
Abstract
1. The clinical features of adult Still’s disease resemble the systemic form of JRA a. Seronegative chronic polyarthritis associated with a systemic inflammatory illness b. Initially described in 1897 by George F. Still (pathologist) c. Subsequently detailed in adults in 1971 by Eric Bywaters 2. Epidemiology a. Rare b. Affects both genders equally c. Exists worldwide d. Majority present at age 16–35 years i. 75% before age 35
You have full access to this open access chapter, Download chapter PDF
Keywords
- Status Epilepticus
- Serum Ferritin
- Connective Tissue Disease
- Mycophenolate Mofetil
- Sensorineural Hearing Loss
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
-
1.
The clinical features of adult Still’s disease resemble the systemic form of JRA
-
a.
Seronegative chronic polyarthritis associated with a systemic inflammatory illness
-
b.
Initially described in 1897 by George F. Still (pathologist)
-
c.
Subsequently detailed in adults in 1971 by Eric Bywaters
-
a.
-
2.
Epidemiology
-
a.
Rare
-
b.
Affects both genders equally
-
c.
Exists worldwide
-
d.
Majority present at age 16–35 years
-
i.
75% before age 35
-
i.
-
a.
-
3.
Pathogenesis
-
a.
Etiology unknown
-
b.
Principal hypothesis implicates a virus or other infectious agent
-
c.
Linkage to HLA antigens inconclusive
-
d.
Immune complexes may play a pathogenic role (not confirmed)
-
e.
NO association with pregnancy and use of hormones
-
f.
Stress may play a role as inducer (not confirmed)
-
g.
Circadian release of proinflammatory cytokines
-
i.
Accounts for many clinical features
-
ii.
IL-6
-
iii.
IL-18
-
1.
Elevated
-
2.
Stimulates ferritin synthesis in monocytes/macrophages
-
1.
-
i.
-
a.
-
4.
Clinical Findings
-
a.
Preceded by a prolonged course of nonspecific signs and symptoms
-
b.
A prodromal sore throat occurs days to weeks before other symptoms
-
i.
Occurs in 70% (50–92%)
-
i.
-
c.
The most striking manifestations
-
i.
Severe arthralgia (98–100%) and myalgia (84–98%)
-
ii.
Malaise
-
iii.
Weight loss (19–76%)
-
iv.
Fever (83–100%)
-
i.
-
d.
Less common clinical manifestations
-
i.
Lymphadenopathy (48–74%)
-
ii.
Splenomegaly (45–55%)
-
iii.
Pleuritis (23–53%)
-
iv.
Abdominal pain (9–48%)
-
v.
Hepatomegaly (29–44%)
-
vi.
Pericarditis (24–37%)
-
vii.
Pneumonitis (9–31%)
-
i.
-
e.
Unusual manifestation (numerous)
-
i.
Alopecia
-
ii.
Sjogren’s
-
iii.
Subcutaneous nodules
-
iv.
Necrotizing lymphadenitis
-
v.
Acute liver failure
-
vi.
Pulmonary fibrosis
-
vii.
Cardiac tamponade
-
viii.
Aseptic meningitis
-
ix.
Peripheral neuropathy
-
x.
Proteinuria
-
xi.
Microscopic hematuria
-
xii.
Amyloidosis
-
xiii.
Hemolytic anemia
-
xiv.
DIC
-
xv.
TTP
-
xvi.
Orbital pseudotumor
-
xvii.
Cataracts
-
xviii.
Sensorineural hearing loss
-
xix.
Hemophagocytic syndrome
-
i.
-
f.
Patients appear severely ill
-
i.
Often receive numerous courses of antibiotics
-
ii.
Presumed septic with negative cultures
-
i.
-
g.
Fever
-
i.
Initial symptom
-
ii.
Usually sudden onset high and spiking
-
iii.
Spikes once daily (rarely twice daily)
-
1.
Usually early morning and/or late afternoon/evening
-
2.
Quotidian or diquotidian pattern
Fig. 16.1 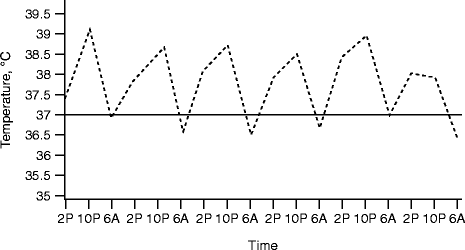
Fever pattern in adult-onset Still’s disease (Reproduced with permission from Rheumatoid arthritis, juvenile rheumatoid arthritis, and related conditions. Atlas of Rheumatology. ImagesMD; 2002-03-07)
-
1.
