
Abstract
Hematopoietic stem cell transplantation offers patients the only prospect of long-term survival for a substantial variety of otherwise incurable malignant neoplasms as well as selected non-neoplastic conditions. This therapeutic modality, however, carries significant risks and is associated with a wide range of complications affecting not only the bone marrow but many organ systems, in particular by graft-versus-host disease. Patients before, during, and following stem cell transplantation thus require close monitoring and the pathologist is frequently implicated in this process. The aim of this chapter is to provide the pathologist with the tools required to interpret biopsies from these patients at all stages of the transplantation process. Following an overview of hematopoietic stem cell transplantation and graft-versus-host disease, the chapter will focus on the histopathologic findings of graft-versus-host disease and other complications in several organs and tissue including bone marrow, skin, lung, kidney, gastrointestinal tract and liver, with emphasis on the diagnostic criteria and approaches to graft-versus-host disease.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Hematopoietic stem cell transplantation
- Autologous stem cell transplantation
- Allogeneic stem cell transplantation
- Graft-versus-host disease
- Idiopathic pneumonia syndrome
- Bronchiolitis obliterans
- Sinusoidal obstruction syndrome
Introduction, History, and General Concepts
Hematopoietic stem cell transplantation (HSCT), defined as the process of infusing hematopoietic stem and progenitor cells intravenously to re-establish normal hematopoiesis in states of marrow failure, is an important strategy to treat a variety of malignant and non-malignant conditions. Of note, the term HSCT has supplanted the term bone marrow transplantation (BMT) as hematopoietic stem cells can be obtained from several sources other than bone marrow, e.g., peripheral blood and umbilical cord blood [1–4]. By definition these cells are of hematopoietic origin, to differentiate them from other types of stem cells derived from bone marrow such as endothelial progenitors used in revascularization therapy of the myocardium, limbs and others sites [5].
The concept of utilizing bone marrow as a form of therapy dates back as far as the Middle Ages but even attempts in the early and mid-twentieth century achieved only a modicum of success. An important driving force for the development of this therapy came in part from the observation of the marked myelosuppressive and other toxic effects of radiation in survivors of the nuclear bomb attacks in Hiroshima and Nagasaki [6]. Although attempts at allogeneic BMT in the 1950s and 1960s were fraught with difficulties, advances in the understanding of the major histocompatibility complex (MHC) and human leukocyte antigens (HLA) as key factors in graft rejection provided the framework for further experimental studies and clinical application of allogeneic HSCT [1, 7]. HSCT came of age in the 1970s, when the Seattle group and others reported improved outcomes in the treatment of aplastic anemia and acute leukemia [8–12]. Further advancements were reported in the 1980s with the introduction of improved conditioning regimens, potent immunosuppressive drugs and novel antibiotics for viral and fungal infections [13].
The early days of autologous HSCT was similarly marked by alternating successes and failures. It was initially used to treat patients with non-Hodgkin lymphoma in the late 1970s followed by selected solid malignancies and Hodgkin lymphoma in the 1980s [14]. In the earliest protocols, autologous bone marrow was infused. Later approaches utilized hematopoietic cells derived from peripheral blood. In the mid to late 1980s the addition of hematopoietic growth factors such as G-CSF and GM-CSF was an important modification of the technique that significantly increased the yield of stem cells [15, 16]. Detailed historical aspects of HSCT can be found in several excellent reviews [1, 7, 13, 14, 17].
Currently, the major categories of HSCT are (1) autologous HSCT in which the stem cells are obtained from the patient’s own bone marrow or peripheral blood and re-infused following conditioning, (2) syngeneic HSCT, where donor cells are from an identical twin, and (3) allogeneic HSCT where the donor cells come from another donor. The choice of autologous vs. allogeneic depends on the availability of a donor and the underlying condition. In general, allogeneic HSCT is indicated when the bone marrow or peripheral blood harbors a significant tumor burden. However, each type has specific indications, limitations, and complications.
Autologous HSCT
Following poor outcomes in the 1960s and early 1970s and initial enthusiasm for allogeneic HSCT, autologous HSCT (auto-HSCT) regained clinical favor in the late 1970s in reaction, in part to the shortcomings of allogeneic HSCT, namely graft-versus-host disease (GvHD) and to the difficulty of finding suitable donors [18, 19]. Auto-HSCT facilitates the prompt reconstitution of a markedly depleted or ablated marrow following very aggressive chemotherapy and radiotherapy intended to eradicate hematologic and non-hematologic malignancies.
The general principles on which autologous HSCT are founded include (1) the sensitivity of the malignancy to chemotherapy, specifically the ability to ablate the marrow with aggressive salvage therapy, (2) the timing of the transplant, i.e., as part of the primary therapy vs. first or second relapse, and (3) the specific biological characteristics of the malignancy, e.g., cytogenetic subgroups in acute myeloid leukemia [19].
Current indications for autologous HSCT include (1) refractory or relapsed Hodgkin and aggressive non-Hodgkin lymphoma and germ cell tumors, (2) plasma cell myeloma after induction therapy, (3) mantle cell lymphoma in first remission, and (4) acute myeloid leukemia in second remission if an allogeneic bone marrow donor is unavailable. Less common indications include low-grade B-cell lymphomas, breast cancer, and autoimmune diseases [19]. In the overwhelming majority of patients, peripheral blood is the source of the stem cells [20].
The advantages of autologous over allogeneic transplantation include the absence of graft-versus-host and the reduced intensity of the conditioning regimens. The drawbacks are the potential inability to harvest the patient’s stem cells, the relapse of the original malignancy (by contamination of the donor cells), the general toxicity of the conditioning process, the absence of the graft-versus-malignancy response, as well as the late development of secondary malignancies such as myelodysplastic syndrome and acute myeloid leukemia.
Allogeneic HSCT
Allogeneic HSCT is used for both hematopoietic malignancies and non-malignant conditions, and as salvage therapy in patients not responding to standard chemotherapy or radiotherapy, or following failure of autologous HSCT. The general principles of allogeneic HSCT include: (1) it enables the rescue of patients following administration of potentially myeloablative doses of chemotherapy and radiation in aggressive diseases or following the development of resistance to conventional therapeutic doses, and (2) it exerts a significant graft-versus-malignancy response that potentiates eradication of the malignancy and prevention of recurrence. Data from the Center for International Blood and Marrow Transplant Research (CIBMTR ) reported a total of 8860 allogeneic transplants in the USA in 2010. The most frequent indications were acute myeloid leukemia (about one-third of cases), acute lymphoblastic leukemia and myeloproliferative/myelodysplastic disorders (each about 10–15 %), followed by smaller percentages of patients with non-Hodgkin lymphomas, chronic myeloid leukemias, other leukemias, aplastic anemia and other non-malignant conditions, plasma cell myeloma and Hodgkin lymphoma [20].
The procedure entails a conditioning regimen of chemotherapy, immunosuppressant drugs, and/or radiation followed by infusion of donor hematopoietic stem cells. Immunosuppressive therapy is subsequently administered to prevent or treat GvHD. The conditioning regimen serves two purposes: to eliminate malignant cells and to diminish the recipient’s immune response and thereby prevent the rejection of the donor hematopoietic cells [21]. Currently, reduced intensity conditioning regimens have expanded the pool of recipients, especially older patients who poorly tolerated the associated toxicity, and lowered transplant-related mortality, although this advantage is offset by higher relapse rates [21]. Further details pertaining to procedures and other therapeutic measures are available in several detailed publications [1, 19, 21, 22].
The source of stem cells between 2005 and 2010, according to the CIBMTR database, in patients over the age of 20, was peripheral blood (80 %), bone marrow (15 %), and cord blood in 5 % of cases. In pediatric patients and young adults up to age 20, the distribution was 25 %, 50 %, and 25 %, respectively. Although analysis of the advantages and drawbacks of each of these sources is dependent on multiple variables and beyond the scope of this chapter, in general peripheral blood stem cells appear to engraft at the highest rate and are associated with a better survival in some disorders, but produce higher rates and severity of GvHD [21].
The causes of mortality in patients undergoing HSCT reported by the CIBMTR vary with the primary source of the stem cells: in autologous HSCT, 72 % of deaths are due to the primary disease, 7 % to infection; when HLA-identical siblings are donors, 49 % die from the primary disease, 16 % from GvHD, and 13 % from infection whereas with unrelated donors the respective percentages are 37, 18, and 18 % [20].
Role of the Pathologist Pre- and Post-HSCT
The pathologist plays an important role in the management of patients both prior to and following HSCT. These include (1) the pre-transplant assessment or confirmation of the primary disease (malignant or non-neoplastic) and/or the disease status of remission or relapse, (2) the posttransplant evaluation for potential complications and possible recurrence of the original disease.
The pre-transplant evaluation is discussed in detail in standard texts of hematopathology including the WHO classification of tumors of the hematopoietic and lymphoid tissues [23–25]. Highlights of important points include firstly the evaluation of the bone marrow, ensuring the precise typing of the myeloproliferative, myelodysplastic or leukemic disorder and assessing the amount of residual disease, if any. For the lymphoma patients, the bone marrow is evaluated to ensure absence of disease prior to autologous HSCT. In the setting of aplastic anemia, mimics such as myelodysplastic syndrome must be ruled out. Also important is assessing the presence of any fibrosis in the marrow that may delay engraftment [26, 27]. Secondly, the possibility of preexisting hepatic disease should be evaluated in selected patients as it may portend the development of sinusoidal obstructive syndrome (previously termed veno-occlusive disease) and related entities discussed in detail below [27].
The role of the pathologist is particularly important in the posttransplant setting, especially in the assessment of complications. There are myriad side effects related to radiation and chemotherapy administered as part of the conditioning process. These occur most frequently in the bone marrow, but other organs such as the liver, heart, and lungs may be affected; these complications occur early on after transplantation. The pathologist also has a critical role in diagnosing other complications such as immunologically mediated graft rejection and graft-versus-host disease later on post-HSCT. Looking for possible infections posttransplant must always be part of the assessment and differential diagnosis of any biopsy performed to assess organ dysfunction following HSCT. Infections should be sought for diligently with appropriate histochemical and immunohistochemical stains, and be correlated with microbiological findings [28–30]. Also important is the assessment of potential reactions to the panoply of drugs the patients usually receive. Lastly, the pathologist is vital in the diagnosis of posttransplant recurrence of the primary malignancy and in the detection of “de novo” neoplasms; on the topic of de novo posttransplant malignancies, the reader is referred to chapter “Transplantation and Malignancy”.
The remainder of the chapter will focus on GvHD and other organ-specific complications following HSCT.
Graft-versus-host disease: General Concepts
GvHD develops as a complication of HSCT for a number of reasons: (1) the graft is composed of immunologically competent cells, (2) recipient cells express different antigens from those of the graft, and (3) the recipient does not generate an effective immunologic response to the engrafted donor cells [31].
According to the National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in chronic GvHD first published in 2005 [32] and updated in 2014 [33], GvHD is classified into acute and chronic forms. Historically, the time point of 100 days posttransplant discriminated acute from chronic GvHD [34]. Previously, GvHD was subdivided into (1) “classic acute GvHD” characterized by a maculopapular skin rash, gastrointestinal symptoms (nausea and vomiting, diarrhea, ileus) or a cholestatic hepatitis, up to 100 days following transplantation or donor lymphocyte infusion (DLI), and (2) “persistent, recurrent, or late acute GvHD,” with similar features but happening beyond 100 days, both subtypes, by definition, occurring without evidence of chronic GvHD. Currently, clinical manifestations rather than time of onset after transplantation distinguish acute and chronic GvHD.
The incidence of acute GvHD following allogeneic HSCT depends on the indication for transplant and other factors. The incidence in patients transplanted for malignant disease approaches 40–60 % in patients receiving conventional conditioning regimens and 20–40 % with corticosteroid therapy added to other immunosuppressive agents. The incidence in patients transplanted for non-malignant diseases is lower on account of the less intense conditioning regimens, reaching 20–40 % or lower in some studies [35].
Acute GvHD
The diagnosis of acute GvHD is primarily a clinical diagnosis that is established by the Gluckenberg grading scheme and a severity index proposed by the International Bone Marrow Transplant Registry (IBMTR). It incorporates a number of signs and symptoms including the body surface area for the severity of cutaneous involvement, the level of serum bilirubin as a measure of hepatic involvement, and the daily volume of diarrhea and the presence or absence of abdominal pain and ileus, reflecting gastrointestinal (GI) disease [36, 37].
Common histopathologic constituents of GvHD in the different sites center on individual cellular apoptosis and ulceration in labile (intestine and skin) or stable (liver) tissues, variable cellular atypia and a generally minor mononuclear inflammatory infiltrate. These alterations are nonspecific and can be manifestations of radiation and chemotherapy-induced injury, drug reactions, and infection and therefore require careful clinical correlation as well as diligence in excluding an infectious etiology. The histopathologic criteria for the different organs are discussed in detail below. Interestingly, acute GvHD of the lung is less common than cutaneous, GI or hepatic GvHD [38].
Chronic GvHD
According to the NIH consensus group, chronic GvHD can occur at any time posttransplant, and includes two subtypes, (1) classic chronic GvHD, without evidence of acute GvHD, and (2) “overlap syndrome” in which features of both acute and chronic GvHD are present [32]. The latter was re-evaluated and clarified in the NIH 2014 consensus project and “overlap syndrome” is now defined as the occurrence of one or more acute manifestations of GvHD in a patient with chronic GvHD. The acute component can occur concurrently with or following the initial diagnosis of chronic GvHD [33]. The incidence of chronic GvHD varies greatly, from less than 10 % to 80 % depending on a wide range of factors [32, 39]. The principal features of chronic GvHD mimic several autoimmune and immunologic disorders, including scleroderma, Sjögren syndrome, primary biliary cirrhosis, bronchiolitis obliterans, immune cytopenias, and chronic immunodeficiency.
The clinical signs and symptoms of chronic GvHD are categorized as (1) “diagnostic” signs and symptoms, denoting manifestations that establish the diagnosis of chronic GvHD without a need for other criteria, (2) “distinctive,” denoting manifestations not usually found in acute GvHD but considered insufficient to establish an unequivocal diagnosis alone, (3) “other” features, i.e., unclassified manifestations of chronic GvHD indicating unusual, controversial, or nonspecific features of chronic GvHD that cannot be used in isolation to confirm the diagnosis, and (4) “common features,” i.e., signs and symptoms encountered in both acute and chronic GvHD [32, 33].
According to the NIH consensus project [32, 33], the diagnosis of chronic GvHD requires (1) distinction from acute GvHD, (2) evidence of at least one “diagnostic” sign of chronic GvHD or of at least one “distinctive” feature with confirmation by biopsy or other appropriate test, and (3) elimination of other disorders that mimic GvHD. Once established, a numeric grading scheme of 0–3 is applied, taking into account the patient’s performance status and severity of involvement of the principal organ systems, specifically skin, mouth, eyes, GI tract, liver, lungs, joints and fascia, and genital tract. By combining the organ-specific scores, a global assessment of GvHD severity (mild, moderate, or severe) is established. In general, systemic therapy is reserved for patients with moderate to severe chronic GvHD [32].
The histopathologic diagnosis of chronic GvHD is challenging for several reasons [40, 41]: (1) the precise histopathologic diagnosis can be confounded by the effects of the conditioning regimens, drugs, infections, and may be altered by immunosuppressive therapy initiated prior to the diagnostic biopsy; (2) uniform strict diagnostic criteria have not been established for all the organ systems; (3) the current histologic grading schemes have not been validated in prospective studies; (4) the distinction between the late forms of acute GvHD and chronic GvHD can be difficult; (5) the degree of inflammation or of epithelial damage is not an accurate predictor of response to therapy; (6) sampling issues, and timing of the biopsy as the disease progresses may also hamper interpretation. In general because the prevalence of chronic GvHD in patients with stem cell transplants is high, the positive predictive value of a biopsy showing GvHD is high, whereas the negative predictive value is low. The relatively high rate of false negatives may be explained by sampling issues or tissue adequacy or by the fact the alterations can be focal in distribution, or altered by concomitant therapy [41]. Nevertheless, despite these shortcomings, biopsies serve a useful purpose in the assessment of patients after HSCT, particularly when the findings are combined with careful clinical correlation.
The indications for biopsy in patients following HSCT as outlined by the NIH consensus guidelines [32, 41] are to confirm the diagnosis of GvHD when (1) only the distinctive clinical features of GvHD are present, (2) other diagnoses are being considered, (3) clinical findings are confined to internal organs, or in general (4) in the presence of atypical clinical features, or when infection or drug toxicity are in the differential diagnosis. The criteria for the histopathologic diagnosis of GvHD in the individual tissues and organs are outlined in the balance of this chapter.
In the 2014 NIH consensus project [41], the recommended categories for final histologic diagnosis have been simplified from the original four groups in the 2006 publication [40] to three: (1) “not GvHD,” (2) “possible GvHD,” with evidence of GvHD but with other possible causes, and (3) “likely GvHD” that combines the previous categories of “consistent with” and “unequivocal,” in which the diagnosis is either clear, or most likely, or confirmed by a subsequent biopsy or by the lack of a significant competing differential diagnosis. These histopathologic findings should always be correlated with the clinical, laboratory, and imaging data and the pathology report should incorporate this recommended terminology.
Bone Marrow Pathology in HSCT, Including GvHD
General Principles
In evaluating the bone marrow in a patient pre- or post-HSCT, the general principles applicable to the practice of hematopathology apply. Firstly there needs to be a clear knowledge of the original disease. Secondly, it is critical to perform a careful morphological examination of the blood smear, the clot and smear of the bone marrow aspirate, and the marrow core biopsy. Of note, the smear of the marrow aspirate is particularly valuable in the evaluation of residual blasts. Aside from morphology, histochemical, immunohistochemical, flow cytometric, genetic and cytogenetic testing, as well as molecular data and other laboratory parameters (e.g., serology and microbiological data) may be useful. Of paramount importance, all of these pathologic and laboratory parameters need to be correlated with the clinical features and status of the patient.
Expected Sequence of Findings Following the Transplant
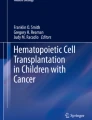
Following HSCT the bone marrow undergoes a series of temporally predictable morphologic alterations. There can be some variation on account of patient-related or disease-specific factors along with the choice of conditioning regimen and source of the stem cells [42, 43]. The conditioning regimen typically produces complete ablation of the marrow that persists into the first week following HSCT. Histologically, this is characterized by a markedly hypocellular marrow with aplasia of myeloid, erythroid and megakaryocytic series, loss of adipocytes, fibrinoid necrosis composed of acellular granular eosinophilic material, a protein-rich edema, dilated sinuses, and variable numbers of residual stromal cells such as lymphocytes, plasma cells, hemosiderin-laden macrophages and histiocytes including small lipogranulomata (Fig. 1) [44–47].

