
Abstract
Acute otitis media is a frequent manifestation of otitis media, mainly during the early childhood. The multifactorial pathogenesis and risk factors are exposed along with its most microbiological agents. The clinical manifestations and their differential diagnoses are presented. General concepts and different actual guidelines of the treatment are described, also the efficient preventive measures are proposed.
The second main issue of this chapter is to deal with the complications of acute otitis media, especially the acute coalescent mastoiditis, that is the most common suppurative complication of AOM. The pathogenesis of coalescent acute mastoiditis, its epidemiology, risk factors and the microbiological agents are presented. The clinical features and differential diagnosis are described, as the specific imaging findings. Complications of acute coalescent mastoiditis are typically the subperiosteal abscess, due to the cortical bony necrosis of the mastoid and its septa, or the intracranial spread of the infection (meningitis, intracranial abscesses and venous sinus thrombosis).
The general concept of management is exposed, with emphasis on the antimicrobial treatment and the different surgical options.
You have full access to this open access chapter, Download chapter PDF
Keywords
- Acute Otitis Media (AOM)
- Coalescent Mastoiditis
- Acute Mastoiditis
- Subperiosteal Abscess
- Otitis Media With Effusion (OME)
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
2.1 Introduction
Otitis media (OM) comprises a wide spectrum of diseases that include acute otitis media (AOM), recurrent acute otitis media (rAOM), otitis media with effusion (OME), chronic otitis media with effusion (COME) and chronic suppurative otitis media (CSOM) [1,2,3].
AOM is an acute inflammation and infection of the middle ear caused by bacteria and/or viruses. In general, it is a childhood disease that manifests as a rapid onset of fever and otalgia [1, 2, 4]; if the child has ≥3 episodes of AOM in the preceding 6 months, or ≥4 episodes in the preceding 12 months, he should be considered to have rAOM [1, 5, 6]. Patients who have more than six episodes in the first 6 years of life are called otitis “prone ” [7]. The presence of fluid in the middle ear with absence of acute signs and symptoms of infection and inflammation is defined as OME, and if the fluid persisted more than 3 months, it is considered as COME [1]. CSOM is defined as an ear discharge with tympanic membrane (TM) perforation for more than 3 months [1].
This chapter will scope on AOM and its complications, mainly acute and coalescent mastoiditis.
2.2 Epidemiology
AOM is the second most common reason for a family physician’s visit and the most common reason for prescribing antimicrobial drugs. It accounts for 10–15% of all childhood medical visits.
AOM has an incidence rate of 10.8/100 people per year [8]. 70% of children manifest at least one episode of AOM even in developed countries. Males have a higher incidence of AOM [1, 9].
AOM has a peak incidence at the age of 6–11 months [1, 9]; 59% of children will have one episode of AOM and 30% will have two episodes or more by the age of 2 [1]. rAOM resolve spontaneously when the child gets older, often at 3–4 years of age. AOM incidence rate drops rapidly after the age of 5 years.
2.3 Pathogenesis
AOM has multiple risk factors (host factors, environmental, microbiological and genetic factors) that interact with each other and make the patient more susceptible to become affected by AOM [10,11,12].
AOM is related to upper respiratory infections (URTI): More than 90% of AOM episodes develop after URTI [1, 7]; one of three children will develop AOM after URTI [12]. URTI causes nasopharyngitis which affects Eustachian tube function, and induces a negative pressure in the middle ear with secondary suction of the nasopharyngeal secretions inside the middle ear. This explains why aspirates of AOM can show bacteria like Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis [2, 9], which are commensal to the nasopharynx [13]. This mechanism is exaggerated by bottle-feeding, pacifier use, and other sucking behaviors. The initial course of the disease is thought to be of viral origin followed by superimposed bacterial infections [2, 12]. Many viruses have been implicated as causative agents which are found in 90% of AOM cases, such as the rhinovirus, coronavirus, enterovirus, respiratory syncytial virus (RSV), parainfluenza type 1, 2 or 3, influenza A or B, and adenovirus [1, 2, 7, 8, 14]. Among all of these, RSV is believed to have the most frequent association with AOM [12]. These viruses are thought to increase the adherence of the bacteria to the epithelium so enhancing bacterial colonization [12, 14], however, there is a rising evidence that viruses alone can cause AOM without bacterial superinfection in 10–15% of cases, a point that should be kept in mind while treating AOM with antibiotics [12, 14].
Genetics play an important role in the susceptibility of an individual to AOM [1, 2, 9, 11, 12]: When comparing genetic to environmental risk factors, genetic predisposition with a specific genotype was found to be a stronger risk factor than the socioeconomic status. Positive family history of otitis media is a strong risk factor for developing AOM and other forms of otitis media.
Native American Maori or Australian Aborigine populations have more prevalence of AOM as compared to the white population [1]. One cohort study showed that heritability is found in 38.5% in rAOM [11]. Some investigators have linked this susceptibility to inherited poor ET function [2]. Other investigators found that specific polymorphisms of some cytokines have been correlated to the susceptibility of an individual to AOM and to the severity of the disease as well [10, 12]. IL-1s, IL-6 and TNFα have been found in nasopharyngeal secretions during URTI and increased levels of IL-1s are linked to the transition to AOM [12]. TNFα-308 polymorphisms are associated with AOM that follows URTI. In addition, some rAOM patients were found to have TNFα-308 and IL-6-174 polymorphisms [12]. Genes for Fcg-receptor IIa (FcgRIIa), IL-10, CD14, toll-like receptor 4 (TLR4), surfactant, and interferon gamma (IFNg) are believed to be responsible for an AOM risk [11].
The importance of environmental factors must not be underestimated in the pathogenesis of AOM; Paternal smoking is one of otitis media major risk factors [1, 3, 8,9,10]. Passive smoking causes mucosal inflammation, goblet cells hyperplasia and an increase in the production of mucus, all together impairs mucosal muco-ciliary clearance and increases bacterial colonization by enhancing the bacterial binding to respiratory epithelium [1, 10]. Children of mothers who smoked during pregnancy and stopped after delivery still have a higher incidence of AOM [10].
Some studies found a role of gastroesophageal reflux disease (GERD) [1, 15]; GERD is found in 62.9% of patient with rAOM. In fact, pepsin/pepsinogen can be found in the middle ear in 85.3% of otitis media patients that could be explained by the reflux; however a cause and effect relationship could not be established [15].
There are other risk factors that are related to AOM, like prematurity [9], young age [1, 8], day care attendance [3, 9, 10], increased number of siblings, dummy use [1, 9], autumn and winter seasons [1], craniofacial anomalies [8], asthma [3] and atopy [3, 8] (Fig. 2.1).
An epidemiological survey from Denmark [16] stated that the following factors were predictive of early AOM and rAOM: male gender, prematurity, parity (number of pregnancies the mother has had), maternal age, maternal self-estimated health, maternal intake of penicillin during pregnancy, and termination of breastfeeding before the child was 6 months old (Fig. 2.1).

Interactive predisposing factors of acute otitis media
2.4 Microbiology
AOM is usually a complication of an acute viral upper respiratory infection. The most common bacterial pathogens associated with the diagnosis of AOM are: Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis [3, 17, 18].
Streptococcus pneumoniae is the most common, found in 35–45% [3, 18]. Patients infected with this microorganism tend to have more severe disease [3, 13]. The serotypes responsible have been changed after the introduction of pneumococcal 7-valent conjugate vaccine (PCV-7) [3].
Haemophilus influenza has become more common after PCV-7 vaccine [3]. It is related to bilateral disease, recurrent cases, and conjunctivitis with the so called “otitis-conjunctivitis syndrome” [3, 13, 17].
Moraxella catarrhalis is found in 10–20% of cases [17], 100% are beta lactamase producers [17].
All of the above pathogens have the ability to form biofilms [13], which are thought to be responsible for the resistance to antimicrobial therapy [13].
Group A Streptococcus, Group B Streptococcus, Staphylococcus aureus and gram-negative bacilli are other bacteria that can be encountered in approximately 15% of cases [3]. A first episode of bacterial infection with invasive strains (like invasive strains of Streptococcus pneumoniae) can lead to mucosal changes which make the ear more susceptible to acquire the disease by less virulent strains [19].
Approximately 5% of ears have multiple pathogens. In approximately 20–30% of ears with clinical AOM [20], no bacterial pathogen was identified by tympanocentesis.
