
Abstract
The concept of a “Double Burden of Disease” conceived in the second half of the last century has by now turned into a success story in sub-Saharan Africa. It has been instrumental in creating the regional and global political momentum to address the “unfinished agenda of infectious diseases” and to fight against HIV/AIDS, Tuberculosis and Malaria in a concerted and sustainably financed action. An estimated three million children under the age of five have been saved from malaria, and the incidence of new HIV cases in sub-Saharan Africa has fallen by more than half between 2001 and 2012. The concept also created an awareness of the rising epidemic of non-communicable diseases (NCDs) in this part of the world. It is too early to predict whether or not this success in the area of infectious disease will repeat itself in the domain of non-communicable diseases. There are some obstacles to overcome. The countries of SSA have to integrate the two separately conceived policies and their different funding into one and to avoid competition in resource allocation between the two areas. They need to develop integrated strategies that begin in the primary health care sector and finally they need to define strategies on how to engage constructively with the private sector.
You have full access to this open access chapter, Download chapter PDF
1 Introduction
Before the turn of the millennium the co-existence of acute and chronic diseases in one and the same region was by some researchers (Murray and Lopez 1996) and the World Health Organization (WHO 1999) coined “the double burden of disease ”. The concept of a double burden of disease finds its root, implicitly or explicitly, in ideas outlined as far back as 1971 by A.R. Omran. According to this theory, health and disease patterns change over time in societies. Like individuals, societies are thought to have a “life cycle”. In young societies infectious diseases, nutritional deficiencies and maternal , newborn and child health problems prevail. When societies grow up accidents and violence-related diseases as well as NCDs become more prevalent. In aging societies, finally, NCDs predominate (Omran 1971). The growing burden of NCDs was thought to be a consequence of demographic transition and the double burden of disease was considered a phenomenon of societies in transition which were hit by the emerging epidemic of NCDs, while still struggling with an “unfinished agenda of infectious diseases” (WHO 1999).
The same line of thinking made it logical to separate the two entities of diseases when putting together a package of health goals for the Millennium Development Goals (MDGs, adopted in 2000). The MDGs focus on the “unfinished agenda” and concentrate on the fight against HIV/AIDS and other infectious diseases and on improving maternal and child health . There is no link made to NCDs, although some researchers such as Stuckler et al. (2010) warned that the MDGs might not be reached without addressing NCDs as cofactors for communicable diseases.
The same logic of division continued to dominate the debate when the world began to address the NCD epidemic. In 2005, the World Health Organization acknowledged in its report “Preventing chronic diseases: a vital investment” that NCDs are not primarily and exclusively a problem of the older and richer countries, but are even more so for the developing world. New research data had shown for instance that some 80% of all cardiovascular disease related deaths occur in low and middle-income countries (WHO 2005).
In 2011, the United Nations General Assembly (UNGASS), in its political declaration on the prevention and control of NCDs, committed all governments to fight the epidemic of NCDs. This declaration also acknowledged that NCDs hit developing countries particularly hard (UNGASS 2012). In 2013 the World Health Assembly adopted the “WHO Global Action Plan for the Prevention and Control of NCDs 2013–2020”. By doing so, they confirmed and reinforced the concept of a double agenda.
Overall, the concept of a “double burden of disease ” is a success story. It has unleashed an unprecedented global response to address the unfinished agenda of infectious diseases, particularly in Africa. It has brought governments , international organizatio ns, the private sector , NGOs and philanthropic organizations together. It was instrumental in launching the Global Alliance for Vaccines and Immunization GAVI (2000), the Global Fund to fight AIDS, Tuberculosis and Malaria GFATM (2002) and for the inclusion of the fight against the major infectious diseases in the Millennium Development Goals Agenda. Finally, the concept mobilized civil society and political leaders in 2011 to adopt a global target of a 25% relative reduction in overall mortality from cardiovascular disease, cancer , diabetes or chronic respiratory diseases by 2025.