(a, b) Bone marrow showing lipogranuloma at medium and high power, a frequent finding pre- or post-stem cell transplant (Giemsa stain). (c) Prussian blue stain showing prominent iron accumulation associated with the lipogranuloma
During week 2, the marrow remains hypocellular but exhibits early regeneration of stromal adipocytes and islands of left-shifted erythroid (megaloblastic) elements. This is followed by the appearance of centrally placed myeloid colonies, i.e., non-paratrabecular in distribution (and in the setting of HSCT, not an indication of myelodysplasia). There is restoration of megakaryocytic elements usually arranged in clusters and displaying dysplastic or hypolobated nuclei. There is frequently a mild increase in reticulin fibers (Fig. 2). Of note, the centrally located early regenerating erythroid colonies are often associated with activated macrophages (so-called pseudo-Gaucher cells) that are thought to promote recovery of erythropoiesis [48]. By week 3, megakaryocytes are present and the expansion and maturation of all three lineages proceed, so that by the end of the first month, the marrow cellularity should reach 50–100 % of normal with near complete resolution of necrosis and reticulin deposition. By 2–3 months, complete regeneration with normal trilineage hematopoiesis is established (Fig. 3). Other findings that are best appreciated on smear preparations include B-cell precursors (hematogones), dysplastic changes with ring sideroblasts and pseudo Pelger-Huët change in neutrophils [45, 46, 49, 50]. Hematogones are more generally prominent in children than adults.

Findings in the first or second week following stem cell transplantation, or with graft failure. (a, b) Medium and high power showing markedly hypocellular marrow and an island of predominantly erythroid elements (PAS stain). (c) Hypocellular marrow with loose aggregate of residual lymphocytes, plasma cells, and histiocytes, and more cellular area with early hematopoietic elements (H&E stain). (d) Reticulin stain showing increased fibers in interstitium, including around the loose aggregate

Bone marrow biopsy post-stem cell transplant for myelodysplastic syndrome with recovery. (a, b) Low and high power showing rich cellularity and trilineage hematopoiesis and no residual disease (PAS stains)
Bone Marrow Complications of HSCT
There are three principal bone marrow complications of HSCT to consider [43, 45, 46]. The first complication is the persistence of a markedly hypocellular or aplastic marrow. The marrow morphology resembles that seen in the first week following transplant with a predominance of plasma cells, histiocytes, and mesenchymal cells. Persistence of a hypocellular/aplastic marrow may result from failure or delay in engraftment. A markedly fibrotic marrow pre-transplant may delay engraftment. Alternatively, this complication may be due to GvHD in the marrow as a consequence of alloreactive donor T-cells. Of note, the marrow is much less frequently involved by GvHD than the other organs as discussed below. The manifestations of GvHD in the marrow are not very specific. Apart from the reduced myeloid, erythroid, and megakaryocytic elements, their progenitor cells are characteristically decreased, as are fibroblastic progenitors and stromal cells, reflecting a derangement of the recipient’s microenvironment important in sustaining the donor cells (Fig. 4) [51]. Another feature of GvHD, particularly chronic, can be an increase in marrow T-cells [43].

Bone marrow biopsy showing graft failure 130 days post-stem cell transplant for myelodysplastic syndrome in a patient with falling blood counts. (a, H&E b, PAS) show a small aggregate of inflammatory cells and early fibrosis (asterisk) in an otherwise markedly hypocellular marrow devoid of hematopoietic elements. (c) Closer view of small inflammatory aggregate (asterisk). (d) Reticulin stain shows increased fibers in interstitium. Most of the remaining cells are CD3-positive T-cells (e) and CD138-positive plasma cells (f). The biopsy core is completely devoid of myeloid elements (MPO stain, g) and of erythroid elements, as glycophorin A here stains only mature erythrocytes (h)
Secondly, infections in the marrow after HSCT, although uncommon, should be borne in mind. Viral infections, particularly cytomegalovirus (CMV ), HHV6 and EBV have been implicated in graft failure due to suppression of stem cells. As noted previously, epithelioid granulomas can be a component of the engraftment process but their presence, especially if conspicuous should also prompt a diligent search for potential infectious agents with appropriate histochemical stains (Fig. 5). Hemophagocytosis can be a manifestation of an infectious incident, particularly viral or parasitic such as toxoplasmosis [43, 52].

Core biopsy of bone marrow pre-stem cell transplant for acute myeloid leukemia. Well-circumscribed granulomas with minimal fat can be found before or following transplantation. Infectious causes should be ruled out with special stains (negative in this case) and by correlation with clinical and microbiological data (a, Giemsa stain; b, high power, H&E)
The third complication is persistence or relapse of the primary malignancy. As detailed above, this complication is the principal cause of mortality (Figs. 6 and 7). Stringent assessment of the marrow for overt or minimal residual disease (MRD ) is therefore mandatory after HSCT. Likewise knowledge of the chimeric status of the transplant in the setting of allogeneic HSCT is essential. For example, complete chimerism (i.e., 100 % of the cells in the marrow are of donor origin) is a marker of complete remission. Mixed chimerism (with 5–90 % of cells of donor origin and the balance from the recipient) raises the possibility of relapse. The presence of a small number of malignant cells, particularly leukemic cells, indicates a failure of the conditioning regimen. Therefore it is imperative to evaluate for MRD and to differentiate it from normal hematopoiesis in the host. A detailed discussion of the topics of MRD and chimerism in HSCT is beyond the scope of this book and chapter but is provided by several excellent sources [45, 53–56].

Bone marrow biopsy showing recurrent acute myeloid leukemia in a patient with falling blood counts 90 days post-stem cell transplant. Many of the cells are blasts (a, PAS stain; b, Giemsa stain). Immunohistochemical stains for CD34 (c) and CD117 (d) confirm that 20–30 % of the cells are blasts

Bone marrow biopsy showing recurrent/residual primary myelofibrosis in a patient 3 months post-stem cell transplant. (a, PAS) medium power shows hypercellular area with fibrosis and aggregates of atypical megakaryocytes, alternating with markedly hypocellular areas (b, H&E). (c and d) Reticulin stain highlights the prominent fibrosis
Skin Pathology of GvHD Following HSCT
The skin is the most frequently involved organ in GvHD and may reveal itself as acute or as chronic GvHD, the latter 4–6 months following the transplant, although, as indicated above, the distinction between the two is somewhat arbitrary [57]. The pathogenesis of skin involvement, as with other organs, implicates the mature donor T-cells infused with the graft, and indeed GvHD is mitigated by T-cell depletion of the transplants. Donor cytotoxic T-cells have been shown to target the host endothelial cells, resulting in a substantial loss of microvessels, thereby promoting the dermal fibrosis characteristic of chronic GvHD [58].
Clinical Manifestations of Cutaneous GvHD
The clinical cutaneous manifestations of acute GvHD are succinctly incorporated by the staging scheme [57, 59]: stage 0—absence of a GvHD-related rash; stage 1—maculopapular rash involving <25 % of the surface area of the body; stage 2—maculopapular rash or erythema involving ≥25–50 % of surface area with associated symptoms such as pruritus; stage 3—generalized erythroderma, or papular, maculopapular, or vesicular eruptions with bullae or desquamation involving over 50 % of the surface area, and stage 4—generalized exfoliative, bullous, or ulcerative dermatitis. These skin manifestations should be corroborated with extracutaneous manifestations of acute GvHD such as hyperbilirubinemia and diarrhea.
The clinical features of chronic GvHD are similarly illustrated by the scoring scheme of the NIH [32, 60]. These are divided into (1) “diagnostic” (sufficient to establish the diagnosis) such as poikiloderma, lichen planus-like features, sclerotic features, morphea-like features and lichen sclerosus-like features; (2) “distinctive” features (alone are insufficient to establish the diagnosis) such as depigmentation for the skin; (3) “other” features (part of the GvHD spectrum if the diagnosis is confirmed by other means) such as impairment of sweating, ichthyosis, keratosis pilaris, hypo- or hyperpigmentation; and (4) “common” (findings of both acute and chronic GvHD) including erythema, maculopapular rash, and pruritus. In addition changes in the nails or scalp and body hair may be encountered and can aid in the diagnosis. These cutaneous findings can then be incorporated into a scoring system ranging from 0 to 3: 0 or absence of findings, 1 (mild) involvement of <19 % body surface area by the disease, without sclerotic features, 2 (moderate) involvement of 19–50 % of body surface, or involvement with superficial sclerotic features, and 3 (severe) involvement of >50 % body surface, or deep sclerotic features, or impaired mobility, ulceration or severe pruritus [60]. These site-specific scores are then incorporated into a global scoring system to assess the overall severity of GvHD. A more detailed description of the clinical features is available in a number of publications [57, 61, 62].
Pathologic Features of GvHD in the Skin
As discussed by Hymes et al. [57], the histopathologic changes in the skin biopsy serve primarily to corroborate the clinical suspicion of GvHD but do not alter its grading or staging. Moreover, the findings are nonspecific and cannot be confidently distinguished from drug reaction (including the conditioning regimen), or infectious dermatitides. The value of the skin biopsy in the diagnosis of GvHD remains controversial [27]. Kuykendall and Smoller [63] argue against the use of skin biopsy in the first 3 months following the transplant while Firoz et al. [64] advocate its use only in patients where the probability of GvHD is low.
The histopathologic findings in acute or active GvHD are centered on the dermal–epidermal junction and include (1) dyskeratotic apoptosis in the basal layer or lower malphigian (spinosum) layer of the epidermis, the outer root sheath of hair follicle or in the most superficial (intraepidermal) portion of the sweat gland duct, (2) lichenoid lymphocytic inflammation in the dermis parallel to the epidermis with or without an associated lymphocytic satellitosis (i.e., lymphocytes surrounding the apoptotic cells in the epidermis or at the dermal–epidermal junction), and (3) vacuolar change in the basal layer [40] (Figs. 8 and 9). Of all these criteria, apoptosis is the key histopathologic finding required to fulfill the “minimal criteria” of the NIH Pathology Working Group.

Skin biopsy 2 months post-stem cell transplant for chronic lymphocytic leukemia with acute and early-chronic changes of GvHD. (a) Low power showing intraepithelial dyskeratotic apoptotic cell (arrow), mild dermal lymphocytic infiltrate and papillary dermal fibrosis. (b, c) High power of dermal–epidermal junction showing several dyskeratotic apoptotic bodies, sparse lymphocytic infiltrate in dermis and lower epidermis, and mild fibrosis in dermis; also note satellitosis in (c) (arrow). High power of sweat gland (d) and hair follicle (e) with lymphocytic infiltrate and apoptotic bodies

Skin biopsy in another patient with GvHD showing dermal–epidermal junction (a) and apocrine gland (b) with sparse lymphocytic infiltrate and several apoptotic bodies
Although there are no recent specific pathologic grading schemes for reporting the severity of the cutaneous changes in acute GvHD, Shulman [27] and others [65] advocate using the older scheme of Lerner et al. [66]. According to this 1974 grading system, grade I is characterized by a superficial perivascular dermatitis with vacuolization of the epidermal basal cells; grade II is an interface dermatitis with scattered apoptotic or dyskeratotic keratinocytes in the basal or lower malphigian layers with or without closely associated lymphocytes (i.e., lymphocytic satellitosis); grade III reveals extensive apoptosis with damage to the basal layer (nuclear irregularities and atypia), formation of suprabasal bullae, and degeneration of the reticular dermis; in grade IV, the epidermis is lost, with ulceration. There are a number of published variations of this grading scheme [62, 67, 68]. These criteria can be used to estimate the severity of acute GvHD and be incorporated into the pathology consultation report. The pathologist should bear in mind that the histopathologic grade does not necessarily correlate well with the overall clinical severity of the acute GvHD, particularly early after transplantation [65, 69]. Serial biopsies may be useful to consolidate the diagnosis.
A variant of GvHD termed “eczematoid GvHD ” was described in ten patients by Creamer et al. [70]. This condition develops 2–18 months posttransplant and presents initially as dermatitis, but progresses to an erythrodermic process. Biopsies of eczematoid GvHD show the histopathologic features of GvHD enunciated above with, in addition, spongiosis, parakeratosis and a sparse perivascular dermal infiltrate. Interestingly multiple biopsies may be required before the diagnosis can be confirmed [71]. Eczematoid GvHD usually requires aggressive immunosuppressive therapy.
The histopathologic findings of chronic GvHD, although distinct from acute or active GvHD, may follow from repeated episodes of acute GvHD or even overlap or occur concurrently. These features also transform over time and are altered by therapeutic interventions. The proper assessment of chronic GvHD requires a full-thickness skin biopsy to evaluate alterations in the dermis, sweat glands, subcutaneous fat, and fascia. The findings can be classified into four principal groupings [27, 41, 72]. The earliest or lichen planus–like changes are characterized by epidermal acanthosis, orthorkeratosis, hypergranulosis with epidermal–dermal lichenoid changes (inflammation, apoptosis and vacuolization of keratinocytes, shortened rete ridges), inflammation of eccrine glands with or without a component of panniculitis. The second phase comprises the sclerotic manifestations (lichen sclerosus-like), usually but not always preceded by the lichen planus-like changes. There is progressive deposition of collagen in the deeper layers, resulting in thickening of the papillary and/or reticular dermis, with or without panniculitis. The third group, morpheic changes, manifests as localized dyspigmented lesions and is characterized by sclerosis in the lower reticular dermis or along the lower dermal–hypodermal border, with or without involvement of the epidermis and appendages. In the fasciitis pattern there is thickening of the fascial septa by inflammation and fibrosis, with or without panniculitis. Typically the epidermis is not involved.
The presence of early lichen planus-like features together with concurrent features of acute GvHD are most likely to progress to the more advanced forms of chronic GvHD than those with chronic changes alone [73].
Pathologic Differential Diagnosis of GvHD
The poor specificity of the cutaneous alterations in acute GvHD makes it difficult to distinguish from other causes of posttransplant rashes such as viral infections, drug reactions, and conditioning regimens and from the engraftment syndrome associated with lymphocyte recovery [74]. For this reason we, like others, are reluctant to make a diagnosis of acute GvHD a priori in the early posttransplant period [63]. Sviland et al. [75] emphasize the lack of specificity of skin biopsy findings in diagnosing GvHD and indicate that rectal biopsy may be more specific.
The principal difficulty is distinguishing acute GvHD from a drug reaction because these patients typically receive multiple medications. As emphasized by Shulman et al. [27], rendering a diagnosis of acute GvHD requires a careful search for apoptotic keratinocytes in the basal layer of the epidermis including at the tips of the rete ridges and the corresponding areas of the hair follicles, as well as a relatively sparse inflammatory infiltrate at the dermal–epidermal junction (Fig. 10). In contrast drug reactions are characterized by an eczema-like pattern with spongiosis, few if any apoptotic cells, and more numerous lymphocytes. However, on occasion, a severe drug reaction resulting in a Steven-Johnson syndrome with formation of bullae or denudation may render the differentiation from GvHD difficult or impossible. Although eosinophils are typically touted as hallmarks of a drug reaction, they may be present also in GvHD [76]. Of interest, however, Weaver and Bergfeld [77] found that they could rule out a diagnosis of acute GvHD when they found more than 16 eosinophils per 10 high-power fields.