Respiratory viruses including RSV, rhinovirus, adenovirus, influenza virus, parainfluenza virus, and CMV are isolated from the cultures of approximately 20% of middle ear samples, half of them have bacterial/viral co-infections [20].
In cases of simultaneous infection with pathogenic viruses and bacteria, antibiotic response appears to be inferior to that of children that have only a bacterial infection, and microbiologic failure can occur despite clear in vitro sensitivity to the used antibiotic. Consequently, a second course of antibiotics can effectively clear the bacteria after the immune system has cleared up the viral infection.
2.5 Clinical Manifestations
2.5.1 Symptomatology
AOM has typically a short history of onset; it is commonly associated with fever, otalgia, ear pulling, irritability, lethargy, anorexia, and vomiting.
Earache is one of the most common and distressing symptoms of AOM.
Ear pulling is not specific as only 10% of ear pullers will have AOM.
These symptoms alone lack sensitivity and specificity; the diagnosis of AOM must rely on otoscopy findings.
Immunosuppressed patients, particularly those undergoing chemotherapy, may not manifest the typical acute inflammatory symptoms whereas systemic sepsis and middle ear effusion might be the only indicators of AOM.
2.5.2 Examination
Performed under ideal conditions, otomicroscopy with adequate visualization of the eardrum (cleaning the ear canal is most often required) allows proper diagnosis of AOM (Fig. 2.2). Non-cooperative children usually need to be restrained. Diagnosis may be difficult in very young children but it is important to accurately do so. A first episode of AOM before 6 months of age is likely to lead to recurrence of AOM, and subsequently, significant periods of OME with diminished hearing and delayed speech.

Left ear acute otitis media with bulging of the hyperemic tympanic membrane and yellowish effusion in the middle ear cavity
The common otoscopic findings of AOM are:
-
Hyperemic and hypervascularized tympanic membrane. Early AOM may be diagnosed by inflammation which is seen along the handle of malleus and in the superior pole of the tympanic membrane.
-
Bulging tympanic membrane is the only specific sign for AOM. In the absence of a bulging ear drum but with clinical suspicion of AOM, pneumatic otoscopy is necessary to differentiate AOM from myringitis.
-
Purulent effusion behind a bulging tympanic membrane.
-
When the process advances, a perforation of the tympanic membrane may occur, which allows spontaneous drainage of pus from middle ear and the patient would generally experience rapid relief of the pain and fever. Nowadays, it is not unusual that the otologist sees the patient at this stage. During otoscopic examination, a yellowish pulsatile discharge is seen oozing through pinpoint perforation.
-
The discharge is initially purulent, though it may be thin and watery or bloody; pulsation of the otorrhea is common. Otorrhea from an acute perforation normally lasts 1–2 days before spontaneous healing occurs. Otorrhea may persist if the perforation is accompanied by mucosal swelling or polypoid changes.
2.6 Diagnosis
The diagnosis of AOM requires the presence of inflammation and pus in the middle ear, and acute onset of symptoms and sign of ear infection, i.e., earache, fever, irritability, poor feeding or vomiting, often associated with cough and rhinitis.
Diagnosis of acute otitis media (AOM) requires
-
1.
Symptoms of fever, otalgia, or irritability in young children
-
2.
Bulging of the tympanic membrane
-
3.
Erythema and hypervascularisation
Pneumatic otoscopy in AOM is very painful and must be avoided.
Otomicroscopy and otoendoscopy are helpful to differentiate AOM from acute bullous myringitis and other differential diagnosis (Fig. 2.3).
Tympanometry is helpful but must still be used in conjunction with compatible history.
Tympanocentesis: Tympanocentesis is considered as the gold standard therapy in AOM; especially after failure of second course of antibiotics, the aspirate provides material for the culture to direct antibiotherapy [4, 7].
Laboratory studies: Not needed for the diagnosis. However one study by Pichichero and Almudevar indicated that the presence of AOM caused by non-typeable H. influenzae, as well as the disease’s cure, can be determined from serum levels of S100A12 protein and interleukin-10 (IL-10) [21].
Imaging studies: Radiologic studies are generally unnecessary in uncomplicated AOM. Role of CT-Scan or MRI in the diagnosis of complications will be presented in a dedicated chapter (see Chap. 9).
2.7 Differential Diagnosis of AOM
-
Myringitis - inflammation of the tympanic membrane. This is usually associated with viral infections of the upper respiratory tract.
-
Acute bullous myringitis , (rare) - caused by Mycoplasma pneumonia, and causes severe localized otalgia without systemic symptoms and without middle ear effusion. The bullae or blebs may contain serous or hemorrhagic fluid and pain is relieved by puncturing the bleb without opening the eardrum (Fig. 2.3).
Fig. 2.3 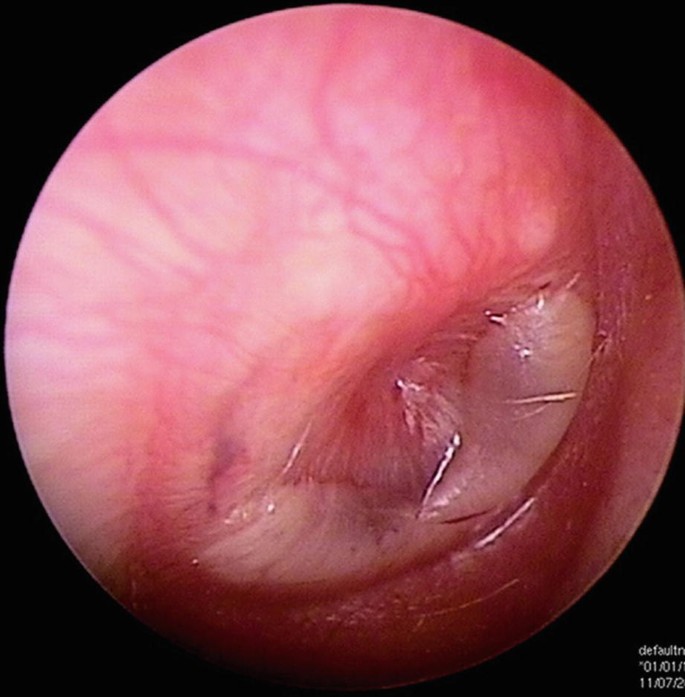
Right ear otoscopy in a child presented with ear pain and fever showing bullous myringitis
-
Otitis externa, rare in children, usually occurs after swimming and is associated with severe pain and tragal tenderness. The child is usually afebrile with good general condition.
-
Dental pain
-
Acute viral pharyngitis

2.8 Management of AOM
2.8.1 General Concepts
-
1.
Routine use of antibiotics, especially in children 2 years and older, is not indicated because of the high rate of spontaneous resolution. Watchful waiting for 48 to 72 hours before initiating antibiotic therapy if symptoms are manageable with analgesics.
-
2.
The goals of antibiotic treatment of AOM are to:
-
• Produce fast clinical cure
-
• Prevent complications
-
• Eradicate bacteria from middle ear and thus reduce recurrence rate
-
-
3.
The most important factor is not to prescribe antibiotics for inappropriate diagnosis of AOM. Inappropriate use of antibiotics have caused adverse effects and increased antibiotic resistance.
-
4.
S. pneumonia has the lowest spontaneous resolution rate and is associated with more serious complications, it is essential to ensure optimal coverage for this organism.
-
5.
Observation alone is not suitable for high-risk or vulnerable populations such as indigenous children in remote settings or those with cleft palate, Down syndrome or immunodeficiency syndromes [2]
-
6.
Children younger than 6 months of age with AOM must be treated with antibiotics without the initial observational waiting time.
-
7.
Oral antibiotic treatment of a first AOM episode occurring during infancy does not affect the number of AOM recurrences.
-
8.
Persistent otitis media infections can arise from the failure to completely eradicate the original bacterial infection, the presence of biofilms, or intracellular bacterial infection of the middle ear mucosal cells, particularly mucus-secreting cells [22].
2.8.2 Guidelines
-
Every nation has its own guidelines of therapy recommendations, there is no universal guidelines. In general, guidelines are more applied by the young generation of physicians than by the older ones.
-
Most guidelines use the same diagnostic criteria, and propose watchful waiting in mild-moderate scenarios
-
The routine prescription of antibiotics for AOM ranges from 31% in the Netherlands to 98% in the USA and Australia.
