
Abstract
Reverse shoulder replacements (RSA) is known to have a high complication rate. Werner reported an overall complication rate of 50% for the first series of Delta III prosthesis (DePuy France, Saint Priest CEDEX, France) [1]. In a review of 10,884 shoulder arthroplasties performed in 2011–2013, the overall complication rates of RSA and anatomical total shoulder arthroplasty (TSA) were compared [2]. At 30 days, the overall complication rate for for both types of shoulder arthroplasties was 2.2%. The higher early complication rate of 3% for RSA compared with 1.7% for TSA reached statistical significance. RSA patients had increased risk of infection, dislocation and revision in the early postoperative period. At 2 years, the complication rates for RSA rose to 21.8% compared with TSA at 14.3%. Dislocation and infection remained as significant complication for RSA. The study also found patients younger than 65 years, male sex, patients with anaemia, and those with worker’s compensation had a higher risk in developing complications.
Similar content being viewed by others
Introduction
Reverse shoulder replacements (RSA) is known to have a high complication rate. Werner reported an overall complication rate of 50% for the first series of Delta III prosthesis (DePuy France, Saint Priest CEDEX, France) [1]. In a review of 10,884 shoulder arthroplasties performed in 2011–2013, the overall complication rates of RSA and anatomical total shoulder arthroplasty (TSA) were compared [2]. At 30 days, the overall complication rate for for both types of shoulder arthroplasties was 2.2%. The higher early complication rate of 3% for RSA compared with 1.7% for TSA reached statistical significance. RSA patients had increased risk of infection, dislocation and revision in the early postoperative period. At 2 years, the complication rates for RSA rose to 21.8% compared with TSA at 14.3%. Dislocation and infection remained as significant complication for RSA. The study also found patients younger than 65 years, male sex, patients with anaemia, and those with worker’s compensation had a higher risk in developing complications.
There were many reasons for this. The prosthesis was a new design in 1985 and it needed time to evolve and improve after clinical use. In 2005, Boileau reported 31% complications in his initial series of RSA with scapular notching noted in 68% [3]. Frankle changed his design to one with stronger locking screws for his glenosphere baseplate as the earlier design failed [4].
Secondly, the procedure is challenging with a steep learning curve. Most authors experience a learning curve in choosing the right prosthesis and their ideal placement location. Harmsden reported a reduction of complication rate from 17.3% to 8% after the first 75 patients [5].
Thirdly, indications for its use are wide and variable. That is RSA is used to treat a variety of conditions including proximal humeral fractures in the elderly, failed fracture fixation as well as revision arthroplasties. Complications for each indication are different. Werner’s high complication rate may be related to the large number of RSA (71%) they used to revise failed arthroplasties [1]. In a literature review of 782 RSA between 1995 and 2008, Zumstein found RSA performed for revision arthroplasties had a complication rate of 33.3% compared with those performed for cuff tear arthropathy at 19.5% [6]. Patients with rheumatoid arthritis did badly with a complication rate of 45% and those after acute fractures had a complication rate of 36%. In order to reduce complications for our RSA, we need to review the causes and adopt the appropriate technique to ensure a good outcome.
Scapular Notching
This is the most common complication after RSA [7]. With medialisation of the centre of rotation, impingement of the humeral component against the scapular neck with the arm by the side of the body is the reason potentially for notching. It has been reported in 44–96% of RSA, usually occurring as early as after 6 months [8]. Sirveaux described four grades of notching based on anteroposterior radiographs (Fig. 19.1a). Grade 1 notching does not involve the inferior screw. Grade 2 notching occurs up to the inferior screw (Fig. 19.1b). Grade 3 notching occurs above the inferior screw and grade 4 extends to the base plate [9].

(a) Sirveaux classification of scapular notching. (b) Type 2 notching 2 years post surgery
Anterior and posterior notching can be detected as areas of lucencies under the base plate on axillary radiographs. In 80 first generation reverse shoulder replacements (Delta, DePuy, France) followed up for 44 months, he reported erosions of grade 3 or above were associated with a compromised Constant score. In a larger series of 326 patients followed up for an average of 47 months, Lévigne reported notching increased with time [7]. They attributed two reasons for this progression. The continued impingement of the humeral component and polyethylene debris particles could cause osteolysis of the glenoid rim. Unlike Sirveaux, they did not find notching to be associated with a poor clinical outcome. Although there is a correlation between notching and lucent lines around the glenoid fixation screws, they only had one case of glenoid loosening. The authors also found notching was associated with the superolateral approach. They postulated that the inability to clear soft tissues off the inferior glenoid rim and neck from this approach was to blame for the higher percentage of notching seen when compared with the delto-pectoral approach.
In cuff arthropathy, proximal migration of the humeral head can cause erosion of the superior part of the glenoid. Favard classified this erosion into neutral (E0), concentric (E1), Superior (E2), Global superior (E3) and inferior (E4) (Fig. 19.2). He found that the Superior tilt (E2) glenoid is associated with notching in 83% [10]. His recommendation was to avoid placing the glenosphere with a superior tilt, even though this may have been the “natural orientation” for that patient.

Favard classification of glenoid erosion
Gerber noted anterior and posterior notching as well as the presence of osteophytes on the inferior scapular neck in his review of 188 Delta III RSA (DePuy Orthopaedics, Warsaw, Indiana) followed up for an average of 44 months [11]. Posterior notching is associated with external rotation. Anterior notching is rare and probably associated with impingement in internal rotation. The osteophytes were probably traction spurs formed after incomplete release of the triceps tendon. None of the observations affected the clinical outcome. He confirmed notching is associated with both a lower Constant score and Subjective Shoulder value.
In order to reduce notching, various technical as well as prosthetic modifications have been introduced.
-
1.
Lateralisation of the centre of rotation by a glenosphere larger than a hemisphere (Fig. 19.3). Theoretically, moving the humeral component away from the scapular neck would allow greater adduction movement at the expense of increased load on the glenoid component, which may induce loosening. Frankle has reported less notching in his first 60 prostheses reviewed at an average of 33 months. It was, however, associated with glenoid loosening in 12% and all required revision [12]. He resolved this by changing the base plate locking screws to 5 mm [13].