-
iv.
Lasts 2–4 h
-
v.
Temperature elevation marked
-
1.
66% with fever >40°C
-
1.
-
vi.
Returns to normal in 80% of untreated patients
-
1.
Can return below normal
-
1.
-
vii.
Very ill when febrile
-
1.
Feels well with normal body temp
-
1.
-
viii.
Pattern contrasts with that seen with infection
-
1.
Baseline elevation in body temperature
-
2.
Episodic fever spikes
-
1.
-
ix.
Patients evaluated for FUO
-
1.
5% eventually diagnosed with Still’s
-
1.
-
i.
-
h.
Arthritis (88–84%)
-
i.
Initially affects only a few joints
-
ii.
Evolves to polyarticular disease
-
iii.
Most commonly affected joints
-
1.
Knee (84%)
-
2.
Wrist (74%)
Fig. 16.2 
Wrist involvement in adult-onset Still’s disease (Reproduced with permission Rheumatoid arthritis, juvenile rheumatoid arthritis, and related conditions. Atlas of Rheumatology. ImagesMD; 2005-01-18)
-
3.
Ankle, shoulder, elbow, and PIP joints (50%)
-
4.
MCP (33%)
-
5.
DIP (20%)
-
1.
-
iv.
Other joints affected
-
1.
MTPs
-
2.
Hips
-
3.
Tempromandibular joint (TMJ)
-
1.
-
v.
Neck pain (50%)
-
vi.
Arthrocentesis yields
-
1.
Class II inflammatory synovial fluid
-
2.
Neutrophil predominance
-
1.
-
vii.
Destructive arthritis (20–25%)
-
i.
-
i.
Still’s rash
-
i.
Present in more than 85% of patients
-
ii.
Almost pathognomonic
-
iii.
Salmon pink
-
iv.
Macular or maculopapular
Fig. 16.3 
Rash in adult-onset Still’s disease (Reproduced with permission from Rheumatoid arthritis, juvenile rheumatoid arthritis, and related conditions. Atlas of Rheumatology. ImagesMD; 2002-03-07)
-
v.
Frequently evanescent
-
vi.
Often occurs with the evening fever spike
-
1.
Evening rounds may detect this near-diagnostic finding
-
1.
-
vii.
More common on the trunk and proximal extremities
-
viii.
Precipitated by
-
1.
Mechanical irritation
-
a.
Clothing
-
b.
Rubbing
-
c.
Koebner’s phenomenon (up to 40%)
-
a.
-
2.
Heat
-
a.
Hot bath
-
b.
Applying a hot towel
-
a.
-
1.
-
ix.
May be mildly pruritic
-
x.
Skin biopsies and immunofluorescent studies
-
1.
Neurivascular mononuclear cell infiltrate
-
2.
Nondiagnostic
-
1.
-
i.
-
a.
-
5.
Laboratory Findings
-
a.
No diagnostic tests
-
b.
Serum ferritin
-
i.
An acute-phase reactant that reflects inflammation
-
ii.
An extremely elevated level suggest the diagnosis
-
iii.
A value of ≥1,000 mg/dl in the proper clinical setting
-
1.
Confirmatory
-
2.
Especially associated with a low glycosylated ferritin
-
1.
-
iv.
Values >4,000 mg/dl seen in <50%
-
v.
Reason for such elevations unknown
-
i.
-
c.
CRP
-
i.
Frequently greater than 10 times upper limit of normal
-
i.
-
d.
ESR
-
i.
Universally elevated >50 (96–100%)
-
i.
-
e.
Leukocytosis
-
i.
Range 12–40,000/mm3 present in 90% (71–97%)
-
ii.
80% have WBC count > 15,000/mm3
-
iii.
Neutrophils ≥ 80% (55–88%)
-
i.
-
f.
LFT
-
i.
Elevated in up to three-quarters of patients (35–85%)
-
i.
-
g.
Anemia
-
i.
Common (59–92%)
-
ii.
Sometimes profound
-
i.
-
h.
Thrombocytosis (52–62%)
-
i.
Hypoalbuminemia (44–88%)
-
j.
RF and ANA
-
i.
Generally negative or low titer
-
i.
-
k.
Synovial and serosal fluids
-
i.
Inflammatory
-
ii.
Predominance of neutrophils
-
i.
-
a.
-
6.
Radiographic Findings
-
a.
Early
-
i.
Soft-tissue swelling
-
ii.
