
Abstract
Infections remain a cause of significant morbidity and mortality following hematopoietic stem cell transplantation (HSCT). The conditioning regimen (chemotherapy, radiation therapy), mucosal damage, type of transplant, immune suppressive therapy, and graft-versus-host disease (GVHD) all predispose the HSCT recipient to infection. Abnormal B- and T-lymphocyte function results in impaired humoral and cellular immunity, respectively. Neutrophil function is impaired by the use of corticosteroids and other medications. Hypogammaglobulinemia and functional asplenia are common. The occurrence of infections in an individual patient varies according to the phase of the transplant process and reflects the type(s) of immune defect(s), underlying disease, endogenous host flora, exposure history, and pre-treatment infections.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others



Keywords
Infections remain a cause of significant morbidity and mortality following hematopoietic stem cell transplantation (HSCT). The conditioning regimen (chemotherapy, radiation therapy), mucosal damage, type of transplant, immune suppressive therapy, and graft-versus-host disease (GVHD) all predispose the HSCT recipient to infection. Abnormal B- and T-lymphocyte function results in impaired humoral and cellular immunity, respectively. Neutrophil function is impaired by the use of corticosteroids and other medications. Hypogammaglobulinemia and functional asplenia are common. The occurrence of infections in an individual patient varies according to the phase of the transplant process and reflects the type(s) of immune defect(s), underlying disease, endogenous host flora, exposure history, and pre-treatment infections.
1 Temporal Sequence of Infections
-
1.
First month post-transplant (pre-engraftment) (see Fig. 17.1):
Fig. 17.1 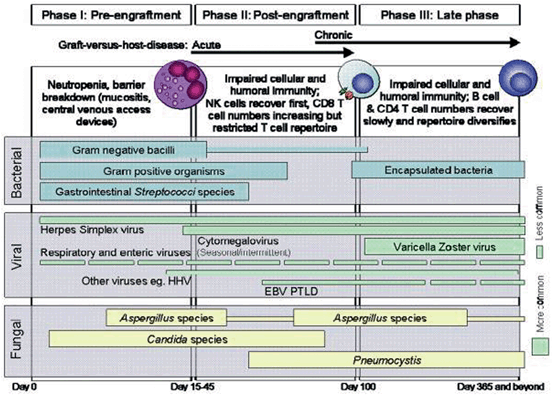
Phases of opportunistic infections among allogeneic HSCT recipients. EBV Epstein–Barr virus, HHV-6 human herpes virus 6, PTLD posttransplant lymphoproliferative disease . © Granted by Elsevier
-
a.
Viral infections: Herpes simplex virus (HSV), varicella zoster virus (VZV), community respiratory viruses, enteric viruses, human herpes virus-6 (HHV-6), etc.
-
b.
Bacterial infections: Gram-positive (Staphylococcus epidermidis, Staphylococcus aureus, Streptococcus species, Enterococcus species) and gram-negative organisms (Klebsiella species, Pseudomonas aeruginosa, Escherichia coli), with resultant bacteremias as well as sinopulmonary, perirectal, gastrointestinal, and skin/soft tissue infections
-
c.
Fungal infections: Predominantly Candida and Aspergillus species
-
a.
-
2.
One to four months post-transplant (early post-engraftment):
-
a.
Viral infections: Cytomegalovirus (CMV), HSV, VZV, community respiratory and enteric viruses, BK virus, and HHV-6, which can cause infection of the sinopulmonary, central nervous system, gastrointestinal, hepatic, and urogenital systems, depending on the causative organism
-
b.
Bacterial infections: Gram-positive and Gram-negative organisms, primarily arising from/involving the sinopulmonary system, the gastrointestinal tract, and skin/soft tissue
-
c.
Fungal infections: Candida, Aspergillus, and Cryptococcus species, Mucorales, reactivation of endemic fungi, typically involving the sinopulmonary, central nervous system, liver, spleen, mouth and/or skin/soft tissue; Pneumocystis jirovecii pneumonia (PCP) in patients on suboptimal PCP prophylaxis
-
d.
Protozoal infections: Toxoplasma gondii, which can affect the central nervous system or present in a disseminated fashion
-
a.
-
3.
Four to twelve months post-transplant (late post-engraftment):
-
a.
Viral infections: VZV, community-acquired respiratory and enteric infections, and CMV infection in patients with GVHD and prior history of early posttransplant CMV reactivation/infection
-
b.
Bacterial infections: Encapsulated organisms (e.g., Streptococcus pneumoniae, Haemophilus influenzae, etc.)
-
c.
Fungal infections: Both yeasts and molds (e.g., Candida, Aspergillus, Cryptococcus species, Mucorales, etc.), particularly in those patients who remain on immunosuppressive therapy, have GVHD and/or CMV infection; Pneumocystis in patients on suboptimal prophylaxis
-
d.
Protozoal infections: T. gondii, which can affect the central nervous system or present in a disseminated fashion
-
a.
-
4.
Greater than 12 months post-transplant:
-
a.
Viral infections: VZV, community-acquired respiratory and enteric infections, and CMV infection in patients with chronic GVHD and prior history of CMV reactivation/infection.
-
b.
Bacterial infections: Encapsulated organisms (e.g., S. pneumoniae, H. influenzae, etc.).
-
c.
Fungal infections: Both yeasts and molds, particularly in those patients who remain on immunosuppressive therapy have GVHD and/or CMV infection.
-
d.
Protozoal infections can occur late as well, again primarily in patients who remain on immunosuppressive therapy.
-
a.

2 Empiric Antimicrobial Therapy and Evaluation of Neutropenic Fever
-
1.
For the first neutropenic fever (T ≥ 38 °C):
-
a.
Comprehensive fever workup to include the following, with additional testing as prompted by localizing signs/symptoms:
-
i.
Blood cultures from peripheral blood draw as well as all lumens of central catheter
-
ii.
Urine analysis (UA) dip/micro and urine culture
-
iii.
Sputum culture if patient is coughing and able to expectorate sample
-
iv.
Two-view chest X-ray (CXR) to evaluate for pulmonary infection
-
i.
-
b.
Discontinue prophylactic antibiotic and begin empiric parenteral antibiotic therapy as soon as possible, and always within 1 h of the initial fever:
-
i.
Empiric antibiotic therapy should be sufficiently broad, providing coverage of P. aeruginosa, Enterobacteriaceae, and oral streptococci.
-
ii.
Options include cefepime (fourth generation cephalosporin), piperacillin/tazobactam, or an antipseudomonal carbapenem (e g., meropenem or imipenem).
-
iii.
Consideration of the local institutional antibiogram as well as any patient-specific history of prior drug-resistant bacteria is critically important in determining the empiric antibiotic selection.
-
iv.
For septic/clinically unstable patients, consider broadening empiric regimen to include an aminoglycoside (e.g., tobramycin 5 mg/kg intravenous (IV) once daily, adjusted for renal function; once-daily dosing is preferred) as well as extended Gram-positive coverage (see Sect. 17.2).
-
i.
-
c.
For subsequent fevers:
-
i.
