences point that the action of FQ seems to be related to inhibition of the hemozoin formation in the food vacuole of the parasite. Despite the similarity in mechanism when compared to CQ, studies indicated that FQ is more efficient than CQ to inhibit the formation of β-hematin. FQ and CQ showed IC50 values of 0.8 and 1.9, respectively (Biot et al. 2005).
The ferroquine compound FQ (SSR97193) is a successful representative of an organometallic drug (Sharma 2005; Biot et al. 2011). Because of its good antimalarial activity, it has been the object of many studies (Barends et al. 2007; Biot et al. 2011; Wani et al. 2015) and is now the only metal-based compound that is in phase II clinical test for malaria therapy. Daher et al. (2006) reported in vitro studies on the metabolism of ferroquine (SSR97193) in animals and humans, indicating potential applications of ferroquine in malaria therapy.
These previous interesting results stimulated the synthesis of several ferroquine derivatives, such as thiosemicarbazones, trioxaferroquines, ferrocene dual conjugates, hydroxyferroquines, and benzothiazoles (Wani et al. 2015; Adams et al. 2017). Thiosemicarbazones (TSCs) correspond to a very important class of compound for medicinal chemistry (Leovac et al. 2007), with interesting biological effects, including antimalarial activity (Bahl et al. 2010).
In vitro tests against P. falciparum strains demonstrated that the antiplasmodial activity of FQ conjugates and thiosemicarbazones was higher than for free thiosemicarbazone. Also, FQ-TSCs (complex 19, Fig. 8.7) displayed higher efficiency against four Plasmodium strains with IC50 values at micromolar range (Biot et al. 2007). Hydroxyferroquine derivatives were also tested, and Wani et al. (2015) observed that they exhibited antiplasmodial activity and antiviral effects against coronavirus severe acute respiratory syndrome. Hydroxyferroquine (FQ-hydroxy) derivatives (Complex 20, Fig. 8.7) represent thus an excellent alternative to treat malaria infections caused by coronavirus in some specific geographical regions.

Derivatives of metal complexes of ferroquine
FQ-trioxaquines (FQ-trioxa) (Complex 21, Fig. 8.7) are potential antiplasmodial agents. In vitro and in vivo experiments demonstrated that these compounds are highly effective against CQ-resistant strains (Wani et al. 2015).
Benzothiazoles exhibit appreciable biological activity, and recently, Adams et al. (2017) evaluated antimalarial activity of ferrocenyl-containing benzothiazoles (Complex 22–24, Fig. 8.7). According to the authors, these compounds presented antiplasmodial activity against CQ-resistant and CQ-sensitive strains. They also observed that ferroquine derivatives were not able to inhibit the formation of β-hematin, indicating that FQ and its derivatives have different mechanisms of action.
The binding of active pharmacophores through covalent linkages is an interesting strategy used for the design of new antimalarial agents, such as ferrocene dual conjugates. The advantage of this strategy is the fact that it causes an increase in the conjugated molecule bioavailability, which diminishes its resistance. Some ferrocene dual conjugates demonstrated good antiplasmodial activities (Meunier 2008).
The development of ferrocene chemistry led to the investigation of ruthenocene analogues as antimalarial agents. Ruthenoquine (RQ) (complex 25, Fig. 8.8) and its derivatives (complexes 26 and 27, Fig. 8.8) were synthesized and presented good inhibition of P. falciparum growth, with similar mechanism of action as FQ (Beagley et al. 2002). All the results available up to the present moment point to an enormous potential of ferroquine and its derivatives for the development of antiplasmodial agents.