-
Current American Academy of Pediatrics Guidelines for the treatment of AOM recommend:
-
that antibiotics should be used in children aged over 6 months when unilateral or bilateral AOM is severe (moderate to severe otalgia, otalgia lasting at least 48 h, temperature 39 °C) [23].
-
Antibiotics should also be prescribed if AOM is not severe but bilateral in a child aged 6–23 months.
-
In the case of non-severe unilateral AOM in a child aged 6–23 months, or non-severe unilateral/bilateral AOM in a child aged 24 months or older, antibiotics may be prescribed or observation offered; if observation is chosen, a mechanism should be in place to give antibiotics if symptoms do not improve in 48–72 h.
-
-
For rAOM, insertion of ventilation tubes should be considered if rAOM is associated with a persistent middle ear effusion between AOM attacks [24]
-
No prophylactic antibiotics for rAOM
2.8.3 Choice of Antibiotics
-
(a)
Amoxicillin is the first-line agent for the treatment of acute otitis media in children [5,6,7]; as most S. pneumoniae and H. influenzae are still susceptible [9]. If severe signs and symptoms persisted more than 2–3 days of amoxicillin use, then antibiotics should be changed to amoxicillin-clavulanate, or second generation or third generation cephalosporin [5].
-
(b)
If there is a recent history of amoxicillin use in the last 30 days, in recurrent cases or if the patient has conjunctivitis, then Beta lactamase coverage should be added [5, 7]. Cefdinir, cefuroxime and ceftriaxone should be considered in case of penicillin allergy [5], macrolides can be used in allergic cases as well [5, 9].
2.8.4 The Duration of Antibiotherapy
The duration of antibiotherapy is for 10 days for children below 2 years and 5–7 days for older children [5,6,7]. Children who present with perforation of the tympanic membrane should receive 10 days of antibiotic therapy.
Antibiotherapy of 10 Days Duration
-
1.
< 24 months old
-
2.
Perforated eardrum
-
3.
Recurrent AOM
-
4.
Failure of first line agents
Clinicians should reevaluate a child whose symptoms have worsened or that did not respond to the initial antibiotic treatment within 48–72 h and change the treatment.
It is not indicated to give antihistamine, decongestants or corticosteroids [2, 6].
2.8.5 Tympanocentesis
Few days after the start of the therapy, when the medical treatment is ineffective and the purulent effusion is under pressure, tympanocentesis is the solution because it permits an efficient drainage and immediate relief of symptoms and allows identification of the causative bacteria and its sensitivity. Also it is found that tube insertion reduces the recurrence rates of AOM [6, 7, 9], and improves the quality of life of children in terms of hearing and speech [5]. Actually one of the main factors behind the rAOM is the lack of good control of the first episode of AOM when the ear is left with an important residual middle ear effusion.
Tympanocentesis should be performed in the following AOM patients [25]:
-
Patients in whom adequate antimicrobial treatment has failed to control the infection
-
Patients who have a complication that requires a culture for adequate therapy
-
Neonates younger than 6 weeks (more likely to have an unusual invasive pathogen)
-
Patients who are immunosuppressed or immunocompromised
2.8.6 Anti-GERD
No sufficient data is present about using anti-reflux in rAOM [15] but some studies found that controlling GERD by anti-reflux medication can decrease rAOM and tympanostomy tube insertion rates.
2.8.7 Follow up
Normally the symptoms of AOM should resolve within 72 hours of initiating antibiotic treatment. However, middle ear effusion may persist for up to 1 month in 50% and up to 3 months in 25% of patients despite bacteriological cure. Therefore, persistence of middle ear fluid after full course of antibiotic therapy for AOM is not an indication for continued antimicrobial therapy. Follow up should be done after 4–8 weeks for uncomplicated cases of AOM to look for persistent middle ear effusion [6] (See Chap. 3). In general, AOM is a symptomatic disease and screening is not indicated [8].
2.9 Prevention of Recurrent AOM
Recurrent otitis media (rAOM) is defined as 3 or more episodes of AOM over the preceding 6 months, or 4 or more episodes in the last year. Under these circumstance, prevention of further attacks is desirable. Modification of risk factors, when possible, are of benefit. Breast feeding has a protective effect at least for the first 6 months and preferentially to be continued for the first year [5]. Elimination of smoking from the environment and avoidance of pacifiers have been shown to help reduce the recurrence of AOM. Vaccinations are other preventive measures [3, 5, 7, 26]. PCV7 has been shown to decrease AOM rates and tympanostomy tube placement for recurrent diseases [26] and is more effective if given during infancy [6]. It can prevent the early episodes of the disease and prevent the mucosal changes, that make the ear more susceptible to infection by other S. pneumoniae serotypes, that are not covered by PCV [19]. Some studies found that Live Attenuated Influenza Vaccine (LAIV) has decreased the incidence of AOM by 12.4%, if given between 6 and 71 months of age [7], but others found influenza vaccine is not effective in preventing AOM [6]. The American Academy of Pediatrics recommends administration of pneumococcal conjugate vaccine and influenza vaccine for all children [5].
Despite promising results, there is still a real concern about the long-term benefit from vaccination. A recent study has highlighted concerns regarding the increasing incidence of AOM-related complications. Following the introduction of vaccinations, AOM-related complications, including mastoiditis and other intracranial complications, diminished considerably, however, they returned to pre-vaccination levels after a few years [27]. Antibiotic prophylaxis has only minimal effects on recurrent otitis media, decreasing recurrence by approximately one episode per year. Antibiotic prophylaxis is no longer recommended in the management of rAOM.
As the child grows older, the incidence of recurrence declines.
2.10 Acute Otitis Media in Adult
AOM in adult is:
Much less common than in children: the incidence in adults is widely quoted as 0.25% per year.
-
Mostly bacteria and mainly Haemophilus Influenzae is the dominating germ; S. pneumoniae is less involved since vaccination
-
Otalgia is a more common presenting symptom and may occur without fever or hearing loss and may be the only presenting feature.
-
Complications are rare
Immediate antibiotic prescription to an adult with AOM:
-
To patients who are systemically unwell but do not require admission.
-
To those at high risk of complications because of significant heart, lung, kidney, diabetes, liver or neuromuscular disease, or to those who are immunocompromised.
2.11 Complications of Acute Otitis Media
Tympanic membrane perforation occurs in 7% of the cases and tends to heal in 98% of cases in the first 1–2 weeks [7]. Other complications and sequelae of AOM are important causes of preventable hearing loss, particularly in developing countries. Meningitis (pneumococcal origin of AOM is the most important pathogen linked to meningitis [7]), facial palsy and coalescent mastoiditis. Also systemic complications could occur such as bacteremia, septic arthritis, or bacterial endocarditis.
2.11.1 Facial Paralysis
Incidence: Nowadays , facial paralysis is a very uncommon complication of AOM with an estimated incidence of 0.005%; it was not so rare in the pre-antibiotic era [28].
Mechanism of facial paralysis: It is thought that facial paralysis in AOM is caused by spread of infection under pressure from the middle ear cavity into the facial nerve sheath with resultant intrafallopian inflammatory edema and consequent ischemia and neuropraxia. Presumably this occurs either through [1] preexistent bony dehiscences [2], physiologic canaliculi between the middle ear and the Fallopian canal, or [3] vascular connections between the Fallopian canal and the mastoid air cells.
Site of involvement: the exact site of the inflammatory involvement causing facial palsy in AOM is difficult to determine, but through the topographic tests it was observed that the site of involvement is infrageniculate in 90% of cases and suprageniculate in 10% [29].
Treatment: it is a consensus among most otologists that the conservative approach for facial palsy in AOM is the most appropriate one: it consists of antibiotherapy and myringotomy with tube placement; steroids may be added. In certain cases when the facial recovery is delayed and the patient keeps a grade VI paralysis after 3 weeks of treatment, imaging is indicated to rule out associated pathologies.
Unlike in CSOM, facial palsy in AOM presents, in most cases, an excellent prognosis with the adequate treatment.
2.12 Acute Coalescent Mastoiditis in Children
Acute coalescent mastoiditis is the most common suppurative complication of AOM in young children.