Frequent (at least daily), thorough clinical evaluation for signs or symptoms of new or emergent infection is imperative.
-
ii.
For T ≥ 38 °C, obtain blood cultures every 24 h for 2–3 days.
-
iii.
If fevers persist, blood cultures should be obtained in the context of clinical worsening and/or prior to any change to the empiric antibiotic regimen.
-
iv.
After initial defervescence with empiric antibiotics, recrudescent fever should be reevaluated with blood cultures and careful clinical assessment.
-
i.
-
d.
Adjustment of empiric antibiotic regimen:
-
i.
If cultures are positive or if source of infection is defined, ensure regimen is appropriate based on pathogen susceptibility pattern and/or source.
-
ii.
Discontinue empiric antibiotic therapy once absolute neutrophil count (ANC) > 500 cells/mm3 if patient remains afebrile and provided there is no documented infection.
-
i.
-
a.
-
2.
Indications for use of empiric extended Gram-positive coverage for neutropenic fever:
-
a.
Add vancomycin for any patient with:
-
i.
Sepsis/unstable clinical condition, particularly for those patients with an established history of methicillin-resistant S. aureus (MRSA) colonization or infection, and not previously known to be colonized/infected with vancomycin-resistant Enterococcus (VRE)
-
ii.
Documented infection with a Gram-positive organism while awaiting results of identification and susceptibility testing (e.g., Gram-positive cocci in clusters or pairs/chains for patient not previously known to be VRE colonized/infected)
-
iii.
Skin/soft tissue infection
-
iv.
Suspected/established catheter-related infection
-
v.
Healthcare-associated pneumonia, while awaiting data from respiratory culture
-
i.
-
b.
For patients known to be VRE colonized/infected, use daptomycin*as extended Gram-positive agent in the setting of sepsis and/or Gram-positive bacteremia (Gram-positive cocci in pairs and/or chains) while awaiting results of identification and susceptibility testing. Given the potential for myelosuppression with linezolid, daptomycin may be the preferred agent in this setting. *Note that daptomycin should not be used for the treatment of pneumonia, given its ineffectiveness in this setting; in the setting of possible/proven MRSA pneumonia, consider the use of vancomycin or linezolid.
-
c.
Blood as well as wound and sputum (when applicable) cultures should be obtained prior to adding vancomycin, daptomycin, or linezolid.
-
d.
Discontinue vancomycin, daptomycin, or linezolid after 72 h if no Gram-positive organisms have been cultured and patient has no evidence of shock, pneumonia, skin/soft tissue, or central venous catheter source, regardless of the presence or absence of fever.
-
a.
-
3.
Management of persistent neutropenic fevers ( > 72 h after initiation of empiric antibacterial therapy):
-
a.
Frequent (at least daily), thorough clinical evaluation for signs or symptoms of new or emergent infection is imperative.
-
b.
Strong consideration for computed tomography (CT) chest to evaluate for opportunistic pulmonary infection.
-
c.
Consideration to broadening empiric antifungal coverage:
-
i.
For patients who are receiving fluconazole prophylaxis, change therapy to voriconazole (see Chap. 10 for dosing guidelines), or to an echinocandin (e.g., micafungin 100 mg IV q24 h; caspofungin 70 mg IV ´ 1, then 50 mg IV q24 h; or anidulafungin 200 mg IV ´ 1, then 100 mg IV q24 h) if azole-resistant candidiasis is suspected/documented.
-
ii.
If voriconazole is contraindicated (e.g., liver enzyme abnormalities, drug–drug interactions), alternatives include:
-
Lipid-based amphotericin product (3–5 mg/kg IV q24 h)
-
Echinocandin, though recognizing the inferiority of these agents for prophylaxis/treatment of mold infections
-
i.
-
d.
For patients who are receiving posaconazole prophylaxis, obtain a CT chest, check serum galactomannan, and send a posaconazole level (if not yet sent). If CT chest is suspicious for fungal infection or if the serum galactomannan is positive, consider switch to alternative agent (e.g., voriconazole or lipid-based amphotericin product) and consult pulmonary service for consideration of diagnostic bronchoscopy and/or other diagnostic testing.
-
e.
If a patient is receiving voriconazole and there is clinical suspicion for invasive mold infection, entertain possibility of subtherapeutic voriconazole level or a voriconazole-resistant organism and consider empiric change to lipid-based amphotericin product (Ambisome® or Abelcet®). Voriconazole level should be checked prior to drug discontinuation (see Table 10.5).
-
a.
-
4.
Clinical criteria necessitating removal of central venous catheters include:
-
a.
Septic patient with suspected line source
-
b.
Tunnel tract infection
-
c.
Failure of response (persistent bacteremia with positive blood cultures after 48 h of appropriate antibiotic therapy)
-
a.
-
5.
Central venous catheters should be removed for positive blood cultures with the following organisms:
-
a.
S. aureus
-
b.
P. aeruginosa
-
c.
Candida species
-
d.
Multidrug resistant Gram-negative organism
-
e.
Mycobacterial species
-
a.
3 Treatment of Common Specific Infections in the HSCT Population
Of paramount importance in the treatment of infections in the HSCT recipient is the ability to obtain an accurate diagnosis . Symptoms of infection may be nonspecific or even attenuated in the heavily immune suppressed HSCT recipient. Diagnosis of infection may require culture of blood or other body fluid, molecular diagnostic testing (e.g., polymerase chain reaction, PCR), radiographic study, invasive diagnostics to obtain tissue or other material, as well as careful ongoing assessment for change in clinical status.
-
1.
Herpes zoster (VZV) infection:
-
a.
Rate of occurrence is decreased with acyclovir (or a related congener) prophylaxis.
-
b.
Typically occurs 4–5 months post-transplant (or later in allogeneic recipients) and may be associated with visceral or central nervous system disease.
-
c.
May be localized to a single dermatome or disseminated (see Fig. 17.2). A thorough skin examination is recommended to evaluate for disseminated disease.
Fig. 17.2 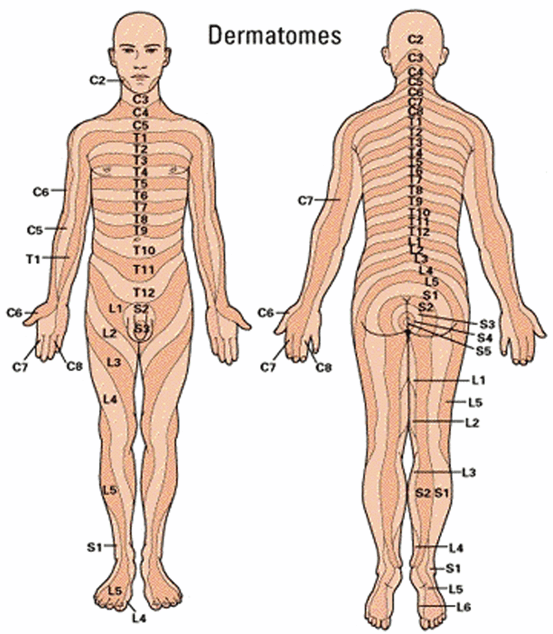
Dermatome map for the determination of the extent of herpes zoster infection
-
d.