Skin biopsy in patient post-stem cell transplant in which a diagnosis of GvHD was favored over a drug reaction. (a) Note spongiosis and mild lymphocytic infiltrate. (b, c) High power showing spongiosis, infiltration of epidermis by lymphocytes but absence of eosinophils. Very few apoptotic bodies are seen
Radiation and chemotherapy effects can be difficult to differentiate from acute GvHD. The pathologist should exercise caution in interpreting biopsies in patients who have received these as part of their preconditioning regimens a short time prior to the biopsy [78, 79]. A related entity is the skin eruption of “ lymphocyte recovery ” that develops 14–21 days following the administration of cytoreductive therapy and coinciding with the normalization of lymphocyte counts. It occurs in the absence of HSCT and produces a maculopapular rash. The histologic findings of lymphocyte recovery in the skin resemble mild GvHD, with mild epidermal changes consisting of variable intercellular edema, exocytosis of lymphocytes, and rare dyskeratotic keratinocytes that can mimic the effects of cyclosporine [67, 80]. Mechanistically the effects of cyclosporine, the cutaneous eruption of lymphocyte recovery, and GvHD in the setting of autologous HSCT are likely related to this same phenomenon [81].
Infections, particularly viral infections (Herpes simplex and zoster) can elicit skin rashes. In the setting of HSCT they are more common in other sites like the gastrointestinal tract, liver, and lung than the skin. Infectious cutaneous lesions after transplant are recognized by their characteristic histopathologic findings and should be correlated with clinical, serological, PCR, and microbiological studies [27, 71]. Other examples of infectious complication due to human herpes virus 6 and toxoplasmosis have been reported [82, 83].
In summary, the role of the skin biopsy in the diagnosis of GvHD remains controversial, largely on account of the lack of specificity of findings. However, a number of points deserve emphasis. Firstly, a biopsy in the first 3 weeks following transplant should be avoided except for clinical indications like herpetic infection. Secondly, the presence of numerous epidermal apoptotic bodies and of lymphocyte satellitosis, particularly in skin appendages, raises the distinct possibility of GvHD. Thirdly, serial skin biopsies may be required to confirm the diagnosis. Fourthly, the diagnosis of GvHD by cutaneous biopsy may be enhanced by the presence of extracutaneous findings such as hyperbilirubinemia and diarrhea [84]. Finally, initiation of therapy for GvHD should not be delayed pending the results of a biopsy or if the histopathologic findings are not diagnostic [85].
Pulmonary Complications of HSCT, Including GvHD
Since the introduction of HSCT in the early 1970s, pulmonary complications have been registered [86] and remain a significant cause of morbidity and mortality. A study in the early 1980s [87] found that 41 % of 525 patients receiving allogeneic stem cell transplants developed nonbacterial pneumonias. The majority were CMV-related (85 cases, untreatable at the time) or idiopathic (64 cases) and the mortality rates ranged up to 91 % in CMV pneumonitis. The histopathologic findings in idiopathic pneumonia consisted of an interstitial mononuclear infiltrate without identifiable organisms by histological or microbiological analyses.
Currently, lung injury occurs in 25–50 % of patients with HSCT. It is highest in allogeneic HSCT, and carries a mortality rate of about 50 %. Non-infectious pulmonary complications of HSCT have now supplanted infections due in part to antimicrobial prophylaxis and more effective therapeutic agents [88]. Of the non-infectious lesions, idiopathic pneumonia syndrome (IPS ) is a particularly devastating and complex complication. Clinically, the vast majority of patients with non-infectious pulmonary complications present with variable respiratory symptoms and signs (fever, cough, dyspnea, hypoxemia), and localized or diffuse infiltrates on pulmonary imaging.
A number of issues related to the pulmonary complications of HSCT should be highlighted. The current nomenclature is confusing, with overlapping entities, poorly defined syndromes of imprecise or multifactorial etiology and/or pathogenesis, and lack of clear definitions, all of which render the interpretation of the literature and the precise assignment of a specific pathological diagnosis challenging. Secondly, there is a paucity of literature describing the pathological findings, particularly the acute ones. The pathological findings are nonspecific and reflect patterns of injury rather than explicit or etiologic entities. Examples include diffuse alveolar damage (DAD), interstitial or organizing pneumonias and airway inflammation, and airway fibrosis amongst others. Although many of the complications may be related to the HSCT per se, lung injury can be compounded by other factors such as the conditioning regimen, infection, aspiration injury, and drug-related toxicity. Finally, the diagnosis of pulmonary GvHD is one of exclusion and an infectious process should always be considered in the differential diagnosis of clinical dysfunction.
Infectious Complications
Despite the diminished incidence of infectious pulmonary complications after HSCT, these remain at the forefront when a patient presents with respiratory symptoms and/or an infiltrate on imaging studies. The spectrum of radiologic changes includes localized consolidation(s) or multifocal or diffuse alveolar and/or interstitial infiltrates. The lung is at risk for both nosocomial and community-acquired infections on account of the perpetual contact with the external environment. Moreover, as the patients are immunocompromised, the normal morphologic patterns of response to infection may be altered, diminished, or even nonspecific. The lung is also at risk for multiple concurrent injuries such as infection, GvHD, and/or drug reaction and the constellation of morphologic findings might consist of variable acute and chronic inflammation, DAD, alveolar hemorrhage, or interstitial inflammatory infiltrates with possible superimposed granulation tissue and fibrosis. Finally, it should be noted that the pathologist faces additional challenges due to the limited tissue samples that are submitted e.g., from bronchoalveolar lavage (BAL ), endoscopic or CT-guided biopsies, transbronchial biopsies (TBBx) or video-assisted thoracoscopic (VATS) biopsies. The liberal use of levelled sections, histochemical, immunohistochemical and molecular testing in these clinical situations is imperative along with awareness of the radiologic findings and communication with the treating clinicians.
Of the different investigative methods available, the simplest and least invasive is BAL, or thoracocentesis in the presence of a pleural effusion. Cytospin- or liquid-based cytologic preparations can be used to evaluate for infectious organisms or malignancy [89]. The fiberoptic TBBx yields sufficient tissue samples to evaluate for patterns of injury and infectious agents. The VATS biopsy is generally reserved for patients who have failed conventional therapies or are suspected of having more than one etiology to account for the radiologic alterations. Regardless of the specimen obtained, a thorough search for infectious agents such as fungal infections including Pneumocystis jiroveci (PJP), Candida and Aspergillus species, and viruses such as CMV, Herpes simplex and Varicella zoster, as well as more uncommon organisms such as Toxoplasma gondii should be performed [90]. Gram-positive and gram-negative bacterial infections remain the most common causes of infection and tissue or fluid Gram stains, microbiologic cultures and molecular sequencing are helpful. Mycobacterial infections are much rarer and usually represent reactivation episodes rather than de novo infections. We routinely perform silver-based stains such as the Gomori-methanamine silver (GMS ) stain on BAL samples and tissue sections to exclude PJP or other fungal organisms. Immunohistochemical staining for viruses and Toxoplasm gondii. may be performed routinely or as indicated [91]. These findings should be correlated with data from the microbiology laboratory (including immunofluorescence staining for viruses, polymerase chain reaction for viruses, fungi, and organisms such as Chlamydia and Mycoplasma), imaging studies and from the clinical context.
Non-Infectious Complications , Including “Idiopathic Pneumonia Syndrome ”
There are a variety of non-infectious complications that can develop after HSCT and these are summarized in Table 1. A useful clinical and radiologic algorithm for evaluating pulmonary complications after HSCT was formulated by Haddad [92].
Delayed Pulmonary Toxicity Syndrome
Delayed pulmonary toxicity syndrome (DPTS ) has been linked closely to the conditioning regimen for HSCT rather than the transplant per se. Whether it is a component of idiopathic pulmonary syndrome (IPS) or a distinct entity is controversial but the 2010 ATS guidelines exclude DPTS from the strictly defined IPS [91, 93]. It occurs in up to two-thirds of patients receiving high-dose chemotherapy prior to autologous HSCT, typically at a median time interval of 45 days posttransplant. Fortunately most patients respond well to corticosteroids.
The pathologic findings, are similar to the toxic effects of high-dose chemotherapy in immunocompetent patients, and comprise an acute alveolar injury pattern with nonspecific interstitial pneumonitis with vascular injury, alveolar edema, alveolocapillary septal thickening with fibrosis, proliferating atypical type-II pneumocytes and increased alveolar macrophages, i.e., similar to a mild form of DAD [94].
Peri-Engraftment Respiratory Distress Syndrome
Peri-engraftment respiratory distress syndrome (PERDS ) is defined as pulmonary dysfunction occurring within 5 days of the neutrophil count returning to normal after HSCT. It accounts for one-third of cases of “idiopathic pneumonia syndrome” after allogeneic HSCT. PERDS is currently included in the spectrum of IPIS according to the 2010 ATS guidelines but its pathogenesis is distinct from the alloimmune response and from GvHD. PERDS occurs after both autologous and allogeneic HSCT [95, 96]. The pulmonary injury is mediated primarily by the newly engrafted neutrophils intensifying the insult of the conditioning regimen. Like DPTS, PERDS responds well to corticosteroids, and has a better prognosis than IPS. The pathological findings of PERDS are nonspecific manifesting predominantly as DAD or diffuse alveolar hemorrhage (DAH ) [91, 97]. Clinicopathological correlation is required to establish this diagnosis.
Idiopathic Pneumonia Syndrome
The term “idiopathic pneumonia syndrome” (IPS) was coined at the 1991 NHLBI workshop [98] and is defined thus: “diffuse lung injury occurring after marrow transplant for which an infectious etiology is not identified.” In 2010, the American Thoracic Society (ATS ) refined IPS as an “idiopathic syndrome of pneumopathy after HSCT, with evidence of widespread alveolar injury and in which infectious etiologies, cardiac dysfunction, acute renal failure, or iatrogenic fluid overload have been excluded” [91]. The manifestations and outcome differ significantly between allogeneic and autologous transplants. In allogeneic recipients the median onset is about 19 days. The incidence in this group has fallen from about 12 % to 2–3 % largely because of less aggressive conditioning regimens but mortality rates remain as high as 60–80 % overall and reach over 95 % in patients needing mechanical ventilation. The incidence of IPS is lower in autologous HSCT patients and the median time of onset is 63 days. These patients generally respond well to corticosteroids with a better prognosis than the allogeneic group.
A variety of risk factors for IPS have been identified [91]. The principal etiopathogenetic mechanisms implicated revolve in part around the toxic conditioning regimens (total body irradiation (TBI) and high-dose chemotherapy), but primarily around immune mechanisms involving donor T-cells and cytokines. TNFα targets endothelial cells causing increased vascular permeability and also damages epithelial cells producing cellular apoptosis and inducing proliferation of type-II pneumocytes. Indeed the proposed therapy of IPS currently under evaluation in clinical trials advocates blocking TNFα signalling with etanercept [91, 99]. Therefore, in the absence of infection, IPS is best regarded primarily as the pulmonary manifestation of acute GvHD.
The pathologic findings in the clinical spectrum of IPS are likewise varied and nonspecific. Firstly, a small number (5–10 %) develop DAH as an early manifestation and clinical complication (1–4 weeks). The diagnosis of DAH is made by progressively increasing bloody return or the presence of >20 % hemosiderin-laden macrophages on BAL [100, 101]. Open or transbronchial lung biopsies are seldom performed. Autopsy examination reveals hemorrhage in at least 30 % of alveoli, with the absence of infection-related changes (Fig. 11) [102]. Other findings include a vasculopathy of small muscular arteries with medial hyperplasia and intimal thickening, myxoid mural change, and thrombotic microangiopathy [103]. Of note, the distinction between IPS and DAH may be difficult and in actuality they probably overlap, both clinically and pathologically. The mortality rate in DAH is high despite corticosteroid therapy [104].

Lung sections from patient who died from pulmonary hemorrhage and diffuse alveolar damage (DAD ) following stem cell transplant for N/K T-cell lymphoma. (a) Extensive alveolar hemorrhage and (b) mixed hemorrhage with hyaline membranes characteristic of DAD
A second pattern reported in IPS is DAD with its clinical correlate, the acute respiratory distress syndrome (ARDS ). The lungs are heavy, consolidated, and edematous with or without hemorrhagic areas. Microscopically, they display alveolar epithelial damage, a protein-rich alveolar fluid with airspace hyaline membranes in the exudative phase (Fig. 12a, b). In the organizational stages, interstitial and alveolar granulation tissue plugs and variable proliferative interstitial fibrosis ensue (Fig. 12c, d). The pattern of DAD also characterizes acute interstitial pneumonia (AIP); parenthetically, the 2010 ATS guidelines include AIP in the clinical spectrum of IPS. However the clear association of the IPS with HSCT suggests that the idiopathic AIP should be excluded from IPS [105].

Patient with respiratory failure following stem cell transplant for acute leukemia. (a) Chest CT scan showing large multifocal areas of edema and consolidation. (b) Section from open lung biopsy with prominent hyaline membranes lining alveoli, consistent with the DAD pattern of idiopathic pneumonia syndrome. Other areas showing evidence of organization with granulation tissue plugs (Masson bodies) (c), and ongoing interstitial fibrosis (d)
A third pattern of injury in IPS is lymphocytic bronchitis/bronchiolitis and interstitial pneumonitis, and rarely lymphoid interstitial pneumonia (LIP) [106]. Xu et al. [107] describe a similar pattern under the term of “chronic interstitial pneumonia.” Light microscopy shows a perivascular and interstitial mononuclear inflammatory infiltrate composed of lymphocytes and plasma cells with direct infiltration and apoptosis of the bronchial and bronchiolar epithelium; the latter may display hyperplastic, dysplastic or squamous metaplastic changes. In addition a lymphocytic perivasculitis, particularly a perivenulitis, may also be present. These alterations closely resemble those described in cutaneous and gastrointestinal GvHD, are rather specific and can assist in distinguishing pulmonary GvHD from pulmonary infections [107]. This form of pulmonary GvHD can progress to bronchiolitis obliterans (BO) described below.
Cryptogenic Organizing Pneumonia or Bronchiolitis Obliterans Organizing Pneumonia (BOOP)
Cryptogenic organizing pneumonia (COP ), unlike bronchiolitis obliterans discussed below, is associated with both acute and chronic GvHD in the setting of HSCT. COP should be distinguished from BO on account of its different clinicopathologic presentation (dry cough, fever, mild restrictive pattern on lung function testing, and variable infiltrates on imaging), response to corticosteroids and a more favorable outcome [108]. The pathological findings resemble those in the non-transplant setting, consisting of distinctive fibromyxoid plugs within in the lumens of the small airways and extending into alveolar ducts and sacs. These are associated with a chronic interstitial inflammatory infiltrate [40, 91, 105]. In the context of HSCT, however, there may also be changes more specific to GvHD such as increased mononuclear cells, infiltration of lymphocytes in the small airway epithelium that may display apoptosis and atypia, and a vasculitis (Fig. 13) [107].

Patient with pulmonary dysfunction due to GvHD following stem cell transplant. (a) Chest CT scan showing increased interstitial markings, thickened airway walls, and tree-in-bud pattern (arrow) characteristic of the cryptogenic organizing pneumonia pattern. (b, c) Low and high power of transbronchial biopsy from same patient with GvHD exhibiting prominent infiltration by lymphocytes with damage and sloughing of the epithelium. (d) Other area showing organizing pneumonia pattern of GvHD with granulation tissue bud surrounded by chronic inflammation and (e) lymphocytic arteritis
Bronchiolitis Obliterans
Bronchiolitis obliterans (BO ), also named bronchiolitis obliterans syndrome (BOS) or obliterative bronchiolitis (OB) is the hallmark of pulmonary chronic GvHD, and is included (loosely) in the spectrum of IPS according to the 2010 ATS definition. According to the 2014 NIH Consensus guidelines BO diagnosed by lung biopsy is classified as a “diagnostic” feature of chronic GvHD provided distinctive clinical signs or symptoms are also present in another organ. Alternatively, the diagnosis of BOS can be rendered by the presence of an obstructive pattern on pulmonary function tests (PFTs) [109]. Indeed, screening PFTs are now recommended at day 100 after transplantation or at other appropriate intervals as warranted [33]. The incidence of BO ranges from 2 to 30 %, although recent data suggests it now approaches the lower end of this spectrum (2.8 % of 2087 patients at 5 years after transplant in the study by Nakaseko et al. [110]). The onset varies from a few months to more than 10 years after HSCT, but generally most patients present 7–15 months after HSCT [91]. Symptoms include dyspnea, cough, wheezing and an obstructive pattern is found on PFTs.
The pathologic findings in BO resemble closely those of BO in chronic lung allograft rejection in lung transplant recipients (see chapter “Lung Transplantation”). The lesions consist of dense eccentric or concentric subepithelial collagenous fibrosis causing partial or complete obliteration of small airways, with variable numbers of lymphocytes and foam cells and associated with flattening, hyperplasia or squamous metaplasia of the epithelium [27, 40, 106, 111].
Pulmonary Alveolar Proteinosis
This rare pulmonary disorder is characterized by the diffuse accumulations of surfactant proteins and lipids within the alveolar spaces. It is caused by defective surfactant clearance by alveolar macrophages resulting in bilateral alveolar infiltrates on chest radiographs. It is considered in the clinical differential diagnosis of IPS but is not generally included under this umbrella term. Pulmonary alveolar proteinosis (PAP) is classified into three subtypes: (1) genetic or congenital forms due to mutations in surfactant proteins or granulocyte-macrophage-colony-stimulating factor (GM-CSF) receptor genes; (2) autoimmune (formerly called primary or idiopathic PAP) (~90 % of cases), wherein anti-GM-CSF antibodies block the activation of alveolar macrophages and (3) secondary forms of PAP most frequently due to toxic exposures, chronic infections (e.g., PJP and other fungi, Nocardia, mycobacteria, CMV, and other viruses), immune deficiencies or hematological disorders [112, 113]. The latter category includes a small number of cases of PAP that have been reported following HSCT in which the putative pathogenesis may involve a combination of the depletion and dysfunction of macrophages related to the profound cytopenia and/or to anti-GM-CSF antibodies generated as part of the immune disparity between donor and recipient [114–116].
The diagnosis of PAP generally relies on examination of BAL fluid, of a transbronchial biopsy or of a VATS biopsy. The BAL fluid is frequently milky brown and microscopically reveals a paucicellular, amorphous or finely granular PAS-positive material, cell debris, and scattered macrophages (Fig. 14). There is minimal if any cellular inflammatory infiltrate and histochemical stains, in particular for PJP, should be negative. In tissue sections, the airspaces are filled and expanded by the granular eosinophilic material with a minimal interstitial inflammatory component.

