
Abstract
The discovery of angiotensin-(1-7) [Ang-(1-7)] in 1988 represented the first deviation from the traditional biochemical cascade of forming bioactive angiotensin peptides. Prior to that time, the biological actions of angiotensin II (Ang II) were being investigated as it relates to cardiovascular function, including hypertension, cardiac hypertrophy and failure, as well as biological actions in the brain and kidney. We now know that Ang II elicits a whole host of actions both within and outside of the cardiovascular system. Furthermore, the discovery of Ang-(1-7) by our laboratory was also the first indication of a biologically active angiotensin peptide that further studies revealed served to counter-balance the actions of Ang II. This chapter reviews the data demonstrating the role of the vasodepressor axis of the renin angiotensin system in the regulation of cardiovascular function and the new data that shows the existence of angiotensin-(1-12) as a novel alternate substrate for the production of angiotensin peptides. The ultimate role of this discovery, as well as the continuing elucidation of mechanisms pertaining to RAS physiology, will likely be clarified in the coming years, in hopes of improving the treatment of cardiovascular disease.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
The existence of the renin angiotensin system (RAS) as a major physiological regulator has been known since Tigerstedt and Bergman first discovered the enzyme renin over a century ago [1]. Nearly 60 years after the initial discovery of renin, Irvine Page from the United States and Braun Menendez from Argentina independently discovered a pressor hormone, “angiotonin” or “hypertensin,” which was later agreeably called “angiotensin” (Ang). We now know this hormone to be the octapeptide pressor hormone, Ang II, which is produced from the sequential cleavage of the protein (Aogen) into Ang I by renin and Ang I into Ang II by angiotensin-converting enzyme (ACE).
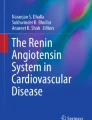
This linear hydrolysis cascade was undisputed for many years until studies from our laboratory in 1988 showed that a previously considered inert metabolite of Ang II, Ang-(1-7), caused the release of vasopressin from the rat brain hypothalamus [2]. This study was the first demonstration of biological activity of a peptide within the RAS that was not Ang II-mediated. The discovery of Ang-(1-7) expanded our knowledge about the complexities of the RAS and has garnered increasing support for a potential target for the therapeutic treatment of diseases such as hypertension, heart disease, and even cancer [3, 4]. This chapter focuses on the functional role of Ang-(1-7) in the heart, as well as the important contribution that angiotensin-converting enzyme 2 (ACE2) plays in degrading Ang II into Ang-(1-7). While the evidence for a protective role for this counterbalancing arm of the RAS continues to accumulate, we also comment on the identification of a new angiotensin peptide upstream of Ang I, called angiotensin-(1-12), and how it may function in tissues as an alternate precursor for angiotensin peptide production. A diagram of the most current view of the renin angiotensin system is shown in Fig. 10.1.

Current view of the renin angiotensin system. Abbreviations: ADAMs, tumor necrosis factor-α convertases, such as ADAM17; sACE2, secreted ACE2
Angiotensin-(1-7): Gaining Favor in the 21st Century
The discovery of Ang-(1-7) in the late 1980s did not lend itself to ready acceptance [2, 5–7]. However, studies investigating the role of Ang-(1-7) are on the rise, and a whole new array of data has been emerging on this bioactive peptide since the turn of the 21st century. Most of the biological effects of Ang-(1-7) that are discussed below have been attributed to the mas receptor, which was identified as a functional receptor for Ang-(1-7) [8].
Angiotensin-(1-7) and the Regulation of Cardiac Dynamics
The presence of Ang-(1-7) in the heart and the ability of the heart to produce Ang-(1-7) were not known for some time. Ang-(1-7) was identified in cardiomyocytes of the heart, but not cardiac fibroblasts, and Averill et al. [9] further showed that its expression was augmented after coronary artery ligation. Several studies have shown that Ang-(1-7) can be synthesized by the heart, and we showed a direct conversion of Ang II into Ang-(1-7) in isolated hearts from normal and hypertensive rats [10]. Early studies investigating a direct role for Ang-(1-7) actions in the heart showed that it was protective against ischemia-induced cardiac dysfunction [11–13], which may be due in part to the activation of the sodium pump [14]. Additional studies in the cardiomyopathy hamster showed that the anti-arrhythmic effects of Ang-(1-7) are mediated through hyperpolarization of the heart cell [15]. Further evidence that Ang-(1-7) is a direct positive effector in the heart stems from data showing its anti-fibrotic and anti-hypertrophic actions [16–20]. Because Ang-(1-7) is a peptide and thus has a short half-life, several studies have investigated a more stable analog of Ang-(1-7), called AVE0991. The administration of this Ang-(1-7) analog is associated with improvement of cardiac function in diabetic rats [21], improved baroreceptor sensitivity [22], and potentiation of the vasodilator actions of bradykinin [23].