Lateralisation of centre of rotation by 5 mm improves adduction by 16°. (Re-drawn with permission from Dr. L. De Wilder)
-
2.
Lateralisation by extending the scapular neck by insertion of a 10 mm bone block under the base plate (Fig. 19.4). Boileau harvested his graft from the humeral head and fixed it to the glenoid with a 25 mm central peg base plate. (Aequalis Reverse Shoulder Prosthesis, Tornier Inc., Houston, TX) [14]. He only had 19% of 42 shoulders with notching at an average follow up of 28 months. Bone graft incorporation to the neck was observed in 98%. There was no glenoid loosening or instability. Good clinical results were obtained. He attributed the success of this modification because the centre of rotation remained at the base plate bone interface.

Lateralisation of 10 mm using more rounded glenosphere and bone graft augmentation
-
3.
Increase in the overhang of the glenosphere by moving the humeral component more distal. This can be achieved by the use of an eccentric glenosphere with inferior overhang (Fig. 19.5), tilting the glenosphere inferiorly (Fig. 19.6), or use of a larger glenosphere (Fig. 19.7).

Inferior overhang with 5 mm increases the adduction angle by 38°

Inferior tilt of 10° improves adduction by 10°

42 mm Glenosphere extra 3 mm overhang reduces scapular notching
Inferior tilt of the glenosphere by 10° only gains 10° of adduction. It medialises the centre of rotation and reduces the inferior locking screw bone purchase as it now has to travel along the inferior part of the glenoid neck rather than down the lateral scapular border. Its beneficial effect is therefore not significant. It is a useful technique to prevent notching in patients with low bmi and those with preoperative evidence of superior glenoid erosion [15]. In a prospective study of 42 RSA, Edwards did not find inferior tilt of the glenosphere reduces notching [16]. Chae found increased micromotion at the bone-glenoid component interface and higher bone stresses in cadaveric specimens with glenospheres fixed with 10° inferior tilt, compared with ones fixed in neutral tilt [17]. They attributed their findings to exposure of the softer cancellous bone after inferior reaming together with decreased bone-screw purchase resulting in a weakened glenosphere fixation.
Increased overhang of the glenosphere by 3 mm from 18 to 21 mm with a larger glenosphere, increases the adduction angle by 31°. The larger 42 mm glenosphere is therefore the recommended choice as it offers automatic overhang. This computer model study was confirmed by Berhouet in a cadaveric specimen study with 40 Aequalis RSA (Tornier Inc., Edina, Minn, USA) [18]. The authors found a 42 mm glenosphere with 7–10 mm lateralization was the best techniques to reduce notching.
Not all patients with cuff arthropathy have a large body frame to accommodate a 42 mm glenosphere with lateral offset. In a smaller patient, one can consider the use of an eccentric glenosphere with a 2–4 mm inferior offset. DeBiase reported 40 patients who were treated with a 36 mm glenosphere with a 4 mm inferior offset (SMR System, Lima Corporate, San Daniele del-Friuli, Italy) with no scapular notching seen after a minimum of 2 years (Fig. 19.8) [19].