(a) CT scan showing multiple patchy infiltrates. At autopsy, pulmonary alveolar proteinosis (PAP) was found. (b, c) Low and high power showing diffuse filling of alveoli by amorphous paucicellular eosinophilic material. (d, e) Low and high power of similar fields showing strong PAS-positivity of the proteinaceous material. No infectious organisms were found
Pulmonary Hypertension
Pulmonary hypertension is a rare complication of HSCT and can be classified into pulmonary arterial hypertension and pulmonary veno-occlusive disease (to distinguish it from hepatic veno-occlusive disease/sinusoidal obstruction syndrome (SOS ) discussed below). Both entities share predominant endothelial dysfunction and damage as part of their pathogenesis.
Pulmonary arterial hypertension (PAH ) is even rarer than pulmonary veno-occlusive disease. Although PAH may be attributable in part to the conditioning regimen, there are recognized cases that are associated with GvHD [117, 118]. Patients present with mild respiratory symptoms and have evidence of elevated pulmonary arterial pressures. Lung biopsies show hyperplastic intimal thickening, although plexiform lesions have not been described (Fig. 15).

Lung biopsy showing alterations of pulmonary hypertension following HSCT. Large (a) and small artery (b) showing prominent medial and intimal thickening. (c, d) Other area showing low and high power of large vein in interlobular septum with prominent medial thickening. (e) There is also evidence of pulmonary veno-occlusive disease with organized thrombus in medium vein
Pulmonary veno-occlusive disease (PVOD ), unlike its hepatic analog, is a very rare complication of HSCT, and is defined as postcapillary pulmonary venular and venous obstruction leading to pulmonary vascular congestion, pulmonary hypertension, and right ventricular heart failure. Although PVOD was first described in 1934 by Hora et al. [119], its occurrence in HSCT was first reported only in 1984 by Troussard [120]. PVOD shares pathogenetic mechanisms with PAH, specifically the role of chemotherapy and radiation used in conditioning, and the immune-mediated damage. To date, most published cases of PVOD develop in allogeneic rather than autologous HSCT. The pathologic findings in PVOD, often discovered only at autopsy, include irregular and often eccentric intimal fibrosis with formation of luminal septa, recanalization, and with variable obstruction of pulmonary venules and small veins, less frequently of larger veins (Fig. 15c, d, e). Secondary congestion of capillaries, arterial intimal fibrosis, and medial hypertrophy may ensue, manifesting clinically as pulmonary edema and pulmonary hypertension. Plexiform lesions are typically absent, but interstitial fibrosis and hemosiderin-laden macrophages within airspaces may be seen.
Pulmonary Cytolytic Thrombi
This rare complication (4 % of 324 pediatric patients in the series of Smith et al. [121]) occurs following allogeneic HSCT. Most patients are under 18 years of age and present with fever, cough, and chest pain, and display multiple peripheral nodular lesions rather than infiltrates on imaging studies. Their pathogenetic association with acute GvHD is supported by the non-occurrence in autologous HSCT and by an association with GvHD in other organs. Pulmonary cytolytic thrombi (PCT) is associated with a greater incidence of GvHD and a lower rate of relapse of leukemia. In general, patients respond to corticosteroids and the prognosis is very good [121, 122]. Open lung biopsy is required to establish the diagnosis and to rule out an Aspergillus infection: VATS biopsy typically shows a nodular lesion composed of areas of hemorrhagic infarction associated with occlusion of small and medium-sized arteries and veins by deeply basophilic amorphous granular or fibrillar thrombus material [123, 124]. The cells within the thrombi are monocytes, primarily of donor origin [125].
Posttransplant Lymphoproliferative Disorder (PTLD)
This topic is covered in chapter “Transplantation and Malignancy”.
Renal Pathology in HSCT
Although the kidney is not generally recognized as a primary target in HSCT, chronic renal disorders develop in 20–60 % of patients following HSCT. The etiopathogenesis is likely multifactorial and includes the conditioning process, episodes of GvHD, acute renal injury, infections, and drug reactions. Renal biopsies often exhibit several simultaneous pathological findings [126, 127]. The principal indications for renal biopsy are nephrotic-range proteinuria and/or persistently elevated creatinine levels. Glomerulopathies constitute the majority of renal dysfunction following HSCT. In descending order of frequency these consist of membranous glomerulonephritis, minimal-change disease, membranoproliferative glomerulonephritis, and focal segmental glomerulosclerosis. Although it has been suggested that membranous glomerulonephritis is a glomerular expression of GvHD [128], its occurrence in autologous HSCT as well as in allogeneic HSCT appears to cast some doubt on that notion. Nonetheless transplant-related immune dysfunction probably still plays a role in the pathogenesis of renal dysfunction and implicates in particular B-cells [127].
Another common complication is thrombotic microangiopathy (TMA ), manifested clinically as hemolytic-uremic syndrome. It is a consequence of endothelial injury by factors like radiation, chemotherapy, ischemia, and sepsis amongst others. An autopsy study found TMA in over 50 % of the 26 HSCT patients [129]. A diagnosis of TMA conveys a poor prognosis. Other less specific renal findings following HSCT include acute renal injury (acute tubular necrosis), polyoma virus nephropathy, interstitial nephritis, calcineurin inhibitor toxicity and recurrent disease, particularly of amyloid and myeloma-related changes [126, 127].
Gastrointestinal Complications of HSCT
Transplant Conditioning
Cytoreductive and myeloablative therapies including radiation and chemotherapy used in conditioning regimens can cause GI tract injury. Symptoms including nausea and vomiting emerge within 15 days of transplantation and can persist for up to 3 weeks [130–132]. It is now thought that this initial mucosal injury contributes to the development and enhancement of acute GvHD.
Acute GvHD
The gastrointestinal (GI) tract is the second most common site of involvement by GvHD, often concurrently with skin and liver involvement [133, 134]. However, the incidence of isolated GI GvHD is increasing [135]. Although enhanced pre-transplant therapy is linked to more severe GvHD, there is no difference in the severity or incidence of GvHD following peripheral blood vs. BMT [132].
Pathogenesis
It is believed that conditioning therapies upregulate the release of cytokines such as tumor necrosis factor-α and interleukins IL1 and IL7 that in turn increase antigen presentation from host to donor T-cells through HLAs [35, 136]. Additionally, GI mucosal damage further exacerbates the inflammatory process by releasing endotoxins that amplify and propagate the “cytokine storm” [137]. Epithelial stem cells, residing in intestinal and gastric crypts are preferentially targeted by donor cytotoxic lymphocytes. Eosinophils and granulocytes are also recruited in GvHD [138].
Clinical and Endoscopic Presentation
Acute GI GvHD usually manifests within the first few days to as many as 100 days after HSCT [139]. As previously noted there can be an overlap between late onset acute and chronic GvHD [140]. Overlap syndromes have been linked to reduced intensity conditioning regimens [141]. Clinically it is important to establish a diagnosis of acute GI GvHD as it guides therapy and is associated with a poorer prognosis, particularly the higher grades of GI GvHD [141]. In addition to the assessment of GI-related signs and symptoms such as diarrhea, abdominal pain and ileus, dysfunction and alterations in other organ systems should be considered [142]. The clinical features of acute GI GvHD are outlined in Table 2.
The decision for upper or lower endoscopic evaluation is guided in part by the type and localization of symptoms. Although newer imaging techniques have been explored for the assessment of GvHD, endoscopy with biopsy remains critical in the correlation with clinical symptoms [143]. The classic endoscopic findings include mucosal edema, sloughing, erythema, erosion, and ulceration [144–148]. Studies have shown that the degree of injury viewed on endoscopy, however, does not always correlate with histopathologic severity [149].
Histopathologic Findings
It should be emphasized that the diagnosis of GI GvHD requires close clinicopathologic correlation because the histologic features are nonspecific. Acute GI GvHD occurs throughout the GI tract, but is least common in the esophagus [150]. The classic finding in acute GvHD is the apoptotic body within the epithelium. Apoptotic bodies can manifest as hyperchromatic karyorrhectic nuclear debris within a large clear halo (so-called “exploding crypts”) or as a shrunken cell with a condensed (pyknotic) nucleus and eosinophilic cytoplasm [41] (Figs. 16 and 17). In the esophagus, apoptotic bodies are in the form of densely eosinophilic dyskeratotic keratinocytes; there may also be a lichenoid interface inflammatory infiltrate, sloughing, and other nonspecific changes in the squamous mucosa (see Table 3). Elsewhere in the GI tract, the apoptotic bodies are within glandular or crypt epithelium, forming intracytoplasmic vacuoles filled with karyorrhectic nuclear debris. In gastric body biopsies, these apoptotic bodies are usually found at the neck of glands where they interface with the gastric pit. In antral biopsies, apoptotic bodies are most often seen in the deep glands [151]. Focally enhanced gastritis, defined as a mixed lymphohistiocytic infiltrate, in some cases with neutrophils, surrounding a small group of foveolae or glands without apoptosis is associated with but not diagnostic of GvHD [152]. In the small intestine, colon, and rectum, the deep crypt cells show apoptosis. When these apoptotic bodies are particularly prominent, the term “exploding crypts” has been used [153]. Other findings in more severe cases include dilated crypts, luminal debris, crypt abscesses, crypt destruction, mucin depletion, regenerative surface epithelium, loss of Paneth cells, Paneth cell metaplasia, a periglandular mononuclear cell infiltrate, and ulceration/denudation. Neuroendocrine cells are generally spared damage and form small clusters at the base of the mucosa [41] (Figs. 18 and 19). The salient findings are summarized in Table 3.

Acute GvHD. Medium and high power of cecal biopsy showing (a) active colitis with denuded surface epithelium, glandular dropout, and (b) crypt apoptotic bodies (arrows)

Acute GvHD. Colonic biopsy showing intraepithelial lymphocytes, chronic active inflammatory infiltrate in lamina propria, and crypt apoptotic bodies (arrow)

GvHD in colonic biopsy . (a) High power showing large apoptotic body (arrow) and minimal inflammation in lamina propria, (b) apoptotic bodies in intestinal crypts, (c) withered glands and (d) attenuated surface epithelium with glandular disarray

Severe GvHD. High power of jejunal biopsy showing surface of an ulcer with complete loss of villi and a neutrophilic exudate
There is controversy around the definition of the minimal histological changes sufficient to establish the diagnosis of acute GvHD. Currently, the consensus favors a minimum of >1–2 apoptotic bodies per biopsy piece as the minimum diagnostic criterion because it increases sensitivity albeit with some loss of specificity [41, 154] (Fig. 18). Unfortunately, due to the patchiness of injury along the GI tract, the rate of false negative error in diagnosis remains a concern. It has been suggested that at least eight and up to 20 serial sections should be reviewed to minimize the risk of missing infrequent apoptotic bodies [41]. Multiple biopsies along the GI tract may also improve the diagnostic yield. Currently, several histologic grading systems have been proposed. These schema, such as the Lerner [66] and the Sale modification [27] serve as useful descriptors but do not necessarily reflect clinical severity; all four grades may be associated with severe symptoms and extensive endoscopic involvement.
Ancillary Tests
Although there has been recent interest in the use of caspase-3 as an apoptotic marker [155], it is not used in routine clinical practice. Immunohistochemistry for CMV as well as histochemical stains for Helicobacter may be useful for excluding infectious causes.
Differential Diagnosis
Given the wide range and lack of specificity of the histologic findings in acute GvHD, there is a considerable differential diagnosis. Conditioning regimens damage the mucosa but typically resolve within 20 days after transplantation. Drugs, including NSAIDs [156], mycophenolate mofetil (MMF), ticlopidine [157], proton-pump inhibitors [158], 5-fluorouracil, cyclosporine A, and phosphate bowel preparations [159] can initiate apoptosis and GvHD-like changes. In particular, MMF-related toxicity causes ulcerative esophagitis, reactive gastropathy, and colonic architectural disarray; in the bowel it leads to increased apoptosis, crypt dilatation with accumulation of luminal debris [160]. However, unlike acute GvHD where neuroendocrine cells are spared, MMF therapy leads to loss of neuroendocrine cell nests [41]. Reflux esophagitis may also need to be excluded. Inflammatory bowel disease and celiac disease should be considered in the setting of chronic architectural disarray and in the appropriate clinical context [161, 162].
Infectious causes of GI symptoms must also be ruled out. The histologic changes should be corroborated by serologic testing, cultures, and immunohistochemical stains. CMV colitis mimics GvHD; more importantly both can coexist [151, 163]. Cryptosporidium has also been associated with increased epithelial apoptosis [164]. Other infectious agents to consider include adenovirus, Clostridium difficile, campylobacter, H. pylori as well as HSV, HIV, candida, rotavirus, and norovirus [165–168].
Chronic GvHD
As discussed previously, there can be significant overlap between acute and chronic GvHD. Symptoms typically manifest between 3 months and 2 years, although two-thirds of patients present within the first 12 months following transplant [169]. There is no time limit on the presentation of chronic GvHD.
Pathogenesis
Chronic GI GvHD is thought to represent an end-stage alloimmune and autoimmune disorder initiated by donor T-cells. The pathogenesis involves insults to both the recipients’ histocompatibility antigens and antigens common to both donor and recipient.
Clinical and Endoscopic Presentation
Unlike acute GvHD, chronic GI GvHD not uncommonly involves the esophagus [150]. The key features of chronic GvHD are esophageal webs, strictures or concentric rings seen on endoscopy or barium contrast studies. According to the latest NIH consensus document, identification of esophageal webs is the only universally accepted criterion to diagnose chronic GI GvHD [41]. Clinically, there is considerable overlap in the symptoms of both acute and chronic GvHD such as nausea, vomiting, weight loss, and diarrhea. Wasting syndrome may also be seen in chronic GvHD although it is likely a multifactorial process [33]. Chronic GvHD may also be associated with pancreatic atrophy and exocrine insufficiency [170].
Histopathologic Findings
Like the clinical presentation of chronic GvHD, there is morphologic overlap with acute GvHD. As with the clinical presentation, the histologic findings of chronic GI GvHD resemble those of acute GvHD affecting the gastrointestinal tract; their distinction cannot be made on histology alone. In addition, chronic GvHD may show changes of long-standing injury including marked architectural disarray, crypt loss, cystic glands, and areas of atrophy admixed with signs of regeneration. Chronic GvHD may show fewer apoptotic bodies and a more pronounced lymphoplasmacytic infiltrate than acute GvHD. Paneth cell metaplasia as well as fibrosis of the lamina propria have also been described. It is important to bear in mind that none of these findings are specific for chronic GvHD; as with acute GvHD clinicopathologic correlation is mandatory [41].
Hepatic Complications of HSCT
Graft-Versus-Host Disease
Introduction
As indicated above, GvHD was historically classified as acute or chronic by using an arbitrary cutoff of 100 days; however, it is now recognized that overlap exists and the distinction between hepatic acute and chronic GvHD is made on clinical grounds [32, 171]. Studies show that liver involvement is present in 30 % and 35–50 % of patients with acute and chronic onset of symptoms, respectively [32, 40, 171], but it can occur in as many as 85 % of patients following BMT [172, 173].
Regardless of chronicity, hepatic GvHD is a process driven by immune-mediated destruction of the small bile ducts and ductules. The role of the pathologist is twofold: firstly, to distinguish GvHD from other causes of liver dysfunction such as drug toxicity and infection, especially in cases where there are atypical or confounding clinical features [174], and secondly, to identify the minimal criteria for active GvHD [40]. Owing to the patchy and irregular distribution of bile ductal involvement, liver biopsies for GvHD have a sensitivity of 66 % and specificity of 91 % [172]. Thus, in cases with normal histologic findings, clinicians may elect to treat patients for hepatic GvHD on the basis of clinical findings alone. Other confounding factors in the diagnosis of hepatic GvHD are listed in Table 4. There is little evidence to support the use of a liver biopsy as a screening tool or to assess response to therapy for GvHD [40]. However, the extent of bile duct damage and inflammation does correlate with liver function tests, and in some cases with outcomes and survival [41].
Clinical Presentation and Risk Factors
Risk factors for the development of hepatic GvHD include older recipient age, female donor cells into a male recipient, use of peripheral blood stem cells and previous episodes of GvHD [175]. Patients can present without symptoms or signs, with painless hepatomegaly alone or with multiorgan involvement. Laboratory tests show an increase in serum bilirubin (both direct and indirect), in alkaline phosphatase and the transaminases. Clinical and laboratory parameters utilized for the diagnosis of hepatic GvHD are in Table 5.
Acute and Chronic Hepatic GvHD
Unfortunately, there is no consensus currently for the minimal histological criteria for the diagnosis of hepatic GvHD [41]. Classically, acute hepatic GvHD manifests as a cholestatic hepatitis with jaundice and elevated bilirubin and alkaline phosphatase levels. Concurrent GI or skin manifestations are usually present: indeed patients rarely present with isolated hepatic involvement [176]. Clinically, liver dysfunction in acute hepatic GvHD typically develops within 25–100 days following transplant.
The pathologic findings in acute hepatic GvHD are dominated by bile duct injury [66, 132]. Table 6 highlights the common histopathologic findings from very early acute to late-chronic GvHD. The minimal histopathologic criteria required for acute or active GvHD include the presence of dysmorphic or attenuated “withered” bile ducts (Fig. 20) which may or may not occur in association with cholestasis, lobular, or portal inflammation (Fig. 21) [41]. These classic morphologic findings may be altered by the type and duration of immunosuppression, the use of ursodeoxycholic acid and any underlying liver disease. At a minimum, evidence of bile duct damage should be present. Lymphocytic portal infiltrate, lobular infiltrate, and prominent necroinflammatory activity can also be seen at any stage, most notably after cessation of immunosuppressive therapy [27]. In small biopsy specimens or cases where tissue was acquired early in disease progression, these findings may be minor or even absent [177, 178]. Very early changes are nonspecific and overlap with a variety of other etiologies [172, 179].