The mas receptor mediates the signaling mechanisms produced by Ang-(1-7) [8]. We further showed that transfection of cultured myocytes with an antisense oligonucleotide to the mas receptor blocked the Ang-(1-7)-mediated inhibition of serum-stimulated mitogen-activated protein kinase (MAPK) activation, whereas a sense oligonucleotide was ineffective [19]. In keeping with these findings, chronic mas deficiency leads to impaired Ca2+ handling in cardiomyocytes in culture [24].
Salt and the ACE2/Ang-(1-7)/mas Axis
A clear relationship between salt intake and prevalence of hypertension has been shown in abundant epidemiological and interventional studies [25–28], giving support for the current recommendation for sodium intake of 2,400 mg per day by the American Heart Association. On the other hand, despite numerous studies suggesting that interruption of ACE2/Ang-(1-7)/mas receptor axis may lead to hypertension and cardiac dysfunction [29–31], little is known about its response to altered sodium intake with respect to blood pressure changes or target organ damage. Our laboratory was among the first one to report the importance of a tonic depressor activity of Ang-(1-7) to the maintenance of blood pressure in the spontaneously hypertensive rats, with endogenous RAS activation induced by chronic salt depletion [32]. Furthermore, in the face of unchanged plasma Ang-(1-7), an enhanced vascular sensitivity to endogenous Ang-(1-7) in salt-restricted state suggests significant amplification in Ang-(1-7) receptor–signaling interaction. Subsequent studies also revealed that, under the condition of increased renal Ang II due to salt depletion [33] or 2K1C Goldblatt hypertension [34], endogenous Ang-(1-7) counterbalanced the effects of Ang II to maintain a glomerular filtration rate and renal plasma flow [34]. Thus, could it be possible that insufficient synthesis or activity of ACE2/Ang-(1-7)/mas may be a critically important mechanism in salt-sensitive hypertension?
Indeed, it has been shown that in female Dahl salt-sensitive rats fed high-salt diet, chronic Ang-(1-7) supplementation reduced increase in blood pressure and improved aortic and renal blood flow by increasing prostacyclin and prostaglandinE2 release. It was believed that an increase in plasma levels of nitric oxide following Ang-(1-7) infusion was responsible for this observed vasodilatory effect [35]. It has also been shown that acute vasodilation by Ang-(1-7) was augmented in rats fed high-sodium versus low-salt diet due to an increase in vasodilatory and a decrease in vasoconstrictor prostanoids [36]. But the antagonistic and nitric oxide-independent effect of Ang-(1-7) on Ang II-induced vasoconstriction in aortic rings from the rats fed high-sodium diet was abolished in rats fed low-sodium diet [37]. Thus, further studies are warranted to define precisely a fine-tuning mechanism of Ang-(1-7) in the regulation of blood pressure and flow as well as vascular reactivity in different status of sodium intake. In this context, it is important to note that in salt-sensitive hypertensive patients, omapatrilat, a dual ACE and neprilysin inhibitor, effectively reduced blood pressure and increased urinary excretion of Ang-(1-7) [38]. This study clearly pointed out that besides the inhibition of Ang II production and degradation of atrial natriuretic peptide and bradykinin, an Ang-(1-7) of renal origin may contribute to the hypotensive effect of omapatrilat in the patients whose blood pressure is sensitive to sodium intake.