Ruthenoquine and their derivative compounds
4 Conclusions
The emergence of drug-resistant strains of Plasmodium spp. led to an urgent need to develop more effective drugs, and metal-based drugs have been considered a promising strategy against new antiplasmodial agents. In this context, metalloantimalarials based on antimalarial drugs, metal chelators, and organometallic complexes were evaluated. Among all these compounds, ferroquine is the most successful representative, already being tested in phase II clinical trials. Studies on the physiology of the parasite allowed the understanding of the mechanisms of action of new drugs and stimulated the design of new more efficient drugs. With these studies, in the near future, it is expected that metallodrugs with low toxicity and high efficiency will be found for the treatment of neglected tropical diseases such as malaria. In addition, the production costs and the final product are extremely important factors, since this guarantees the accessibility of the population of poor countries affected by these diseases.
References
Achan J, Talisuna AO, Erhart A, Yeka A, Tibenderana JK, Baliraine FN, D’Alessandro U (2011) Quinine, an old anti-malarial drug in a modern world: role in the treatment of malaria. Malaria J 10:144
Ackerknecht EH (1966) Malaria in the Upper Mississipi Valley, 1760-1900. Johns Hopkins Press, Baltimore
Adams M, Kock C, Smith JP, Chibale K, Smith SG (2017) Evaluation of ferrocenyl-containing benzothiazoles as potential antiplasmodial agents. Eur J Inorg Chem 2:242–246
Adediji FJ, Olayinka TE, Adebayo AM, Babatunde O (2009) Antimalarial mixed ligand metal complexes: synthesis, physicochemical and biological activities. Int J Phys Sci 9:529–534
Albert A (1981) Selective toxicity. Chapman and Hill, New York
Alessio E (2011) Bioinorganic medicinal chemistry. Wiley-VCH Velarg & Co, Germany
Bahl D, Athar F, Soares PBM, Sá SM, Moreira MRD, Srivastava MR, Leite ACL, Azam A (2010) Structure-activity relationship of mononuclear metal-thiosemicabazone complexes endowed with potent antiplasmodial and antiamoebic activities. Bioorg Med Chem 18:6857–6864
Barends M, Jaidee A, Khaohirum N, Singhasivanon P, Nosten F (2007) In vitro activity of ferroquine (SSR97193) agaisnt Plasmodim falciparum isolates from the Thai-Burmese border. Malaria J 6:1–5
Beagley P, Blackie MAL, Chibale K, Clarkson C, Moss JR, Smith PJ (2002) Synthesis and antimalarial activity in vitro of new ruthenocene-chloroquine analogues. Dalton Trans 23:4426–4433
Biot C, Glorian G, Maciejewski LA, Brocard JS, Domarle O, Blampain G et al (1997) Synthesis and antimalarial activity in vitro and in vivo of a new ferrocene-chloroquine analogue. J Med Chem 40:3715–3718
Biot C, Delhaes L, Abessolo H, Domarle O, Maciejewski LA, Mortuaire M, Delcourt P, Deloron P, Camus D, Dive D, Brocard JS (1999) Novel metallocenic compounds as antimalarial agents. Study of the position of ferrocene in chloroquine. J Organomet Chem 589:59–65
Biot C, Taramelli D, Forfar-Bares I, Maciejewski L, Boyce M, Nowogrocki G, Brocard JS, Basilico N, Olliaro P, Egan TJ (2005) Insights into the mechanism of action of ferroquine. Relationship between physicochemical properties and antiplasmodial activity. Mol Pharm 2:185–196