In his 2012 Science Perspective paper, I.C. Bygbjerg rightly points to three possible and unintended side effects of this double approach (Bygbjerg 2012):
-
It does not take into account the growing scientific evidence of links between infectious diseases (particularly TB and HIV) and NCDs (particularly diabetes, cancer and chronic obstructive lung diseases) or the importance of improved maternal and child health in the prevention of NCDs.
-
It creates a competition in resource allocation between the two areas : “At a time of global financial crises and shrinking health budgets, there is a threat that the battle against common and future health problems, both communicable and non-communicable, may become a fight for funds to control either health problem, rather than a fight against the double burden of disease .”
-
It blurs the fact that a comprehensive “double burden of disease ” policy requires integrated control strategies that have to begin in the primary health care sector and need a multidimensional approach.
The dual approach in addressing the burden of two disease groups was, however, necessary for political reasons. The HIV/AIDS crisis of the end of the 20th century and the high burden of communicable diseases in low and middle-income countries made it imperative to address the challenge of infectious diseases as a high priority. A delay would not have been understood and could have jeopardized the willingness of low-income countries to cooperate with high-income countries in the area of newly emerging and re-emerging infectious diseases, such as SARS , or pandemic s of different strains of the influenza virus. It might also have affected their willingness to collaborate with the WHO and its Global Outbreak Alert and Response Network , established in 2000.
The challenge for Governments and particularly for Ministries of Health in SSA, is how to address the two burdens of disease in tandem. Internationally they have to negotiate with organizations active in one or the other field. On the national and subnational level they have to come up with public health responses that take into account the need of their populations for an integrated control strategy.
2 Changing Patterns of Diseases and Mortality in Sub-Saharan Africa
2.1 The Development of the Burden of Disease and of Mortality in SSA Between 1990 and 2010
The publication of the World Bank Disease and Mortality in sub-Saharan sub-Saharan Africa (Jamison et al. 2006) and the 2013 report of the Institute of Health Metrics on the Global Burden of Disease (sub-Saharan Africa regional edition, IHME 2013) give a comprehensive report of the actual burden of diseases in the region. The overall findings were:
-
1.
Non-communicable diseases and disability caused a greater share of health loss in 2010 compared to 1990 in most regions of the world. At the same time the leading causes of disability-adjusted life years (DALYs) in SSA have changed little over the past 20 years. There is, however, evidence for progress made in SSA in the reductions in mortality from malaria, HIV/AIDS , and in maternal conditions.
-
2.
Remarkable declines in health loss from diarrheal diseases, lower respiratory infections , and measles have been achieved. Despite this progress, many of these conditions still top many countries’ health burdens and account for a large portion of childhood death and illness. Malaria and HIV/AIDS continue to drive substantial health loss throughout the region, and do so at rates higher than those two decades earlier; it appears, however, that the total health burdens caused by these diseases peaked between 2000 and 2005 for most countries.
-
3.
While most countries in SSA still face large health burdens due to communicable, neonatal, maternal , and nutritional conditions, many have also experienced an increasing disease burden due to injuries and non-communicable diseases from 1990 to 2010. These dual burdens of communicable and non-communicable diseases are largely found among the lower- and upper-middle-income countries , but even low-income countries are now seeing ailments such as stroke among their top 10 drivers of premature death and disability. Road injuries have become an increasingly dominant cause of health loss in the region, with many countries, including Ghana, Kenya, and Nigeria, documenting at least twice the health burden caused by road injuries in 2010 than in 1990.
-
4.
War and conflict affected many countries in SSA in 1990, accounting for a substantial amount of health loss in countries such as Ethiopia and Liberia ; by 2010, these causes were no longer primary drivers of premature death and disability.
-
5.
Overall, a number of risk factors, including suboptimal breastfeeding, vitamin deficiencies , childhood underweight , and others associated with under-nutrition , have declined throughout SSA. This has likely contributed to the regional progress in reducing health loss caused by several childhood conditions. However, risk factors associated with growing burdens of chronic diseases, such as high body mass index and physical inactivity , have become important threats to public health in many countries in the region (Fig. 1).