Finally, having in mind the anti-hypertrophic and anti-fibrotic effects of Ang-(1-7), it is intriguing to hypothesize that salt-induced left ventricular remodeling and renal injury observed in different forms of experimental and human hypertension [39–43] may be, at least in part, governed by alteration of the ACE2/Ang-(1-7)/ mas axis. In fact, in Dahl salt-sensitive rats fed high-salt diet, cardiac enlargement and fibrosis were associated with an increased cardiac angiotensinogen but reduced cardiac ACE2 mRNA. Treatment with AT1 receptor antagonist, but not mineralocorticoid receptor blocker, reversed the effect of salt on ACE2 gene expression [44]. Importantly, both therapies ameliorated salt-induced cardiac remodeling along with a reduction in angiotensinogen and ACE mRNA. Therefore, it seems that the effects of salt-intake variation or RAS blockade may ultimately depend on their net effects on the two opposing arms of the RAS. Furthermore, low sodium intake in Wistar rats reduced renal ACE, but not ACE2 mRNA and activity; this effect was not amplified during ACE inhibition [45]. Neither plasma Ang II nor Ang-(1-7) were affected by low sodium intake, but ACE inhibition increased plasma Ang-(1-7) shifting the balance between the two opposing peptides toward Ang-(1-7) more effectively during a low sodium intake. Moreover, blood pressure was the lowest in the group treated with ACE inhibitor and low-salt intake. The findings from these studies corroborate well with previous conclusion that anti-hypertensive and cardio-renal protective effects of RAS blockade stemmed, at least in part, from Ang-(1-7) pathway activation [46–48] and that these effects may be more pronounced if followed by dietary sodium restriction [49]. Further studies are clearly necessary to explore whether the beneficial effects of dietary sodium alteration and/or pharmacological intervention indeed depend on preferable ACE/ACE2 and ultimately Ang II/Ang-(1-7) balance in the target organs.
ACE2: A Critical Enzyme Regulator in the Heart
The discovery of the biological effector peptide, Ang-(1-7) in 1988 represented the first expansion of the classical RAS cascade in that it was the only other known peptide member of the RAS to elicit some physiological function. However, the formation of Ang-(1-7) remained elusive for several years. Welches and colleagues [50] first showed that Ang-(1-7) could be formed from the traditional RAS precursor peptide, Ang I, by endopeptidases including prolyl oligopeptidase (POP, E.C. 21.26), neprilysin (NEP, E.C. 24.11), and thimet oligopeptidase (TOP, E.C. 24.15). While it was known that prolyl oligopeptidase could cleave the Pro7-Phe8 bond of Ang II, the studies were not supported by convincing in vivo evidence. Moreover, studies by Yang et al. [51] found that prolyl carboxypeptidase (PCP, E.C. 16.2), a lysosomal enzyme with an acidic pH optimum, could cleave Ang II into Ang-(1-7). The hydrolysis appeared to be an intracellular cleavage, and the observation that the acidic pH optimum of PCP of 5.0 provided some doubt as to the physiological role for this enzyme in producing Ang-(1-7).
It was not until 2000, when two independent research groups described a homolog of ACE, called angiotensin-converting enzyme 2 (ACE2) [52, 53], that a viable Ang-(1-7)-forming enzyme from Ang II was discovered. Shortly after its discovery, Vickers et al. [54] showed that ACE2 could cleave Ang II into Ang-(1-7) with high affinity. ACE2 also cleaved apelin, des-Arg9-bradykinin, and the opioid peptide dynorphin A 1-13 with similar affinities, but its involvement in modulating these peptides in vivo remains to be clarified. Subsequent studies revealed the generation of Ang-(1-7) in human failing heart tissue, which was dependent on Ang II [55], suggesting that ACE2 was required for the cleavage of Ang II into Ang-(1-7). Studies from our laboratory represented the first direct in vivo evidence for ACE2’s participation in hydrolyzing Ang II into Ang-(1-7) in hearts isolated from both normal and hypertensive rats [10]. We further showed that the hypertrophied hearts from hypertensive rats were almost completely reliant on ACE2 for the production of Ang-(1-7) from Ang II, whereas ACE2 in the normal heart was of less importance.
ACE2 is widely expressed in many tissues in humans [56] and rodents [56, 57], including the heart. In addition, work from this laboratory first demonstrated that cardiac expression of ACE2 mRNA was regulated by the actions of Ang II via an AT1 receptor pathway [58]. A more recent study showed that the negative actions of Ang II on cardiac ACE2 mRNA could be mimicked by the addition of endothelin-1 and that both effects could be blocked by inhibitors of mitogen-activated protein (MAP) kinase kinase 1, suggesting that Ang II or endothelin-1 activate ERK1/ERK2 to reduce ACE2 [59].