36 mm glenosphere increases inferior offset by 4 mm (right) compared with a standard (left)
Dislocation
Dislocation of RSA is the most common postoperative complication at 4.7% [6]. There are many causes of instability. Revision arthroplasty surgery has a higher dislocation rate at 9.4% compared with primary arthroplasty at 4.1%. 97.3% of RSA with instability were operated via a deltopectoral approach. The superolateral approach with subscapularis sparing was believed to be the reason behind the apparent lack of dislocation [20]. Damage to the subscapularis muscle after extensive release and its poor repair after has often been quoted as a causative factor [21]. Controversy still exists as to whether it is possible to repair the subscapularis. RSA in shoulders with distorted anatomy secondary to previous fracture also have a high dislocation rate. Martinez reported a dislocation rate of 13.6% in RSA used in the treatment for fracture sequalae [22]. Inadequate deltoid tensioning due to incorrect choice or positioning of the implants is the most common cause of recurrent instability in primary RSA [23].
In an in vivo study, Gerber has shown that if the glenosphere has been retroverted by 20°, significant instability occurs with any humeral version [24]. This can occur in a situation where the posterior glenoid bone is of poor bone quality. In order to obtain good quality bone for fixation, the base plate may have been fixed in a retroverted manner. Of more serious consequence, he found retroversion of the humeral component could lead to instability of the RSA. In his model, if the glenoid is in neutral, and the humeral component is inserted to the anatomical retroversion of 20°, the joint will become unstable when the arm is abducted at 90°. By increasing anteversion of the humeral component to neutral, intrinsic stability returns. His conclusion is that the glenoid component should be fixed without retroversion of more than 10°, and the humeral component should be inserted in neutral or slight anteversion.
In a 2D computer scapula model , de Wilde concluded that overhang of the glenosphere is the most important factor in achieving stability [25]. The extra 3 mm overhang in a 42 mm glenosphere affords more stability when compared with a 38 mm glenosphere. Increasing the thickness of the polyethylene insert increases the contact area of the articular surface, increases the deltoid tension, but decreases the impingement angle. The thicker plastic liner will hit the scapular neck earlier on adduction.
Most dislocations occur early, usually within the first 3 months [26]. Closed reduction should be attempted first. When recurrent, it is likely to be secondary to surgical error and revision of the components may become necessary [7]. Chalmers reviewed 11 of 385 patients (2.9%) who dislocated their RSA within the first 3 months. Ten were Trabecular Metal Reverse Shoulders (Zimmer Inc., Warsaw, IN, USA) and one was Delta III (DePuy Inc., Warsaw, IN, USA). Their patients were mainly male (82%), obese with poor subscapularis muscle. All but one dislocated within the first 5 weeks. They were all dislocated anteriorly. Closed reduction was only successful in 4.7 (56%) required revision surgery. Five required thicker polyethylene liner to increase deltoid tension and 2 were converted to hemiarthroplasty. As their patient shoulders stabilized after insertion of a thicker insert, they believed inadequate tensioning of the deltoid muscles was the primary cause of instability. Also the thicker insert automatically increases the compressive forces across the joint thus making it more stable. This trade off being to decrease the impingement angle of the humeral component against the glenoid neck.
In a recent study, Frankle reported a more successful outcome with closed reduction of his dislocated lateralized prosthesis (DJO Surgical, Austin Tx, USA). In a 10 year period, he had 2.3% dislocations, 30 out of 1293 RSA [27]. 48% of his patients had previous surgery, 80% being revision surgery. He performed his reduction in the outpatient department. With the patient’s arm by the side, longitudinal traction was applied while a posteriorly directed force is applied to the upper humerus. Meanwhile, the humerus is gently external rotated. After closed reduction, 62% remained stable. 29% required revision surgery with larger components for both the glenoid and humerus. 9% remained unstable but patients were unfit for further surgery. He concluded that closed reduction, whether early or late in the postoperative period, had an equal good outcome. Secondly, closed reduction results were equally as good as that of revision surgery. After closed reduction, the arm should be rested in a sling for 4–6 weeks, avoiding adduction, internal rotation and extension.
If closed reduction fails, one should prepare for open reduction and revision. Before surgery, it is necessary to assess the positions of the glenosphere by CT scan. New software can reduce metal scatter which blocks assessment of the components position. We suggest looking for the following. Retroversion of the glenosphere should be checked, it should be 10° or less. The humeral component should be in neutral. There should be an overhang of the glenosphere at the scapula neck. During surgery, all soft tissues, including scar tissues, have to be cleared from the inferior margins of the glenoid to ensure the glenosphere has an adequate overhang. This is particularly important if preoperative assessment has shown all the components are in their optimal solution.
The following is an example of a RSA with early recurrent dislocation that illustrates the discussed management.
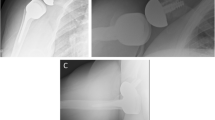
Fifty year old patient with rheumatoid arthritis developed avascular necrosis of the humeral head (Fig. 19.9a). She also had an eroded glenoid with very poor bone stock (Fig. 19.9b). At initial surgery, the base plate just managed to cover the glenoid. A 36 mm glenosphere was locked into position with apparent stability (Aequalis, Tornier Inc., Bloomington, MN, USA) (Fig. 19.10). She returned 1 week later with an acute anterior dislocation. This was reduced closed under general anaesthesia. Screening of the RSA in theatre showed apparent stability. Patient was discharged home and she was requested to rest her arm in a sling. Three days later, the shoulder re-dislocated. As it was a second dislocation, her instability was perceived to be secondary to inadequate deltoid tension. The humeral insert was then changed to a thicker variety (Fig. 19.11). After a week, her shoulder dislocated again. On this occasion, she had a CT scan. Careful assessment of the glenoid component showed the lack of overhang in the glenosphere over the scapular neck (Fig. 19.12). The 36 mm glenosphere was exchanged to sized 42 mm. A + 3 mm humeral insert was used. The shoulder felt immediately stable and has remained so since (Fig. 19.13). This case illustrates the importance of Glenoid overhang as the major factor in contribution to RSA stability.

(a) MRI shows AVN of left humeral head. (b) Axial view shows shallow eroded glenoid