In many cases, this may be the presenting complaint of children with AOM. Early diagnosis and adequate treatment of this condition are essential to avoid fatal complications. In the era of antibiotics, coalescent mastoiditis has an incidence of <1% in patients with AOM [30]. The incidence and the clinical picture of mastoiditis have changed greatly with the advent of antibiotics when reliance on antibiotics alone leads to less vigilance in diagnostic and therapeutic interventions; “this has led to a generation of ENT specialists and pediatricians trained in an atmosphere of complacency in the treatment of AOM; recently, a delay is noted in the recognition of mastoiditis and its related intracranial complications in children and in the initiation of the appropriate therapy” [31].
Despite the use of advanced imaging modalities, antibiotics, and microsurgical procedures, the resulting mortality of intracranial otogenic complications in acute coalescent mastoiditis remains of approximately 10% [32].
2.12.1 Definitions
Acute mastoiditis is subdivided according to the pathologic stage:
-
Acute mastoiditis with periostitis (also called incipient mastoiditis) is defined by the presence of purulent material only in the mastoid cavity.
-
Acute coalescent mastoiditis (also called “acute mastoid osteitis”) is defined by the acute form of destruction of the thin bony septae between mastoid air cells. It may be followed by the formation of abscess cavities and the dissipation of pus into adjacent areas.
-
Masked mastoiditis (also called subacute mastoiditis) refers to a low-grade, subacute, but persistent infection in the middle ear and mastoid with destruction of the bony septae between air cells. It occurs in patients with persistent middle ear effusion or recurrent episodes of AOM without sufficient antimicrobial therapy.
2.12.2 Pathogenesis
The clinical course of AOM is often short and self limited because of the host’s immune system defense, the infection-resistant nature of the mucosal linings, and the susceptibility of the major organisms to oral antibiotics.
Approximately 1–5% of untreated or inadequately treated patients with AOM may experience complications. Prior to these complications, alarming signs and symptoms may appear: severe earache and/or headache; vertigo; chills and fever; and meningeal symptoms or signs [33].
Acute coalescent mastoiditis is a rare complication of severe AOM. During an episode of severe AOM, the mucosa in the epitympanum becomes hyperplastic, it blocks the aditus ad antrum leading to entrapment of purulent material within the mastoid air cells. As pus and granulations accumulate under pressure, mastoid air cells bony septation become subjected to pressure and osteitic necrosis; small air cells coalesce into larger ones by bony septation necrosis with a resultant coalescence of mastoid air cells called “acute coalescent mastoiditis” (Fig. 2.4).

Pathogenesis of coalescent mastoiditis
Essentially, coalescent mastoiditis is an empyema of the temporal bone. Pus may leave the area of coalescence by direct extension, thrombophlebitis, or through preformed bony pathways. If the outer cortical bone is violated a postauricular, subperiosteal abscess is formed, causing an ear protrusion downward and outward. However, if the inner cortical table is violated, an intracranial complication can occur: sigmoid sinus thrombosis, meningitis, epidural or subdural abscess, or brain abscess.
Subperiosteal abscess is seen in nearly 50% of patients diagnosed with coalescent mastoiditis [34,35,36,37]. If not recognized at its early stage, the coalescent mastoiditis could be the cause of fatal intracranial complications. The incidence of intracranial complications has been reported between 6.8% and 23% when acute mastoiditis is diagnosed [38, 39] (see Chap. 9).
2.12.3 Risk Factors
As with most infectious processes, host and microbial factors have to be considered when evaluating acute mastoiditis (Fig. 2.5).

Risk factors of acute coalescent mastoiditis
2.12.3.1 Host Factors
Age < 2 years: Most children presenting with acute coalescent mastoiditis are younger than 2 years of age and have little history of otitis media. At this age, the immune system is relatively immature, particularly with regard to its ability to respond to challenges from polysaccharide antigens.
Incomplete mastoid pneumatization: Mastoid antrum is the only mastoid air cell present at birth. Mastoid pneumatization starts shortly after birth, but it is not active during the first two years of life. After the age of 2 years, mastoid pneumatization becomes very active and is almost complete at the age of 10 years. The antrum and the mastoid air cells are lined with respiratory epithelium that becomes oedematous due to inflammation and infection. Non-pneumatized mastoid is more prone to coalescent mastoiditis because the narrow aditus ad antrum can be easily blocked by inflammatory epitympanic mucosa during an episode of severe AOM.
Other host factors, such autism spectrum disorders , have shown an increased likelihood of developing middle ear infections and more than two-fold greater predisposition for coalescent mastoiditis [40].
2.12.3.2 Microbial Factors
The most common etiologic agent causing mastoiditis is Streptococcus pneumoniae, followed by Haemophilus influenzae and group A Streptococcus pyogenes (GAS). Each of these bacteria has invasive forms and is recovered most often from children presenting with acute mastoiditis.
Reported pathogens in mastoiditis include the following [41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60]
-
Streptococcus pneumoniae—Most frequently isolated pathogen in acute mastoiditis, prevalence is approximately 25%
-
Group A beta-hemolytic streptococci
-
Staphylococcus aureus
-
Streptococcus pyogenes
-
Haemophilus influenzae
Several case series show that 33–81% of patients diagnosed with acute coalescent mastoiditis had been treated with appropriate first-line agents for AOM prior to development of mastoiditis, suggesting that antibiotics administered for AOM treatment do not eliminate the risk of developing this complication [61].
2.12.4 Epidemiology (Figs. 2.6 and 2.7)
Today, the estimated incidence of coalescent mastoiditis is less than 0.01% of AOM [55].

Epidemiology of acute coalescent mastoiditis

The evolution of incidence of acute coalescent mastoiditis over time
Acute mastoiditis is a disease of the very young. Most patients present younger than the age of 2 years, with a median age of 12 months. However, it can occur in persons of any age. Some fear that untreated otitis media increases the risk of acute mastoiditis and is the cause of higher incidences in developing countries and very young children [62, 63].
In the pre-antibiotic era, up to 20% of cases of AOM were complicated by acute mastoiditis and were frequently associated with more severe intracranial complications [64].
The advent of sulfonamides in the 1930s and 1940s decreased hospitalizations for AOM by 50% and mastoidectomies by 80% [65]. This reduction was amplified with the introduction of penicillin and other early antibiotic regimens directed toward common pathogens of the middle ear [66]. The reported incidences decreased from 0.4% in 1959 [67] to 0.004% in the 1980s [68].
Since 1989, however, several investigators have documented an epidemiologic resurgence of acute mastoiditis in children [64, 67,68,69,70,71]. Some studies have incriminated the common practice of administering broad-spectrum antibiotics in increasing the prevalence of resistant bacteria that can spread the infection into the mastoid bone [72,73,74,75,76].
The incidence of acute mastoiditis in children <2 years of age exhibited a dynamic pattern from 1999 to 2008: a significant decline early after introduction of PCV-7 was followed by an increase in subsequent years to pre-PCV-7 levels.
A retrospective review of pediatric patients in Colorado found that the annual incidence of acute coalescent mastoiditis in children under age 2 years dropped from 11.0 per 100,000 population in 2001, a year after PCV-7 was introduced, to 4.5 per 100,000 population in 2003. By 2008, however, the incidence had again raised to 12 per 100,000 population [77].
Non-PCV-7 pneumococcal serotypes and increased pneumococcal antibiotic resistance may be responsible for this increase in incidence in comparison to pre-PCV-7 rates.
Although becoming less common, coalescent mastoiditis remains even nowadays a subject of first interest and concern for pediatricians and otolaryngologists .
2.12.5 Clinical Features
Approximately 40% of children with acute mastoiditis had a positive history of previous AOM, and 50% of patients having coalescent mastoiditis had received antibiotics before presentation. However, the absence of AOM (current or recent) does not exclude the diagnosis of coalescent mastoiditis because it may take place very rapidly during the onset of an AOM episode.
The diagnosis of acute mastoiditis is usually made clinically in children with characteristic findings. The most frequent diagnostic criteria include (Figs. 2.8 and 2.9):
-
1.
Irritability and lethargy
-
2.
Fever
-
3.
Otalgia
-
4.
Postauricular erythema, tenderness, swelling, fluctuance, or mass
-
5.
Protrusion of the auricle
-
6.
Oedema and sagging of the posterosuperior wall of the external auditory canal
-
7.