Oral antiviral therapy with acyclovir 800 mg orally (po) five times daily (adjust dose for renal function) is standard of care for lesions confined to a single dermatome. Valacyclovir (Valtrex®) achieves better therapeutic plasma levels against VZV and may be used as preferred alternative to oral acyclovir if cost does not preclude use (dosed at 1000 mg po three times daily (TID), renal dose adjustment as indicted; see Table 10.2).
-
e.
For severe herpes zoster infections (> 1 dermatome, trigeminal nerve involvement, visceral or disseminated disease), patients should be hospitalized and treated with intravenous acyclovir (10 mg/kg IV every 8 h, renal dose adjustment as indicated; see Table 10.2) until lesions have completely crusted and no new lesions are evident, then transitioned to an oral compound (acyclovir or valacyclovir) to complete the treatment course. Monitor for acute kidney injury and encephalopathy as possible adverse effects of high-dose, parenteral acyclovir.
-
f.
Acyclovir-resistant VZV is relatively unusual; if suspected, a viral culture should be obtained for phenotypic resistance testing, with consideration to use foscarnet (40 mg/kg IV every 8 h, renal dose adjustment as indicated) if resistance is proven or in the context of life-threatening infection while awaiting results of resistance testing, along with consultation to the infectious diseases service.
-
a.

-
2.
HSV infection:
-
a.
Infection is largely related to reactivation in the post-transplant setting, and absent prophylaxis, occurs early (within the first month post-transplant) .
-
b.
Risk for infection is decreased with acyclovir (or a related congener) prophylaxis.
-
c.
HSV-1 infections most often present as severe mucositis and occasionally esophagitis, and less often with secondary infection of various organs in the context of viremia. HSV-2 infections are less common and typically affect the genital/perineal/buttocks region.
-
d.
For non-severe infection limited to the mucous membranes, oral antiviral therapy is usually adequate: acyclovir 400 mg po five times daily for approximately 7 days. If unable to tolerate oral medications, then use acyclovir 5 mg/kg IV every 8 h for approximately 7 days. Alternative therapy includes valacyclovir 500–1000 mg po two times daily (BID) for 5–10 days.
-
e.
In the case of suspected/proven visceral dissemination (e.g., encephalitis, hepatitis, pneumonitis), acyclovir 10 mg/kg IV every 8 h should be used as initial therapy, with duration typically 14–21 days, depending on clinical syndrome and clinical course.
-
f.
Select patients with frequently recurring outbreaks may require chronic antiviral suppression. Any of the following regimens is acceptable: acyclovir 400–800 mg po BID-TID or valacyclovir 500 mg po BID.
-
g.
Drug doses should be renally adjusted as indicated (see Table 10.2).
-
a.
-
3.
HHV-6 infection:
-
a.
Infection is almost universally related to reactivation and occurs in 30–50 % of transplant recipients in the early post-HSCT period (2–4 weeks).
-
b.
Viremia is often asymptomatic, though has been purported to be associated with a variety of nonspecific presentations (e.g., bone marrow suppression, delirium) . A causal association with encephalitis is supported by numerous case reports and case series.
-
c.
When encephalitis is suspected, HHV-6 PCR testing (cerebrospinal fluid (CSF), blood) should be performed; magnetic resonance imaging (MRI) of the brain may reveal abnormalities, often involving the temporal lobes.
-
d.
Treatment is controversial, but for established encephalitis, foscarnet or ganciclovir should be used in therapeutic doses. Treatment decisions should be made on a case-by-case basis in consultation with the infectious diseases service.
-
a.
-
4.
CMV infection:
-
a.
CMV infection can lead to end-organ disease in the HSCT recipient, manifesting as pneumonia, gastroenteritis, hepatitis , retinitis, encephalitis, etc .
-
b.
While detection of CMV by PCR in blood in the context of clinical signs/symptoms consistent with CMV disease is suggestive, more certain diagnosis typically requires diagnostic bronchoscopy and/or tissue biopsy. Furthermore, CMV PCR detection in blood is not fully sensitive for the detection of end-organ disease, particularly gastrointestinal disease . If CMV disease is suspected, tissue biopsy (for histopathology and viral culture) should be obtained when feasible.
-
c.
When CMV end-organ disease is suspected/proven, consultation with the infectious diseases service for patient-specific treatment recommendations is advised. First-line therapy for CMV disease is generally IV ganciclovir, with foscarnet reserved for cases with intolerance to ganciclovir (e.g., refractory cytopenias) or if ganciclovir resistance is suspected (e.g., if CMV viral load increases while on therapy for more than 2 weeks) or documented.
-
d.
Ganciclovir-resistant virus is an unusual occurrence in the HSCT population and most often occurs in patients who have had prolonged exposure to ganciclovir or valganciclovir.
-
e.
Treatment duration should be determined on a case-by-case basis, taking into consideration the severity of CMV disease and the immune status of the host. Typically, induction dosing should be given for at least 3 weeks until the CMV viral load is undetectable and symptoms of end-organ disease have resolved, with several weeks of maintenance IV ganciclovir or oral valganciclovir dosing thereafter (see Tables 10.3 and 10.4 for dosing).
-
f.
For CMV pneumonia, in addition to antiviral therapy, adjuvant immune globulin is generally recommended, largely based on small uncontrolled studies, though recent analyses have raised question about the value of this intervention:
-
i.
CMV-specific immune globulin has not been shown to be more effective than intravenous immunoglobulin (IVIG) and is more costly
-
ii.
The dose, frequency, and duration of IVIG for CMV pneumonia have not been well studied. Historically, IVIG dosing has been 500 mg/kg IV every other day for up to ten doses .
-
i.
-
a.
-
5.
Adenovirus and BK virus infections of the genitourinary (GU) tract:
-
a.
Both adenovirus and BK virus can result in hemorrhagic cystitis post-transplant.
-
b.
For patients who develop BK viral cystitis, the initial approach should consist of supportive care:
-
i.
Begin with antispasmotics (e.g., oxybutinin) or urinary tract analgesics (e.g., phenazopyridine).
-
ii.
Consider reducing immune suppression if feasible and begin continuous bladder irrigation if symptoms are not controlled with antispasmotics.
-
iii.
For patients who develop fulminant hemorrhagic cystitis, consider therapy with cidofovir; a variety of cidofovir dosing protocols have been reported in case reports and small case series (e.g., 1 mg/kg weekly to three times weekly without probenecid), with the goal of minimizing drug toxicity. Important adverse drug effects associated with cidofovir administration include nephrotoxicity as well as hematologic and ocular toxicity, and so careful monitoring is recommended in this setting.
-
iv.
Viral load quantification does not correlate with symptoms, and the clinical significance of the viral load is unknown.
-
i.
-
c.
Adenovirus infection can manifest as hemorrhagic cystitis, but is significantly more likely than BK virus to result in disseminated and potentially life-threatening disease:
-
i.
Adenovirus can affect the lungs, gastrointestinal tract, liver, GU system and/or the central nervous system.