Acute hepatic GvHD. (a) High power showing nuclear pleomorphism/atypia (arrow), withered ducts and (b) cytoplasmic vacuolization (chevron) and neutrophilic/lymphocytic portal infiltrate (arrow)

Late-chronic hepatic GvHD showing high power of cholestasis (arrow), withered ducts (chevron), and vacuolated biliary epithelium (arrowhead)
The diagnosis of chronic hepatic GvHD requires distinctive manifestations in at least one other organ system such as the GI tract or skin [32]. The histopathologic features of chronic hepatic GvHD can also overlap with those of acute GvHD and the transition between the two may be subtle. The presence of marked biliary ductopenia and portal fibrosis suggest chronicity [132] but still a potentially reversible process [180]. In summary, the current criteria for chronic hepatic GvHD include ductopenia, portal fibrosis, chronic cholestasis but these are not specific for the disease (Fig. 22). Prolonged GvHD gives rise to a more pronounced cholestatic pattern in which canalicular bile plugs, pigment-laden macrophages and hepatocyte ballooning degeneration can be seen. It is not uncommon to observe also bile ductular proliferation (ductular reaction). Chronic hepatic GvHD rarely progresses to frank cirrhosis and this finding warrants extensive clinical and pathologic workup for other etiologies such as hepatitis C viral infection [181–184]. Parenthetically, other than the presence of bile ductular proliferation, the changes of GvHD in the liver closely resemble those found in chronic rejection of the liver allograft (see chapter “Liver Transplantation”).

Hepatic chronic GvHD showing centrilobular cholestasis (arrow) in the setting of interlobular bile duct loss
Histologic grading schemes for hepatic GvHD have been described but have shown poor correlation between clinical outcome and the severity of liver injury on histology (including bile duct injury and portal inflammation) [66, 185]. Moreover, none have been prospectively validated [40]. Due to their weak prognostic and predictive power, current guidelines do not recommend their use [41].
Ancillary Studies
The diagnosis of GvHD usually can be made on H&E-stained slides. Masson’s trichrome stain highlights portal fibrosis, and the loss of bile ducts can also be highlighted by immunohistochemical (IHC) staining for cytokeratin 7 or cytokeratin 19. Bile ductal cells can show the same senescence-related changes that are seen in chronic liver allograft rejection; these can be highlighted by p21 IHC staining [186]. However p21 staining, determination of the Th17/T regulatory cell ratio or C4d immunostaining have not been fully validated for routine clinical use [187, 188]. IHC or in situ hybridization for CMV, herpes simplex virus (HSV), adenovirus, varicella zoster virus, human herpesvirus-6 and Epstein-Barr virus (EBV) can be useful to exclude infectious causes of hepatic dysfunction.
Differential Diagnosis
The differential diagnosis of hepatic GvHD is broad and is dependent on the timing of presentation and the level of liver enzymatic abnormalities. Table 7 lists the important entities to consider in the setting of HSCT and abnormal liver function. Notably, CMV, adenovirus, and herpes simplex virus I/II should be ruled out as potentially treatable causes. Drugs, including cyclosporine, can cause a mild increase in bilirubin by altering bile transport [189]. As there is no definitive histologic pattern of this drug-related etiology, discontinuation of the drug(s), if possible, is helpful in establishing the cause. Sepsis can cause a cholestatic pattern of injury, resulting, in some cases in cholangitis lenta [190]. In the setting of hepatic GvHD and severe concomitant gastrointestinal GvHD, a severe bile ductular reaction with dilated ductules filled with bile pigment and fibrosis can occur and morphologically overlap with cholangitis lenta. In cases where viral hepatitis is suspected, the qualitative assessment of bile duct injury may be useful. Hepatitis C virus tends to incite focal rather than diffuse bile duct injury and has prominent lymphoid aggregates.
Iron Overload
Iron overload is now recognized as an important contributor to both hepatic and pulmonary disorders post-HSCT [191–193]. Iron overload can arise from repeated blood transfusions and by increased intestinal iron absorption secondary to ineffective hematopoiesis. Many patients, due to the nature of their underlying disease, present with a 1.25 fold increase in iron stores [194, 195]. This can increase the risk for systemic opportunistic infections and has been associated with a reduced overall survival [196–198]. Iron overload has also been implicated in the early development of SOS following HSCT [192]. A serum ferritin level over 1000 ng/mL is considered an adverse prognostic factor [199]. Prussian blue staining reveals increased iron in parenchymal cells (i.e., hepatocytes) and variably in mesenchymal cells (i.e., macrophages and endothelial cells) (Fig. 23) [200]. The pathologist should indicate the degree or “grade” of iron deposition and qualify its location (parenchymal vs. mesenchymal vs. mixed). The grade of iron in the liver can be assessed using either the semi-quantitative Scheuer system or more recent modifications [201–203]. Identifying iron overload in patient post-HSCT is particularly important because phlebotomy and chelation therapies can improve survival [193]. Hepatic iron overload can be superimposed on opportunistic infections such as Listeria monocytogenes, Mucormycosis, Yersinia enterocolitica, and non-cholera Vibrio species [195, 204, 205].

Hepatic iron overload. High power H&E (a) and iron (b) stains demonstrating increased iron in hepatocytes and in macrophages. This patient had received multiple blood transfusions
Sinusoidal Obstruction Syndrome
Introduction
SOS [206], previously termed veno-occlusive disease of the liver (VOD) [207] results from cytotoxic liver injury. It is characterized by obliterative venulitis of the terminal hepatic venules. SOS is linked to myeloablative regimens for HSCT, cyclophosphamide, and TBI.
The incidence of SOS varies, with centers reporting rates as low as 5.3 % to upwards of 54 %, depending on the type and dose of various chemotherapeutic agents and the use of TBI [208–212]. Recent studies have suggested that the rate of SOS has dropped dramatically due to lower doses of TBI, the use of fludarabine and the utilization of prophylactic therapy in patients considered at increased risk [212]. SOS is associated with increased morbidity and mortality, and severe SOS confers a mortality rate surpassing 90 % [210, 211].
SOS usually manifests within 10–21 days posttransplant [213] but can occur up to 50 days [214]. SOS severity can be graded by different sets of clinical parameters. One approach classifies SOS as mild when resolution occurs in the absence of treatment, moderate when resolution occurs after therapeutic intervention, and severe when patients show signs and symptoms of SOS-related liver disease that do not resolve before the 100th day post-HSCT or which cause death [208]. Most patients succumb to renal, cardiorespiratory, and multiorgan failure [211]. Another scheme for severity of SOS is based on modifications of clinical parameters used in the Modified Seattle and Baltimore criteria detailed below [215].
Clinical Presentation and Risk Factors
The classic presentation of SOS includes painful hepatomegaly, jaundice, and rapid weight gain due to fluid retention (ascites) [216]. The Modified Seattle [217] and the Baltimore criteria [218] both factor in hepatomegaly, weight gain, and bilirubin levels but differ in their diagnostic weighting (see Table 8). Moreover, the presence of portal hypertension, renal and pulmonary dysfunction as well as refractory thrombocytopenia provides additional support for the diagnosis of SOS [212]. Currently there are no laboratory parameters with diagnostic specificity or prognostic significance.
In most cases the diagnosis of SOS is a clinical diagnosis and a liver biopsy is reserved for inconclusive or atypical presentations. Several studies have advocated a transvenous approach, that allows for simultaneous tissue biopsy sampling and hemodynamic measurements of free and wedged hepatic venous pressures (and therefore the hepatic venous pressure gradient), and provides the most accurate diagnosis of SOS [219, 220]. A hepatic venous pressure gradient >10 mmHg is highly specific and sensitive for the diagnosis of SOS in the appropriate clinical setting (e.g., provided there is no cirrhosis).
Factors that increase risk for the development of SOS in HSCT patients include advanced age, a history of prior liver injury (such as viral hepatitis, steatohepatitis, iron overload), systemic inflammation, infection and long-term use of antibiotics [221, 222].
Pathogenesis of SOS
The pathogenesis of SOS and the sequence of events have been established in rodent models [206] and are described below. The initiating event is sinusoidal endothelial cell injury; endothelial cells appear to be more susceptible to cytotoxic injury than hepatocytes [222, 223]. By light microscopy, very early in the course of the disease (24–48 h) the earliest manifestations are gradual subtle injury of sinusoidal endothelial cells and sinusoidal hemorrhage [206]. Between 3 and 5 days, there was marked sinusoidal and central venous endothelial damage with sloughing and downstream embolization into the sinusoids and subsequent obstruction, associated with predominantly centrilobular hemorrhage and coagulative necrosis of hepatocytes (Fig. 24) [224]. Livers at days 6–7 show deposition of subendothelial and adventitial fibrosis mediated by proliferation of stellate cells and of subendothelial fibroblasts. By day 8, either resolution ensues or the hepatic injury persists as variably severe late SOS.

Sinusoidal obstruction syndrome in liver biopsy from a patient following chemotherapy. Note hemorrhage, sinusoidal congestion, and the atrophic hepatocytes
Histopathologic Findings
The histologic hallmark of SOS is luminal obliteration of central (terminal hepatic) veins (Fig. 25). Table 9 highlights the principal histopathologic findings and differential diagnoses are enumerated in Table 10.