Fig. 1 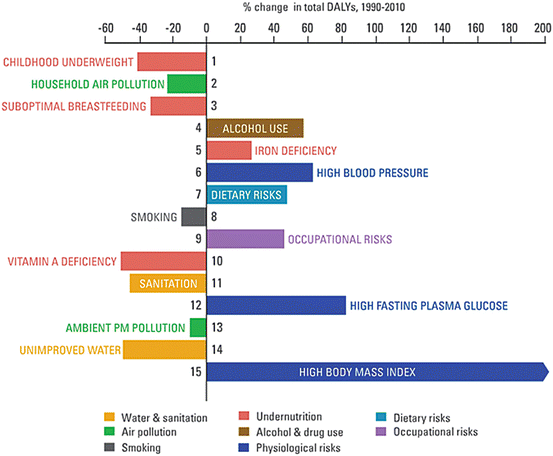
Shifts in ranking of DALYs in SSA for top 15 risk factors, 1990–2010 (Source: IHME, Human Development Network, The World Bank. The Global Burden of Disease: Generating Evidence, Guiding Policy — Sub-Saharan Africa, Regional Edition. Seattle, WA: IHME, 2013)

The leading 15 risk factors are ranked from top to bottom in order of the number of DALYs they contributed in 2010. Bars going right show the percentage by which risk factors have increased since 1990. Bars going left show the percentage by which risk factors have decreased. Pointed arrows indicate causes that have increased by a greater amount than shown on the x-axis.
2.2 Projection of the Burden of Disease and the Mortality in SSA Until 2030
Shona Dalal et al. (2011) reviewed the literature for SSA and summarized the data of the WHO and of the International Agency for Research on Cancer. Based on this review, the authors predict that the burden of NCDs such as cardiovascular diseases, diabetes mellitus type 2, and cancer will grow in SSA. There is, however, a substantial amount of uncertainty because there are few community-based studies that examine the NCDs prevalence, incidence, and risk factors and allow for a projection. Furthermore the prevalence of NCDs and risk factors varies considerably between countries, urban/rural locations, and other sub-populations. The prevalence of stroke ranged from 0.07 to 0.3%, diabetes mellitus from 0 to 16%, hypertension from 6 to 48%, obesity from 0.4 to 43%, and current smoking from 0.4 to 71%. Hypertension prevalence was consistently similar among men and women, whereas women were more frequently obese and men were more frequently current smokers. The authors therefore call for more research in Africa to provide evidence for NCDs prevention and treatment in SSA.
Based on their analyses the authors summarize the estimated proportion of age-standardized mortality rates for communicable and non-communicable diseases, injuries as well as for maternal , perinatal, and nutritional causes between 2002 and 2030 as shown in Fig. 2.

Estimated proportions of age-standardized mortality rates by cause in SSA (Source: WHO. Global Burden of Disease . Projections of mortality and burden of disease , 2002–2030. SSA mortality estimates were standardized to the WHO World Standard Population)
3 Challenges/Solutions
Sub-Saharan Africa faces the challenge of building and strengthening health systems that address its dual burden of disease effectively, equitably and sustainably. In doing so, it must recognize its pioneering role, as there are no equivalent models to learn from. While many countries have effectively solved their infectious disease challenges, and while there are more and more (but still sub-scale) examples of managing NCDs well in resource-limited settings, no country can be held up as a role model for success in tackling the challenges facing SSA.
The problem is two-fold. Firstly, the types of policies and delivery systems that work for infectious diseases are often different from those that work for chronic conditions . Secondly, even if these systems were both available, integrating them into a coherent, unified health system is a very difficult task. This becomes clearer as we look at specific challenges and examples of progress:
3.1 Leadership and Policy Challenges
The challenge of getting the dual burden of disease onto an already crowded global health and development agenda has already been raised above. This challenge is further complicated by some differences between infectious diseases and chronic ones: (1) for most infectious diseases, there is a relatively high consensus on the technical interventions and on appropriate policies and delivery systems; for most chronic diseases, the technical consensus is mostly there, but not yet accompanied by broad agreement on policy and delivery options . Efforts such as the WHO’s NCD “best buys” (WHO 2011a) represent a good path forward. (2) For most infectious diseases, the time lapse between starting interventions and seeing improvements in mortality and morbidity is low – months or years; for most chronic diseases, it is high – years to decades. National leaders will need to define success, progress, and interim milestones in ways that ensure implementation and support through multiple political cycles. (3) Most infectious disease programs are administered by the public sector, with limited private sector involvement; much of chronic disease care in SSA is delivered and insured by the private and non-profit sectors. National leaders will have to determine the role and extent of the different sectors and of public-private partnerships, to maximize population health benefits and equity of access.