Biot C, Pradines B, Sergeant MH, Gut J, Rosenthal PJ, Chibale K (2007) Design, synthesis, and antimalarial activity of structural chimeras of thiosemicarbazone and ferroquine analogues. Bioorg Med Chem Lett 17:6434–6438
Biot C, Delhaes L, Maclejewski AL (2000) Synthetic ferrocene mefloquine and quinine analogues as potential antimalarial agents. Eur J Med Chem 35: 7–8
Biot C, Nosten F, Fraisse L, Ter-minassian D, Khalife J, Dive D (2011) The antimalarial ferroquine: from bench to clinic. Parasite 18:207–214
Biot C, Castro W, Botté YC, Navarro M (2012) The therapeutic potential of metal-based antimalarial agents: implications for the mechanism of action. Dalton Trans 21:6321–6580
Biot C, Delhaes L, Maclejewski AL, Mortuaire M, Camus D, Dive D, Brocard S J (2000) Synthetic ferrocenic mefloquine and quinine analogues as potential antimalarial agentes. Eur J Med Chem 35:707–714
Biot C, Daher W, Ndiaye C M, Melnyk P, Pradines B, Chavain N, Pellet A, Fraisse L, Pelinski L, Jarry C, Brocard J, Khalife J, Forfar-Bares I, Dive D (2006) Probing the role of the covalent linkage of ferrocene into a chloroquine template. J Med Chem 49:4707–4714
Blackie ALM, Chibale K (2008) Metallocene antimalarials: the continuing quest. Metals Based Drug 1:1–10
Blackie ALM, Beagley CK, Clarkson C, Hutton TA, Moss RJ, Smith JP (2003) Synthesis and antimalarial activity in vitro of new heterobimetallic complexes: Rh and Au derivatives of chloroquine and a series of ferrocenyl-4-amino-7-chloroquines and a series of ferroceny-4-amino-7-chloroquines. J Organomet Chem 688:144–152
Boss C, Richard-Bildstein S, Weller T, Fischli W, Meyer S, Binkert C (2003) Inhibitors of the Plasmodium falciparum parasite aspartic protease plasmepsin II as potential antimalarial agents. Curr Med Chem 10:883–907
Brittenham GM (1988) Iron chelating agentes. Curr Ther Hematol Oncol 3:149–153
Bruce-Chwatt LJ (1988) History of malaria from prehistory to eradication. In: Wernsdorfer WH, McGregor I (eds) Malaria: principles and practice of malariology. Churchill Livingstone, Edinburgh, pp 1–59
Cabantchik ZI, Glickstein H, Golenser J, Loyevsky M, Tsafack A (1996) Iron chelators: mode of action as antimalarials. Acta Haematol 95:70–77
Celli A (1925) Storia della malaria nell’agro romano. Roma, Academia dei Lincei
Centers for Disease Control and Prevention (2006) Malaria: topic home. In: http://www.cdc.gov/malaria/
Chavain N, Biot C (2010) Organometallic complexes: new tools for chemotherapy. Curr Med Chem 17:2729–2745
Chevion M, Chuang L, Golenser J (1995) Effects of zinc-desferrioxamine on Plasmodium falciparum in culture. Antimicrob Agents Chemother 39:1902–1905
Correa SR, Silva MM, Graminha EA, Meira SC, Santos FAJ, Moreira MRD, Soares PBM, Poelhsitz VG, Castellano EE, Bloch C Jr, Batista RM, Cominetti AA (2016) Ruthenium (II) complexes of 1,3-thiazolidine-2-thione: cytotoxicity against tumor cells and anti-Trypanosoma cruzi activity enhanced upon combination with benzidazole. J Inorg Biochem 156:153–163
Crumbliss AL (1990) Iron bioavailability and the coordination chemistry of hydroxamic acids. Coord Chem Rev 105:155
Cunico W, Carvalho AS, Gomes CRB, Marques GH (2008) Fármacos antimalariais—história e perspectives. Revista Brasileira de Farmácia 89:49–55
Daher W, Pelinski L, Klieber S, Sadoun F, Meunier V, Bourri M, Biot C, Guilou F, Fabre G, Brocard J, Fraisse L, Maffrand J, Khalife J, Dive D (2006) In vitro metabolism of ferroquine (SSR97193) in animal and human hepatic models and antimalarial activity of major metabolites on Plasmodium falciparum. Drug Metab Dispos 34:667–682