The importance of ACE2 in the regulation of cardiac function was determined when Crackower and colleagues [29] demonstrated that genetic inactivation of ACE2 in mice resulted in severe blood-pressure-independent systolic impairments in cardiac function, which was associated with significant accumulation of circulating and cardiac Ang II. The concomitant genetic inactivation of ACE completely rescued the ACE2-null cardiac phenotype, further implicating elevated Ang II in cardiac dysfunction observed in the ACE2-null mice. These studies were the first to support the in vivo importance of ACE2 in regulating cardiac function and Ang II metabolism. In addition to these findings, two additional ACE2-null mice strains were generated by separate groups [60, 61]. One strain exhibited cardiac dysfunction only in response to pressure overload, which was also associated with increased cardiac Ang II [61]. The impairments in cardiac dysfunction were abrogated with the co-administration of the AT1 receptor antagonist, candesartan. In contrast, Gurley et al. [60] reported that genetic inactivation of ACE2 in 129/SvEv, C57BL/6, or mixed mouse backgrounds did not induce any functional impairments in the heart, suggesting that the importance of cardiac ACE2 may be dependent on the genetic background of the animal model [62]. In this context, Mercure et al. [63] reported that an eightfold increase in Ang(1-7) in the heart of transgenic animals was associated with less ventricular hypertrophy and fibrosis than their nontransgenic littermates in response to a hypertensive challenge.
A view from an opposite approach to determine the physiological importance of ACE2 further favors a cardioprotective role for the enzyme. Indeed, the overexpression of ACE2 protects the heart from Ang II-induced cardiac hypertrophy and myocardial fibrosis in rats [64]. Moreover, elevations in cardiac ACE2 exhibited a partial rescue of the cardiac functional deficits induced by coronary artery ligation in rats [65]. The cardioprotective persona given to ACE2 is further illustrated by its regulation in pathological conditions. Three very important independent studies showed that cardiac ACE2 was upregulated in both humans and rodent models of heart failure [66–68]. Moreover, we first showed that secreted ACE2 (sACE2) was elevated in the cardiac effluent of hypertrophied hearts, suggesting that the enzyme was attempting to protect the heart from progressing toward overt failure as is known in the Ren-2 transgenic rats [10]. These data were very recently supported by human studies that measured sACE2 activity in human plasma, and the authors showed that the sACE2 was indeed markedly increased in patients diagnosed with heart failure [69]. Intriguingly, Lambert et al. [70] recently demonstrated that the tumor necrosis factor convertase, ADAM17, participated in the shedding of ACE2 from the membrane, and other studies have reported that ADAM17 is upregulated in heart failure [71].
Collectively, the data on the physiological importance of cardiac ACE2 are clear: it exerts a cardioprotective role from the early stages of cardiac hypertrophy through overt heart failure, although its efforts may be insufficient to overcome the progression of heart disease. However, further studies are required to determine the importance of the discovery of an endogenous ACE2 inhibitor [72], as well as the emerging data that ACE2 is a functional receptor for the SARS coronavirus [73], as these may provide alternative therapeutic targets for the treatment of cardiovascular disease.
Angiotensin-(1-12)
Over the years, questions have been raised regarding the capability of cardiac and vascular tissue to synthesize Ang II [74–78]. The heart remains a critical example. Although a large body of evidence suggests the existence of local tissue RAS in the regulation of cardiac function and remodeling, most studies revealed low levels of gene expression for both cardiac renin and Aogen [79]. Neither the identification of renin in cardiac mast cells [80] excludes an uptake mechanism from the blood compartment nor does the finding of renin activation by binding of prorenin to the prorenin/renin receptor [81–83] can be construed as evidence for local production of cellular renin. Likewise, Aogen gene expression in cardiac tissue has been reported at very low expression levels while the question of how much of the Aogen mRNA is due to its presence in the endothelial cells of intracoronary vessels and cardiac fibroblast has not been answered.