Nipplelike protrusion of the central tympanic membrane, usually oozing pus

Main clinical features of acute coalescent mastoiditis

Signs and symptoms of acute coalescent mastoiditis in order of frequency: Lethargy/malaise (96%); Abnormal tympanic membrane (82%); Postauricular erythema, postauricular tenderness, and/or protrusion of the pinna (80%); Fever (76%); Narrowing of the external auditory canal (71%); Ear pain (67%); Otorrhea (50%)
Fever is a nonspecific sign but it is sensitive and may be predictive of complications or the need for surgical intervention. High-spiking “picket-fence” fever may be indicative of sigmoid sinus thrombophlebitis.
Examination of the tympanic membrane: Tympanic membrane findings consistent with AOM (e.g., bulging, marked erythema or acute perforation with purulent otorrhea in the absence of otitis externa) are often present.
A normal-appearing tympanic membrane usually (but not invariably) excludes mastoiditis.
Laboratory Features: The peripheral white blood cell count in children with acute coalescent mastoiditis is usually elevated, often with a left shift. The erythrocyte sedimentation rate and C-reactive protein are also elevated.
Immunologic evaluation may be warranted in children with recurrent episodes of AOM leading to mastoiditis.
2.12.6 CT-Imaging
The CT Imaging plays a determinant role in confirming the diagnosis and in orienting plans for management. CT allows differentiation between a mere condensation of the mastoid system in common acute purulent otitis media and disruption of the intercellular bone septa that is indicative for coalescent mastoiditis. Also CT-Scan may confirm the diagnosis in children without characteristic clinical findings.
CT findings in children with acute coalescent mastoiditis include the following:
-
1.
Fluid and/or mucosal thickening in the middle ear and mastoid condensation images: this is a nonspecific finding that occurs early in the course; it is often seen in children with AOM with mastoiditis and may even be observed as an incidental finding in asymptomatic children.
-
2.
Loss of definition of the bony septae that define the mastoid air cells: this finding is diagnostic of coalescent mastoiditis (Fig. 2.10).
-
3.
Destruction or irregularity of the mastoid cortex (Fig. 2.11).
-
4.
Periosteal thickening, disruption of the periosteum, subperiosteal abscess (Figs. 2.10 and 2.11).

Axial non injected CT-image of a 2 y-o boy with acute otitis media on both sides. Mastoid cells are opacified on the right side (single arrow), the bony septa are preserved: non specific sign of mastoiditis. On the left side, the bony septa of the mastoid are resorbed (double arrow): sign of coalescent mastoiditis. Associated large retroauricular soft tissue swelling (between the white arrows) with protrusion of the auricle (empty arrow), but no lysis of the mastoid cortex. Note the diffuse condensation of the ethmoidal (E) and sphenoidal (S) sinusses

Axial non injected CT-image of another 1½ year child, with acute otitis media and retroauricular swelling. (a) The mastoid is not well developed, atticoantral and mastoid cell condensations. (b) destruction of the mastoid cortex (between the two arrows) and a voluminous extratemporal soft tissue thickening (*): subperiosteal abscess
In case of suspected complications, CT has preferentially to be done with contrast injection or should be followed by MRI, dependent on age and compliance of the patient.
2.12.7 Differential Diagnosis
The differential diagnosis of acute coalescent mastoiditis includes other causes of postauricular inflammation or swelling:
-
Periauricular cellulitis related to otitis externa: This is a common mimicker of mastoiditis. Severe pain over the tragus and pinna differentiates this entity from mastoiditis.
-
Perichondritis of the auricle: Characterized by swelling and erythema of the pinna and may spread to the periosteum of the postauricular area. In contrast to acute mastoiditis, the postauricular crease is preserved, and the tympanic membrane appears normal.
-
Tumoral : Benign and malignant tumors of the mastoid bone (e.g., aneurysmal bone cyst, acute lymphocytic leukemia, Langerhans cell histiocytosis) may have clinical features similar to mastoiditis.
2.12.8 Complications
Complications of coalescent mastoiditis are related to the spread of infection from the middle ear or mastoid to contiguous structures. In some cases, the complication is the presenting complaint.
In most case series, the rate of complications is approximately 10–20% (range 7–60%) [41, 42, 46, 47, 57, 58, 78, 79]. In a multicenter study, S. pyogenes was associated with the highest rate of complications at presentation (50%) and S. aureus with the highest rate of complications during hospitalization (31%) [42].
2.12.8.1 Extracranial Complications of Acute Coalescent Mastoiditis Include (See also Chap. 9)
2.12.8.1.1 Subperiosteal Abscess—(Fig. 2.12)
Signs of subperiosteal abscess include erythema, fluctuance, and a tender mass overlying the mastoid bone. Subperiosteal abscess occurs in about 50% of cases of acute mastoiditis [79].

Coalescent mastoditis with subperiosteal abscess (a) schematic drawing (b) T1 weighted MRI image after i.v. injection of gadolinium showing the coalescent mastoiditis (M) with exteriorisation of the purulent material in the subperiosteal space (SPA) through a large cortical defect. An intracerebral abscess (ICA) is another concomitant complication in this case
2.12.8.1.2 Facial Nerve Palsy
Facial nerve palsy can result from infectious neuritis or inflammatory compression of the facial nerve as it traverses the temporal bone.
2.12.8.1.3 Labyrinthitis
Clinical features of labyrinthitis include tinnitus, hearing loss, nausea, vomiting, dizziness, vertigo, and nystagmus. Labyrinthtitis is caused by spread of bacteria from the middle ear to the labyrinthine space through the round window membrane. More often the involvement of the labyrinth is a reaction to bacterial exotoxins rather than bacterial invasion. This so-called otogenic labyrinthitis is unilateral in contrast to meningogenic labyrinthitis which is usually bilateral. MRI is the study of choice and shows that the endo- and perilymphatic spaces are filled with purulent material (Fig. 2.13a). The inner ear enhances on the T1-weighted images performed after gadolinium injection (Fig. 2.13b).

Axial IRM images of a coalescent mastoiditis complicated by labyrinthitis (a) T2 weighted axial image showing purulent material in the mastoid as being slightly hyperintense (*). The endolymphatic/perilymphatic spaces of the cochlea (short arrow) and the semicircular canals (long arrow) are hypointens, as the content of the IAC (white empty arrowhead) in comparison to the normal left side with hyperintense fluid in the cochlea (short dashed arrow), the semicircular canals (long dashed arrow) and the IAC (dashed arrowhead). (b) on T1 weighted image post Gd and fatsat, the purulent material in the mastoid does not show any enhancement (*), but the whole right labyrinth shows an important contrast uptake, also the ICA, in comparison to the normal left side (same annotations for the different anatomic structures as in (a)
2.12.8.1.4 Petrous apicitis
Infection in the mastoid may spread to other parts of the skull, resulting in osteomyelitis. Osteomyelitis of the petrous apex may be associated with facial nerve palsy or Gradenigo syndrome (i.e., otorrhea, retro-orbital pain, ipsilateral abducens [sixth cranial nerve] palsy, and possibly other cranial nerve deficits) .
2.12.8.1.5 Bezold abscess
A Bezold abscess is a neck abscess located in the sheath of the sternocleidomastoid muscle. Clinical features of Bezold abscess include swelling and tenderness below the mastoid process and under the sternocleidomastoid muscle.
2.12.8.2 Intracranial Complications of Acute Coalescent Mastoiditis
Intracranial complications occurs in about 6% to 23% of cases with coalescent mastoiditis [38, 39, 79]. Altered mental status, neurologic deficits including cranial nerve palsy, high fever, neck stiffness, seizures, and severe headache should be concerning for intracranial disease.
2.12.8.2.1 Meningitis
2.12.8.2.2 Temporal Lobe or Cerebellar Abscess
Increasing temporoparietal headache, near the affected ear, is often the only indication of otogenic brain abscess formation [33] (See Figs. 9.17–9.20, Sect. 9.9).
2.12.8.2.3 Epidural or Subdural Abscess
Although rarely seen, among all intracranial complications of middle ear disease, epidural abscess formation is the most common [80] (See Fig. 9.19, Sect. 9.9).
2.12.8.2.4 Venous Sinus Thrombosis
Sinus thrombosis is the least frequent one [81]. Sigmoid sinus thrombosis has become increasingly uncommon, whereas in the pre-antibiotic era this complication was mortal in over 90% of the cases [81, 82].