Despomnier DD, Gwadz RW and Hotez PJ (2006) Parasitic diseases 5th In: http://www.medicalecology.org/pdf/pd_malaria.pdf
Donnici LC, Araujo HM, Oliveira SH, Moreira MRD, Pereira ARV, Souza AM, Castro BACM, Leite LCA (2009) Ruthenium complexes endowed with potent anti-Trypanosoma cruzi activity: synthesis, biological characterization and structure-activity relationships. Bioorg Med Chem 17:5038–5043
Duffy J (1953) Epidemics in Colonial América. Lousiana State University Press, Baton Rouge
FioCruz—Malaria (2017) In: http://www.cpqrr.fiocruz.br/informacao_em_saude/CICT/malaria/ malaria.htm
Foley M, Tilley L (1998) Quinoline antimalarials: mechanisms of action and resistance and prospects for new agents. Pharmacol Ther 79:55–87
Fouda MFR, Abd-Elzaher MM, Abdelsamaia RA, Labib AA (2007) On the medicinal chemistry of ferrocene. Appl Organomet Chem 21:613–625
França TCC, Santos MG, Figueroa-Villar JD (2008) Malária: aspectos históricos e quimioterapia. Quim Nova 5:1271–1278
Fricker PS, Mosi MR, Cameron RB, Baird I, Zhu Y, Anastassov V, Cox J, Doyle SP, Hansell E, Lau G, Langille J, Olsen M, Qin L, Skerlj R, Wong RSY, Santucci Z, Mckerrow HJ (2008) Metal compounds for the treatment of parasitic diseases. J Inorg Biochem 102:1839–1845
Furrer J, Süss-Fink G (2016) Thiolato-bridged dinuclear arene rutheium complexes and their potential as anticaner drug. Coordination Chem 309:36–50
Gambino D, Otero L (2012) Perspectives on what ruthenium-based compounds could offer in the development of potential antiparasitic drugs. Inorg Chim Acta 393:103–114
Glickstein H, Breuer B, Loyevsky M, Konijn A, Libman J, Shanzer A, Cabantchik ZI (1996) Differential cytotoxicity of iron chelators on malaria-infected cells versus mammalian cells. Blood 87:4871–4878
Gokhale HN, Padhye BS, Croft LS, Kendrick DH, Davies W, Anson EC, Powell KA (2003) Transition metal complexes of buparvaquone as potent new antimalarial agents Synthesis, X-ray crystal-structures, electrochemistry and antimalarial activity against Plasmodium falciparum. J Inorg Biochem 95:249–258
Gokhale HN, Shirisha K, Padhye BS, Croft LS, Kendrick DH, Mckee V (2006) Metalloantimalarials: Synthesis, x-ray Crystal structure of potent antimalarial copper(II) complex of arylazo-4-hydroxy-1,2-naphthoquinone. Bioorg Med Chem Lett 16:430–432
Goodwin JF, Whitten CF (1965) Chelation of ferrous sulfate solutions by desferrioxamine B. Nature 205:281–283
Hawass Z, Gad YZ, Ismail S, Khairat R, Fathalla D, Hasan N, Ahmed A, Elleithy H, Ball M, Gaballah F, Wasef S, Fateen M, Amer H, Gostner P, Selim A, Zink A, Pusch CM (2010) Ancestry and pathology in King Tutankhamun’s family. JAMA 7:638–647
Haynes R (2001) Artemisia and derivatives: the future of malaria treatment. Curr Opin Inf Dis 14:719–726. http://rollbackmalaria.org. Accessed on 25 Nov 2017
Keeble TW (1997) A cure for the ague: the contribuition of Robert Talbor (1642–81). J R Soc Med 90:285–290
Khanye DS, Smith SG, Lategan C, Smith JP, Gut J, Rosenthal JP, Chibale K (2010) Synthesis and in vitro evaluation of gold(I) thiosemicarbazone complexes for antimalarial activity. J Inorg Biochem 104:1079–1083
Korolkovas A, Burckhalter JH (1982) Química Farmacêutica. São Paulo, Guanabara Dois