Our current view of the RAS as a complex system entailing several levels of regulation and processing is now further expanded with the identification of proangiotensin-12 [angiotensin-(1-12), Ang-(1-12)] as an upstream propeptide to Ang I [84]. These investigators first isolated this novel Aogen-derived peptide from the rat small intestine. Consisting of 12 amino acids, this peptide was termed proangiotensin-12 based on its possible role as an Ang II precursor. Ang-(1-12) constricted aortic strips and, when infused intravenously, raised blood pressure in rats. The vasoconstrictor responses to Ang-(1-12) were abolished by either captopril or the AT1 blocker CV-11974. Current studies from this laboratory now demonstrate the existence of Ang-(1-12) in both the heart and the kidneys of spontaneously hypertensive rats (SHR), primarily restricted to cardiac myocytes and renal tubular cells [85]. In addition, the cardiac content of Ang-(1-12) was significantly augmented in the heart of SHR compared to Wistar-Kyoto (WKY) controls [85]. Moreover, an insight into the processing of Ang-(1-12) into Ang I, Ang II, and Ang-(1-7) was accomplished by studying the effects of exogenously administered Ang-(1-12) in isolated hearts from both normotensive and hypertensive rat strains [86]. In these studies, we showed processing of Ang-(1-12) into Ang I, Ang II, and Ang-(1-7). Moreover, in the group of WKY and SHR investigated in this study, the addition of a specific renin inhibitor to the preparation in no manner altered the production of angiotensins from Ang-(1-12). These data showed that Ang-(1-12) is processed into the active angiotensin peptides by a non-renin mechanism. While further work will be required to ascertain the biological role of Ang-(1-12), these data expand on our knowledge of the mechanisms by which the RAS regulates the expression of angiotensins in tissues [87–90].
Conclusions
The discovery of the counter-balancing ACE2/Ang-(1-7)/mas arm of the RAS has expanded knowledge of the intrinsic mechanisms by which the system regulates homeostasis and tissue perfusion in both physiology and pathology [91]. Rapid advances in this field now suggest alternate approaches to suppress the pathological actions of Ang II by enhancing the counter-regulatory actions of Ang-(1-7), augmenting the activity of ACE2, or both. Moreover, the discovery of Ang-(1-12) in multiple tissues including the heart may provide additional mechanistic insights that could lead to the better treatment and management of hypertension and heart failure.
References
Tigerstedt, R., and Bergman, P.G. (1998) Niere und Kreislauf. Scan Arch Physiol 8, 223–271. Ref Type: Abstract
Schiavone, M.T., Santos, R.A., Brosnihan, K.B., Khosla, M.C., and Ferrario, C.M. (1988) Release of vasopressin from the rat hypothalamo-neurohypophysial system by angiotensin-(1-7) heptapeptide. Proc Natl Acad Sci USA 85(11), 4095–4098.
Gallagher, P.E., and Tallant, E.A. (2004) Inhibition of human lung cancer cell growth by angiotensin-(1-7). Carcinogenesis 25(11), 2045–2052.
Menon, J., Soto-Pantoja, D.R., Callahan M.F. et al. (2007) Angiotensin-(1-7) inhibits growth of human lung adenocarcinoma xenografts in nude mice through a reduction in cyclooxygenase-2. Cancer Res 67(6), 2809–2815.
Ferrario, C.M., Barnes, K.L., Block C.H. et al. (1990) Pathways of angiotensin formation and function in the brain. Hypertension 15(2 Suppl), I13–I19.
Ferrario, C.M., Brosnihan, K.B., Diz, D.I. et al. (1991) Angiotensin-(1-7): a new hormone of the angiotensin system. Hypertension 18(5 Suppl), III126–III133.
Ferrario, C.M., and Iyer, S.N. (1998) Angiotensin-(1-7): a bioactive fragment of the renin-angiotensin system. Regul Pept 78(1–3), 13–18.
Santos, R.A., Simoes, E., Silva, A.C., Maric, C. et al. (2003) Angiotensin-(1-7) is an endogenous ligand for the G protein-coupled receptor mas. Proc Natl Acad Sci USA 100(14),8258–8263.
Averill, D.B., Ishiyama, Y., Chappell, M.C., and Ferrario, C.M. (2003) Cardiac angiotensin-(1-7) in ischemic cardiomyopathy. Circulation 108(17), 2141–2146.
Trask, A.J., Averill, D.B., Ganten, D., Chappell, M.C., and Ferrario, C.M. (2007) Primary role of angiotensin-converting enzyme-2 in cardiac production of angiotensin-(1-7) in transgenic Ren-2 hypertensive rats. Am J Physiol Heart Circ Physiol 292(6), H3019–H3024.
Ferreira, A.J., Santos, R.A., and Almeida, A.P. (2001) Angiotensin-(1-7): cardioprotective effect in myocardial ischemia/reperfusion. Hypertension 38(3 Pt 2), 665–668.