On table radiograph shows apparent stable RSA

Anterior dislocation of humeral component

CT scan shows 36 mm glenosphere with no overhang

Revision to 42 mm glenosphere with good overhang
Humeral Fractures
The incidence of periprosthetic humeral fracture around shoulder arthroplasties is between 0.6% and 3% [28]. García-Fernández et al. reported an overall incidence of 3.4% in a series of 203 RSA patients with a mean age of 75 years [29].
The fractures can occur during surgery or in the postoperative period, following trauma. Intraoperative fracture increases the operation time, increases blood loss, alters implant choices, increase the need for bone graft or fixation and may have an effect on postoperative outcome. The risk factors associated with increased periprosthetic fractures in shoulder arthroplasty include female sex, osteopenia, Rheumatoid Arthritis, over-reaming of humeral canal, insertion of oversized broach, proximal humeral deformity or malunion and soft tissue contracture requiring excessive external rotation force for dislocation [30].
The incidence of periprosthetic fracture is higher in patients undergoing revision RSA compared to primary RSA [29, 31]. Wagner et al. reported 16% of intraoperative periprosthetic fractures in a series of 224 patients that underwent revision surgery to RSA. Most fractures occurred during humeral component removal. A history of instability and prior hemiarthroplasty were found to be significant risk factors [31]. A few studies also show higher incidence of periprosthetic fractures with the use of press fit uncemented components. King et al. compared 51 uncemented RSA with 32 cemented RSA and reported an incidence of fracture in 6.02% in uncemented group compared to 1.2% in the cemented group [32].
Periprosthetic fractures are classified according to the location of fracture. Wright and Cofield’s classification is the most commonly used. This was originally created for postoperative fractures and is limited to those occurring around the tip of humeral stem [33]. Type A fractures include the tip and extend proximally. Type B fractures extends from the tip. Type C fracture occur distal to the end of humeral component.
Campbell proposed a classification system, that included tuberosity and metaphyseal fractures [30] This is more suitable for intra-operative fractures, particularly following the use of press-fit implants. Campbell divided these fractures into four types based on location. Type A include greater and lesser tuberosity fractures. Type B include fracture of the metaphyseal portion or surgical neck of humerus. Type C involves proximal humeral diaphysis. Type D involves the mid and distal diaphysis of humerus.
Worland et al. classified these fractures depending on fracture anatomy and implant stability so as to guide the treatment [34]. Type A fractures involve the tuberosities. Type B fractures occur around the stem and are subclassified into three types, B1 fractures are spiral fractures with a stable implant. B2 fractures are transverse or short oblique fractures about the tip of the stem with a stable implant. B3 fractures are fractures about the stem with an unstable implant. Type C fractures occur distal to the tip of the stem.
As most fractures occur intra-operatively, prevention is the best way to avoid this complication. Special attention should be paid to bone quality especially in elderly patients, osteoporotic and female patients, Rheumatoid Arthritis patients, when using press fit components and in revision surgery [29].
The following preventive measures are useful in reducing the incidence of fracture:
-
1.
Preoperative templating and awareness of proximal humeral geometry like malunion, deformity, canal stenosis and osteopenia to prevent use of oversized reamers, broaches and implants
-
2.
Use of intraoperative fluoroscopy to guide humeral preparation in complex cases
-
3.
Careful exposure and complete soft tissue release to facilitate easy dislocation
-
4.
Systematic approach for removing well fixed humeral components – cortical window, proximal humeral splitting osteotomy and use of implant specific removal device
During surgery, once a fracture has occurred, the surgeon should follow a systematic approach. The surgical approach should be extended if necessary to identify and characterize the fracture. If a distal fracture is suspected, fluoroscopy of the entire arm should be obtained.
Fractures occurring intraoperatively should undergo fixation appropriate to fracture configuration and implant stability. This will allow early mobilization and prevent further displacement of the fracture and therefore a shorter time to union. Outcomes of intraoperative fractures managed with fixation or long stemmed implant are equivalent in terms of range of movement and pain as those primary arthroplasty cases [35].
Fractures involving greater /lesser tuberosity (Campbell Type A) should be assessed for stability. If deemed stable, with the periosteum intact and without displacement, they may be treated with insertion of standard implants without specific fixation. If the fracture is mobile or there is displacement, suture fixation of the fractured tuberosity to the humeral implant and around the proximal part of humerus is recommended. Fractures involving the metaphysis (Campbell Type B) are treated with standard –length implant with cerclage wire fixation (Fig. 19.14). Care should be taken when passing the cerclage wires to avoid iatrogenic nerve damage. The fracture site may be augmented with bone graft from the humeral head to promote union. Fracture involving the proximal part (Campbell Type C) and the middle and distal parts (Campbell Type D) of the humeral shaft are best treated with long stemmed implants with cerclage fixation and in some cases with supplementary plate or allograft cortical strut fixation (Fig. 19.15).

Intra-operative fracture (Campbell Type B) treated by cerclage

Campbell Type D fracture , treated by long stemmed humerus implant
Treatment for postoperative fracture include both conservative and surgical management. This depends on fracture location, displacement, stability of prosthesis and bone quality. If the fracture is undisplaced or minimally displaced, and thes implant is stable, the fracture can be treated by nonoperative methods. For unstable diaphyseal fracture with well-fixed components, it is recommended to fix using multiple cerclage wires or a heavy plate with proximal cerclage wires and distal screws [36] (Fig. 19.16). For diaphyseal fracture with loose stem, revision to long stem prosthesis is recommended [29]. Fractures distal to the prosthesis responds well to conservative treatment, and require fixation in very selected cases only.

Post-operative fracture 2 years after RSA, treated by multiple cerclage
Glenoid Complications
These include intraoperative fracture, glenoid baseplate loosening and glenosphere disassembly. In a multicentre study of 1953 cases, glenoid loosening was reported to be 1.7% and glenoid disassembly was observed in 0.5% [37].
Glenoid Fracture
Intraoperative glenoid fractures can occur during reaming or the subsequent fixation. It can be challenging in patients with severe osteoporosis, those with previous glenoid fracture or failed hemiarthroplasty. The reamer should start on full speed before bone contact and only the sclerotic surface is lightly reamed to avoid weakening the subchondral bone. In cases of bone insufficiency, the reaming is best done by hand. A pre-op CT scan is mandatory to assess the position of the triangular cone of bone of the glenoid in relation to its articular surface. This will help the surgeon to determine the best position to drill for the central peg. The humeral head can be used as bone graft to place on the glenoid in cases of bone deficiency. If intraoperative fracture does occur, the use of a longer central peg and redirectioning of the peripheral locking screws may be able to salvage the situation. If fixation is not possible, then a two stage procedure may be performed with bone grafting of the glenoid using either autologous or allograft and once the bone graft has incorporated, the humeral component is inserted as a secondary procedure.
Glenoid Loosening
The most common causes are infection, failure to achieve adequate fixation at the time of initial surgery, loosening of the screws secondary to osteolysis and technical problems. When the baseplate is loose, it is usually associated with bone loss and screw breakage is often seen. Screw failure is induced by a seesaw movement of the glenosphere onto the baseplate. Middernacht found that the design of the prosthesis, including the use of 5.0-mm locking peripheral screws, and the technique of implantation, incorporating a 15° inferior tilt of the baseplate were the most important factors to prevent mechanical failure of the baseplate fixation [38] (Fig. 19.17).