3.2 Infrastructure and Input Challenges
The challenge is in expanding the healthcare infrastructure in SSA beyond that which is required for managing infectious diseases, to also being able to support prevention, diagnosis, treatment, and palliation of a broad range of chronic conditions . Furthermore, this expansion must be affordable, sustainable, and adaptable for the future. There are many examples of possible solutions to these challenges, many of which are being developed and implemented in SSA, for example:
-
Physical infrastructure: it is far more cost-effective to manage chronic conditions in outpatient and near-home settings than it is to build more acute-care facilities. Mobile technology is making it increasingly feasible and cost-effective for care to be delivered by front-line healthcare workers in the community, and even by patients themselves. The WHO and International Telecommunicatio ns Union (ITU) Health Initiative are bringing together governments and private sector partners to develop, pilot, and scale up successful mobile-based tools and applications for the prevention and treatment of chronic diseases (WHO 2012).
-
Medical equipment: the equipment required for the diagnosis and treatment of many chronic conditions conditions (e.g., CT scanners , MRI scanners, cardiac pacemaker s) has historically been priced beyond what most health systems in sub-Saharan Africa could afford. This situation is changing, both as manufacturers from other countries such as India and China enter the market, and as the main Western manufacturers (e.g., Medtronic, GE, Siemens) recognize the need and opportunity for “frugal innovation”, expand R&D activities in developing countries, and develop products which are not only considerably cheaper, but also technologically advanced and adapted for use in local settings (Economist 2011).
-
Medicines: many chronic conditions conditions (and indeed many infectious diseases) can today be managed well with relatively affordable generic medicines. However, in much of Africa, there are still major barriers to access, caused by inefficient supply chains and by complex national regulations that are not yet harmonized with each other. These issues have been recently evaluated and a set of recommendations developed in Galambos and Sturchio (2013).
3.3 Financial Resourcing and Sustainability Challenges
The financial resources dedicated to the health sector in SSA (public and private, preventative and curative) have been and still are very low. They are in the same order of magnitude as in India, but represent only 2% of what is spent on health per capita in the OECD countries . In 2005 health expenditures per capita were at low US$ 59.7 in sub-Saharan African countries, compared to US$ 709.1 worldwide (8.33%). Till 2012 they have grown to US$ 96.2, representing a growth rate of 61.1% (Fig. 3).

Health expenditure per Capita (current US$) (Source: World Health Organization National Health Account database, World Development Indicators) (See http://apps.who.int/nha/database (accessed 25 June 2016) for the most recent updates)
Total health expenditure is the sum of public and private health expenditures as a ratio of total population. It covers the provision of health services (preventive and curative), family planning activities, nutrition activities, and emergency aid designated for health but does not include provision of water and sanitation. Data is in current U.S. dollars.
Data of 2013 show that 44% comes from public sources. In about half of African countries, 40% or more of the total health expenditure is constituted of household out of pocket payments, which is the most regressive way of funding health care . The reliance on this payment mechanism creates financial barriers to access to health services and puts people at the risk of impoverishment (WHO 2013).
The funding of the health sector is lagging behind the promises made by the African Union countries in 2001.
In that year, 53 of the African Union countries, during a meeting in Abuja, Nigeria, pledged to increase government funding for health to at least 15% and urged donor countries to scale up support. Ten years later only one African country had reached this target. Overall, 26 have increased the proportion of government expenditures allocated to health and 11 have reduced it since 2001. In the other 9, there was no obvious trend up or down (WHO 2011b). At the same time a substantive number of African countries continue to significantly depend upon external (international) sources to finance their health sector (World Bank data 2012, see Table 1).