Lee MR (2002) Plants against malaria Part 1: Chinchona or Peruvian Bark. J Roy Coll Phys Edinburg 32:189–196
Leovac MV, Jovanovic SL, Jevtovic SV, Pelosi G, Bisceglie F (2007) Transition metal complexes with thiiosemicarbazide-based ligand—Part LV: Synthesis and X-ray structural study of novel Ni(II) complexes with pyridoxal semicarbazone and pyridoxal thiosemicabazone. Polyhedron 26:2971–2978
Lessa AJ, Parrilha LG, Beraldo H (2012) Gallium complexes as new promising metallodrugs candidates. Inorg Chim Acta 393:53–63
Levina A, Mitra A, Lay AP (2009) Recent developments in ruthenium anticancer drugs. Metallomics 1:458–470
Li Y, Wu YL (1998) How Chinese scientists discovered qinghaosu (artemisinin) and developed its derivatives? What are the future perspectives? Med Tropicale (Mars) 58(3 Suppl):9–12
Lima GR, Rodrigues SRB, Silva SR, Bendhack ML (2014) Ruthenium complexes as no donors for vascular relaxation induction. Molecules 19:9628–9654
Loyevsky M, Lytton SD, Mester B, Libman J, Shanzer A, Cabantchik ZIJ (1993) The Antimalarial action of deferral involves a direct access route to erythrocytic (Plasmodium falciparum) parasites. Clin Inv 91:218–224
Lytton SD, Mester B, Dayan I, Glickstein H, Libman J, Shanzer A, Cabantchik ZI (1993) Mode of action of iron (III) chelators as antimalarials: I. Membrane permeation properties and cytotoxic activity. Blood 81:214–221
Mabeza FG, Loyevsky M, Victor R, Gordeuk RV, Weiss G (1999) Iron chelation therapy for malaria: a review. Pharmacol Ther 81:53–75
Martínez A, Rajapakse CSK, Naoulou B, Kopkalli Y, Davenport L, Sánchez-Delgado RA (2008) The mechanism of antimalarial action of the ruthenium(II)-chloroquine complex [RuCl2(CQ)]2. J Biol Inorg Chem 13:703
Martínez A, Suárez J, Shand T, Magliozzo SR, Sánchez-Delgado AR (2011) Interactions of arene-Ru(II)-chloroquine complexes of know antimalarial and antitumor activity with human sérum albumin (HSA) and transferrin. J Inorg Biochem 105:39–45
Mazuryk O, Lomzik M, Martineau D, Beley M, Brendell M, Stochel G, Gros CP (2016) Anticancer activity of ruthenium(II) polypyridine complexes bearing pyrrolidine substituents. Inorg Chimica Acta 443:86–90
Meunier B (2008) Hybrid molecules with a dual mode of action: dream or reality. Acc Chem Res 41:69–77
Miessler LG, Tarr AD (2004) Inorganic chemistry, 3rd edn. Minnesota, Pearson
Modell B, Berdoukas V (1984) The clinical approach to Thalassemia. Grune and Stratton, London
Navarro M (2009) Gold complexes as potential anti-parasitic agentes. Coord Chem Rev 253:1619–1626
Navarro M, Pérez H, Sanchez-Delgado RA (1997) Toward a novel metal-based chemotherapy against tropical diseases. 3. Synthesis and antimalarial activity in vitro and in vivo of the new gold-chloroquine complex [Au(PPh3)(CQ)]PF6. J Med Chem 40:1937–1939
Navarro M, Vásquez F, Sánchez-Delgado RA, Pérez H, Sinou V, Schrével J (2004) Toward a novel metal-based chemotherapy against tropical diseases. 7. Synthesis and in vitro antimalarial activity of new gold-chloroquine complexes. J Med Chem 21:5204–5209
Navarro M, Gabbiani C, Messori L, Gambino D (2010) Metal-based drugs for malaria, trypanosomiasis and leishmaniasis: recent achievements and perspectives. Drug Discovery Today 15:1070–1078
Navarro M, Castro W, Martínez A, Sánchez Delgado RA (2011) The mechanism of antimalarial action of [Au(CQ)(PPh)3]PF6: structural effects and increased drug lipophilicity enhance heme aggregation inhibition at lipid/water interfaces. J Inorg Biochem 105:276–282