Sinusoidal obstruction syndrome showing a medium-sized-central vein (a) with near complete luminal obliteration. Trichrome (b) and reticulin (c) stains highlight perivenular fibrosis and recanalization
Ancillary Studies and Immunohistochemical Findings
In the appropriate clinical context the majority of cases of SOS can be established by the presence of obliterative venulitis and fibrosis using routine H&E-stained slides in combination with Masson’s trichrome and/or reticulin stains. It has been suggested that sinusoidal capillarization defined as the ultrastructural transformation of endothelial sinusoidal cells into cells that more closely resemble capillary vessels can be highlighted by CD34 positivity and may be contributed to the hepatic dysfunction of SOS [225, 226]. However, immunostains for CD34 are not used routinely in the diagnosis of SOS.
Nodular Regenerative Hyperplasia
Nodular regenerative hyperplasia (NRH ) in HSCT is thought to result from hepatic vascular injury in the setting of SOS or it may represent a manifestation of chemotherapy-induced drug injury. It arises as a specific adaptive response to changes in blood flow secondary to a wide variety of insults [227]. Histologically, it is characterized by partial or complete transformation of the normal liver parenchyma into hepatocellular nodules less than 3 mm in diameter. These nodules contain regenerating hepatocytes more than one cell wide, and are not associated with periportal or perisinusoidal fibrosis or septa. The regenerating nodules cause compression of adjacent structures, leading to hepatocyte atrophy and sinusoidal dilatation, best highlighted with a reticulin stain. NRH is often asymptomatic but may be complicated by portal hypertension, bleeding varices, ascites, and splenomegaly [228].
Summary
The principal types of HSCT are autologous and allogeneic: the choice is dependent on the primary disease, the availability of a suitable donor, and recipient-related issues.
Autologous HSCT has the advantage of near absence of graft-versus-host (GvHD) but the drawback of increased disease recurrence.
Allogeneic HSCT, important in the therapy of many hematological conditions, has the advantage of an important graft-versus-malignancy effect but the complication of GvHD.
GvHD is currently classified as acute and chronic primarily on clinical features rather than the arbitrary cutoff of 100 days.
The histopathologic findings of GvHD are often nonspecific and require careful clinical correlation and preferably confirmation by multiorgan involvement.
The principal bone marrow complications following HSCT are persistence of hypocellularity, infection, and persistence or relapse of the primary malignancy.
The key features of cutaneous acute GvHD are apoptosis in the lower malphigian epithelium and basal layers of appendages, satellitosis, and lichenoid inflammation.
There are several forms of chronic GvHD in the skin: the pathologic features overlap with those of acute GvHD but also display variable inflammation and fibrosis of deeper layers of dermis and subcutaneous tissue.
Pulmonary complications are important determinants in the outcome of patients following HSCT.
Infections remain an important consideration and should be carefully evaluated in all cytologic and histopathologic specimens.
Most of the acute non-infectious complications are categorized under the umbrella term of “idiopathic pneumonia syndrome.” It likely represents a manifestation of GvHD. The pathologic manifestations include several entities characterized pathologically by variable pulmonary edema and/or hemorrhage, DAD and interstitial or organizing pneumonias.
The subacute and chronic forms of GvHD are COP and bronchiolitis obliterans, respectively. The latter is the most characteristic and has a poor prognosis.
Pulmonary alveolar proteinosis, pulmonary hypertension, and pulmonary cytolytic thrombi are occasionally encountered after HSCT.
The principal renal complications following HSCT are acute tubular necrosis, thrombotic microangiopathy and glomerulopathy; the relationship of the latter two to GvHD remains unsettled.
The gastrointestinal tract is the second most common site of involvement by GvHD. The principal pathologic finding in acute GvHD is crypt or gastric gland epithelial cell apoptosis. Differential diagnostic considerations include infection (e.g., CMV) and drug-related alterations.
The pathologic findings of GvHD in the liver closely resemble those of chronic liver allograft rejection and include dysmorphic or attenuated “withered” bile ducts, ductopenia (in advanced stages), variable cholestasis, and lobular, and/or portal inflammation. Other hepatic alterations following HSCT that should be included in the pathology report include the presence of iron overload and sinusoidal obstruction syndrome.
References
Giralt S, Bishop MR. Principles and overview of allogeneic hematopoietic stem cell transplantation. In: Bishop MR, editor. Hematopoietic stem cell transplantation. Cancer treatment and Research. Berlin: Springer; 2009. p. 1–21.
Armitage JO. Bone marrow transplantation. N Engl J Med. 1994;330(12):827–38.
Weissman IL. Translating stem and progenitor cell biology to the clinic: barriers and opportunities. Science. 2000;287(5457):1442–6.
Heslop HE. Overview of hematopoietic stem cell transplantation. In: Hoffman R, Benz Jr EJ, Silberstein LE, Heslop HE, Weitz JI, Anastasi J, editors. Hematology basic principles and practice. Philadelphia, PA: Saunders/Elsevier; 2013. p. 1542–5.
Rafii S, Lyden D. Therapeutic stem and progenitor cell transplantation for organ vascularization and regeneration. Nat Med. 2003;9(6):702–12.
Clark ML, Lynch FX. Clinical symptoms of radiation sickness, time to onset and duration of symptoms among Hiroshima survivors in the lethal and median lethal ranges of radiation. Mil Surg. 1952;111(5):360–8.
Thomas ED. A history of allogeneic hematopoietic cell transplantation. In: Appelbaum FR, Forman SJ, Negrin RS, Blume KG, editors. Thomas’ hematopoietic cell transplantation. 4th ed. Oxford: Wiley-Blackwell; 2009. p. 1–7.
Thomas E, Storb R, Clift RA, Fefer A, Johnson FL, Neiman PE, et al. Bone-marrow transplantation (first of two parts). N Engl J Med. 1975;292(16):832–43.
Thomas ED, Buckner CD, Banaji M, Clift RA, Fefer A, Flournoy N, et al. One hundred patients with acute leukemia treated by chemotherapy, total body irradiation, and allogeneic marrow transplantation. Blood. 1977;49(4):511–33.
Thomas ED, Buckner CD, Clift RA, Fefer A, Johnson FL, Neiman PE, et al. Marrow transplantation for acute nonlymphoblastic leukemia in first remission. N Engl J Med. 1979;301(11):597–9.
Thomas ED, Fefer A, Buckner CD, Storb R. Current status of bone marrow transplantation for aplastic anemia and acute leukemia. Blood. 1977;49(5):671–81.
Thomas ED, Storb R, Clift RA, Fefer A, Johnson L, Neiman PE, et al. Bone-marrow transplantation (second of two parts). N Engl J Med. 1975;292(17):895–902.
Treleaven J. Introduction. In: Treleaven J, Barrett AJ, editors. Hematopoietic stem cell transplantation in clinical practice. Edinburgh: Churchill Livingstone/Elsevier; 2009. p. 3–8.
Armitage JO. The history of autologous hematopoietic cell transplantation. In: Appelbaum FR, Forman SJ, Negrin RS, Blume KG, editors. Thomas’ hematopoietic cell transplantation. Oxford: Wiley-Blackwell; 2009. p. 8–14.
Antman KS, Griffin JD, Elias A, Socinski MA, Ryan L, Cannistra SA, et al. Effect of recombinant human granulocyte-macrophage colony-stimulating factor on chemotherapy-induced myelosuppression. N Engl J Med. 1988;319(10):593–8.
Socinski MA, Cannistra SA, Elias A, Antman KH, Schnipper L, Griffin JD. Granulocyte-macrophage colony stimulating factor expands the circulating haemopoietic progenitor cell compartment in man. Lancet. 1988;1(8596):1194–8.
Groth CG, Brent LB, Calne RY, Dausset JB, Good RA, Murray JE, et al. Historic landmarks in clinical transplantation: conclusions from the consensus conference at the University of California, Los Angeles. World J Surg. 2000;24(7):834–43.
Dicke KA, Zander A, Spitzer G, Verma DS, Peters L, Vellekoop L, et al. Autologous bone-marrow transplantation in relapsed adult acute leukaemia. Lancet. 1979;1(8115):514–7.
Vaughan W, Seshadri T, Bridges M, Keating A. The principles and overview of autologous hematopoietic stem cell transplantation. In: Bishop MR, editor. Hematopoietic stem cell transplantation. Cancer treatment and research. Berlin: Springer; 2009. p. 23–45.
Pasquini M, Wang Z (2013) Current use and outcome of hematopoietic stem cell transplantation: CIBMTR Summary Slides 2012. Available from http://www.cibmtr.org
Hari P, Horowitz M. Indications and outcome of allogeneic hematopoietic cell transplantation for hematologic malignancies in adults. In: Hoffman R, Benz Jr EJ, Silberstein LE, Heslop HE, Weitz JI, Anastasi J, editors. Hematology basic principles and practice. Philadelphia, PA: Saunders/Elsevier; 2013. p. 1546–56.
Lazarus HM, Laughlin MJ. Allogeneic stem cell transplantation. In: Karp JE, editor. New York: Humana Springer; 2010. 883 p
Jaffe ES, Harris NL, Vardiman JW, Campo E, Arber DA. Hematopathology. St. Louis: Saunders/Elsevier; 2011. 1058 p.
Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. WHO classification of tumours of haematopoietic and lymphoid tissues. 4th ed. Lyon: International Agency for Research on Cancer; 2008. 439 p.
Orazi A, Foucar K, Knowles D, Weiss LM. Knowles neoplastic hematopathology. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2014. 1304 p.
Soll E, Massumoto C, Clift RA, Buckner CD, Appelbaum FR, Storb R, et al. Relevance of marrow fibrosis in bone marrow transplantation: a retrospective analysis of engraftment. Blood. 1995;86(12):4667–73.
Shulman HM, Hackman RC, Sale GE. Pathology of hematopoietic cell transplantation. In: Appelbaum FR, Forman SJ, Negrin RS, Blume KG, editors. Thomas’ hematopoietic cell transplantation. 4th ed. Oxford: Wiley-Blackwell; 2009. p. 390–405.
Ljungman P. Viral infections in hematopoietic stem cell transplant recipients. In: Lazarus HM, Laughlin MJ, editors. Allogeneic stem cell transplantation. Contemporary hematology. 2nd ed. New York: Humana Springer; 2010. p. 505–32.
Wingard JR. Fungal infections. In: Lazarus HM, Laughlin MJ, editors. Allogeneic stem cell transplantation. Contemporary hematology. 2nd ed. New York: Humana Springer; 2010. p. 533–44.
Kradin RL. Diagnostic pathology of infectious disease. Philadelphia, PA: Saunders Elsevier; 2010. 644 p.
Goldman JM. Allogeneic stem cell transplantation: The last century. In: Lazarus HM, Laughlin MJ, editors. Allogeneic stem cell transplantation. Contemporary hematology. 2nd ed. New York: Humana Press Springer; 2010. p. 1–9.
Filipovich AH, Weisdorf D, Pavletic S, Socie G, Wingard JR, Lee SJ, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005;11(12):945–56.
Jagasia MH, Greinix HT, Arora M, Williams KM, Wolff D, Cowen EW, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. The 2014 diagnosis and staging working group report. Biol Blood Marrow Transplant. 2015;21(3):389–401. e1.
Shulman HM, Sullivan KM, Weiden PL, McDonald GB, Striker GE, Sale GE, et al. Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am J Med. 1980;69(2):204–17.
Deeg J, Flowers MED. Acute graft-versus-host disease. In: Treleaven J, Barrett AJ, editors. Hematopoietic stem cell transplantation in clinical practice. Edinburgh: Churchill Livingstone/Elsevier; 2009. p. 387–400.
Rowlings PA, Przepiorka D, Klein JP, Gale RP, Passweg JR, Henslee-Downey PJ, et al. IBMTR severity index for grading acute graft-versus-host disease: retrospective comparison with Glucksberg grade. Br J Haematol. 1997;97(4):855–64.
Goldstein SC, Stein SD, Porter DL. Treatment of acute graft-vs-host disease. In: Lazarus HM, Laughlin MJ, editors. Allogeneic stem cell transplantation. Contemporary hematology. 2nd ed. New York: Springer; 2010. p. 747–65.
Watkins TR, Chien JW, Crawford SW. Graft versus host-associated pulmonary disease and other idiopathic pulmonary complications after hematopoietic stem cell transplant. Semin Respir Crit Care Med. 2005;26(5):482–9.
Jagasia M, Pavletic S. Chronic graft-versus-host disease. In: Lazarus HM, Laughlin MJ, editors. Allogeneic stem cell transplantation. Contemporary hematology. 2nd ed. New York: Springer; 2010. p. 577–95.
Shulman HM, Kleiner D, Lee SJ, Morton T, Pavletic SZ, Farmer E, et al. Histopathologic diagnosis of chronic graft-versus-host disease: National Institutes of Health Consensus Development Project on criteria for clinical trials in chronic graft-versus-host disease: II. Pathology Working Group Report. Biol Blood Marrow Transplant. 2006;12(1):31–47.
Shulman HM, Cardona DM, Greenson JK, Hingorani S, Horn T, Huber E, et al. NIH consensus development project on criteria for clinical trials in chronic graft-versus-host disease: II. The 2014 Pathology Working Group Report. Biol Blood Marrow Transplant. 2015;21(4):589–603.
Wilkins BS, Bostanci AG, Ryan MF, Jones DB. Haemopoietic regrowth after chemotherapy for acute leukaemia: an immunohistochemical study of bone marrow trephine biopsy specimens. J Clin Pathol. 1993;46(10):915–21.
van Marion AM, Thiele J, Kvasnicka HM, van den Tweel JG. Morphology of the bone marrow after stem cell transplantation. Histopathology. 2006;48(4):329–42.
Wittels B. Bone marrow biopsy changes following chemotherapy for acute leukemia. Am J Surg Pathol. 1980;4(2):135–42.
Natkunam Y, Arber DA. Evaluation of the bone marrow after therapy. In: Jaffe ES, Harris NL, Vardiman JW, Campo E, Arber DA, editors. Hematopathology. St. Louis: Saunders/Elsevier; 2011. p. 918–38.
Reichard K. Post-therapy bone marrow findings. In: Foucar K, Reichard K, Czuchlewski D, editors. Bone marrow pathology. 2. 3rd ed. Chicago: ASCP Press; 2010. p. 792–817.
Foucar K. Bone marrow stroma and bone disorders. In: Foucar K, Reichard K, Czuchlewski D, editors. Bone marrow pathology. Chicago: ASCP Press; 2010. p. 652–85.
Thiele J, Kvasnicka HM, Beelen DW, Wenzel P, Koepke ML, Leder LD, et al. Macrophages and their subpopulations following allogenic bone marrow transplantation for chronic myeloid leukaemia. Virchows Arch. 2000;437(2):160–6.
van den Berg H, Kluin PM, Vossen JM. Early reconstitution of haematopoiesis after allogeneic bone marrow transplantation: a prospective histopathological study of bone marrow biopsy specimens. J Clin Pathol. 1990;43(5):365–9.
van den berg H, Kluin PM, Zwaan FE, Vossen JM. Histopathology of bone marrow reconstitution after allogeneic bone marrow transplantation. Histopathology. 1989;15(4):363–73.
Martinez-Jaramillo G, Gomez-Morales E, Sanchez-Valle E, Mayani H. Severe hematopoietic alterations in vitro, in bone marrow transplant recipients who develop graft-versus-host disease. J Hematother Stem Cell Res. 2001;10(3):347–54.
Saavedra S, Jarque I, Sanz GF, Moscardo F, Jimenez C, Martin G, et al. Infectious complications in patients undergoing unrelated donor bone marrow transplantation: experience from a single institution. Clin Microbiol Infect. 2002;8(11):725–33.
Reichard K. Minimal residual disease. In: Foucar K, Reichard K, Czuchlewski D, editors. Bone marrow pathology. 3rd ed. Chicago: ASCP Press; 2010. p. 818–25.
Khan F, Agarwal A, Agrawal S. Significance of chimerism in hematopoietic stem cell transplantation: new variations on an old theme. Bone Marrow Transplant. 2004;34(1):1–12.
McCann SR, Crampe M, Molloy K, Lawler M. Hemopoietic chimerism following stem cell transplantation. Transfus Apher Sci. 2005;32(1):55–61.
Stikvoort A, Gertow J, Sundin M, Remberger M, Mattsson J, Uhlin M. Chimerism patterns of long-term stable mixed chimeras posthematopoietic stem cell transplantation in patients with nonmalignant diseases: follow-up of long-term stable mixed chimerism patients. Biol Blood Marrow Transplant. 2013;19(5):838–44.
Hymes SR, Alousi AM, Cowen EW. Graft-versus-host disease: part I. Pathogenesis and clinical manifestations of graft-versus-host disease. J Am Acad Dermatol. 2012;66(4):515e1–18. quiz 33-4.
Biedermann BC, Sahner S, Gregor M, Tsakiris DA, Jeanneret C, Pober JS, et al. Endothelial injury mediated by cytotoxic T lymphocytes and loss of microvessels in chronic graft versus host disease. Lancet. 2002;359(9323):2078–83.
Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J, et al. 1994 consensus conference on acute GVHD grading. Bone Marrow Transplant. 1995;15(6):825–8.
Baird K, Steinberg SM, Grkovic L, Pulanic D, Cowen EW, Mitchell SA, et al. National Institutes of Health chronic graft-versus-host disease staging in severely affected patients: organ and global scoring correlate with established indicators of disease severity and prognosis. Biol Blood Marrow Transplant. 2013;19(4):632–9.
Hymes SR, Turner ML, Champlin RE, Couriel DR. Cutaneous manifestations of chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2006;12(11):1101–13.
Patterson JW. The spongiotic reaction pattern. In: Patterson JW, Hosler GA, editors. Weedon’s skin pathology. Philadelphia, PA: Churchill Livingstone/Elsevier; 2016. p. 103–34.
Kuykendall TD, Smoller BR. Lack of specificity in skin biopsy specimens to assess for acute graft-versus-host disease in initial 3 weeks after bone-marrow transplantation. J Am Acad Dermatol. 2003;49(6):1081–5.
Firoz BF, Lee SJ, Nghiem P, Qureshi AA. Role of skin biopsy to confirm suspected acute graft-vs-host disease: results of decision analysis. Arch Dermatol. 2006;142(2):175–82.