A major challenge is the long “payback time” of many chronic diseases. Investments in primary prevention pay back financially in decades, investments in secondary prevention in years. It is possible to develop lower-cost, high-quality delivery systems to meet this challenge, and indeed this is already happening in many countries, in particular India. The Naryana Cardiac Clinics for example, established in 2001, have become Asia’s largest cardiac care center with hospitals and outpatient facilities in 17 cities in India. Their focus on high volumes, high throughput, and “lean” processes has allowed them to deliver more affordable cardiac surgery at a fraction of the cost in the West with outcomes that are global best practice: their mortality rate of 2% and hospital-acquired infection rate of 2.8% per 1000 intensive care unit days are comparable with the best hospitals in the world. This focus, along with a tiered pricing model, allows them to serve all income levels and not turn anyone away because of his or her inability to pay (see case study, Reform UK 2014). Naturally economic sustainability can also be helped by focusing more on diseases that primarily affect working-age and income -earning populations (e.g., diabetes rather than dementia), but policy-makers must also address the issues of equity across generations and socioeconomic classes.
3.4 Prevention and Health Promotion
While prevention is almost always seen as superior to treatment, SSA faces some real challenges in this area. As shown by the figures above, the burden of chronic disease is already high and many people already need care, not just prevention. In addition, prevention and health promotion for metabolic and cardiovascular conditions depend to a large extent on individual and population behavior modification, and the interventions that support these are complex and often require coordination across multiple government agencies. For example:
-
Developing integrated transport and urban design policies that favor activity and exercise;
-
Developing food supply and nutrition policies that support healthy eating;
-
Determining the balance of individual freedom and business freedom vs. population health priorities.
Perhaps the biggest opportunity is in tobacco control. Smoking rates are relatively low in SSA, and if governments can keep citizens from starting to smoke, the health and economic payoff will be huge. The WHO’s Framework Convention for Tobacco Control and associated guidelines for tobacco control are relevant here, as is the experience of countries that have successfully reduced tobacco use, such as Brazil.
Box 1:Country Example: Ghana
Ghana, like many other low and middle income countries, has gone through a transition in which the major cause of death has shifted away from predominantly communicable diseases to a combination of communicable and non-communicable diseases (NCDs). The WHO (2014) estimates that 42% of all deaths in Ghana can be accounted to NCDs. In 2012 NCDs killed roughly 84,000 people. The leading cause for NCD death is cardiovascular diseases, which account for 18% of all death or 37,800 persons. However, contrary to widespread beliefs, not only older generations are affected. The probability of dying between the exact ages of 30 and 70 from any cardiovascular disease, cancer, diabetes, or chronic respiratory diseases amounts to 20% (WHO 2014). The increase in the NCD burden is on the one hand related to the achievement of population ageing and on the other hand to modifiable risk factors of which many are linked to rapid urbanization and unhealthy lifestyles. Ghana’s NCD burden is expected to further increase due to the continued development of the aforementioned factors.
In August 2012 the Ministry of Health published the “National Policy for the Prevention and Control of Chronic Non-Communicable Diseases in Ghana”. This policy defines the broad path which Ghana wants to follow in order to prevent and control NCDs. In line with the WHO, the country’s NCD policy focuses on cardiovascular diseases, diabetes, cancers, and chronic respiratory diseases (Ghana Ministry of Health 2012). These four NCDs share risk factors and therefore allow for a coordinated approach. To tackle these four NCDs the policy defines five strategic areas, namely: primary prevention, early detection and clinical care, strengthening of the health system, research and development, and the surveillance of NCDs and their respective risk factors.
One of the most recent and most prominent initiatives launched was the “Ghana Access and Affordability Program” (GAAP). The GAAP is a public/private partnership which aims to provide safe and affordable medicine for the treatment of NCDs. Ghana is one of three countries that have been selected to pilot this program (Ghana News Agency 2014).
The national policy outlines an ambitious strategic plan. First steps into the right direction have already been taken and measures have been implemented. Nevertheless, Ghana is still showing deficits in certain areas, for example the failure to put a NCD surveillance and monitoring system in place (WHO 2014). Such a system would allow the country to report results against the nine global NCD targets defined by the WHO. Furthermore, it would provide higher transparency to the decision makers and other countries keen to learn from Ghana’s experiences.