Complete loosening of baseplate and significant glenoid bone loss
Three types of bone defects have been described, based on the location and severity on CT namely, Cavity defect (type A), uncontained wall defect (Type B) and Complex defect (Type C).
Small contained defects can be filled with either autograft or allograft, whereas larger defects will require structural support usually with a tricortical iliac crest graft.
Glenoid Disassembly
Disassembly can occur between the baseplate and the glenosphere. In a series of 479 RSA (468 Delta III and 11 Aequalis), the incidence of glenosphere disengagement was found to be 3.2%. In 13 patients, the disengagement was partial and was not associated with a poor functional outcome [38]. In three patients, the disengagement led to a fracture of the central screw and complete disengagement of the glenosphere from the baseplate. Improper seating of the glenosphere on the baseplate can occur as a result of inadequate reaming of bone around the peripheral edge of the baseplate, interposition of bone or soft tissue between the glenosphere and the baseplate at the time of impaction and failure of the locking mechanism between the central peg and glenosphere. The positioning of the baseplate is also crucial, if the baseplate is being positioned too high or associated with superior tilt, there is excess shear stress which may induce early failure (Fig. 19.18 a, b).

(a) The baseplate is positioned with superior tilt and there is bony impingement superiorly against the glenosphere with partial disengagement from the baseplate. (b) Early failure with glenoid disassembly occurred due to excess shear stress
Measures to try and prevent the risk of glenoid loosening include inferior placement of the baseplate in relation to glenoid, placement of locking screws in best quality bone, larger central screw, multiple peripheral screws, and larger diameter screws. Cusick et al. reported a significantly higher likelihood of glenosphere dissociation when larger diameter glenospheres (40 and 44 mm) were implanted; thought to be related to the larger exposed surface area for potential soft tissue or bone impingement [39].
Acromial Fracture
The incidence of a fracture of the acromion following RSA varies from 1% to 7% according to the reported series. These fractures can occur at any point after surgery ranging from 1 to 94 months postoperatively.
The exact aetiology of acromion fractures is unclear but it is thought to be due to a combination of bone insufficiency and intra-operative technical factors. Preop risk factors include osteoporosis, os acromiale, acromion erosion, spine non-union. Intra-operative risk factors include excess tension on the deltoid with resultant arm lengthening and the position as well as the length of the glenoid baseplate screws. The superior 12 o’clock and posterior 9 o’clock screws have been implicated as stress risers in the development of scapular spine fractures. Crosby found that three of the four Type III fractures appeared to propagate from the tip of the most superiorly placed metaglene screws and as a consequence they no longer use the most superior screw hole for fixation of the metaglene.
It is likely that the reported incidence will increase due to the longer duration of follow up of our patients and better diagnostic techniques. Undisplaced acromial or scapular spine fractures are difficult to diagnose on plain radiographs and the reported accuracy rate is only 78.8% (Otto). The investigation of choice is single photon emission computed tomography (SPECT CT) which has significantly less radiation exposure than conventional CT scans [40] (Fig. 19.19).

Spect CT showing acromon fracture
There are three classification systems described. Rouleau proposed a classification system which is descriptive and based on the anatomy and functionality of the scapula [41] (Fig. 19.20). Fractures of the tip were those of the most lateral or anterior portion of the acromion. Fractures of the body of the acromion are those medial to the tip of the acromion and lateral to the beginning of the scapular base. The scapular base is the lateral border of the scapular spine, which is smooth and round.

Rouleau’s classification of acromion fracture
Crosby’s classification system was intended to recommend the best choice of treatment [42] (Table 19.1).
Levy proposed a further classification based on the involvement of the deltoid origin. Type I indicated involvement of a portion of the anterior and middle deltoid origin; type II, at least the entire middle deltoid origin with a portion but not all of the posterior deltoid origin; and type III, the entire middle and posterior deltoid origin [43] (Fig. 19.21).

Levy’s classification of acromion fracture
In their series of 16 patients, all were treated non operatively with a shoulder immobiliser for 6 weeks and were instructed to limit activities to pendulum exercises. Teusink et al. reported a series of 25 patients with acromion fractures and all were treated non operatively. The union rate was 57% for acromial fractures and 50% for scapular spine fractures. They found that the location of the fracture (acromion or spine) did not affect the outcome. Overall, patients with acromion fracture still had improved scores but inferior clinical outcome.
Hattrup also managed his series of nine patients with acromial fracture non operatively and concluded that a decision for surgical treatment will need to balance the challenges of internal fixation with the incremental improvement that may occur with improved fracture healing.
Operative treatment is potentially challenging as the bone is soft and the amount of bone that can hold fixation is limited. Furthermore, despite fixation, the rate of non-union and malunion remains high. There are two surgical techniques described. For distal acromion fractures, the authors recommend the use of tension band wire fixation to control the rotation of the distal fragment and provide compression at the fracture site. However, this technique is not without its problems, notably hardware loosening and failure due to the strong pull of the deltoid. For this reason, De Wilde advocates the use of a second tension band fixation across the acromioclavicular joint (Fig. 19.22 a, b).

(a) Displaced acromion fracture (Figures kindly provided by L De Wilde). (b) Double Tension Band fixation (Figures kindly provided by L De Wilde)
Alternatively, the fracture may be fixed with two locking plates with one over the superior superior edge of the scapular spine in a compression mode and the other applied from the posterior acromion to the posterior cortex of the scapular spine, in the infraspinatus fossa (a 90/90 configuration) (Fig. 19.23).