Effusions
-
iii.
Periarticular osteoporosis (occasionally)
-
i.
-
b.
Late
-
i.
Joint erosions
-
ii.
Fusions
-
1.
Carpal bones (50%)
-
2.
Tarsal bones (20%)
-
3.
Cervical spine (10%)
-
1.
-
i.
-
c.
Characteristic radiographic findings
-
i.
Typically found in the wrist
-
ii.
Nonerosive narrowing of carpometacarpal and intercarpal joints
-
iii.
Progresses to bony ankylosis
-
i.
Fig. 16.4 
Radiographic changes in adult-onset Still’s disease include periarticular osteopenia and loss of joint space (Reproduced with permission from Rheumatoid arthritis, juvenile rheumatoid arthritis, and related conditions. Atlas of Rheumatology. ImagesMD; 2002-03-07)
-
a.
-
7.
Diagnosis
-
a.
Diagnosis one of exclusion
-
i.
With the proper clinical and laboratory abnormalities
-
ii.
With the absence of another explanation (infection or malignancy)
-
i.
-
b.
Criteria of Cush (practical guide)
-
i.
Diagnosis requires the presence of all of the following
-
1.
Fever >39°C (102.2°F)
-
2.
Arthralgia or arthritis
-
3.
RF < 1:80
-
4.
ANA < 1:100
-
1.
-
ii.
In addition, any two of the following
-
1.
WBC count ≥ 15,000 cells/mm3
-
2.
Still’s rash
-
3.
Pleuritis or pericarditis
-
4.
Hepatomegaly or splenomegaly or generalized lymphadenopathy
-
1.
-
i.
-
c.
Most do not present with the full-blown syndrome
-
d.
Typical presentation for adult Still’s disease
-
i.
High, daily fever spikes
-
ii.
Severe myalgia, arthralgia, and arthritis
-
iii.
Still’s rash
-
iv.
Leukocytosis
-
i.
-
e.
Markedly elevated serum ferritin highly suggestive
-
a.
-
8.
Differential Diagnosis
-
a.
Granulomatous disorders
-
i.
Sarcoidosis
-
ii.
Idiopathic granulomatosis hepatitis
-
iii.
Crohn’s disease
-
i.
-
b.
Vasculitis
-
i.
Serum sickness
-
ii.
PAN
-
iii.
Wegener’s
-
iv.
TTP
-
v.
Takayasu’s
-
i.
-
c.
Infection
-
i.
Viral
-
1.
Hepatitis B
-
2.
Rubella
-
3.
Parvovirus
-
4.
Coxsackie
-
5.
EBV
-
6.
CMV
-
7.
HIV
-
1.
-
ii.
Subacute bacterial endocarditis
-
iii.
Chronic meningococcemia
-
iv.
Gonococcemia
-
v.
TB
-
vi.
Lyme
-
vii.
Syphilis
-
viii.
Rheumatic fever
-
i.
-
d.
Malignancy
-
i.
Leukemia
-
ii.
Lymphoma
-
iii.
Angioblastic lymphadenopathy
-
i.
-
e.
Connective tissue disease
-
i.
SLE
-
ii.
Mixed connective tissue disease
-
i.
-
a.
-
9.
Disease Course and Outcome
-
a.
Median time to achieve clinical and laboratory remission
-
i.
10 months while receiving therapy
-
ii.
32 months requiring no therapy
-
i.
-
b.
Can remit years after onset
-
c.
Course generally follows one of three patterns (one-third of patients each)
-
i.
Self-limited disease
-
1.
Remission within 6–9 months
-
2.
One-fifth to one-third
-
1.
-
ii.
Intermittent flares
-
1.
One recurrence
-
a.
Two-thirds
-
b.
10–36 months from the original illness
-
a.
-
2.
Multiple flares
-
a.
Up to ten flares reported
-
b.
Intervals of 3–48 months
-
c.
Recurrent episodes generally milder than the original
-
d.
Respond to lower doses of meds
-
e.
Timing of relapse unpredictable
-
a.
-
1.
-
iii.
Chronic Still’s disease
-
1.
Chronic arthritis is the principle problem
-
2.
Severe involvement of the knees and hips
-
a.
Require total joint replacement
-
a.
-
3.
Most common in the hip
-
1.
-
i.
-
d.
Markers of chronic disease or poor prognosis
-
i.
Presence of polyarthritis (four or more joints involved)
-
ii.
Root joint involvement (shoulders or hips)
-
iii.
A childhood episode
-
1.