4 Outlook
4.1 The International Framework
Four global frameworks will impact upon the development of the health agenda of the sub-Saharan African Countries:
-
1.
The Millennium Development Goals (MDGs) 2000–2015, adopted at the Millennium Summit of the United Nations in 2000;
-
2.
Report of the UN High Level Panel to strengthen national and international systems to prevent and manage future health crises such as the Ebola crisis (2015);
-
3.
The WHO Global Action Plan for the Prevention and Control of NCDs 2013–2020 , adopted by the World Health Assembly in 2013;
-
4.
The Sustainable Development Goals , proposed to replace the MDGs and adopted by the United Nations in September 2015.
The MDGs and the “Ebola-Report” will continue to influence national and regional responses to infectious diseases, particularly to Malaria, TB and HIV/AIDs, as well as to health crises caused by infectious diseases.
The latest report on the achievement of the MDGs concludes that the lives of an estimated three million children under age five were saved from malaria due to coordinated interventions in sub-Saharan Africa between 2000 and 2012. The report says that SSA is on its way to halting the spread of and reversing the incidence of tuberculosis. The incidence of new HIV cases in the region fell by more than half between 2001 and 2012. SSA has the second highest rate of access to treatment for HIV/AIDS , with 63 per cent of people living with HIV receiving antiretroviral therapy in 2012. However, sub-Saharan Africa remains most severely affected by HIV. Seventy percent of the estimated number of new infections in 2012–1.6 million cases – occurred in the region.
Most importantly, the MDGs have had a major impact on the social determinants of health in SSA. From 1981 to 1999, extreme poverty in sub-Saharan Africa rose from 52% of the population to 58%. But since the launch of the MDGs, it has declined sharply, to 48% in 2008. Much of this was likely driven by MDG-backed investments in healthier and better-educated work forces in the region (McArthur 2013). Finally, the report concluded that the SSA region will not meet most of its goals by their 2015 target date.
The countries of the African Union decided therefore in 2014 on a Common African Position (CAP) on the Post-2015 Development Agenda (African Union 2014). Concerning the health agenda they committed themselves to continue their efforts “in reducing the incidence of communicable diseases, non-communicable diseases (e.g. mental health) and emerging diseases; ending the epidemics of HIV and AIDS, tuberculosis and malaria; reducing malnutrition; and improving hygiene and sanitation. This can be achieved by: ensuring universal and equitable access to quality healthcare, including access to comprehensive sexual reproductive health and reproductive rights (e.g. family planning), improving health systems and health financing and medical infrastructure, the local manufacturing of health equipment (e.g. commitment to the Abuja Declaration); and setting up monitoring and evaluation, and quality assurance systems.”
The Millennium Development Goals have mobilized governments and the business sector to donate tens of billions of US$. Not so the WHO Global Action Plan for the Prevention and Control of NCDs 2013–2020. It is a non-binding set of recommendations to the member states of the WHO aiming to reduce the number of premature deaths from NCDs by 25% by 2025 through nine voluntary global targets. The nine targets focus in part on addressing factors such as tobacco use, harmful use of alcohol, unhealthy diet, and physical inactivity that increase people’s risk of developing these diseases. The plan offers a menu of “best buy” or cost-effective, high-impact interventions for meeting the nine voluntary global targets. These include banning all forms of tobacco and alcohol advertising, replacing trans fats with polyunsaturated fats, promoting and protecting breastfeeding, and preventing cervical cancer through screening.
Given the non-compulsory nature of the action plan, special efforts are needed to raise awareness on the NCDs and scale up efforts to address NCDs in the different countries. Supranational coalitions, such as the East African NCD Alliance Post-2015 Initiative, have been formed to convince governments and civil society of the urgent need for action locally and internationally (The East Africa NCD Alliance Initiative, 2014). They also advocate for the inclusion of a health specific target in the Agenda of the Sustainable Development Goals.