Nzila A (2006) The past, present and future of antifolates in the treatment of Plasmodium falciparum infection. J Antimicrob Chemother 57:1043–1054
Ockenhouse CF, Magill A, Smith D, Milhous W (2005) History of U.S. Military contributions to study of malaria. Mil Med 170:6–12
Pangjit K, Banjerdpongchai R, Phisalaphong C, Fucharoen S, Xie YY, Lu ZD, Hider RC, Srichairatanakool S (2015) Characterisation of a novel oral iron chelator: 1-(N-Acetyl-6-Aminohexyl)-3-Hydroxy-2-Methylpyridin-4-one. J Pharm Pharmacol 67:703–713
Ponka P, Richardson DR, Edward JT, Chubb FL (1994) Iron chelators of the pyridoxal isonycotinoyl hydrazone class. Relationship of the lipophilicity of the apo chelator to its ability to mobilize iron from reticulocyte in vitro. Can J Physiol Pharmacol 72:659–666
Prince R (2000) Artemisinin drugs: novel antimalarial agents. Expert Opin Investig Drugs 9:1815–1827
Quirante J, Ruiz D, Gonzalez A, López C, Cascante M, Cortés R, Messeguer R, Calvis C, Baldoma L, Pascual A, Guérardel Y, Pradines B, Font-Bardía M, Calvet T, Biot C (2011) Platinum(II) and palladium(II) complexes with (N, N′) and (C, N, N′) ligands derived from pyrazole as anti-cancer and antimalarial agents: Synthesis, characterization and in vitro activities. J Inorg Biochem 105:1720–1728
Rabinovitch L, Silva CMB, Alves RSA (1999) Controle biológico de vetores de doenças tropicais utilizando Bacillus entomopatogênicos. In: Melo IS, Azevedo JL (eds) Controle biológico. Jaguariúna, EMBRAPA Meio Ambiente
Rai MK, Ingle AP, Paralikar P, Gupta I, Medici S, Santo CA (2017) Recent Advances in use of silver nanoparticles as antimalarial agents. Int J Pharm 526:254–270
Ridley RG (2002) Medical need, specific opportunity and the drive for antimalarial drugs. Nature 415:686–693
Robert A, Benoii-Vical F, Dechy-Cabaret O et al (2001) From classical antimalarial drugs to new compounds based on the mechanism of action of artemisinin. Pure Appl Chem 73:1173–1188
Rocha MNA, Ferreira EAP, Souza JM (2006) Aspecto histórico da malária. Rev Para Med 20:81–82
Russel PF (1968) The United States and malaria: debits and credits. Bulletin of the New York Academy of Medicine. 44:623
Salas FP, Herrmann C, Orvig C (2013) Metalloantimalarials. Chem Rev 113:3450–3492
Sanchez-Delgado R, Navarro M, Perez H, Urbina JA (1996) Toward a novel metal-based chemotherapy against tropical diseases. 2. Synthesis and antimalarial activity in vitro and in vivo of new ruthenium and rhodium-chloroquine complexes. J Med Chem 39:1095–1099
Scheibel LW, Rodriguez S (1989) Anti-malarial activity of selected aromatic chelators. V. Localization of 59Fe in Plasmodium falciparum in the presence of oxines. Prog Clin Biol Res 313:119–149
Seuanes GC, Moreira MB, Petta T, Moraes DMPF, Moraes LAB, Oliveira ARM, Naal GZMR, Nikolaou S (2015) Novel binuclear μ-oxo diruthenium complexes combined with ibuprofen and ketoprofen: interaction with relevant target biomolecules and anti-allergic potential. J Inorg Biochem 153:178–185
Sharma V (2005) Therapeutic drugs for targeting chloroquine resistance in malaria. Mini-Rev Med Chem 5:337–351
Sibley CH, Ringwald PA (2007) Database of antimalarial drug resistance. In http:www.malariajournal.com/ content/5/1/48