Ferreira, A.J., Santos, R.A., and Almeida, A.P. (2002) Angiotensin-(1-7) improves the post-ischemic function in isolated perfused rat hearts. Braz J Med Biol Res 35(9), 1083–1090.
Loot, A.E., Roks, A.J., Henning, R.H. et al. (2002) Angiotensin-(1-7) attenuates the development of heart failure after myocardial infarction in rats. Circulation 105(13), 1548–1550.
De Mello, W.C. (2004) Angiotensin (1-7) re-establishes impulse conduction in cardiac muscle during ischaemia-reperfusion. The role of the sodium pump. J Renin Angiotensin Aldosterone Syst 5(4), 203–208.
De Mello, W.C., Ferrario, C.M., and Jessup, J.A. (2007) Beneficial versus harmful effects of Angiotensin (1-7) on impulse propagation and cardiac arrhythmias in the failing heart. J Renin Angiotensin Aldosterone Syst 8(2), 74–80.
Grobe, J.L, Mecca, A.P., Mao, H., and Katovich, M.J. (2006) Chronic angiotensin-(1-7) prevents cardiac fibrosis in DOCA-salt model of hypertension. Am J Physiol Heart Circ Physiol 290(6), H2417–H2423.
Grobe, J.L., Mecca, A.P., Lingis, M. et al. (2007, Feb) Prevention of angiotensin ii-induced cardiac remodeling by angiotensin-(1-7). Am J Physiol Heart Circ Physiol 292(2), H736–H7420.
Iwata, M., Cowling, R.T., Gurantz, D. et al. (2005) Angiotensin-(1-7) binds to specific receptors on cardiac fibroblasts to initiate antifibrotic and antitrophic effects. Am J Physiol Heart Circ Physiol 289(6), H2356–H2363.
Tallant, E.A., Ferrario, C.M., and Gallagher, P.E. (2005) Angiotensin-(1-7) inhibits growth of cardiac myocytes through activation of the mas receptor. Am J Physiol Heart Circ Physiol 289(4), H1560–H1566.
Wang, L.J, He, J.G., Ma, H. et al. (2005) Chronic administration of angiotensin-(1-7) attenuates pressure-overload left ventricular hypertrophy and fibrosis in rats. Di Yi Jun Yi Da Xue Xue Bao 25(5), 481–487.
Ebermann, L., Spillmann, F., Sidiropoulos, M. et al. (2008) The angiotensin-(1-7) receptor agonist AVE0991 is cardioprotective in diabetic rats. Eur J Pharmacol 590(1–3), 276–280.
Wessel, N., Malberg, H., Heringer-Walther, S., Schultheiss, H.P., and Walther, T. (2007) The angiotensin-(1-7) receptor agonist AVE0991 dominates the circadian rhythm and baroreflex in spontaneously hypertensive rats. J Cardiovasc Pharmacol 49(2), 67–73.
Carvalho, M.B., Duarte, F.V., Faria-Silva, R. et al. (2007) Evidence for mas-mediated bradykinin potentiation by the angiotensin-(1-7) nonpeptide mimic AVE 0991 in normotensive rats. Hypertension 50(4), 762–767.
as-Peixoto, M.F., Santos, R.A., Gomes, E.R. et al. (2008) Molecular mechanisms involved in the angiotensin-(1-7)/mas signaling pathway in cardiomyocytes. Hypertension 52(3),542–548.
Elliott, P., Stamler, J., Nichols, R. et al. (1996) Intersalt revisited: further analyses of 24 hour sodium excretion and blood pressure within and across populations. Intersalt Cooperative Research Group. BMJ 312(7041), 1249–1253.
Sacks, F.M., Svetkey, L.P., Vollmer, W.M. et al. (2001) Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med 344(1), 3–10.
Stamler, J. (1997) The INTERSALT Study: background, methods, findings, and implications. Am J Clin Nutr 65(2 Suppl), 626S–642S.
Whelton, P.K., Appel, L.J., Espeland, M.A. et al. (1998) Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled trial of nonpharmacologic interventions in the elderly (TONE). TONE Collaborative Research Group. JAMA 279(11), 839–846.
Crackower, M.A., Sarao, R., Oudit, G.Y. et al. (2002) Angiotensin-converting enzyme 2 is an essential regulator of heart function. Nature 417(6891), 822–828.