: Patient presented with mild discomfort over acromion, 2 years following RSA. Acromion stress fracture was treated by conservative measures
Neurological Injury
The rate of neurological injury following all forms of shoulder arthroplasty is reported to be around 1%. It can occur immediately after surgery as seen in proximal lesions involving axillary, brachial plexus, radial and musculocutaneous nerves. It can also have a delayed presentation, manifesting as nerve entrapment syndromes including carpal tunnel and cubital tunnel syndromes.
Nerve injury can occur intraoperatively due to a variety of reasons including surgical approach, placement of retractors, screw malposition, compression from haematoma or cement and injury from interscalene block. The use of a cement removal heat probe can generate high temperature within the humeral canal. This in turn can lead to neurapraxia of the radial nerve. Ladermann found the rate of neurological injury following reverse arthroplasty is 10.9 times higher than anatomical arthroplasty, with the axillary nerve involved in 50%. This is probably related to the design of reverse prosthesis which distalises the centre of rotation. The humerus is lengthened by approximately 2.7 cm (+/− 1.8 cm). This in turn increases the tension on the axillary nerve. An anatomical study has found that when the humerus is lowered, the axillary nerve below the mid glenoid level which corresponds to the highest level of nerve tension, loses its curvature and becomes more vertical and straight. When the humerus is lateralised, there was no evidence of stretching of the nerve. The practical implication of this study is that if the reverse shoulder arthroplasty is found to be unstable intraoperatively, it would be safer to increase the size of the glenosphere, thereby increasing the lateralisation, rather than using a thicker polyethylene insert or metallic spacer which lowers the humerus increasing the risk of brachial plexus stretching [44, 45].
Haematoma
Haematoma formation is relatively common in RSA. In 2005, Gerber reported postoperative haematoma occurred in 20% of his RSA [1] By moving the gleno-humeral articulation medially and distally, a large dead space below the acromion is thus created. Without the tamponade effect of the rotator cuff over this dead space, blood and fluid will accumulate there. Haematoma formation is invariably present after RSA but does not necessarily require intervention. Historically, the concern is that the presence of a haematoma may lead to joint infection [46]. In a literature review in 2011, Zumstein found only 20 cases of haematoma reported in 782 RSA [6]. A much lower reported rate at 2.6%. Nine cases required intervention and five cases were aspirated. None led to infection.
The current practice to reduce haematoma formation is the use of tranexamic acid before surgery to reduce bleeding. During surgery, meticulous attention is paid to control all bleeding points. After surgery, a suction drain is left in the dead space for 24–48 h. Frequently, 400 mls of blood will be drained. Gentle early mobilization is encouraged to allow the deltoid muscle to pump any fluid out of the dead space. If a haematoma is formed, one can monitor its progress before aspiration or rushing in to evacuate it.
Infection
Infection is the third commonest complication following reverse shoulder arthroplasty at 3–6%. This is substantially higher than the 2% rate quoted for anatomical shoulder arthroplasty. Florschutz found infection rates following primary anatomical and primary reverse shoulder arthroplasty were the same at 2%. When RSA was used in revision arthroplasty, the infection rate was 7%. Morris et al. have found that a history of previous failed arthroplasty and age less than 65 were independent risk factors for infection after RSA. Other factors implicated include an increased subacromial dead space after RSA where haematoma collects; those with poor soft tissue envelope around the prosthesis, as well as in patients with rheumatoid arthritis.
Propionibacterium acnes and staphylococcus epidermidis were the most common organisms identified, accounting for 87.5%. Propionibacterium acnes is a gram positive anaerobic bacillus which is found in the sebaceous glands associated with hair follicles. It is postulated that men have more sebaceous glands and therefore have a higher rate of Propionibacterium acnes infection around the shoulder (Patel et al). Other potential risk factors for Propionibacterium acnes infection include long duration of surgery and age. Lucas et al. recommended that at least 5 explant or tissue specimens should be obtained for microbiologic testing and extended cultures for at least 17 days [47]. Sethi et al. [48] have shown that the positive culture rate for Propionibacterium acnes after 7 days of culture was 8.8% whereas the rate increases to 15.8% after 14 days and 22.8% after 28 days of incubation. Clindamycin is effective against most strains of Propionibacterium and can be considered as suitable prophylactic antibiotics [49]. A dose of 600 mg given iv 30 min before surgery is recommended. Gentamicin impregnated collagen sponge has been found to reduce surgical site infection in orthopaedic surgery [50]. Our practice is to place a small amount inside the glenosphere which may help to reduce possible dead space infection.
For established infection treatment options include early debridement with removal and exchange of liner and glenosphere, one or two stage revision and resection arthroplasty.
If infection occurred at less than 60 days from surgery, we recommend initial debridement, washout and exchange of polyethylene liner and glenosphere. This is on the assumption that the implants are not loose and surrounding soft tissues are healthy. Arthroscopy and lavage may be helpful to obtain a microbiological sample but should not be relied on solely as therapeutic procedure.