Patients may present with otorrhea, otalgia, neck pain, fever, and chills [83]. But often presenting signs and symptoms are subtle or nonspecific and not in proportion to the magnitude of the problem, leading to a common delay in diagnosis [84, 85]. Consequently, a high index of suspicion is actually required to make the diagnosis [81, 82].
Imaging studies should be performed in all coalescent mastoiditis patients with pain or vertigo that is not rapidly resolving after appropriate antibiotic treatment [82] (See Figs. 9.14 and 9.15, Sect. 9.9). The therapeutic strategy is a point of debate, and ranges from internal jugular vein ligation, anticoagulation therapy, to the administration of less conventional antibiotic therapy [86].
2.12.9 Management
2.12.9.1 General Concept
The treatment of acute coalescent mastoiditis depends upon the stage and presence or absence of complications.
-
Antimicrobial therapy and drainage of the middle ear and mastoid are the cornerstones of therapy for coalescent mastoiditis.
-
The rates of mastoidectomy in treatment of acute coalescent mastoiditis vary greatly in the range between 9 and 88%, as is reported in the literature [62]
-
Antimicrobial therapy alone may fail to prevent the development of complications of acute coalescent mastoiditis. In a series of 223 patients, 8.5% developed complications during antimicrobial therapy [42].
-
The use of single, high-dose intravenous (IV) steroids is warranted to decrease mucosal swelling and promote natural drainage through the aditus ad antrum into the middle ear.
-
Mastoidectomy may be warranted if one or more of the following are present
-
Postauricular fluctuant, mass, or swelling (suggesting subperiosteal abscess)
-
Cervical fluctuance (i.e., Bezold abscess).
-
Imaging studies with evidence of rim-enhancing fluid collection, mastoid air cell coalescence, cortical bone erosion, or intracranial involvement.
-
High-spiking “picket-fence” fever (may indicate sigmoid sinus thrombophlebitis)
-
Neurologic signs (e.g., facial weakness, meningeal signs, focal deficits, altered level of consciousness, seizures); consultation by a neurosurgeon is also indicated.
-
2.12.9.2 Management of Uncomplicated Coalescent Mastoiditis
-
Uncomplicated acute coalescent mastoiditis is treated with intravenous (IV) antimicrobial therapy and myringotomy with placement of a tympanostomy tube
Numerous patients with uncomplicated mastoiditis respond well to conservative treatment. Unfortunately, we are still not able to predict which patient will have a poor response or which will develop severe complications.
-
Patients should be monitored daily for clinical response. If there is no clinical improvement in 48 h, mastoidectomy should be done .
2.12.9.3 Management of Complicated Mastoiditis
Acute coalescent mastoiditis with extracranial or intracranial complications is usually treated with IV antibiotics, myringotomy with placement of a tympanostomy tube, and mastoidectomy.
When a subperiosteal abscess is noted at presentation, some otologists favor postauricular aspiration as the initial procedure [87].
2.12.9.4 Antimicrobial Therapy
Because of the diversity of causative organisms in acute coalescent mastoiditis and the growing resistance of bacteria to the various antibiotics, all means to obtain a sample for culture and sensitivity prior to antibiotic treatment should be taken.
Empiric antimicrobial therapy for children with acute mastoiditis without a history of recurrent AOM or recent antibiotic administration should provide coverage for the most frequent bacterial pathogens: S. pneumoniae (including multiply resistant S. pneumoniae), S. pyogenes, and S. aureus (including methicillin-resistant S. aureus).
In a child with either no previous history of AOM or a history of a remote episode (i.e., >6 months before), empiric antimicrobial therapy with vancomycin alone (60 mg/kg per day divided every 6 h with a maximum dose of 4 gm/day) should be started until microbiologic results are available.
For children with a history of recurrent AOM (most recent episode within 6 months) or recent antibiotic use, adequate coverage for gram-positive and gram-negative pathogens usually entails combination therapy. Antibiotics active against P. aeruginosa should be included in the empiric regimen.
Upon diagnosis of the acute mastoiditis, initial antimicrobial is given intravenously. The patient can be switched to oral antibiotics when improved clinically and culture sensitivity days and oral antibiotics to complete a 4 weeks course.
2.12.9.5 Surgical Treatment
Early drainage interrupts the pathologic process and prevents complications [42].
2.12.9.5.1 Myringotomy
Myringotomy permits drainage of the mastoid if the aditus ad antrum is not blocked. Tympanostomy tubes permit drainage over a longer duration. Postoperatively, antibiotic/steroid drops are used to keep the tube patent and to reduce middle ear swelling. Antibiotic/steroid drops are continued until the otorrhea ceases.
2.12.9.5.2 Mastoidectomy
Mastoidectomy is performed to remove the mastoid infection, open the aditus ad antrum, and provide external drainage. Indications for mastoidectomy may include:
-
Computed tomography evidence of coalescent mastoiditis (regardless of other clinical features)
-
Subperiosteal abscess
-
Other suppurative complications of acute mastoiditis
-
Progression or persistence of fever, ear pain, postauricular swelling, or drainage despite parenteral antimicrobial therapy and tympanocentesis/myringotomy
2.12.9.6 Treatment Response
The response to treatment of acute mastoiditis is monitored through serial examination of the postauricular region, the external auditory canal, and the tympanic membrane and through measurement of inflammatory markers (WBC count and CRP).
In patients with acute mastoiditis, the above signs and symptoms should start to improve 48 hours after tympanocentesis/myringotomy and initiation of adequate antimicrobial therapy. Mastoidectomy is indicated in children who do not demonstrate adequate treatment response after 48 h. In this condition, imaging control of the temporal bone with intravenous contrast is indicated preoperatively.
2.12.9.7 Prevention
Early and adequate treatment of AOM reduces the risk of developing mastoiditis. Early recognition of the coalescent mastoiditis and its prompt treatment will decrease the risk of developing complications of mastoiditis.
2.12.10 Summary of Acute Coalescent Mastoiditis
Acute coalescent mastoiditis is a complication of AOM in which purulent material accumulates within the mastoid cavity. As the pressure increases, the bony septae between the mastoid air cells may be destroyed (coalescent mastoiditis), abscess cavities may form, and the purulent material may progress into adjacent areas.
Characteristic features of coalescent mastoiditis include postauricular abnormalities (tenderness, erythema, swelling, fluctuance, mass and protrusion) of the auricle; most patients also have fever and ear pain.
The diagnosis of acute coalescent mastoiditis is usually made clinically in children with characteristic examination findings. Imaging is necessary to confirm the diagnosis and evaluate suspected complications.
Treatment requires empiric antimicrobial therapy and drainage of pus from the middle ear and mastoid cavity.
Conclusion
AOM remains a common pathology for children even in developed countries. Its accurate diagnosis is simple and relies on adequate otoscopy. In nowadays practice, presumptive or confused diagnosis is inacceptable. The correct evaluation of the middle ear under perfect conditions during the presenting episode must be the rule. Antibiotics and paracentesis are the valuable means of treatment.
Strict follow up when the child becomes asymptomatic is of the utmost importance in order to evaluate residual effusions, avoid recurrences, complications and sequelae. For these objectives, the positive collaboration between family physicians, pediatrics and otologists is a major disciplinary measure to implement for a better outcome.
References
Bhutta MF. Epidemiology and pathogenesis of otitis media: construction of a phenotype landscape. Audiol Neurootol. 2014;19(3):210–23. https://doi.org/10.1159/000358549. Epub 2014 May 10. Review
Morris PS, Leach AJ. Acute and chronic otitis media. Pediatr Clin N Am. 2009;56(6):1383–99. https://doi.org/10.1016/j.pcl.2009.09.007. Review
Cunningham M, Guardiani E, Kim HJ, Brook I. Otitis media. Future Microbiol. 2012;7(6):733–53. https://doi.org/10.2217/fmb.12.38. Review
Pichichero ME. Acute otitis media: Part I. Improving diagnostic accuracy. Am Fam Physician. 2000;61(7):2051–6. Review
Siddiq S, Grainger J. The diagnosis and management of acute otitis media: American Academy of Pediatrics Guidelines 2013. Arch Dis Child Educ Pract Ed. 2015;100(4):193–7.