4.2 Integrated Approaches to Address the Double Burden of Disease
By now, many SSA countries have recognized NCDs as a national health and development priority and have started formulating national NCD plans (see Box 1, Country Example Ghana). A particular problem remains often unresolved, however: namely how to gear up to the challenge of non-communicable diseases in a way that avoids creating new vertical programs in competition for scarce resources.
Much focus has been given in the past years to identify the most cost-effective intervention for a specific disease and multi-sectoral approaches have not yet been developed. Marquez and Farrington (Marquez and Farrington, 2012) have proposed a 3-line approach to overcome silo thinking and acting within SSA countries:
-
(a)
Capitalize on the links between communicable and non-communicable diseases and the underlying social conditions. People diagnosed with HIV/AIDS can be screened for hypertension and diabetes; immunization programs can be expanded to include not only vaccine preventable diseases, but also HPV vaccines to protect against cervical cancer;
-
(b)
Focus on common care needs rather than disease categories. Care models for HIV/AIDS and tuberculosis can be extended and adapted to chronic conditions and comorbidities. Projects to integrate and improve quality of care for chronic conditions such as HIV, hypertension, and diabetes are already underway in Uganda, Tanzania, and South Africa.
-
(c)
Capitalize on existing resources and capabilities. The case has been made for reshaping primary healthcare as part of a continuum of care involving coordinated primary, secondary, and tertiary care as well as the community with patients at the center.
International support is still too often disease specific and will continue to be so. Countries therefore have to negotiate collaborations between “silos” and integrate the different international support chains nationally.
A final challenge to be addressed is how to engage with the private sector entities without getting trapped in major conflicts of interest. In the 1980s, multi-sectoral collaboration for health meant creating productive working relationships with sectors such as education, housing, nutrition, water supply and sanitation, and particularly meant productive collaboration with other governmental sectors. Today and in the years to come multi-sectoral collaboration consists of offering people the opportunity to adopt a healthy lifestyle and live in an environment preventing them from developing NCDs. This approach could go against the interests of whole business sectors. The WHO has developed guidelines and strategies on how to engage with private sector entities that should allow for a transparent and productive collaboration, which would reduce the risk of a conflict of interest. The reality check of how well they will function in the context of SSA countries is, however, still outstanding.
References
African Union. (2014). Common African position (CAP) on the post-2015 development agenda. Addis Ababa: African Union. http://www.nepad.org/sites/default/files/Common%20African%20Position-%20ENG%20final.pdf. Accessed 30 July 2015.
Bygbjerg, I. C. (2012). Double burden of non-communicable and infectious diseases in developing countries. Science, 337(6101), 1499–1501.
Dalal, S., Beunza, J. J., Volmink, J., Adebamowo, C., Bajunirwe, F., Njelekela, M., Mozaffarian, D., Fawzi, W., Willett, W., Adami, H. O., & Holmes, M. D. (2011). Non-communicable diseases in sub-Saharan Africa: What we know now. International Journal of Epidemiology, 40(4), 885–901.
Economist. (2011). Frugal healing. http://www.economist.com/node/17963427. Accessed 30 July 2015.
Galambos, L., & Sturchio, J. L. (2013). Non-communicable diseases in the developing world: Addressing gaps in global policy and research. Baltimore: Johns Hopkins University Press.
Ghana Ministry of Health. (2012). National policy for the prevention and control of chronic non-communicable diseases. http://www.iccp-portal.org/sites/default/files/plans/national_policy_for_the_prevention_and_control_of_chronic_non-communicable_diseases_in_ghana%281%29.pdf. Accessed 30 July 2015.
Ghana News Agency. (2014). Ghana access and affordability programme launched. http://www.ghananewsagency.org/health/ghana-access-and-affordability-programme-launched-71085. Accessed 30 July 2015.
Institute for Health Metrics and Evaluation, & Human Development Network, The World Bank. (2013). The global burden of disease: Generating evidence, guiding policy – Sub-Saharan Africa (Regional ed.). Seattle: IHME.