-
ii.
Patients who have a positive culture or PCR for adenovirus from their urine should have blood sent for quantitative adenovirus PCR.
-
iii.
For adenovirus viremic patients and/or in the setting of fulminant hemorrhagic cystitis, strong consideration should be given to systemic treatment, with cidofovir 5 mg/kg IV once weekly for 2 weeks and then every other week or 1 mg/kg three times weekly (renal dose adjustment as indicated). If systemic or disseminated disease (e.g., disease outside the GU tract) is suspected, add probenecid 2 g po 3 h prior to cidofovir dose, then 1 g po at 2 and 8 h after dose.
-
i.
-
a.
-
6.
Community respiratory viral infections:
Community respiratory viral infections are common in HSCT recipients and can result in a spectrum of clinical findings, from upper respiratory tract infection (URI) to lower respiratory tract infection (LRTI), with often serious associated morbidity and even mortality. In addition to the “direct effects” of viral infection, there is increased risk for coinfection (e.g., with bacteria or fungi) in this setting, as well as risk for late airflow obstruction. While some of the community respiratory viruses have a distinct seasonality (e.g., influenza and respiratory syncytial virus, RSV), others occur year round (e.g., rhinovirus). Testing for community respiratory viral infections should be by molecular methods/multiplex PCR from nasopharyngeal sample or lower respiratory tract sample, as this methodology offers the highest sensitivity for diagnosis. Evaluation of suspected LRTI in patients with URI should include chest imaging (CXR and/or CT chest). Droplet and contact precautions should be initiated for hospitalized patients with either suspected or documented community respiratory viral infection, with the use of airborne precautions in the context of aerosol-generating procedures (e.g., bilevel positive airway pressure (BiPAP), suctioning, etc.); these precautions should continue until the patient is asymptomatic and repeat testing for viral infection is negative. If inhalational ribavirin is used, patient must be in a negative airflow room with airborne isolation.
-
a.
RSV:
-
i.
With RSV LRTI, patients should receive ribavirin 20 mg/ml (2 gm over 6 h every 8 h) × 7 days using a Viratek© small particle generator (SPAG-2) by face mask or endotracheal tube with adjuvant IVIG (500 mg/kg QOD × 5 doses).
-
ii.
Consider inhalational ribavirin therapy along with IVIG administration, as above, for any allogeneic recipient with an absolute lymphocyte count (ALC) < 300 cells/mm3 and/or steroid dose > 0.5 mg/kg/day (prednisone equivalent) presenting with RSV URI, with the goal of preventing progression to LRTI (acknowledging, however, the limited data on this approach).
-
iii.
There are limited data from case series and uncontrolled studies on the use of systemic (oral or intravenous) ribavirin for treatment of RSV infection.
-
i.
-
b.
Influenza A and B:
-
i.
Initiate therapy with an appropriate antiviral agent as soon as possible. The two main classes of drugs are neuraminidase inhibitors (e.g., osteltamivir and zanamavir) and M2 inhibitors (e.g., amantadine and rimantadine). Antiviral therapy for influenza will vary depending on the drug resistance patterns of circulating strains. Duration of therapy with neuraminidase inhibitors is typically 5 days, though a longer duration of therapy (> 10 days) may be considered in hospitalized patients with severe influenza infection.
-
ii.
Unvaccinated caregivers and patients who have been exposed to a case of documented influenza should be referred for chemoprophylaxis as soon as possible and within 48 h of the exposure. Drug resistance patterns of the circulating influenza strain should guide the choice of antiviral prophylaxis.
-
iii.
In the context of a significant community outbreak or transmission on the transplant unit/transplant clinic, policies for chemoprophylaxis should be discussed with the infectious diseases service/infection control and considered based on drug resistance patterns of the circulating influenza strain.
-
i.
-
c.
Adenovirus:
-
i.
Systemic cidofovir should be strongly considered in the context of invasive adenovirus infection. While data on optimal dosing of cidofovir are not available, the usual practice is to use 5 mg/kg IV once weekly (renal dose adjustment as indicated) for 2 weeks and then every other week in the setting of life-threatening or disseminated disease, along with probenecid 2 g po 3 h prior to cidofovir dose, then 1 g po at 2 and 8 h after dose. Important adverse drug effects associated with cidofovir administration include nephrotoxicity as well as hematologic and ocular toxicity, and so careful monitoring is recommended in this setting.
-
ii.
When possible, immune suppression should be reduced in the setting of life-threatening or disseminated adenovirus disease.
-
i.
-
a.
Parainfluenza virus 1–4:
-
i.
Care is supportive.
-
i.
-
b.
Rhinovirus:
-
i.
Care is supportive.
-
i.
-
c.
Human coronavirus:
-
i.
Care is supportive.
-
i.
-
d.
Metapneumovirus:
-
i.
Care is supportive.
-
i.
-
a.
-
7.
Epstein–Barr virus (EBV):
-
a.
EBV can result in post-transplant lymphoproliferative disease (PTLD) , manifesting as fever, adenopathy, and/or extranodal disease.
-
b.
Quantitative EBV PCR from blood and/or other body fluids (e.g., CSF) may support the diagnosis, though certain diagnosis requires tissue biopsy with immunohistochemistry.
-
c.
EBV viral load monitoring has been recommended by some for certain high-risk HSCT recipients, though the threshold for preemptive intervention is not clear. Patients who have received T cell depleted, cord blood, or haplo-identical stem cell products, or who have been exposed to Anti-thymocyte globulin (ATG) should be considered for preemptive monitoring with quantitative EBV viral load monitoring.
-
d.
First-line therapy for established CD20-positive PTLD is the administration of anti-CD20 monoclonal antibody (rituximab). Infusion of EBV-specific cytotoxic T-lymphocytes has been used with success in various study protocols, though this requires significant time for in vitro generation. There is little evidence at this time to support the contribution of antiviral therapy for this indication.
-
a.
-
8.
P. jirovecii pneumonia:
-
a.
Infection is rare in patients compliant with first-line PCP prophylaxis (e.g., trimethoprim–sulfamethoxazole), but breakthrough infections are possible, in particular in patients on other than first-line agents.
-
b.
Radiographic studies of the chest (CT and CXR) typically reveal diffuse interstitial infiltrates with ground glass appearance, although appearance can be quite varied.
-
c.
Diagnosis is typically by visualization of the organism in respiratory specimens under microscopy with staining of induced sputum or bronchoalveolar lavage (BAL) specimens. While still considered investigational, PCR of BAL fluid or induced sputum can increase the diagnostic yield over conventional microscopy. At times, lung biopsy is required to make the diagnosis.
-
d.
First-line treatment is trimethoprim–sulfamethoxazole 20 mg/kg/day (renal dose adjustment as indicated) of trimethoprim equivalent divided into 3–4 daily doses for 21 days.
-
e.
In the case of significant sulfa allergy or intolerance, alternative therapies include pentamidine 4 mg/kg/day IV (renal dose adjustment as indicated) for 21 days for severe disease, or clindamycin 450 mg po every 6 h with primaquine 15 mg (base) po daily for mild to moderate disease. Unique side effects associated with daily pentamidine therapy include hypotension, hypo- or hyperglycemia, pancreatitis and/or cardiac arrhythmias.