Wasson JD, Yung MW. Evidence-based management of otitis media: a 5S model approach. J Laryngol Otol. 2015;129(2):112–9.
Thomas JP, Berner R, Zahnert T, Dazert S. Acute otitis media – a structured approach. Dtsch Arztebl Int. 2014;111(9):151–9.
Schilder AG, Chonmaitree T, Cripps AW, Rosenfeld RM, Casselbrant ML, Haggard MP, Venekamp RP. Otitis media. Nat Rev Dis Primers. 2016;2:16063.
Atkinson H, Wallis S, Coatesworth AP. Acute otitis media. Postgrad Med. 2015;127(4):386–90. https://doi.org/10.1080/00325481.2015.1028872. Review
McCormick DP, Grady JJ, Diego A, Matalon R, Revai K, Patel JA, Han Y, Chonmaitree T. Acute otitis media severity: association with cytokine genepolymorphisms and other risk factors. Int J Pediatr Otorhinolaryngol. 2011;75(5):708–12.
Hafrén L, Kentala E, Järvinen TM, Leinonen E, Onkamo P, Kere J, Mattila PS. Genetic background and the risk of otitis media. Int J Pediatr Otorhinolaryngol. 2012;76(1):41–4.
Nokso-Koivisto J, Marom T, Chonmaitree T. Importance of viruses in acute otitis media. Curr Opin Pediatr. 2015;27(1):110–5.
Vergison A. Microbiology of otitis media: a moving target. Vaccine. 2008;26(Suppl 7):G5–10. https://doi.org/10.1016/j.vaccine.2008.11.006. Review
Heikkinen T, Chonmaitree T. Importance of respiratory viruses in acute otitis media. Clin Microbiol Rev. 2003;16(2):230–41. Review
Miura MS, Mascaro M, Rosenfeld RM. Association between otitis media and gastroesophageal reflux: a systematic review. Otolaryngol Head Neck Surg. 2012;146(3):345–52.
Kørvel-Hanquist A, Koch A, Niclasen J, Dammeye J, Lous J, Olsen SF, et al. Risk factors of early otitis media in the Danish National Birth Cohort. PLoS One. 2016;11(11):e0166465.
Gould JM, Matz PS. Otitis media. Pediatr Rev. 2010;31(3):102–16. Review
Ngo CC, Massa HM, Thornton RB, Cripps AW. Predominant bacteria detected from the middle ear fluid of children experiencing otitis media: a systematic review. PLoS One. 2016;11(3):e0150949.
Dagan R, Pelton S, Bakaletz L, Cohen R. Prevention of early episodes of otitismedia by pneumococcal vaccines might reduce progression to complex disease. Lancet Infect Dis. 2016;16(4):480–92.
Shawabka MA, Haidar H, Larem A, Aboul-Mahmood Z, Alsaadi A, et al. Acute otitis media- an update. J Otolaryngol ENT Res. 2017;8(2):00252.
Pichichero ME, Almudevar A. Serum cytokine biomarkers accurately predict presence of acute otitis media infection and recovery caused by Haemophilus influenzae. Int J Pediatr Otorhinolaryngol. 2016;83:200–4.
Massa HM, Cripps AW, Lehmann D. Otitis media: viruses, bacteria, biofilms and vaccines. Med J Aust. 2009;191(9 Suppl):S44.
American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004;113(5):1451–65.
Rosenfeld RM, Schwartz SR, Pynnonen MA, Tunkel DE, Hussey HM, Fichera JS, Grimes AM, Hackell JM, Harrison MF, Haskell H, Haynes DS, Kim TW, Lafreniere DC, LeBlanc K, Mackey WL, Netterville JL, Pipan ME, Raol NP, Schellhase KG. Clinical practice guideline: tympanostomy tubes in children. Otolaryngol Head Neck Surg. 2013;149(1 Suppl):S1–35.
Donaldson JD. Acute otitis media workup. In: Meyers AD, editor. Drugs & diseases, Otolaryngology and facial plastic surgery; 2017.
Levi JR, Brody RM, McKee-Cole K, Pribitkin E, O’Reilly R. Complementary and alternative medicine for pediatric otitis media. Int J Pediatr Otorhinolaryngol. 2013;77(6):926–31.
Daniel M, Gautam S, Scrivener TA, Meller C, Levin B, Curotta JJ. What effect has pneumococcal vaccination had on acute mastoiditis? Laryngol Otol. 2013;127(Suppl 1):S30–4.
Gaio E, Marioni G, de Filippis C, Tregnaghi A, Caltran S, Staffieri A. Facial nerve paralysis secondary to acute otitis media in infants and children. J Paediatr Child Health. 2004;40(8):483–6.
Yonamine FK, Tuma J, Silva RF, Soares MC, Testa JR. Facial paralysis associated with acute otitis media. Braz J Otorhinolaryngol. 2009;75(2):228–30.
Piegel JH, Lustig LR, Lee KC, Murr AH, Schindler RA. Contemporary presentation and management of a spectrum of mastoid abscesses. Laryngoscope. 1998;108(6):822–8.
Kuczkowski J, Mikaszewski B. Intracranial complications of acute and chronic mastoiditis: report of two cases in children. Int J Pediatr Otorhinolaryngol. 2001;60(3):227–37.
Kaftan H, Draf W. Intracranial otogenic complications: inspite of therapeutic progress still a serious problem. Laryngorhinootologie. 2000;79(10):609–15.
Dobben GD, Raofi B, Mafee MF, Kamel A, Mercurio S. Otogenic intracranial inflammations: role of magnetic resonance imaging. Top Magn Reson Imaging. 2000;11(2):76–86.
Glynn F, Osman L, Colreavy M, et al. Acute mastoiditis in children: Presentation and long term consequences. J Laryngol Otol. 2008;122(3):233–7., http://dx.doi.org/S0022215107009929 [pii].
Psarommatis I, Giannakopoulos P, Theodorou E, et al: Mastoid subperiosteal abscess in children: Drainage or mastoidectomy? J Laryngol Otol 126(12):1204-1208, http://dx.doi.org/10.1017/S0022215 112002332, 2012
Zevallos JP, Vrabec JT, Williamson RA, et al. Advanced pediatric mastoiditis with and without intracranial complications. Laryngoscope. 2009;119(8):1610–5., https://doi.org/10.1002/lary.20259.
Luntz M, Keren G, Nusem S, et al. Acute mastoiditis—revisited. Ear Nose Throat J. 1994;73(9):648–54.
Adams DJ, Susi A, Erdie-Lalena CR, Gorman G, Hisle-Gorman E, Rajnik M, Elrod M, Nylund CM. Otitis media and related complications among children with autism spectrum disorders. J Autism Dev Disord. 2016;46(5):1636–42. (ISSN: 1573-3432)
Geva A, Oestreicher-Kedem Y, Fishman G, et al. Conservative management of acute mastoiditis in children. Int J Pediatr Otorhinolaryngol. 2008;72:629.
Luntz M, Brodsky A, Nusem S, et al. Acute mastoiditis – the antibiotic era: a multicenter study. Int J Pediatr Otorhinolaryngol. 2001;57:1.
Katz A, Leibovitz E, Greenberg D, et al. Acute mastoiditis in Southern Israel: a twelve year retrospective study (1990 through 2001). Pediatr Infect Dis J. 2003;22:878.
Thorne MC, Chewaproug L, Elden LM. Suppurative complications of acute otitis media: changes in frequency over time. Arch Otolaryngol Head Neck Surg. 2009;135:638.
Benito MB, Gorricho BP. Acute mastoiditis: increase in the incidence and complications. Int J Pediatr Otorhinolaryngol. 2007;71:1007.
Bilavsky E, Yarden-Bilavsky H, Samra Z, et al. Clinical, laboratory, and microbiological differences between children with simple or complicated mastoiditis. Int J Pediatr Otorhinolaryngol. 2009;73:1270.
Oestreicher-Kedem Y, Raveh E, Kornreich L, et al. Complications of mastoiditis in children at the onset of a new millennium. Ann Otol Rhinol Laryngol. 2005;114:147.
Palma S, Fiumana E, Borgonzoni M, et al. Acute mastoiditis in children: the “Ferrara” experience. Int J Pediatr Otorhinolaryngol. 2007;71:1663.