Kohler S, Hendrickson MR, Chao NJ, Smoller BR. Value of skin biopsies in assessing prognosis and progression of acute graft-versus-host disease. Am J Surg Pathol. 1997;21(9):988–96.
Lerner KG, Kao GF, Storb R, Buckner CD, Clift RA, Thomas ED. Histopathology of graft-vs.-host reaction (GvHR) in human recipients of marrow from HL-A-matched sibling donors. Transplant Proc. 1974;6(4):367–71.
Horn TD. Acute cutaneous eruptions after marrow ablation: roses by other names? J Cutan Pathol. 1994;21(5):385–92.
Horn TD, Bauer DJ, Vogelsang GB, Hess AD. Reappraisal of histologic features of the acute cutaneous graft-versus-host reaction based on an allogeneic rodent model. J Invest Dermatol. 1994;103(2):206–10.
Zhou Y, Barnett MJ, Rivers JK. Clinical significance of skin biopsies in the diagnosis and management of graft-vs-host disease in early postallogeneic bone marrow transplantation. Arch Dermatol. 2000;136(6):717–21.
Creamer D, Martyn-Simmons CL, Osborne G, Kenyon M, Salisbury JR, Devereux S, et al. Eczematoid graft-vs-host disease: a novel form of chronic cutaneous graft-vs-host disease and its response to psoralen UV-A therapy. Arch Dermatol. 2007;143(9):1157–62.
Patterson JW. Cutaneous infections and infestations—histological patterns. In: Patterson JW, Hosler GA, editors. Weedon's skin pathology. Philadelphia, PA: Churchill Livingstone/Elsevier; 2016. p. 633–5.
Schultz KR, Miklos DB, Fowler D, Cooke K, Shizuru J, Zorn E, et al. Toward biomarkers for chronic graft-versus-host disease: National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: III. Biomarker Working Group Report. Biol Blood Marrow Transplant. 2006;12(2):126–37.
Bridge AT, Nelson Jr RP, Schwartz JE, Mirowski GW, Billings SD. Histological evaluation of acute mucocutaneous graft-versus-host disease in nonmyeloablative hematologic stem cell transplants with an observation predicting an increased risk of progression to chronic graft-versus-host disease. Am J Dermatopathol. 2007;29(1):1–6.
Oyama Y, Cohen B, Traynor A, Brush M, Rodriguez J, Burt RK. Engraftment syndrome: a common cause for rash and fever following autologous hematopoietic stem cell transplantation for multiple sclerosis. Bone Marrow Transplant. 2002;29(1):81–5.
Sviland L, Pearson AD, Eastham EJ, Hamilton PJ, Proctor SJ, Malcolm AJ. Histological features of skin and rectal biopsy specimens after autologous and allogeneic bone marrow transplantation. J Clin Pathol. 1988;41(2):148–54.
Marra DE, McKee PH, Nghiem P. Tissue eosinophils and the perils of using skin biopsy specimens to distinguish between drug hypersensitivity and cutaneous graft-versus-host disease. J Am Acad Dermatol. 2004;51(4):543–6.
Weaver J, Bergfeld WF. Quantitative analysis of eosinophils in acute graft-versus-host disease compared with drug hypersensitivity reactions. Am J Dermatopathol. 2010;32(1):31–4.
LeBoit PE. Subacute radiation dermatitis: a histologic imitator of acute cutaneous graft-versus-host disease. J Am Acad Dermatol. 1989;20(2 Pt 1):236–41.
Sale GE, Lerner KG, Barker EA, Shulman HM, Thomas ED. The skin biopsy in the diagnosis of acute graft-versus-host disease in man. Am J Pathol. 1977;89(3):621–36.
Patterson JW. The lichenoid reaction pattern (‘interface dermatitis’). In: Patterson JW, Hosler GA, editors. Weedon's skin pathology. Philadelphia, PA: Churchill Livingstone/Elsevier; 2016. p. 38–80.
Nellen RG, van Marion AM, Frank J, Poblete-Gutierrez P, Steijlen PM. Eruption of lymphocyte recovery or autologous graft-versus-host disease? Int J Dermatol. 2008;47 Suppl 1:32–4.
Roux J, Battistella M, Fornecker L, Legoff J, Deau B, Houhou N, et al. Human Herpesvirus-6 cytopathic inclusions: an exceptional and recognizable finding on skin biopsy during HHV6 reactivation after autologous stem-cell transplantation. Am J Dermatopathol. 2012;34(6):e73–6.
Vidal CI, Pollack M, Uliasz A, del Toro G, Emanuel PO. Cutaneous toxoplasmosis histologically mimicking graft-versus-host disease. Am J Dermatopathol. 2008;30(5):492–3.
Byun HJ, Yang JI, Kim BK, Cho KH. Clinical differentiation of acute cutaneous graft-versus-host disease from drug hypersensitivity reactions. J Am Acad Dermatol. 2011;65(4):726–32.
Nghiem P. The “drug vs graft-vs-host disease” conundrum gets tougher, but there is an answer: the challenge to dermatologists. Arch Dermatol. 2001;137(1):75–6.
Neiman P, Wasserman PB, Wentwort BB, Kao GF, Lerner KG, Storb R, et al. Interstitial pneumonia and cytomegalovirus infection as complications of human marrow transplantation. Transplantation. 1973;15(5):478–85.
Meyers JD, Flournoy N, Thomas ED. Nonbacterial pneumonia after allogeneic marrow transplantation—a review of 10 years experience. Rev Infect Dis. 1982;4(6):1119–32.
Afessa B, Litzow MR, Tefferi A. Bronchiolitis obliterans and other late onset non-infectious pulmonary complications in hematopoietic stem cell transplantation. Bone Marrow Transplant. 2001;28(5):425–34.
Adam AK, Zamlut M, Soubani AO. The yield and safety of thoracentesis in hematopoietic stem cell transplantation recipients. Lung. 2007;185(5):257–62.
Majhail NS, Weisdorf DJ. Complications after hematopoietic stem cell transplantation. In: Hoffman R, Benz Jr EJ, Silberstein LE, Heslop HE, Weitz JI, Anastasi J, editors. Hematology basic principles and practice. Philadelphia, PA: Saunders/Elsevier; 2013. p. 1612–26.
Panoskaltsis-Mortari A, Griese M, Madtes DK, Belperio JA, Haddad IY, Folz RJ, et al. An official American Thoracic Society research statement: noninfectious lung injury after hematopoietic stem cell transplantation: idiopathic pneumonia syndrome. Am J Respir Crit Care Med. 2011;183(9):1262–79.
Haddad IY. Stem cell transplantation and lung dysfunction. Curr Opin Pediatr. 2013;25(3):350–6.
Wilczynski SW, Erasmus JJ, Petros WP, Vredenburgh JJ, Folz RJ. Delayed pulmonary toxicity syndrome following high-dose chemotherapy and bone marrow transplantation for breast cancer. Am J Respir Crit Care Med. 1998;157(2):565–73.
Todd NW, Peters WP, Ost AH, Roggli VL, Piantadosi CA. Pulmonary drug toxicity in patients with primary breast cancer treated with high-dose combination chemotherapy and autologous bone marrow transplantation. Am Rev Respir Dis. 1993;147(5):1264–70.
Afessa B, Peters SG. Noninfectious pneumonitis after blood and marrow transplant. Curr Opin Oncol. 2008;20(2):227–33.
Gorak E, Geller N, Srinivasan R, Espinoza-Delgado I, Donohue T, Barrett AJ, et al. Engraftment syndrome after nonmyeloablative allogeneic hematopoietic stem cell transplantation: incidence and effects on survival. Biol Blood Marrow Transplant. 2005;11(7):542–50.
Capizzi SA, Kumar S, Huneke NE, Gertz MA, Inwards DJ, Litzow MR, et al. Peri-engraftment respiratory distress syndrome during autologous hematopoietic stem cell transplantation. Bone Marrow Transplant. 2001;27(12):1299–303.
Clark JG, Hansen JA, Hertz MI, Parkman R, Jensen L, Peavy HH. NHLBI workshop summary. Idiopathic pneumonia syndrome after bone marrow transplantation. Am Rev Respir Dis. 1993;147(6 Pt 1):1601–6.
Yanik GA, Grupp SA, Pulsipher MA, Levine JE, Schultz KR, Wall DA, et al. TNF-receptor inhibitor therapy for the treatment of children with idiopathic pneumonia syndrome. A joint Pediatric Blood and Marrow Transplant Consortium and Children's Oncology Group study (ASCT0521). Biol Blood Marrow Transplant. 2015;21(1):67–73.
Afessa B, Tefferi A, Litzow MR, Krowka MJ, Wylam ME, Peters SG. Diffuse alveolar hemorrhage in hematopoietic stem cell transplant recipients. Am J Respir Crit Care Med. 2002;166(5):641–5.
De Lassence A, Fleury-Feith J, Escudier E, Beaune J, Bernaudin JF, Cordonnier C. Alveolar hemorrhage. Diagnostic criteria and results in 194 immunocompromised hosts. Am J Respir Crit Care Med. 1995;151(1):157–63.
Agusti C, Ramirez J, Picado C, Xaubet A, Carreras E, Ballester E, et al. Diffuse alveolar hemorrhage in allogeneic bone marrow transplantation. A postmortem study. Am J Respir Crit Care Med. 1995;151(4):1006–10.
Srivastava A, Gottlieb D, Bradstock KF. Diffuse alveolar hemorrhage associated with microangiopathy after allogeneic bone-marrow transplantation. Bone Marrow Transplant. 1995;15(6):863–7.
Majhail NS, Parks K, Defor TE, Weisdorf DJ. Diffuse alveolar hemorrhage and infection-associated alveolar hemorrhage following hematopoietic stem cell transplantation: related and high-risk clinical syndromes. Biol Blood Marrow Transplant. 2006;12(10):1038–46.
Travis WD, Costabel U, Hansell DM, King Jr TE, Lynch DA, Nicholson AG, et al. An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733–48.
Yousem SA. The histological spectrum of pulmonary graft-versus-host disease in bone marrow transplant recipients. Hum Pathol. 1995;26(6):668–75.
Xu L, Drachenberg C, Tavora F, Burke A. Histologic findings in lung biopsies in patients with suspected graft-versus-host disease. Hum Pathol. 2013;44(7):1233–40.
Yoshihara S, Yanik G, Cooke KR, Mineishi S. Bronchiolitis obliterans syndrome (BOS), bronchiolitis obliterans organizing pneumonia (BOOP), and other late-onset noninfectious pulmonary complications following allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2007;13(7):749–59.
Hildebrandt GC, Fazekas T, Lawitschka A, Bertz H, Greinix H, Halter J, et al. Diagnosis and treatment of pulmonary chronic GVHD: report from the consensus conference on clinical practice in chronic GVHD. Bone Marrow Transplant. 2011;46(10):1283–95.
Nakaseko C, Ozawa S, Sakaida E, Sakai M, Kanda Y, Oshima K, et al. Incidence, risk factors and outcomes of bronchiolitis obliterans after allogeneic stem cell transplantation. Int J Hematol. 2011;93(3):375–82.
Uhlving HH, Andersen CB, Christensen IJ, Gormsen M, Pedersen KD, Buchvald F, et al. Biopsy-verified bronchiolitis obliterans and other noninfectious lung pathologies after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2015;21(3):531–8.
Borie R, Danel C, Debray MP, Taille C, Dombret MC, Aubier M, et al. Pulmonary alveolar proteinosis. Eur Respir Rev. 2011;20(120):98–107.
Patel SM, Sekiguchi H, Reynolds JP, Krowka MJ. Pulmonary alveolar proteinosis. Can Respir J. 2012;19(4):243–5.
Ansari M, Rougemont AL, Le Deist F, Ozsahin H, Duval M, Champagne MA, et al. Secondary pulmonary alveolar proteinosis after unrelated cord blood hematopoietic cell transplantation. Pediatr Transplant. 2012;16(5):E146–9.
Sharma S, Nadrous HF, Peters SG, Tefferi A, Litzow MR, Aubry MC, et al. Pulmonary complications in adult blood and marrow transplant recipients: autopsy findings. Chest. 2005;128(3):1385–92.
Pidala J, Khalil F, Fernandez H. Pulmonary alveolar proteinosis following allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. 2011;46(11):1480–3.
Grigg A, Buchanan M, Whitford H. Late-onset pulmonary arterial hypertension in association with graft-versus-host disease after allogeneic stem-cell transplantation. Am J Hematol. 2005;80(1):38–42.
Limsuwan A, Pakakasama S, Rochanawutanon M, Hong-eng S. Pulmonary arterial hypertension after childhood cancer therapy and bone marrow transplantation. Cardiology. 2006;105(3):188–94.
Höra J. Zur histologie der klinischen “primaren Pulmonalsklerose”. Frankf Z Pathol. 1934;47:100.
Troussard X, Bernaudin JF, Cordonnier C, Fleury J, Payen D, Briere J, et al. Pulmonary veno-occlusive disease after bone marrow transplantation. Thorax. 1984;39(12):956–7.
Smith AR, Gulbahce E, Burke MJ, Cao Q, Macmillan ML, Tolar J, et al. Lower leukemia relapse in pediatric patients with pulmonary cytolytic thrombi following allogeneic transplant. Bone Marrow Transplant. 2011;46(3):368–71.
Gulbahce HE, Pambuccian SE, Jessurun J, Woodard P, Steiner ME, Manivel JC, et al. Pulmonary nodular lesions in bone marrow transplant recipients: impact of histologic diagnosis on patient management and prognosis. Am J Clin Pathol. 2004;121(2):205–10.
Gulbahce HE, Manivel JC, Jessurun J. Pulmonary cytolytic thrombi: a previously unrecognized complication of bone marrow transplantation. Am J Surg Pathol. 2000;24(8):1147–52.
Morales IJ, Anderson PM, Tazelaar HD, Wylam ME. Pulmonary cytolytic thrombi: unusual complication of hematopoietic stem cell transplantation. J Pediatr Hematol Oncol. 2003;25(1):89–92.
Peters A, Manivel JC, Dolan M, Gulbahce HE, Baker KS, Verneris MR. Pulmonary cytolytic thrombi after allogeneic hematopoietic cell transplantation: a further histologic description. Biol Blood Marrow Transplant. 2005;11(6):484–5.
Chang A, Hingorani S, Kowalewska J, Flowers ME, Aneja T, Smith KD, et al. Spectrum of renal pathology in hematopoietic cell transplantation: a series of 20 patients and review of the literature. Clin J Am Soc Nephrol. 2007;2(5):1014–23.
Troxell ML, Pilapil M, Miklos DB, Higgins JP, Kambham N. Renal pathology in hematopoietic cell transplantation recipients. Mod Pathol. 2008;21(4):396–406.
Brukamp K, Doyle AM, Bloom RD, Bunin N, Tomaszewski JE, Cizman B. Nephrotic syndrome after hematopoietic cell transplantation: do glomerular lesions represent renal graft-versus-host disease? Clin J Am Soc Nephrol. 2006;1(4):685–94.
El-Seisi S, Gupta R, Clase CM, Forrest DL, Milandinovic M, Couban S. Renal pathology at autopsy in patients who died after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2003;9(11):683–8.
Bacigalupo A, Ballen K, Rizzo D, Giralt S, Lazarus H, Ho V, et al. Defining the intensity of conditioning regimens: working definitions. Biol Blood Marrow Transplant. 2009;15(12):1628–33.
Tuncer HH, Rana N, Milani C, Darko A, Al-Homsi SA. Gastrointestinal and hepatic complications of hematopoietic stem cell transplantation. World J Gastroenterol. 2012;18(16):1851–60.
Kambham N, Higgins JP, Sundram U, Troxell ML. Hematopoietic stem cell transplantation: graft versus host disease and pathology of gastrointestinal tract, liver, and lung. Adv Anat Pathol. 2014;21(5):301–20.
Ferrara JLM, Deeg HJ, Burakoff SJ. Graft-vs.-host disease. 2nd ed. New York: Marcel Dekker; 1997. 824 p.
Przepiorka D, Smith TL, Folloder J, Khouri I, Ueno NT, Mehra R, et al. Risk factors for acute graft-versus-host disease after allogeneic blood stem cell transplantation. Blood. 1999;94(4):1465–70.
Martin PJ, McDonald GB, Sanders JE, Anasetti C, Appelbaum FR, Deeg HJ, et al. Increasingly frequent diagnosis of acute gastrointestinal graft-versus-host disease after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2004;10(5):320–7.
Hill GR, Crawford JM, Cooke KR, Brinson YS, Pan L, Ferrara JL. Total body irradiation and acute graft-versus-host disease: the role of gastrointestinal damage and inflammatory cytokines. Blood. 1997;90(8):3204–13.
Hill GR, Ferrara JL. The primacy of the gastrointestinal tract as a target organ of acute graft-versus-host disease: rationale for the use of cytokine shields in allogeneic bone marrow transplantation. Blood. 2000;95(9):2754–9.
Socie G, Mary JY, Lemann M, Daneshpouy M, Guardiola P, Meignin V, et al. Prognostic value of apoptotic cells and infiltrating neutrophils in graft-versus-host disease of the gastrointestinal tract in humans: TNF and Fas expression. Blood. 2004;103(1):50–7.
Ferrara JL, Levine JE, Reddy P, Holler E. Graft-versus-host disease. Lancet. 2009;373(9674):1550–61.
Griffith LM, Pavletic SZ, Lee SJ, Martin PJ, Schultz KR, Vogelsang GB. Chronic graft-versus-host disease—implementation of the National Institutes of Health consensus criteria for clinical trials. Biol Blood Marrow Transplant. 2008;14(4):379–84.
Chirletti P, Caronna R, Arcese W, Iori AP, Calcaterra D, Cartoni C, et al. Gastrointestinal emergencies in patients with acute intestinal graft-versus-host disease. Leuk Lymphoma. 1998;29(1–2):129–37.
Deeg HJ, Antin JH. The clinical spectrum of acute graft-versus-host disease. Semin Hematol. 2006;43(1):24–31.
Stelljes M, Hermann S, Albring J, Kohler G, Loffler M, Franzius C, et al. Clinical molecular imaging in intestinal graft-versus-host disease: mapping of disease activity, prediction, and monitoring of treatment efficiency by positron emission tomography. Blood. 2008;111(5):2909–18.
Thompson B, Salzman D, Steinhauer J, Lazenby AJ, Wilcox CM. Prospective endoscopic evaluation for gastrointestinal graft-versus-host disease: determination of the best diagnostic approach. Bone Marrow Transplant. 2006;38(5):371–6.
Velasco-Guardado A, Lopez-Corral L, Alvarez-Delgado A, Flores-Corral T, Geijo-Martinez F, Caballero-Barrigon D, et al. Endoscopic evaluation and histological findings in graft-versus-host disease. Rev Esp Enferm Dig. 2012;104(6):310–4.
Sultan M, Ramprasad J, Jensen MK, Margolis D, Werlin S. Endoscopic diagnosis of pediatric acute gastrointestinal graft-versus-host disease. J Pediatr Gastroenterol Nutr. 2012;55(4):417–20.
Ponec RJ, Hackman RC, McDonald GB. Endoscopic and histologic diagnosis of intestinal graft-versus-host disease after marrow transplantation. Gastrointest Endosc. 1999;49(5):612–21.
Onozawa M, Yonezumi M, Kawarazaki M, Izumiyama K, Chiba K, Kondo T, et al. Usefulness of magnifying endoscopic evaluation of the terminal ileum for a patient with graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Ann Hematol. 2005;84(2):106–9.
Cruz-Correa M, Poonawala A, Abraham SC, Wu TT, Zahurak M, Vogelsang G, et al. Endoscopic findings predict the histologic diagnosis in gastrointestinal graft-versus-host disease. Endoscopy. 2002;34(10):808–13.
Xu CF, Zhu LX, Xu XM, Chen WC, Wu DP. Endoscopic diagnosis of gastrointestinal graft-versus-host disease. World J Gastroenterol. 2008;14(14):2262–7.
Washington K, Bentley RC, Green A, Olson J, Treem WR, Krigman HR. Gastric graft-versus-host disease: a blinded histologic study. Am J Surg Pathol. 1997;21(9):1037–46.
Xin W, Greenson JK. The clinical significance of focally enhanced gastritis. Am J Surg Pathol. 2004;28(10):1347–51.