-
f.
In the context of moderate to severe disease, adjunctive corticosteroids should be considered, though recognizing that direct data for this intervention in the HIV-negative population is lacking:
-
i.
For patients with partial pressure of arterial oxygen (PaO2) < 70 mmHg and/or an alveolar–arterial oxygen gradient > 35 mmHg and/or hypoxemia on pulse oximetry, prednisone 40 mg po BID days 1–5, then 40 mg po daily on days 6–10, and then 20 mg po daily on days 11–21 can be considered in combination with antimicrobial therapy, if patient is not already receiving steroids in comparable dosages.
-
ii.
Patients who are on corticosteroids at the time of PCP diagnosis (e.g., for GVHD) should continue on their current regimen.
-
i.
-
a.
-
9.
T. gondii:
-
a.
The risk of toxoplasmosis following allogeneic HSCT depends on the seroprevalence in the population and on the conditioning regimen/degree of immune suppression. Seroprevalence studies indicate that 15–30 % of the US population has been previously infected with toxoplasmosis. Most toxoplasmosis in transplant HSCT recipients is reactivation disease.
-
b.
Toxoplasmosis often affects the central nervous system, but can also present as disseminated infection in HSCT recipients. A CT or an MRI of the brain may reveal focal mass lesion(s) or less commonly, diffuse encephalitis.
-
c.
If toxoplasmosis is suspected, a Toxoplasma PCR (CSF and/or blood) should be obtained. Tissue biopsy is often necessary to establish a certain diagnosis. Given the often nonspecific presentation of disseminated toxoplasmosis, a high index of suspicion for this diagnosis should be maintained, in particular in seropositive individuals.
-
d.
Treatment of established disease due to toxoplasmosis includes:
-
i.
Pyrimethamine 200 mg loading dose on day 1 then 50 mg po daily for patients < 60 kg or 75 mg po daily for patients > 60 kg
-
ii.
Sulfadiazine 1000 mg po four times daily for patients < 60 kg or 1500 mg po four times daily for patients > 60 kg
-
iii.
Folinic acid (10–25 mg po daily)
-
i.
-
e.
For patients who cannot tolerate sulfadiazine due to significant allergy or other contraindication, pyrimethamine and folinic acid plus clindamycin 600 mg po/IV four times daily (QID) or azithromycin 900–1200 mg po daily can be used.
-
f.
For patients who cannot tolerate pyrimethamine, sulfadiazine plus atovaquone 1500 mg po BID can be used, with salvage single-agent atovaquone for those unable to tolerate either sulfadiazine or pyrimethamine.
-
g.
Duration of therapy is typically 6 weeks followed by a course of suppressive therapy; however, this should be individualized based on clinical/radiographic response.
-
h.
Toxoplasma -seropositive transplant candidates/recipients should receive trimethoprim–sulfamethoxazole as PCP prophylaxis given the protection this provides against toxoplasmosis, presuming no significant allergy or other strict contraindication.
-
a.
-
10.
Clostridium difficile:
-
a.
C. difficile is a frequent cause of infectious diarrhea among hospitalized patients, particularly HSCT recipients, owing to often long hospitalizations, receipt of broad-spectrum antibiotics, and chemotherapy-induced gut disruption. The 1-year incidence of C. difficile following transplantation was 9.2 % in a recent large single-center study by Alonso et al. There is a suggestion of a strong interaction between gastrointestinal GVHD and C. difficile.
-
b.
C. difficile should be considered in all HSCT recipients with new/worsening diarrhea, with the caveat that diarrhea is common post-HSCT, with a broad differential diagnosis.
-
c.
Laboratory diagnosis of C. difficile is typically by demonstration of C. difficile toxin(s). A number of tests are available for broad clinical use: PCR for toxins A and B, enzyme immunoassay (EIA) for C. difficile toxins A and B, and EIA for C. difficile glutamate dehydrogenase (GDH, an enzyme produced by toxigenic and nontoxigenic C. difficile strains):
-
i.
PCR is more sensitive than EIA for toxins A and B, but has potential for false positive results.
-
ii.
EIA for GDH is sensitive but not specific
-
iii.
Some laboratories favor the use of tiered screening, with EIA for GDH the first test, then reflexing to EIA and/or PCR for toxins A and B if the GDH test is positive.
-
i.
-
d.
General principles of management include discontinuation or narrowing of antibacterials as able, fluid and electrolyte support, avoidance of antiperistaltic agents (e.g., loperimide, diphenoxylate/atropine), institution of appropriate infection control measures (contact precautions, strict hand hygiene with antibacterial soap and water, environmental cleaning with bleach, etc.), and antimicrobial therapy for C. difficile.
-
e.
The two main drugs used for treatment of C. difficile are oral metronidazole and oral vancomycin:
-
i.
Oral metronidazole (500 mg po/IV q 8 h) can be used for mild-to-moderate disease.
-
ii.
Oral vancomycin (125 mg po QID, and per rectum if ileus present) for severe disease.
-
iii.
With severe complicated C. difficile (ileus, megacolon, etc.), many providers use a combination of oral vancomycin (often at high dose, 500 mg QID) and intravenous metronidazole (500 mg IV q 8 h).
-
iv.
Duration of therapy is at least 14 days, and for patients who have an indication for other antibiotic therapy, providers often choose to extend the course of C. difficile-active therapy for a fixed period (e.g., 1 week) following the discontinuation of other antibacterials.
-
v.
The parameters are still being defined for the use of fidaxomicin, an antibiotic that is bactericidal against C. difficile and has been shown in a phase 3 study of patients with nonsevere C. difficile infection to have lower recurrence rates than vancomycin; cost remains a major barrier to the use of this agent.
-
i.
-
f.
Early surgical evaluation should be obtained for patients with severe complicated C. difficile, with colectomy an aggressive but potentially life-saving intervention.
-
g.
Recurrence after initial infection is not uncommon, affecting as many as 25 % of patients. Management of the first recurrence is guided by the same principles for first infection, with often prolonged/tapering courses of oral vancomycin for patients with multiple recurrences.
-
h.
For patients with multiple C. difficile recurrences, fecal microbiota transplantation can be considered, though with the caveats that this should be avoided in patients who are neutropenic, early post-transplant (e.g., < 3 months), on high-dose immune suppression or with active GVHD or other gut mucosal disruption. Experience is limited to case reports, with data on long-term outcomes/sequnce lacking at this time.
-
i.
“Secondary” prophylaxis, or the use of C. difficile-active therapy for patients with a history of C. difficile and subsequently requiring prophylactic or treatment antibiotics, is sometimes used by providers, though at this point there is no prospective data to support this practice. It should be noted that prolonged oral metronidazole is not advised, given risks for emergent drug toxicity (e.g., peripheral neuropathy , neutropenia) with protracted use.
-
a.
-
11.