Santos, R.A., Castro, C.H., Gava, E. et al. (2006) Impairment of in vitro and in vivo heart function in angiotensin-(1-7) receptor MAS knockout mice. Hypertension 47(5), 996–1002.
Xu, P., Costa-Goncalves, A.C., Todiras, M. et al. (2008) Endothelial dysfunction and elevated blood pressure in MAS gene-deleted mice. Hypertension 51(2), 574–580.
Iyer, S.N., Averill, D.B., Chappell, M.C., Yamada, K., Allred, A.J., and Ferrario, C.M. (2000) Contribution of angiotensin-(1-7) to blood pressure regulation in salt-depleted hypertensive rats. Hypertension 36(3), 417–422.
Nakamura, S., Averill, D.B., Chappell, M.C., Diz, D.I., Brosnihan, K.B., and Ferrario, C.M. (2003) Angiotensin receptors contribute to blood pressure homeostasis in salt-depleted SHR. Am J Physiol Regul Integr Comp Physio 284(1), R164–R173.
Burgelova, M., Kramer, H.J., Teplan, V., Thumova, M., and Cervenka, L. (2005) Effects of angiotensin-(1-7) blockade on renal function in rats with enhanced intrarenal Ang II activity. Kidney Int 67(4), 1453–1461.
Eatman, D., Wang, M., Socci, R.R., Thierry-Palmer, M., Emmett, N., and Bayorh MA. (2001) Gender differences in the attenuation of salt-induced hypertension by angiotensin (1-7). Peptides 22(6), 927–933.
Bayorh, M.A., Eatman, D., Walton, M., Socci, R.R., Thierry-Palmer, M., and Emmett, N. (2002) 1A-779 attenuates angiotensin-(1-7) depressor response in salt-induced hypertensive rats. Peptides 23(1), 57–64.
Roks, A.J., Nijholt, J., van Buiten, A., van Gilst, W.H., de Zeeuw, D., and Henning, R.H. (2004) Low sodium diet inhibits the local counter-regulator effect of angiotensin-(1-7) on angiotensin II. J Hypertens 22(12), 2355–2361.
Ferrario, C.M., Smith, R.D., Brosnihan, K.B. et al. (2002) Effects of omapatrilat on the renin angiotensin system in salt sensitive hypertension. Am J Hyperten 15, 557–564.
Doi, R., Masuyama, T., Yamamoto, K. et al. (2000) Development of different phenotypes of hypertensive heart failure: systolic versus diastolic failure in Dahl salt-sensitive rats. J Hypertens 18(1), 111–120.
du Cailar , C.G., Ribstein, J., and Mimran, A. (2002) Dietary sodium and target organ damage in essential hypertension. Am J Hypertens 15(3), 222–229.
Nishiyama, A., Yoshizumi, M., Rahman, M. et al. (2004) Effects of AT1 receptor blockade on renal injury and mitogen-activated protein activity in Dahl salt-sensitive rats. Kidney Int 65(3), 972–981.
Ono, K., Masuyama, T., Yamamotom K. et al. (2002) Echo Doppler assessment of left ventricular function in rats with hypertensive hypertrophy. J Am Soc Echocardiogr 15(2), 109–117.
Varagic, J., Frohlich, E.D., Diez, J. et al. (2006) Myocardial fibrosis, impaired coronary hemodynamics, and biventricular dysfunction in salt-loaded SHR. Am J Physiol Heart Circ Physiol 290(4), H1503–H1509.
Takeda, Y., Zhu, A., Yoneda, T., Usukura, M., Takata, H., and Yamagishi, M. (2007) Effects of aldosterone and angiotensin II receptor blockade on cardiac angiotensinogen and angiotensin-converting enzyme 2 expression in Dahl salt-sensitive hypertensive rats. Am J Hypertens 20(10), 1119–1124.
Hamming, I., van, G.H., Turner, A.J. et al. (2008) Differential regulation of renal angiotensin-converting enzyme (ACE) and ACE2 during ACE inhibition and dietary sodium restriction in healthy rats. Exp Physiol 93(5), 631–638.
Ferrario, C.M., Jessup, J., Gallagher, P.E. et al. (2005) Effects of renin-angiotensin system blockade on renal angiotensin-(1-7) forming enzymes and receptors. Kidney Int 68(5), 2189–2196.