Occurs in about one of six patients
-
1.
-
iv.
More than 2 years of therapy with systemic corticosteroids
-
i.
-
e.
A controlled study of patients 10 years after the diagnosis of Still’s
-
i.
Significant higher levels of pain, physical disability, and psychologic disability than unaffected siblings
-
ii.
Levels of pain and disability lower than other chronic rheumatic disease
-
iii.
No difference in Still’s patients and controls in overcoming handicaps
-
1.
Educational attainment
-
2.
Occupational prestige
-
3.
Social functioning
-
4.
Family income
-
1.
-
i.
-
f.
5 year survival rate 90–95%
-
i.
Similar to the survival rate for lupus
-
ii.
Vast majority lead remarkably full lives after disease onset
-
i.
-
g.
Premature death may be slightly increased
-
h.
Causes of mortality
-
i.
Hepatic failure
-
ii.
DIC
-
iii.
Amyloidosis
-
iv.
Sepsis
-
v.
Acute respiratory distress syndrome (ARDS)
-
vi.
Heart failure
-
vii.
Carcinoma of the lung
-
viii.
Status epilepticus
-
i.
-
a.
-
10.
Acute Treatment
-
a.
NSAIDs
-
i.
About one-fourth respond (20–40%)
-
ii.
A commonly used regimen
-
1.
High dose enteric-coated aspirin
-
2.
Achieve a serum salicylate level of 15–25 mg/dl
-
3.
Sometimes combined with indomethacin (150 mg/day)
-
1.
-
iii.
Side effects
-
1.
Hepatotoxicity
-
a.
Elevated LFTs usually return to normal
-
b.
Despite continued NSAID therapy
-
a.
-
2.
Increased risk of DIC
-
1.
-
i.
-
b.
Systemic corticosteroids
-
i.
Patients who fail to respond to NSAIDs
-
ii.
For severe disease
-
1.
Pericardial tamponade
-
2.
Myocarditis
-
3.
Severe pneumonitis
-
4.
DIC
-
5.
Rising LFTs during NSAID treatment
-
1.
-
iii.
Prednisone in a dose of 0.5–1.0 mg/kg/day
-
iv.
About one-third require at least 60 mg of prednisone daily
-
v.
Relapses occur during tapering
-
1.
Add one of the slow-acting antirheumatic drugs
-
a.
Methotrexate
-
a.
-
1.
-
vi.
IV pulse methylprednisolone used for life-threatening disease
-
i.
-
a.
-
11.
Chronic Treatment
-
a.
Medications used to treat arthritis (the most common cause of chronicity)
-
i.
IM gold
-
ii.
Hydroxychloroquine
-
1.
Mild chronic systemic disease may respond as well
-
a.
Fatigue
-
b.
Fever
-
c.
Rash
-
d.
Serositis
-
a.
-
1.
-
iii.
Sulfasalazine
-
1.
Increased toxicity may occur
-
1.
-
iv.
Penicillamine
-
v.
Methotrexate
-
1.
Low doses (similar to those used in RA)
-
2.
Used in both chronic arthritis and chronic systemic disease
-
1.
-
i.
-
b.
Immunosuppressive agents
-
i.
Used in resistant cases
-
ii.
Azathioprine
-
iii.
Cyclophosphamide
-
iv.
Cyclosporine
-
v.
IVIG (controversial)
-
vi.
Mycophenolate mofetil
-
vii.
Leflunomide
-
i.
-
c.
Biologics
-
i.
TNF-α elevated in Still’s disease
-
ii.
Etanercept and infliximab beneficial
-
1.
Especially articular manifestations
-
1.
-
iii.
Anakinra
-
1.
Successful in refractory disease
-
1.
-
i.
-
d.
Therapy after a decade of disease
-
i.
About one-half of patients will require second-line agents
-
ii.
One-third will require low-dose corticosteroids
-
i.
-
e.
Multidisciplinary approach
-
i.
Physiotherapists
-
ii.
Occupational therapists
-
iii.
Psychologists
-
iv.
Arthritis support groups
-
i.
-
a.




Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer-Verlag London Limited
About this chapter
Cite this chapter
Colburn, N.T. (2011). Adult Still’s Disease. In: Review of Rheumatology. Springer, London. https://doi.org/10.1007/978-1-84882-093-7_16
Download citation
DOI: https://doi.org/10.1007/978-1-84882-093-7_16
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-84882-092-0
Online ISBN: 978-1-84882-093-7
eBook Packages: MedicineMedicine (R0)