Candidiasis:
Infections with Candida species can be classified as invasive (e.g., candidemia, hepatosplenic candidiasis, etc.) or superficial (e.g., mucosal). In the era of widespread use of azole prophylaxis, candidiasis occurs with relative infrequency in the HSCT population; however, fluconazole-resistant Candida species (C. krusei and C. glabrata) are of particular concern.
-
a.
Candidemia:
-
i.
An echinocandin (micafungin 100 mg IV daily or caspofungin 70 mg IV load then 50 mg IV daily, or anidulafungin 200 mg IV load then 100 mg IV daily) or an amphotericin B lipid-based product (dose 3–5 mg/kg IV daily) are recommended for empiric treatment of candidemia in neutropenic hosts while awaiting species-level identification which can guide further therapy. For patients who are not critically ill and without recent azole exposure, high-dose fluconazole (800 mg po/IV loading dose, followed by 400 mg po/IV daily) can be considered, or voriconazole (6 mg/kg po BID for two doses as load, followed by 4 mg/kg po BID) if mold coverage is also desired.
-
ii.
Once species-level identification +/- antifungal susceptibility data are available, antifungal therapy should be adjusted:
-
For infections due to C. albicans or C. parapsilosis, either fluconazole or an amphotericin-based product is acceptable, with fluconazole a less toxic and more convenient choice once the patient has stabilized.
-
For infections due to C. glabrata, an echinocandin is often preferred, though acknowledging recent reports of emergence of echinocandin resistance, with amphotericin-based therapy a less attractive option in light of the potential for toxicity.
-
For infections due to C. krusei, either an echinocandin, voriconazole, or a lipid formulation of amphotericin is generally acceptable.
-
iii.
Duration of therapy for candidemia is 2 weeks from documented clearance of blood cultures and until resolution of neutropenia, providing there is no concern for deep-seated foci or persistent positive blood cultures.
-
iv.
Removal of vascular catheter(s) should be strongly considered in the setting of candidemia, though acknowledging that gut translocation can be a source of infection.
-
v.
An ophthalmology consultation should be obtained to evaluate for Candida endophthalmitis. A CT of the abdomen should be considered to evaluate for hepatosplenic candidiasis (see Sect. 17.11.b) in the appropriate clinical setting.
-
vi.
With high-grade and persistent candidemia, an echocardiogram should be obtained to evaluate for endocarditis.
-
i.
-
b.
Chronic disseminated candidiasis:
-
i.
This syndrome, also referred to as hepatosplenic candidiasis, is most often seen during or soon after recovery from neutropenia.
-
ii.
C. albicans is most often the causative organism with other species seen far less often.
-
iii.
Presenting signs/symptoms are often vague with malaise, fever, and/or nonspecific gastrointestinal complaints.
-
iv.
Diagnosis is suggested by an elevation of the serum alkaline phosphatase and/or multiple hepatic hypodensities seen on abdominal CT. Blood cultures are often negative.
-
v.
Definitive diagnosis is established by liver biopsy which classically demonstrates multiple granulomas with visualization of yeast and hyphal elements on special stains. More often than not, culture of tissue from liver biopsy is negative, particularly if the patient has received antifungal therapy.
-
vi.
Molecular diagnostic studies (e.g., fungal PCR) can offer additional sensitivity and provide species-level information.
-
vii.
Treatment considerations include azole therapy (frequently fluconazole, as C. albicans is the most common species implicated in this setting), an echinocandin, or a lipid-based amphotericin product. The bulk of available data is with amphotericin B deoxycholate and fluconazole. Treatment decisions should be based on previous antifungal therapy and, when available, microbiologic data.
-
viii.
Duration of therapy is typically prolonged (many months) and is guided by clinical response and radiographic resolution or calcification.
-
i.
-
c.
Candida cystitis:
-
i.
Consider whether a urine culture with Candida species represents colonization or infection based on whether the patient is displaying signs and/or symptoms of urinary tract infection (UTI).
-
ii.
If the patient has an indwelling catheter, remove or, if it cannot be removed, exchange the catheter and repeat urine studies.
-
iii.
Treatment of candiduria is indicated in neutropenic hosts, whether symptomatic or asymptomatic.
-
iv.
Fluconazole 200 mg po/IV daily for 7–14 days is the treatment of choice for candidal cystitis due to fluconazole-sensitive organisms:
-
For treatment of cystitis due to fluconazole-resistant organisms (e.g., C. krusei and C. glabrata), amphotericin B deoxycholate can be used, either systemically (at very low doses) or by bladder irrigation. One should note that urinary tract drug levels of lipid formulations of amphotericin B are not high enough to provide adequate treatment.
-
Voriconazole is not an effective drug for candidal cystitis given that active drug is not excreted to the urine in a significant amount.
-
Although echinocandins achieve low concentrations in the urine, there is limited data describing successful use of these antifungal agents for treatment of renal parenchymal infections.
-
-
v.
In patients with recurrent or seemingly complicated Candida cystitis, a renal ultrasound should be performed to evaluate for a fungal mass which would entail systemic antifungal therapy as well as consideration of surgical approach.
-
i.
-
d.
Oropharyngeal candidiasis:
-
i.
Topical therapy with nystatin suspension 5–10 mL (100,000 units/mL) swish and spit/swallow QID or clotrimazole troches 10 mg dissolved in mouth 4–5 times per day is first line, with use of systemic therapy with an azole, an echinocandin, or a low-dose amphotericin B lipid-based product for moderate to severe disease.
-
i.
-
e.
Esophageal candidiasis:
-
i.
Fluconazole 200–400 mg po/IV daily for 14–21 days is first line in azole-inexperienced individuals:
-
In patients with significant antecedent azole exposure, for infection with culture-documented fluconazole-resistant Candida species, or for fluconazole-refractory disease, an echinocandin (e.g., micafungin 150 mg IV daily) or an extended spectrum azole (e.g., posaconazole 400 mg po BID (suspension) or voriconazole 200 mg po BID) can be used.
-
Low-dose amphotericin B lipid-based product is an alternative for patients refractory to other agents.
-
i.
-
f.
Vulvovaginal candidiasis:
-
i.
Fluconazole 100–200 mg po/IV daily for 7–10 days or topical antifungal treatment (e.g., clotrimazole, miconazole, or nystatin) for 7–10 days can be used.
-
ii.
If refractory or recurrent vulvovaginal candidiasis (> 4 symptomatic episodes within a year) occurs, cultures may help to guide antifungal therapy and consultation with the infectious diseases service should be considered.
-
i.
-
a.
-
12.
Invasive aspergillosis:
-
a.
Aspergillus fumigatus is the most common Aspergillus species implicated as a cause of infection in immunocompromised hosts, though other species can also result in invasive infection.
-
b.
Pulmonary infection is the most common presentation, with sinus disease and/or hematogenous dissemination with other organ involvement (e.g., central nervous system, sinuses, skin, etc.) seen on occasion.
-
c.
The key to successful management is early consideration of this process, with imaging and appropriate diagnostic evaluation, along with prompt initiation of antifungal therapy.
-
d.