Sale GE, Shulman HM, McDonald GB, Thomas ED. Gastrointestinal graft-versus-host disease in man. A clinicopathologic study of the rectal biopsy. Am J Surg Pathol. 1979;3(4):291–9.
Nguyen T, Park JY, Scudiere JR, Montgomery E. Mycophenolic acid (Cellcept and Myofortic) induced injury of the upper GI tract. Am J Surg Pathol. 2009;33(9):1355–63.
Tzankov A, Stifter G, Tschorner I, Gastl G, Mikuz G. Detection of apoptoses in gastro-intestinal graft-versus-host disease and cytomegalovirus colitis by a commercially available antibody against caspase-3. Pathol Res Pract. 2003;199(5):337–40.
Lee FD. Drug-related pathological lesions of the intestinal tract. Histopathology. 1994;25(4):303–8.
Berrebi D, Sautet A, Flejou JF, Dauge MC, Peuchmaur M, Potet F. Ticlopidine induced colitis: a histopathological study including apoptosis. J Clin Pathol. 1998;51(4):280–3.
Yeo M, Kim DK, Kim YB, Oh TY, Lee JE, Cho SW, et al. Selective induction of apoptosis with proton pump inhibitor in gastric cancer cells. Clin Cancer Res. 2004;10(24):8687–96.
Driman DK, Preiksaitis HG. Colorectal inflammation and increased cell proliferation associated with oral sodium phosphate bowel preparation solution. Hum Pathol. 1998;29(9):972–8.
Parfitt JR, Jayakumar S, Driman DK. Mycophenolate mofetil-related gastrointestinal mucosal injury: variable injury patterns, including graft-versus-host disease-like changes. Am J Surg Pathol. 2008;32(9):1367–72.
Lee FD. Importance of apoptosis in the histopathology of drug related lesions in the large intestine. J Clin Pathol. 1993;46(2):118–22.
Moss SF, Attia L, Scholes JV, Walters JR, Holt PR. Increased small intestinal apoptosis in coeliac disease. Gut. 1996;39(6):811–7.
Cho BS, Yahng SA, Kim JH, Yoon JH, Shin SH, Lee SE, et al. Impact of cytomegalovirus gastrointestinal disease on the clinical outcomes in patients with gastrointestinal graft-versus-host disease in the era of preemptive therapy. Ann Hematol. 2013;92(4):497–504.
McCole DF, Eckmann L, Laurent F, Kagnoff MF. Intestinal epithelial cell apoptosis following Cryptosporidium parvum infection. Infect Immun. 2000;68(3):1710–3.
Brito GA, Fujji J, Carneiro-Filho BA, Lima AA, Obrig T, Guerrant RL. Mechanism of Clostridium difficile toxin A-induced apoptosis in T84 cells. J Infect Dis. 2002;186(10):1438–47.
Moss SF, Calam J, Agarwal B, Wang S, Holt PR. Induction of gastric epithelial apoptosis by Helicobacter pylori. Gut. 1996;38(4):498–501.
Jones NL, Shannon PT, Cutz E, Yeger H, Sherman PM. Increase in proliferation and apoptosis of gastric epithelial cells early in the natural history of Helicobacter pylori infection. Am J Pathol. 1997;151(6):1695–703.
Velasco Guardado A, Lopez-Corral L, Perez-Simon JA, Caballero-Velazquez T, Flores Corral T, Caballero Barrigon D, et al. Helicobacter pylori infection and graft-versus-host disease. Biol Blood Marrow Transplant. 2011;17(5):765–9.
Pavletic S, Vogelsang G. Chronic graft-versus-host disease: clinical manifestations and therapy. In: Thomas ED, Blume KG, Forman SJ, Appelbaum FR, editors. Thomas’ hematopoietic cell transplantation. 3rd ed. Malden, MA: Blackwell; 2004. p. 1304–24.
Brook OR, Mullan CP, Mendiratta-Lala M, Joyce R, Sheiman R, Brook A, et al. Pancreatic atrophy in patients with chronic graft-versus-host disease. Abdom Imaging. 2014;39(2):342–7.
Vigorito AC, Campregher PV, Storer BE, Carpenter PA, Moravec CK, Kiem HP, et al. Evaluation of NIH consensus criteria for classification of late acute and chronic GVHD. Blood. 2009;114(3):702–8.
Shulman HM, Sharma P, Amos D, Fenster LF, McDonald GB. A coded histologic study of hepatic graft-versus-host disease after human bone marrow transplantation. Hepatology. 1988;8(3):463–70.
McDonald GB, Shulman HM, Wolford JL, Spencer GD. Liver disease after human marrow transplantation. Semin Liver Dis. 1987;7(3):210–29.
Jacobsohn DA, Montross S, Anders V, Vogelsang GB. Clinical importance of confirming or excluding the diagnosis of chronic graft-versus-host disease. Bone Marrow Transplant. 2001;28(11):1047–51.
Choi SW, Levine JE, Ferrara JL. Pathogenesis and management of graft-versus-host disease. Immunol Allergy Clin North Am. 2010;30(1):75–101.
Ratanatharathorn V, Nash RA, Przepiorka D, Devine SM, Klein JL, Weisdorf D, et al. Phase III study comparing methotrexate and tacrolimus (prograf, FK506) with methotrexate and cyclosporine for graft-versus-host disease prophylaxis after HLA-identical sibling bone marrow transplantation. Blood. 1998;92(7):2303–14.
McDonald GB, Shulman HM, Sullivan KM, Spencer GD. Intestinal and hepatic complications of human bone marrow transplantation. Part II. Gastroenterology. 1986;90(3):770–84.
McDonald GB, Shulman HM, Sullivan KM, Spencer GD. Intestinal and hepatic complications of human bone marrow transplantation. Part I. Gastroenterology. 1986;90(2):460–77.
Sloane JP, Norton J. The pathology of bone marrow transplantation. Histopathology. 1993;22(3):201–9.
Strasser SI, Shulman HM, Flowers ME, Reddy R, Margolis DA, Prumbaum M, et al. Chronic graft-versus-host disease of the liver: presentation as an acute hepatitis. Hepatology. 2000;32(6):1265–71.
Quaranta S, Shulman H, Ahmed A, Shoenfeld Y, Peter J, McDonald GB, et al. Autoantibodies in human chronic graft-versus-host disease after hematopoietic cell transplantation. Clin Immunol. 1999;91(1):106–16.
Strasser SI, McDonald GB. Hepatitis viruses and hematopoietic cell transplantation: a guide to patient and donor management. Blood. 1999;93(4):1127–36.
Strasser SI, Myerson D, Spurgeon CL, Sullivan KM, Storer B, Schoch HG, et al. Hepatitis C virus infection and bone marrow transplantation: a cohort study with 10-year follow-up. Hepatology. 1999;29(6):1893–9.
Strasser SI, Sullivan KM, Myerson D, Spurgeon CL, Storer B, Schoch HG, et al. Cirrhosis of the liver in long-term marrow transplant survivors. Blood. 1999;93(10):3259–66.
Duarte RF, Delgado J, Shaw BE, Wrench DJ, Ethell M, Patch D, et al. Histologic features of the liver biopsy predict the clinical outcome for patients with graft-versus-host disease of the liver. Biol Blood Marrow Transplant. 2005;11(10):805–13.
Lunz 3rd JG, Contrucci S, Ruppert K, Murase N, Fung JJ, Starzl TE, et al. Replicative senescence of biliary epithelial cells precedes bile duct loss in chronic liver allograft rejection: increased expression of p21(WAF1/Cip1) as a disease marker and the influence of immunosuppressive drugs. Am J Pathol. 2001;158(4):1379–90.
Malard F, Bossard C, Brissot E, Chevallier P, Guillaume T, Delaunay J, et al. Increased Th17/Treg ratio in chronic liver GVHD. Bone Marrow Transplant. 2014;49(4):539–44.
Ali SA, Shah V, McKinnon R, Van Harn M, Janakiraman N. Frequent expression of C4d in hepatic graft-versus-host disease: potential clue for diagnosis and distinguishing acute and chronic form. Transpl Immunol. 2010;23(1–2):77–80.
List AF, Spier C, Greer J, Wolff S, Hutter J, Dorr R, et al. Phase I/II trial of cyclosporine as a chemotherapy-resistance modifier in acute leukemia. J Clin Oncol. 1993;11(9):1652–60.
Chand N, Sanyal AJ. Sepsis-induced cholestasis. Hepatology. 2007;45(1):230–41.
Ozyilmaz E, Aydogdu M, Sucak G, Aki SZ, Ozkurt ZN, Yegin ZA, et al. Risk factors for fungal pulmonary infections in hematopoietic stem cell transplantation recipients: the role of iron overload. Bone Marrow Transplant. 2010;45(10):1528–33.
Sucak GT, Yegin ZA, Ozkurt ZN, Aki SZ, Yagci M. Iron overload: predictor of adverse outcome in hematopoietic stem cell transplantation. Transplant Proc. 2010;42(5):1841–8.
Pullarkat V. Iron overload in patients undergoing hematopoietic stem cell transplantation. Adv Hematol. 2010;2010:12.
Scheimberg IB, Pollock DJ, Collins PW, Doran HM, Newland AC, van der Walt JD. Pathology of the liver in leukaemia and lymphoma. A study of 110 autopsies. Histopathology. 1995;26(4):311–21.
Majhail NS, Lazarus HM, Burns LJ. Iron overload in hematopoietic cell transplantation. Bone Marrow Transplant. 2008;41(12):997–1003.
Mahendra P, Hood IM, Bass G, Patterson P, Marcus RE. Severe hemosiderosis post allogenic bone marrow transplantation. Hematol Oncol. 1996;14(1):33–5.
Harrison P, Neilson JR, Marwah SS, Madden L, Bareford D, Milligan DW. Role of non-transferrin bound iron in iron overload and liver dysfunction in long term survivors of acute leukaemia and bone marrow transplantation. J Clin Pathol. 1996;49(10):853–6.
Cross CE, Halliwell B, Borish ET, Pryor WA, Ames BN, Saul RL, et al. Oxygen radicals and human disease. Ann Intern Med. 1987;107(4):526–45.
Armand P, Kim HT, Virtanen JM, Parkkola RK, Itala-Remes MA, Majhail NS, et al. Iron overload in allogeneic hematopoietic cell transplantation outcome: a meta-analysis. Biol Blood Marrow Transplant. 2014;20(8):1248–51.
Ali S, Pimentel JD, Munoz J, Shah V, McKinnon R, Divine G, et al. Iron overload in allogeneic hematopoietic stem cell transplant recipients. Arch Pathol Lab Med. 2012;136(5):532–8.
Brissot P, Bourel M, Herry D, Verger JP, Messner M, Beaumont C, et al. Assessment of liver iron content in 271 patients: a reevaluation of direct and indirect methods. Gastroenterology. 1981;80(3):557–65.
Deugnier Y, Turlin B. Pathology of hepatic iron overload. World J Gastroenterol. 2007;13(35):4755–60.
Deugnier YM, Turlin B, Powell LW, Summers KM, Moirand R, Fletcher L, et al. Differentiation between heterozygotes and homozygotes in genetic hemochromatosis by means of a histological hepatic iron index: a study of 192 cases. Hepatology. 1993;17(1):30–4.
Majhail NS, DeFor T, Lazarus HM, Burns LJ. High prevalence of iron overload in adult allogeneic hematopoietic cell transplant survivors. Biol Blood Marrow Transplant. 2008;14(7):790–4.
Majhail NS, DeFor TE, Lazarus HM, Burns LJ. Iron-overload after autologous hematopoietic cell transplantation. Leuk Res. 2009;33(4):578–9.
DeLeve LD, McCuskey RS, Wang X, Hu L, McCuskey MK, Epstein RB, et al. Characterization of a reproducible rat model of hepatic veno-occlusive disease. Hepatology. 1999;29(6):1779–91.
Bras G, Jelliffe DB, Stuart KL. Veno-occlusive disease of liver with nonportal type of cirrhosis, occurring in Jamaica. AMA Arch Pathol. 1954;57(4):285–300.
McDonald GB, Hinds MS, Fisher LD, Schoch HG, Wolford JL, Banaji M, et al. Veno-occlusive disease of the liver and multiorgan failure after bone marrow transplantation: a cohort study of 355 patients. Ann Intern Med. 1993;118(4):255–67.
Shulman HM, McDonald GB, Matthews D, Doney KC, Kopecky KJ, Gauvreau JM, et al. An analysis of hepatic venocclusive disease and centrilobular hepatic degeneration following bone marrow transplantation. Gastroenterology. 1980;79(6):1178–91.
Carreras E, Bertz H, Arcese W, Vernant JP, Tomas JF, Hagglund H, et al. Incidence and outcome of hepatic veno-occlusive disease after blood or marrow transplantation: a prospective cohort study of the European Group for Blood and Marrow Transplantation. European Group for Blood and Marrow Transplantation Chronic Leukemia Working Party. Blood. 1998;92(10):3599–604.
Coppell JA, Richardson PG, Soiffer R, Martin PL, Kernan NA, Chen A, et al. Hepatic veno-occlusive disease following stem cell transplantation: incidence, clinical course, and outcome. Biol Blood Marrow Transplant. 2010;16(2):157–68.
McDonald GB. Hepatobiliary complications of hematopoietic cell transplantation, 40 years on. Hepatology. 2010;51(4):1450–60.
Dignan FL, Wynn RF, Hadzic N, Karani J, Quaglia A, Pagliuca A, et al. BCSH/BSBMT guideline: diagnosis and management of veno-occlusive disease (sinusoidal obstruction syndrome) following haematopoietic stem cell transplantation. Br J Haematol. 2013;163(4):444–57.
Lee JL, Gooley T, Bensinger W, Schiffman K, McDonald GB. Veno-occlusive disease of the liver after busulfan, melphalan, and thiotepa conditioning therapy: incidence, risk factors, and outcome. Biol Blood Marrow Transplant. 1999;5(5):306–15.
Chao N. How I, treat sinusoidal obstruction syndrome. Blood. 2014;123(26):4023–6.
McDonald GB, Sharma P, Matthews DE, Shulman HM, Thomas ED. Venocclusive disease of the liver after bone marrow transplantation: diagnosis, incidence, and predisposing factors. Hepatology. 1984;4(1):116–22.
Shulman HM, Hinterberger W. Hepatic veno-occlusive disease liver toxicity syndrome after bone marrow transplantation. Bone Marrow Transplant. 1992;10(3):197–214.
Jones RJ, Lee KS, Beschorner WE, Vogel VG, Grochow LB, Braine HG, et al. Venoocclusive disease of the liver following bone marrow transplantation. Transplantation. 1987;44(6):778–83.
Carreras E, Granena A, Navasa M, Bruguera M, Marco V, Sierra J, et al. Transjugular liver biopsy in BMT. Bone Marrow Transplant. 1993;11(1):21–6.
Shulman HM, Gooley T, Dudley MD, Kofler T, Feldman R, Dwyer D, et al. Utility of transvenous liver biopsies and wedged hepatic venous pressure measurements in sixty marrow transplant recipients. Transplantation. 1995;59(7):1015–22.
Johnson DB, Savani BN. How can we reduce hepatic veno-occlusive disease-related deaths after allogeneic stem cell transplantation? Exp Hematol. 2012;40(7):513–7.
Kumar S, DeLeve LD, Kamath PS, Tefferi A. Hepatic veno-occlusive disease (sinusoidal obstruction syndrome) after hematopoietic stem cell transplantation. Mayo Clin Proc. 2003;78(5):589–98.
Helmy A. Review article: updates in the pathogenesis and therapy of hepatic sinusoidal obstruction syndrome. Aliment Pharmacol Ther. 2006;23(1):11–25.
Crawford JM. Vascular disorders of the liver. Clin Liver Dis. 2010;14(4):635–50.
Narita M, Oussoultzoglou E, Chenard MP, Fuchshuber P, Rather M, Rosso E, et al. Liver injury due to chemotherapy-induced sinusoidal obstruction syndrome is associated with sinusoidal capillarization. Ann Surg Oncol. 2012;19(7):2230–7.
Schaffner F, Poper H. Capillarization of hepatic sinusoids in man. Gastroenterology. 1963;44:239–42.
Wanless IR. Micronodular transformation (nodular regenerative hyperplasia) of the liver: a report of 64 cases among 2,500 autopsies and a new classification of benign hepatocellular nodules. Hepatology. 1990;11(5):787–97.
Reshamwala PA, Kleiner DE, Heller T. Nodular regenerative hyperplasia: not all nodules are created equal. Hepatology. 2006;44(1):7–14.
Bacigalupo A, Chien J, Barisione G, Pavletic S. Late pulmonary complications after allogeneic hematopoietic stem cell transplantation: diagnosis, monitoring, prevention, and treatment. Semin Hematol. 2012;49(1):15–24.
Bunte MC, Patnaik MM, Pritzker MR, Burns LJ. Pulmonary veno-occlusive disease following hematopoietic stem cell transplantation: a rare model of endothelial dysfunction. Bone Marrow Transplant. 2008;41(8):677–86.
Au BK, Au MA, Chien JW. Bronchiolitis obliterans syndrome epidemiology after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2011;17(7):1072–8.
Chien JW, Duncan S, Williams KM, Pavletic SZ. Bronchiolitis obliterans syndrome after allogeneic hematopoietic stem cell transplantation—an increasingly recognized manifestation of chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2010;16(1 Suppl):S106–14.
Cooke KR, Yanik GA. Lung injury following hematopoietic cell transplantation. In: Appelbaum FR, Forman SJ, Negrin RS, Blume KG, editors. Thomas' hematopoietic cell transplantation. Oxford: Wiley-Blackwell; 2009. p. 1456–72.
Freudenberger TD, Madtes DK, Curtis JR, Cummings P, Storer BE, Hackman RC. Association between acute and chronic graft-versus-host disease and bronchiolitis obliterans organizing pneumonia in recipients of hematopoietic stem cell transplants. Blood. 2003;102(10):3822–8.
Holland HK, Wingard JR, Beschorner WE, Saral R, Santos GW. Bronchiolitis obliterans in bone-marrow transplantation and its relationship to chronic graft-v-host disease and low serum IgG. Blood. 1988;72(2):621–7.
Perreault C, Cousineau S, D’Angelo G, Gyger M, Nepveu F, Boileau J, et al. Lymphoid interstitial pneumonia after allogeneic bone marrow transplantation. A possible manifestation of chronic graft-versus-host disease. Cancer. 1985;55(1):1–9.
Soubani AO, Uberti JP. Bronchiolitis obliterans following haematopoietic stem cell transplantation. Eur Respir J. 2007;29(5):1007–19.
Tichelli A, Rovo A, Gratwohl A. Late pulmonary, cardiovascular, and renal complications after hematopoietic stem cell transplantation and recommended screening practices. Hematology Am Soc Hematol Educ Program. 2008;125–133
Washington K, Jagasia M. Pathology of graft-versus-host disease in the gastrointestinal tract. Hum Pathol. 2009;40(7):909–17.
Arai S, Jagasia M, Storer B, Chai X, Pidala J, Cutler C, et al. Global and organ-specific chronic graft-versus-host disease severity according to the 2005 NIH Consensus Criteria. Blood. 2011;118(15):4242–9.
Ferrara JL, Deeg HJ. Graft-versus-host disease. N Engl J Med. 1991;324(10):667–74.
El-Sayed MH, El-Haddad A, Fahmy OA, Salama II, Mahmoud HK. Liver disease is a major cause of mortality following allogeneic bone-marrow transplantation. Eur J Gastroenterol Hepatol. 2004;16(12):1347–54.
Al Sobhi E, Zahrani Z, Zevallos E, Zuraiki A. Imatinib-induced immune hepatitis: case report and literature review. Hematology. 2007;12(1):49–53.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Maedler-Kron, C., Marcus, V.A., Michel, R.P. (2016). Hematopoietic Stem Cell Transplantation. In: Michel, R., Berry, G. (eds) Pathology of Transplantation. Springer, Cham. https://doi.org/10.1007/978-3-319-29683-8_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-29683-8_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-29681-4
Online ISBN: 978-3-319-29683-8
eBook Packages: MedicineMedicine (R0)