Silva THA, Oliveira MT, dos Santos HF, de Oliveira AB, de Almeida WB (2005) Estudo de modelagem molecular de complexos ferriprotoporfirina-IX e quinolinocarbinolaminas antimaláricos: Proposta de um farmacóforo. Quim Nova 28:244–249
Souza BN, Carmo LMA, Lagatta CD, Alves MJM, Fontes SPA, Coimbra SE, Silva DA, Abramo C (2011) 4-aminoquinoline analogues and its platinum (II) complexes as antimalarials agents. Biomed Pharmacother 65:313–316
Tapanelli S, Habluetzel A, Pellei M, Marchió L, Tombesi A, Capparé A, Santini A (2017) Novel metalloantimalarials: Transmission blocking effects of water soluble Cu (I), Ag(I) and Au(I) phosphane complexes on the murine malaria parasite Plasmodium berghei. J Inorg Biochem 166:1–4
Van Schalkuyk DA, Walder JC, Smith PJ (2001) Reversal of chloroquine resistance in Plasmodium falciparum using combinations of chemosensitizers. Antimicrob Agents Chemotherapy 45:593–597
Van-Staveren DR, Metzler-Nolte N (2004) Bioorganometallic chemistry of ferrocene. Chem Rev 104:5931–5986
Vieites M, Smircich P, Guggeri L, Marchán E, Gónrez-Barrio A, Navarro M, Garat B, Gambino D (2009) Synthesis and characteization of a pyridine-2-thiol N-oxide gold(I) complex with potent antiproferative effect against Trypanosoma cruzi and Leishmania sp insight into its mechanism of action. J Inorg Biochem 103:1300–1306
Wallace DJ (1989) The use of quinacrine (atrabine) in rheumatic diseases: a reexamination. Semin Arthritis Rheu 18:282–297
Wani AW, Jameel E, Baig U, Mumtazuddin S, Hun TL (2015) Ferroquine and its derivatives: new generation of antimalarial agents. Eur J Med Chem 01:534–551
Wasi N, Singh HB, Gajanana A, Raichowdhary AN (1987) Synthesis of metal complexes of antimalarial drugs and in vitro evaluation of their activity against Plasmodium falciparum. Original Inorg Chimica Acta 135:133–137
WHO (2017) http://www.who.int/malaria/en/
WHO Facts on ACTs (Artemisinin-based Combination Therapies) (2007) In:http://rbm.who.int/cmc_upload/ 0/000/015/364/RBMInfosheet_9.htm
Yalcindag E, Elguero E, Arnathau C, Durand P, Akiana J, Anderson TJ, Aubouy A, Balloux F, Besnard P, Bogreau H, Carnevale P, D’Alessandro U, Fontenille Gamboa D, Jombart T, Le Mire J, Leroy E, Maestre A, Mayxay M, Ménard D, Musset L, Newton PN, Nkoghé D, Noya O, Ollomo B, Rogier C, Veron V, Wide A, Zakeri S, Carme B, Legrand E, Chevillon C, Ayala FJ, Renaud F, Prugnolle F (2012) Multiple independent introductions of Plasmodium falciparum in South America. Proc Nat Acad Sci 109:511–516
Zhang C, Han B, Zeng C, Lai S, Li W, Tang B, Wan D, Jiang G, Liu Y (2016) Synthesis characterization in vitro cytotoxicity and anticancer affects of ruthenium(II) complexes on BEL-7402 cells. J Inorg Biochem 157:62–72
Acknowledgments
The authors thank FAPESP (process number 15/06238-4) and CNPq (process number 304826/2013-8) for the financial support of research carried out in our laboratories.
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Marcelino, P.R.F., Moreira, M.B., Lacerda, T.M., da Silva, S.S. (2018). Metal-Based Drugs for Treatment of Malaria. In: Rai, M., Ingle, A., Medici, S. (eds) Biomedical Applications of Metals. Springer, Cham. https://doi.org/10.1007/978-3-319-74814-6_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-74814-6_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-74813-9
Online ISBN: 978-3-319-74814-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)