Chest imaging can be suggestive in the appropriate context, but proven or probable diagnosis requires a mycologic diagnosis, either by culture or fungal biomarker.
-
e.
Diagnosis of pulmonary infection can often be established with use of Aspergillus galactomannan testing on bronchoalveolar lavage fluid. When a diagnosis cannot be obtained by less invasive means, surgical biopsy should be considered.
-
f.
Voriconazole is first-line therapy for invasive aspergillosis:
-
i.
Voriconazole trough levels should be measured early in any patient with proven or probable invasive aspergillosis, or with a poor response to treatment, possible side effects of therapy, suspicion of poor oral absorption, or complex drug–drug interactions (see Table 10.5 for dosing guidelines and trough targets).
-
i.
-
g.
If a significant increase in serum transaminase levels is noted while on voriconazole therapy (> 5 times the upper limit of normal), check a voriconazole level and consider change to a lipid-based amphotericin product or posaconazole (200 mg po QID x 1 week, then 400 mg po BID suspension) with careful monitoring. Posaconazole delayed-release tablets appear offer better oral bioavailability than suspension, with the convenience of once daily dosing after an initial load (300 mg po BID for 1 day, then 300 mg once daily); the tablet formulation and dosing schema has been studied and approved for prophylaxis, but is an approach that can be considered for treatment in patients refractory or intolerant of conventional therapy for invasive fungal infection (e.g., amphotericin product, voriconazole, etc.). If the voriconazole level is supratherapeutic, reintroduction at a lower dose, with close monitoring, can be considered after normalization of serum transaminases.
-
h.
Echinocandins are considered an inferior single-agent choice for management of invasive aspergillosis.
-
i.
Preliminary results from a phase 4 clinical trial of combination therapy (voriconazole + anidulafungin or placebo) for invasive aspergillosis showed a trend toward improved outcome but did not meet statistical significance.
-
j.
Reduction of immunosuppression is advised (especially taper or withdrawal of corticosteroids) when possible.
-
k.
The use of recombinant human growth factors such as filgrastim or sargramostim may be helpful in this population, primarily in the neutropenic patient. A prospective study to determine the utility of granulocyte transfusions in this setting is ongoing.
-
l.
Surgical resection should be considered when pulmonary lesions are in close proximity to the great vessels or pericardium, or in patients with persistent hemoptysis from a single cavitary lesion, pericardial infection or chest wall invasion.
-
m.
Patients with a history of invasive aspergillosis prior to transplant should receive at least 6 weeks of antifungal therapy and have a documented partial or complete response to therapy before proceeding to conditioning. Strong consideration should be made for nonmyeloablative conditioning in patients with history of invasive aspergillosis:
-
i.
Secondary prophylaxis with an Aspergillus-active azole antifungal (voriconazole or posaconazole) should be given to patients in the posttransplant setting.
-
ii.
If significant drug–drug interaction or drug toxicity limits azole use, a lipid-based amphotericin product or an echinocandin can be used as a second-line approach in this setting.
-
i.
-
a.
-
13.
Other fungal infections
While Aspergillus and Candida species are the most common fungal infections encountered in HSCT recipients, there are other fungi to consider in this patient population:
-
a.
Mucormycosis (or zygomycosis) is increasingly recognized in highly immune suppressed HSCT recipients:
-
i.
In addition to intensive immune suppressive regimens, iron overload and chelation with deferoxamine predispose patients to infection.
-
ii.
Clinical presentation may include angioinvasive infection of the lungs, skin, brain, and/or widespread visceral involvement in the setting of disseminated disease.
-
iii.
Diagnosis often requires tissue biopsy, though bronchoscopy with bronchoalveolar lavage can sometimes be informative in the setting of pulmonary infection.
-
iv.
Management of this infection should include antifungal therapy, reversal of underlying defects in host defense when possible including tapering of immune suppression and restoration of euglycemia, and surgical debridement where applicable.
-
v.
Liposomal amphotericin 5–7.5 mg/kg IV daily is first-line antifungal therapy. Posaconazole can be considered as salvage therapy for patients intolerant of first-line therapy or for secondary prophylaxis. Voriconazole does not have activity against mucormycosis.
-
vi.
Despite aggressive management of this infection, mortality rates remain very high. Consultation with the infectious diseases service is recommended.
-
i.
-
b.
Disseminated fusariosis can be seen in highly immunosuppressed HSCT recipients and is often characterized by cutaneous lesions and positive blood cultures, with or without visceral involvement:
-
i.
Antifungal susceptibility varies by species. Treatment of disseminated infection is with either voriconazole or liposomal amphotericin (indicated for Fusarium solani or F. verticillioides).
-
ii.
In addition to antifungal treatment, management should include surgical debridement when applicable and manuevers to improve host immune response. Growth factor support and/or granulocyte transfusions can be considered as adjuvants to care in persistently neutropenic individuals.
-
iii.
Prognosis for disseminated diseases is generally poor and is largely determined by the degree of immune suppression.
-
iv.
Consultation with the infectious diseases service is recommended.
-
i.
-
c.
Cryptococcosis is reported uncommonly in the HSCT population. This may well relate to widespread use of azole prophylaxis in this patient population:
-
i.
Cryptococcal infection may result in pulmonary, central nervous system, cutaneous, or widely disseminated infection.
-
ii.
Common diagnostic modalities include culture (from blood and/or other body fluids/tissue) and antigen-based testing (serum or CSF cryptococcal antigen). Diagnostic workup should include lumbar puncture when this entity is considered.
-
iii.
Management is with liposomal amphotericin or fluconazole, along with serial lumbar punctures for management of elevated intracranial pressure in the context of cryptococcal meningitis.
-
iv.
Although a mainstay of combination therapy with an amphotericin B formulation for HIV-positive patients with cryptococcal meningitis, concurrent use of flucytosine is often poorly tolerated in HSCT recipients given the potential for marrow suppression.
-
v.
Consultation with the infectious diseases service is recommended.
-
i.
-
a.
Bibliography
Alonso CD, Treadway SB, Hanna DB, et al. Epidemiology and outcomes of Clostridium difficile infection in hematopoietic stem cell transplant recipients Clin Infect Dis. 2012;54:1053–63.
Bobak M, Arfons LM, Cregar RJ, Lazarus HM. Clostridium difficile-associated disease in human stem cell transplant recipients: coming epidemic or false alarm. Bone Marrow Transplant. 2008;42:705–13.
Boeckh M. The challenge of respiratory virus infections in hematopoietic cell transplant recipients. Br J Haematol. 2008;143:455–67.
Boeckh M.. Complications, diagnosis, management and prevention of CMV infections: current and future. Hematology. 2011;2011:305–9.
Cesaro S, Hirsch HH, Faraci M, et al. Cidofovir for BK virus-associated hemorrhagic cystitis: a retrospective study. Clin Infect Dis. 2009;49:233–40.
Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31:431–55.
Emanuel D, Cunningham I, Jules-Elysee K, et al. Cytomegalovirus pneumonia after bone marrow transplantation successfully treated with the combination of ganciclovir and high-dose intravenous immune globulin. Ann Intern Med. 1988;109:777–82.