If debridement fails to control the infection, the next step would be either a one stage or two stage revision. There is no clear consensus in the published literature as to whether one stage or two stage is better. One stage revision has better functional results with a lower morbidity and complication rate, but with a greater risk of recurrent infection. De Wilde advocated a single stage approach with the advantages of significantly shorter treatment, less patient morbidity, lower costs and avoiding glenoid erosion by the antibiotic spacer [51].
Boileau on the other hand advocates a two stage approach and reported eradication of infection in all cases [52]. It has a higher morbidity but higher success rate for infection eradication. It also allows complex problems such as bone loss to be addressed. The potential benefit of an antibiotic-impregnated cement spacer is controversial. They deliver a high concentration of antibiotics locally at the infected site and maintain soft tissue tension whilst waiting for reimplantation after eradication of infection. Verhelst found no improvement in outcome with the use of antibiotic-impregnated cement spacers after retrieval of the infected prosthesis, compared with resection arthroplasty alone.
Resection arthroplasty remains a salvage option with a high complication rate (33%). A much poorer outcome is to be expected when compared with resection arthroplasty following hemiarthroplasty or anatomical shoulder arthroplasty.
References
Werner CM, Steinmann PA, Gilbart M, Gerber C. Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am. 2005;87(7):1476–86.
Villacis D, Sivasundaram L, Pannell W, Heckmann N, Omid R, Hatch GR. Complication rate and implants survival for reverse shoulder arthroplasty versus total shoulder arthroplasty: results during the initial 2 years. J Shoulder Elb Surg. 2016;25:927–35.
Boileau P, Watkinson D, Hatzidakis AM, Hovorka I. Neer award 2005: the Grammont reverse shoulder prosthesis: results in cuff tear arthritis, fracture sequale, and revision arthroplasty. J Shoulder Elb Surg. 2006;15:527–40.
Cheung E, Willis M, Walker M, Clark R, Frankle MA. Complications in reverse Total shoulder arthroplasty. J Am Acad Orthop Surg. 2011;19(7):439–49.
Harmsen SM, Chang YH, Hattrup SJ. Simple moving average: a method of reporting evolving complication rates. Orthopedics. 2016;23:1–8.
Zumstein MA, Pinedo M, Old J, Boileau P. Problems, complications, reoperations, and revisions in reverse total shoulder arthroplasty: a systemic review. J Shoulder Elb Surg. 2011;20:146–57.
Farshad F, Gerber C. Reverse total shoulder arthroplasty—from the most to the least common complication. Int Orthop (SICOT). 2010;34:1075–82.
Nicholson GP, Srauss EJ, Sherman SL. Scapular nothching: recognition and strategies to minimize clinical impact. Clin Orthop Relat Res. 2011;469(9):2521–30.
Sirveaux F, Favard L, Oudet D, Huquet D, Walch G, Molé D. Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff. Results of a multicenter study of 80mshoulders. J Bone Joint Surg Br. 2004;86:388–95.
Levigne C, Garret J, Boileau P, Alami G, Favard L, Walch G. Scapular notching in reverse shoulder arthroplasty: is it important to avoid it and how? Clin Orthop Relat Res. 2011;469:2512–20.
Simovitch RW, Zumstein MA, Lohri E, Helmy N, Gerber C. Predictors of scapular notching in patients managed with delta III ReverseTotal shoulder replacement. J Bone Joint Surg. 2007;89A(3):588–600.
Frankle M, Levy JC, Pupello D, Siegal S, Saleem A, Mighell M, Vasey M. The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: a minimum two-year follow-up study of sixty patients: surgical technique. J Bone Joint Surg Am. 2006;88(suppl 1):178–90.
Cuff D, Pupello D, Virani N, Levy J, Frankle M. Reverse shoulder arthroplasty for the treatment of rotator cuff deficiency. J Bone Joint Surg Am. 2008;90:1244–51.
Boileau P, Moineau G, Roussanne Y, O’Shea K. Bony increaed-offset reversed shoulder arthroplasty. Clin Orthop Relat Res. 2011;469:2558–67.
Edwards TB, Trappey GJ, Riley C, O’Connor DP, Elkousy HA, Gartsman GM. Inferior tilt of the glenoid component does not decrease scapular notching in reverse shoulder arthroplasty: results of a prospective randomized study. J Shoulder Elb Surg. 2012;21(5):641–6.
Falaise V, Levigne C, Favard L, SOFEC. Scapular notching in reverse shoulder arthroplasties: the influence of glenometaphyseal angle. Orthop Traumatol Surg Res. 2011;97(6 supp):S131–7.
Chae SW, Lee H, Kim SM, Lee J, Han SH, Kim SY. Primary stability of inferior tilt fixation of the glenoid component in reverse total shoulder arthroplasty: a finite element study. J Orthop Res. 2016;34(6):1061–8.
Berhouet J, Garaud P, Favard L. Evaluation of the role of glenosphere design and humeral component retroversion in avoiding scapular notching during reverse shoulder arthroplasty. J Shoulder Elb Surg. 2014;23:151–8.
De Biase CF, Delcogliano M, Borroni M, Castagna A. Reverse total shoulder arthroplasty: radiological and clinical result using an eccentric glenosphere. Musculoskelet Surg. 2012;96(Suppl 1):S27–34.
Walch G, Wall B, Mottier F. Complications and revision of the reverse prosthesis: a multicenter study of 457 cases. In: Boileau P, editor. Reverse shoulder arthroplasty. Nice: Sauramps; 2006. p. 335–52.
Edwards TB, Williams MD, Labriola JE, Elkousy HA, Gartsman GM, O’Connor DP. Subscapularis insufficiency and the risk of shoulder dislocation after reverse shoulder arthroplasty. J Shoulder Elb Surg. 2009;18(6):892–6.
Martinez AA, Calvo A, Bejarano C, Carbonel I, Herrera A. The use of the Lima reverse shoulder arthroplasty for the treatment of fracture sequelae of the proximal humerus. J Orthop Sci. 2012;17:141–7.