Ruiz Díaz AI, del Castillo Martín F, Bilbao Garitagoitia A, et al. Acute mastoiditis: an increasing entity. An Esp Pediatr. 2002;57:427.
Roddy MG, Glazier SS, Agrawal D. Pediatric mastoiditis in the pneumococcal conjugate vaccine era: symptom duration guides empiric antimicrobial therapy. Pediatr Emerg Care. 2007;23:779.
Ho D, Rotenberg BW, Berkowitz RG. The relationship between acute mastoiditis and antibiotic use for acute otitis media in children. Arch Otolaryngol Head Neck Surg. 2008;134:45.
Mustafa A, Debry CH, Wiorowski M, et al. Treatment of acute mastoiditis: report of 31 cases over a ten year period. Rev Laryngol Otol Rhinol (Bord). 2004;125:165.
Baljosevic I, Mircetic N, Subarevic V, Markovic G. Acute mastoiditis in infants. Eur Arch Otorhinolaryngol. 2006;263:906.
Heslop A, Ovesen T. Severe acute middle ear infections: microbiology and treatment. Int J Pediatr Otorhinolaryngol. 2006;70:1811.
Nussinovitch M, Yoeli R, Elishkevitz K, Varsano I. Acute mastoiditis in children: epidemiologic, clinical, microbiologic, and therapeutic aspects over past years. Clin Pediatr (Phila). 2004;43:261–7. (ISSN: 0009-9228)
Ongkasuwan J, Valdez TA, Hulten KG, et al. Pneumococcal mastoiditis in children and the emergence of multidrug-resistant serotype 19A isolates. Pediatrics. 2008;122:34.
Stähelin-Massik J, Podvinec M, Jakscha J, et al. Mastoiditis in children: a prospective, observational study comparing clinical presentation, microbiology, computed tomography, surgical findings and histology. Eur J Pediatr. 2008;167:541.
Groth A, Enoksson F, Hultcrantz M, et al. Acute mastoiditis in children aged 0–16 years – a national study of 678 cases in Sweden comparing different age groups. Int J Pediatr Otorhinolaryngol. 2012;76:1494.
Anthonsen K, Høstmark K, Hansen S, et al. Acute mastoiditis in children: a 10-year retrospective and validated multicenter study. Pediatr Infect Dis J. 2013;32:436.
Ghadersohi S, Young NM, Smith-Bronstein V, et al. Management of acute complicated mastoiditis at an urban, tertiary care pediatric hospital. Laryngoscope. 2017;127(10):2321–7.
Lieberthal AS, Carroll AE, Chonmaitree T. The diagnosis and management of acute otitis media. Pediatrics. 2013;131:e964–99.
Psarommatis IM, Voudouris C, Douros K, Giannakopoulos P, Bairamis T, Carabinos C. Algorithmic management of pediatric acute mastoiditis. Int J Pediatr Otorhinolaryngol. 2012;76(6):791–6. (ISSN: 1872-8464)
Palma S, Bovo R, Benatti A, Aimoni C, Rosignoli M, Libanore M, Martini A. Mastoiditis in adults: a 19-year retrospective study. Eur Arch Otorhinolaryngol. 2014;271(5):925–31. (ISSN: 1434-4726)
Spratley J, Silveira H, Alvarez I, PaisClemente M. Acute mastoiditis in children. Review of the current status. Int J Pediatr Otolaryngol. 2000;56:33–40.
House HP. Otitis media; a comparative study of the results obtained in therapy before and after the introduction of the sulfonamide compounds. Arch Otolaryngol. 1946;43:371–8.
Goldstein NA, Casselbrant ML, Bluestone CD, et al. Intratemporal complications of acute otitis media in infants and children. Otolaryngol Head Neck Surg. 1998;119(5):444–54., http://dx.doi.org/S019459989 8003507 [pii].
Palva T, Pulkkinen K. Mastoiditis. J Laryngol Otol. 1959;73:573–88.
Lund FH. Acute and latent mastoiditis. J Laryngol Otol. 1989;103:1158–60.
Hoppe JE, Koster S, Bootz F, Neithammer D. Acute mastoiditis—relevant once again. Infection. 1994;22:178–82.
Ghaffar FA, Wordemann M, McCracken GH Jr. Acute mastoiditis in children: a seventeen-year experience in Dallas. Texas Pediatr Infect Dis J. 2001;20:376–80.
Dhooge IJ, Alberts FW, Van Cauwenberge PB. Intratemporal and intracranial complications of acute suppurative otitis media in children: renewed interest. Int J Pediatr Otorhinolaryngol. 1999;49:S109–14.
Antonelli PJ, Dhanani N, Giannoni CM, Kubilis PS. Impact of resistant pneumococcus on rates of acute mastoiditis. Otolaryngol Head Neck Surg. 1999;121:190–4.
Gliklich RE, Eavey RD, Iannuzzi RA, Camacho AE. A contemporary analysis of acute mastoiditis. Arch Otolaryngol Head Neck Surg. 1996;122:135–9.
Mathews TJ, Oliver SP. Bacteriology of mastoiditis. A five-year experience at Groote Schuur Hospital. J Laryngol Otol. 1988;102:397–8.
Meyerhoff WL, Gates GA, Montalbo PJ. Pseudomonas mastoiditis. Laryngoscope. 1977;87:483–92.
Ostfeld E, Rubinstein E. Acute gramnegative bacilliary infections of middle ear and mastoid. Ann Otol Rhinol Laryngol. 1980;89:33–6.
Halgrimson WR, Chan KH, Abzug MJ, Perkins JN, Carosone-Link P, Simões EA. Incidence of acute mastoiditis in Colorado children in the pneumococcal conjugate vaccine era. Pediatr Infect Dis J. 2014;33(5):453–7. (ISSN: 1532-0987)
Pang LH, Barakate MS, Havas TE. Mastoiditis in a paediatric population: a review of 11 years experience in management. Int J Pediatr Otorhinolaryngol. 2009;73:1520.
van den Aardweg MT, Rovers MM, de Ru JA, et al. A systematic review of diagnostic criteria for acute mastoiditis in children. Otol Neurotol. 2008;29:751.
Bizakis JG, Velegrakis GA, Papadakis CE, Karampekios SK, Helidonis ES. The silent epidural abscess as a complication of acute otitis media in children. Int J Pediatr Otorhinolaryngol. 1998;45(2):163–6.
Rocha JL, Kondo W, Gracia CM, Baptista MI, Büchele G, da Cunha CA, Martins LT. Central venous sinus thrombosis following mastoiditis: report of 4 cases and literature review. Braz J Infect Dis. 2000;4(6):307–12.
Keogh IJ, Hone SW, Colreavy M, Gaffney R. Sigmoid sinus thrombosis: an old foe revisited. Ir Med J. 2001;94(4):117–8.
See KC, Leong JL, Tan HK. Otogenic lateral sinus thrombosis – a case report. Ann Acad Med Singap. 2000;29(6):753–6.
Fritsch MH, Miyamoto RT, Wood TL. Sigmoid sinus thrombosis diagnosis by contrasted MRI scanning. Otolaryngol Head Neck Surg. 1990;103(3):451–6.
Ram B, Meiklejohn DJ, Nunez DA, Murray A, Watson HG. Combined risk factors contributing to cerebral venous thrombosis in a young woman. J Laryngol Otol. 2001;115(4):307–10.
Dallari S, Zaccarelli SC, Sintini M, Gatti G, Balli R. Acute mastoiditis with complications: a report of two cases. Acta Otorhinolaryngol Belg. 1997;51(2):113–8.
Lahav J, Handzel O, Gertler R, et al. Postauricular needle aspiration of subperiosteal abscess in acute mastoiditis. Ann Otol Rhinol Laryngol. 2005;114:323.
Nitsche MP, Carreño M. Antibiotics for acute otitis media in children. Medwave. 2015;15(Suppl 2):e6295. https://doi.org/10.5867/medwave.2015.6295.
Venekamp RP, Sanders SL, Glasziou PP, Del Mar CB, Rovers MM. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev. 2015;6:CD000219.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Mansour, S., Magnan, J., Nicolas, K., Haidar, H. (2018). Acute Otitis Media and Acute Coalescent Mastoiditis. In: Middle Ear Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-72962-6_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-72962-6_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-72961-9
Online ISBN: 978-3-319-72962-6
eBook Packages: MedicineMedicine (R0)