Foo H, Gottlieb T. Lack of cross-hepatotoxicity between voriconazole and posaconazole. Clin Infect Dis. 2007;45:803–5.
Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guidelines for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis. 2011;15:e56–93.
Fricker-Hidalgo H, Bulabois CE, Brenier-Pinchart MP, et al. Diagnosis of toxoplasmosis after allogeneic stem cell transplantation: results of DNA detection and serological techniques. Clin Infect Dis. 2009;48:e9–15.
Ison MG. Adenovirus infections in transplant recipients. Clin Infect Dis. 2006;43:331–9.
Lee WM, Grindle K, Pappas T, et al. High-throughput, sensitive, and accurate multiplex PCR microsphere flow cytometry system for large-scale comprehensive detection of respiratory viruses. J Clin Microbiol. 2007;45:2626–34.
Jones JL, Kruszon-Moran D, Wilson M, McQuillan G, Navin T, McAuley JB. Toxoplasma gondii infection in the United States: seroprevalence and risk factors. Am J Epidemiol. 2001;154:357–65.
Kontoyiannis DP, Marr KA, Park BJ, et al. Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001–2006: overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) database. Clin Infect Dis. 2010;50:1091–100.
Ljungman P, de la Camara R, Milpied N, et al. Randomized study of valacyclovir as prophylaxis against cytomegalo virus reactivation in recipients of allogeneic bone marrow transplants. Blood. 2002;99:3050–6.
Ljungman P, de la Camara R, Cordonnier C, et al. Management of CMV, HHV-6, HHV-7 and Kaposi-sarcoma herpes virus (HHV-8) infections in patients with hematological malignancies and after SCT. Bone Marrow Transplant. 2008;42:227–40.
Marcelin JR, Wilson JW, Ratonale RR; Mayo Clinic Hemaotology/Oncology and Transplant Infectious Diseases Services. Oral ribavirin therapy for respiratory syncitial virus infections in moderately to severely immunocompromised patients. Transpl Infect Dis. 2014;16:242–50.
Martino R, Parody R, Fukuda T, et al. Impact of the intensity of the pretransplantation conditioning regimen in patients with prior invasive aspergillosis undergoing allogeneic hematopoietic stem cell transplantation: a retrospective survey of the Infectious Diseases Working Party of the European Group for Blood and Marrow Transplantation. Blood. 2006;108:2928–36.
Meers S, Lagrou K, Theunissen K, et al. Myeloablative conditioning predisposes patients for Toxoplasma gondii reactivation after allogeneic stem cell transplantation. Clin Infect Dis. 2010;50:1127–34.
Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis. 2009;49:1–45.
Musher B, Fredricks D, Leisenring W, Balajee SA, Smith C, Marr KA. Aspergillus galactomannan enzyme immunoassay and quantitative PCR for diagnosis of invasive aspergillosis with bronchoalveolar lavage fluid. J Clin Microbiol. 2004;42:5517–22.
Nucci M, Anaissie, E. Fusarium infections in immunocompromised patients. Clin Microbiol Rev. 2007;20:695–704.
Pappas GP, Kauffman CA, Andes D, et al. Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis. 2009;48:503–35.
Pascual A, Calandra T, Bolay S, Buclin T, Bille J, Marchetti O. Voriconazole therapeutic drug monitoring in patients with invasive mycoses improves efficacy and safety outcomes. Clin Infect Dis. 2008;46:201–11.
Reed EC, Bowden RA, Dandliker PS, Lilleby KE, Meyers JD. Treatment of cytomegalovirus pneumonia with ganciclovir and intravenous cytomegalovirus immunoglobulin in patients with bone marrow transplants. Ann Intern Med. 1988;109:783–8.
Renaud C, Xie H, Seo S, et al. Mortality rates of human metapneumovirus and respiratory syncytial virus lower respiratory tract infections in hematopoietic stem cell transplant recipients. Biol Blood Marrow Transplant. 2013;19:1220–6.
Savona MR, Newton D, Frame D, Levine JE, Mineishi S, Kaul DR. Low-dose cidofovir treatment of BK virus-associated hemorrhagic cystitis in recipients of hematopoietic stem cell transplant. Bone Marrow Transplant. 2007;39:783–7.
Schmidt GM, Kovacs A, Zaia JA, et al. Ganciclovir/immunoglobulin combination therapy for the treatment of human cytomegalovirus-associated interstitial pneumonia in bone marrow allograft recipients. Transplantation. 1988;46:905–7.
Shah DP, Ghantoji SS, Mulanovich VE, Ariza-Heredia EJ, Chemaly RF. Management of respiratory viral infections in hematopoietic cell transplant recipients. Am J Blood Res. 2012;2:203–18.
Smith J, Andes D. Therapeutic drug monitoring of antifungals: pharmacokinetic and pharmacodynamic considerations. Ther Drug Monit. 2008;30:167–72.
Sobel JD, Bradshaw SK, Lipka CJ, Kartsonis NA. Caspofungin in the treatment of symptomatic candiduria. Clin Infect Dis. 2007;44:e46–9.
Sokos DR, Berger M, Lazarus HM. Intravenous immunologlobulin: appropriate indications and uses in hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2002;8:117–30.
Spellberg B, Walsh TJ, Kontoyiannis DP, Edwards J Jr, Ibrahim AS. Recent advances in the management of mucormycosis: from bench to bedside. Clin Infect Dis. 2009;48:1743–51.
Styczynski J, Einsele H, Gil L, Ljungman P. Outcome of treatment of Epstein-Barr virus related post-transplant lymphoproliferative disorder in hematopoietic stem cell recipients: a comprehensive review of reported cases. Transpl Infect Dis. 2009;11:383–92.
Sun HY, Wagener MM, Singh, N. Cryptococcosis in solid-organ, hematopoietic stem cell, and tissue transplant recipients: evidence-based evolving trends. Clin Infect Dis. 2009;48:1566–76.
Tomblyn M, Chiller T, Einsele H, et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective. Biol Blood Marrow Transplant 2009;15:1143–238.
Walsh TJ, Anaissie EJ, Denning DW, et al. Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2008;46:327–60.
Weinstock DM, Ambrossi GG, Brennan C, Kiehn TE, Jakubowski A. Preemptive diagnosis and treatment of Epstein-Barr virus-associated post transplant lymphoproliferative disorder after hematopoietic stem cell transplant: an approach in development. Bone Marrow Transplant. 2006;37:539–46.
Zerr DM, Corey L, Kim HW, Huang ML, Nguy L, Boeckh M. Clinical outcomes of human herpes virus 6 reactivation after hematopoietic stem cell transplantation. Clin Infect Dis. 2005;40:932–40.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Strasfeld, L. (2015). Infectious Complications. In: Maziarz, R., Slater, S. (eds) Blood and Marrow Transplant Handbook. Springer, Cham. https://doi.org/10.1007/978-3-319-13832-9_17
Download citation
DOI: https://doi.org/10.1007/978-3-319-13832-9_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-13831-2
Online ISBN: 978-3-319-13832-9
eBook Packages: MedicineMedicine (R0)