Alentorn-Geli E, Samtier G, Torrens C, Wright TW. Reverse shoulder arthroplasty. Part2: systemic review of reoperations, revisions, problems and complications. Int J Shoulder Surg. 2015;9(2):60–7.
Favre P, Sussmann PS, Gerber C. The effect of component positioning on intrinsic stability of the reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2010;19:550–6.
De Wilde LF, Poncet D, Middemacht B, Ekelund A. Prosthetic overhang is the most effective way to prevent scaular conflict in a reverse total shoulder shoulder prosthesis. Acta Orthop. 2010;81(6):719–26.
Chalmers PN, Rahman Z, Romeo AA, Nicholson GP. Early dislocations after reverse total shoulder arthroplasty. J Shoulder Elb Surg. 2014;23:737–44.
Teusink MJ, Pappou IP, Schwarts DG, Cottrell BJ. Frankle MA results of closed management of acute dislocation after reverse shoulder arthroplasty. J Shoulder Elb Surg. 2015;24(4):621–7.
Kumar S, Sperling JW, Haidukewych GH, Cofield RH. Periprosthetic humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am. 2004;86-A(4):680–9.
García-Fernández C, Lópiz-Morales Y, Rodríguez A, López-Durán L, Martínez FM. Periprosthetic humeral fractures associated with reverse total shoulder arthroplasty: incidence and management. Int Orthop. 2015;39(10):1965–9.
Campbell JT, Moore RS, Iannotti JP, Norris TR, Williams GR. Periprosthetic humeral fractures: mechanisms of fracture and treatment options. J Shoulder Elbow Surg Am Shoulder Elbow Surg. 1998;7(4):406–13.
Wagner ER, Houdek MT, Elhassan BT, Sanchez-Sotelo J, Cofield RH, Sperling JW. What are risk factors for intraoperative humerus fractures during revision reverse shoulder arthroplasty and do they influence outcomes? Clin Orthop Relat Res. 2015;473(10):3228–34.
King JJ, Farmer KW, Struk AM, Wright TW. Uncemented versus cemented humeral stem fixation in reverse shoulder arthroplasty. Int Orthop. 2015;39:291–8.
Wright TW, Cofield RH. Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am. 1995;77(9):1340–6.
Worland RL, Kim DY, Arredondo J. Periprosthetic humeral fractures: management and classification. J Shoulder Elbow Surg J Bone Joint Surg. 1999;8(6):590–4.
Athwal GS, Sperling JW, Rispoli DM, Cofield RH. Periprosthetic humeral fractures during shoulder arthroplasty. J Bone Joint Surg Am. 2009;91(3):594–603.
Cameron B, Iannotti JP. Periprosthetic fractures of the humerus and scapula: management and prevention. Orthop Clin North Am. 1999;30(2):305–18.
Molé D, Godeneche A, Laedermann A. Problems & complications related to the Glenoid. Shoulder concepts 2016 – reverse shoulder arthroplasty 20 year anniversary.
Middernacht B, De Wilde L, Molé D, Favard L, Debeer P. Glenosphere disengagement: a potentially serious default in reverse shoulder surgery. Clin Orthop Relat Res. 2008;466:892–8.
Cusick MC, Hussey MM, Steen BM, Hartzler RU, Clark RE, Cuff DJ, Cabezas AF, Santoni BG, Frankle MA. Glenosphere dissociation after reverse shoulder arthroplasty. J Shoulder Elb Surg. 2015;24(7):1061–8.
Teasing MJ, Otto RJ, Cottrell BJ, Frankle MA. What is the effect of postoperative scapular fracture on outcomes of reverse shoulder arthroplasty? J Shoulder Elb Surg. 2014;23(6):782–90.
Rouleau DM, Gaudelli C. Successful treatment of fractures of the base of the acromion after reverse shoulder arthroplasty: case report and review of the literature. Int J Shoulder Surg. 2013;7(4):149–52.
Crosby LA, Hamilton A, Twiss T. Scapula fractures after reverse total shoulder arthroplasty: classification and treatment. Clin Orthop Relat Res. 2011;469:2544–9.
Levy JC, Anderson C, Samson A. Classification of postoperative acromial fractures following reverse shoulder arthroplasty. J Bone Joint Surg Am. 2013;95(15):e104.
Lädermann A, Williams M, Mekis B, Hoffmeyer P, Walch G. Objective evaluation of lengthening in reverse shoulder arthroplasty. J Shoulder Elb Surg. 2009;18(4):588–95.
Marion B, Leclère FM, Casoli V, Paganini F, Unglaub F, Spies C, Valenti P. Potential axillary nerve stretching during RSA implantation: an anatomical study. Anat Sci Int. 2014;89(4):232–7. Epub 2014 Feb 5.
Cheung EV, Sperling JW, Cofield RH. Infection associated with haematoma formation after shoulder arthroplasty. Clin Orthop Relat Res. 2008;466(6):1363–7.
Lucas RM, Hsu JE, Whitney IJ, Wasserburger J, Matsen FA III. Loose glenoid components in revision shoulder arthroplasty: is there an association with positive cultures? J Shoulder Elb Surg. 2016;25(8):1371–5.
Sethi PM, Sabetta JR, Stuek SJ, Horine SV, Vadasdi KB, Greene RT, Cunningham JG, Miller SR. Presence of Propionibacterium acnes inprimary shoulder arthroscopy: results of aspiration and tissue cultures. J Shoulder Elb Surg. 2015;24(5):796–803.
Crane JK, Hohman DW, Nodzo SR, Duquin TR. Antimicrobial susceptibility of propionibacterium acnes isolates from shoulder surgery. Antimicrob Agents Chemother. 2013;57(7):3424–6.
Knaepler H. Local application of gentamicin-containing collagen implant in the prophylaxis and treatment of surgical site infection in orthopaedic surgery. Int J Surg. 2012;10(Suppl 1):S15–20.
De Wild L, Walch G. Humeral prosthetic failure of reversed total shoulder hemiarthroplasty: a report of three cases. J Shoulder Elbow Surg. 2006;15:261–4.
Boileau P, Melis B, Duperron D, Moineau G, Rumian AP, Han Y. Revision surgery of reverse shoulder arthroplasty. J Shoulder Elb Surg. 2013;22(10):1359–70.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Mok, D., Lam, F., Chidambaram, R. (2019). Complications of the Reverse Implant. In: Trail, I., Funk, L., Rangan, A., Nixon, M. (eds) Textbook of Shoulder Surgery . Springer, Cham. https://doi.org/10.1007/978-3-319-70099-1_19
Download citation
DOI: https://doi.org/10.1007/978-3-319-70099-1_19
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-70098-4
Online ISBN: 978-3-319-70099-1
eBook Packages: MedicineMedicine (R0)