Jamison D. T., Feacham, R. G., Makgoba, M. W., Bos, E. R., Baingana, F. K., Hofman, K. J., & Rogo, K. O. (2006). Disease and mortality in sub-Saharan Africa (2nd ed.). Washington, DC: World Bank. https://openknowledge.worldbank.org/handle/10986/7050. Accessed 30 July 2015.
Marquez, P., & Farrington, J. (2012). No more disease silos for sub-Saharan Africa. BMJ, 345, e5943. http://www.bmj.com/content/345/bmj.e5812.full?ijkey=6ASzFlPzz6TrKkW&keytype=ref. Accessed 30 July 2015.
McArthur, J. W. (2013). Own the goals. What the millennium development goals have accomplished. http://www.foreignaffairs.com/articles/138821/john-w-mcarthur/own-the-goals. Accessed 30 July 2015.
Murray, C. L., & Lopez, A. D. (1996). The Global burden of disease. A comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Cambridge, MA: Harvard School of Public Health on behalf of the World Health Organization and the World Bank.
Omran, A. R. (1971). The epidemiologic transition. A theory of the epidemiology of population change. The Milbank Memorial Fund Quarterly, 49(4/1), 509–538.
Reform UK. (2014). High volume, specialist cardiac care in Bangalore, India. http://ww.reform.co.uk/wp-content/uploads/2014/11/Naryana_Hrudayalaya.pdf. Accessed 30 July 2015.
Stuckler, D., Basu, S., & McKee, M. (2010). Drivers of inequality in millennium development goal progress: A statistical analysis. PLoS Medicine, 7(3), e1000241.
The East Africa NCD Alliance Initiative. (2014). Responses to NCDs in East Africa. http://www.uncda.org/sites/default/files/resources/East%20Africa%20NCD%20Alliance%20Civil%20Society%20Survey%20Report_v5_layouted.pdf. Accessed 30 July 2015.
UNGASS. (2012, January 24). Political declaration of the high-level meeting of the general assembly on the prevention and control of non-communicable diseases. Resolution 66/2. New York: United Nations General Assembly. http://www.who.int/nmh/events/un_ncd_summit2011/political_declaration_en.pdf?ua=1. Accessed 30 July 2015.
WHO. (1999). The double burden: Emerging epidemics and persistent problems (The World Health Report 1999). Geneva: World Health Organization. http://www.who.int/whr/1999/en/whr99_ch2_en.pdf. Accessed 30 July 2015.
WHO. (2005). Preventing chronic diseases: A vital investment. In WHO global report. http//apps.who.int/iris/handle/10665/43314/1/9241563001_eng.pdf. Accessed 10 Dec 2016.
WHO. (2011a). From burden to “best buys”: Reducing the economic impact of NCDs in low- and middle-income countries. Geneva: World Health Organization. http://www.who.int/nmh/publications/best_buys_summary/en. Accessed 30 July 2015.
WHO. (2011b). The Abuja declaration: Ten years on. Geneva: World Health Organization. http://www.who.int/healthsystems/publications/abuja_declaration/en. Accessed 30 July 2015.
WHO. (2012). ITU and WHO launch health initiative to combat non communicable diseases. Geneva: World Health Organization. http://www.who.int/nmh/events/2012/mhealth/en. Accessed 30 July 2015.
WHO. (2013). Global action plan for the prevention and control of noncommunicable diseases 2013–2020. Geneva: World Health Organization. http://apps.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf. Accessed 10 Dec 2016.
WHO. (2014). World Health Organization – Non communicable diseases (NCD) country profiles. Geneva: World Health Organization. http://www.who.int/nmh/countries/gha_en.pdf?ua=1. Accessed 30 July 2015.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Zeltner, T., Riahi, F., Huber, J. (2017). Acute and Chronic Health Challenges in Sub-Saharan Africa: An Unfinished Agenda. In: Groth, H., May, J. (eds) Africa's Population: In Search of a Demographic Dividend. Springer, Cham. https://doi.org/10.1007/978-3-319-46889-1_18
Download citation
DOI: https://doi.org/10.1007/978-3-319-46889-1_18
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-46887-7
Online ISBN: 978-3-319-46889-1
eBook Packages: Social SciencesSocial Sciences (R0)