Ferrario, C.M., Jessup, J., Chappell, M.C. et al. (2005) Effect of angiotensin-converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin-converting enzyme 2. Circulation 111(20), 2605–2610.
Jessup, J.A., Gallagher, P.E., Averill, D.B. et al. (2006) Effect of angiotensin II blockade on a new congenic model of hypertension derived from transgenic Ren-2 rats. Am J Physiol Heart Circ Physiol 291(5), H2166–H2172.
Kocks, M.J., Lely, A.T., Boomsma, F., de Jong, P.E., and Navis, G.(2005) Sodium status and angiotensin-converting enzyme inhibition: effects on plasma angiotensin-(1-7) in healthy man. J Hypertens 23(3), 597–602.
Welches, W.R., Brosnihan, K.B., and Ferrario, C.M. (1993) A comparison of the properties and enzymatic activities of three angiotensin processing enzymes: angiotensin converting enzyme, prolyl endopeptidase and neutral endopeptidase 24.11. Life Sci 52(18), 1461–1480.
Yang, H.Y., Erdos, E.G, and Chiang, T.S. (1968) New enzymatic route for the inactivation of angiotensin. Nature 218(5148), 1224–1226.
Donoghue, M., Hsieh, F., Baronas, E. et al. (2000) A novel angiotensin-converting enzyme-related carboxypeptidase (ACE2) converts angiotensin I to angiotensin 1-9. Circ Res 87(5), E1–E9.
Tipnis, S.R., Hooper, N.M., Hyde, R., Karran, E., Christie, G., and Turner, A.J. (2000) A human homolog of angiotensin-converting enzyme. Cloning and functional expression as a captopril-insensitive carboxypeptidase. J Biol Chem 275(43), 33238–33243.
Vickers, C., Hales, P., Kaushik, V. et al. (2002) Hydrolysis of biological peptides by human angiotensin-converting enzyme-related carboxypeptidase. J Biol Chem 277(17), 14838–14843.
Zisman, L.S., Meixell, G.E., Bristow, M.R., and Canver, C.C. (2003) Angiotensin-(1-7) formation in the intact human heart: in vivo dependence on angiotensin II as substrate. Circulation 108(14), 1679–1681.
Hamming, I., Timens, W., Bulthuis, M.L., Lely. A.T., Navis, G.J., and van Goor, H. (2004) Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol 203(2), 631–637.
Gembardt, F., Sterner-Kock, A., Imboden, H. et al. (2005) Organ-specific distribution of ACE2 mRNA and correlating peptidase activity in rodents. Peptides 26(7), 1270–1277.
Ishiyama, Y., Gallagher,P.E., Averill, D.B., Tallant, E.A., Brosnihan, K.B., and Ferrario, C.M. (2004) Upregulation of angiotensin-converting enzyme 2 after myocardial infarction by blockade of angiotensin II receptors. Hypertension 43(5), 970–976.
Gallagher, P.E., Ferrario, C.M., and Tallant, E.A. (2008) Regulation of ACE2 in Cardiac Myocytes and Fibroblasts. Am J Physiol Heart Circ Physiol 295(6), H2373–2379.
Gurley, S.B., Allred, A., Le, T.H. et al. (2006) Altered blood pressure responses and normal cardiac phenotype in ACE2-null mice. J Clin Invest 116(8), 2218–2225.
Yamamoto, K., Ohishi, M., Katsuya, T. et al. (2006) Deletion of angiotensin-converting enzyme 2 accelerates pressure overload-induced cardiac dysfunction by increasing local angiotensin II. Hypertension 47(4), 718–726.
Gurley, S.B., and Coffman T.M. (2008) Angiotensin-converting enzyme 2 gene targeting studies in mice: mixed messages. Exp Physiol 93(5), 538–542.
Mercure, C., Yogi, A., Callera, G.E. et al. (2008) Angiotensin(1-7) blunts hypertensive cardiac remodeling by a direct effect on the heart. Circ Res 103(11), 1319–1326.
Huentelman, M.J., Grobe, J.L., Vazquez, J. et al. (2005) Protection from angiotensin II-induced cardiac hypertrophy and fibrosis by systemic lentiviral delivery of ACE2 in rats. Exp Physiol 90(5), 783–790.
Der, S.S., Grobe, J.L., Yuan, L. et al. (2008) Cardiac overexpression of angiotensin converting enzyme 2 protects the heart from ischemia-induced pathophysiology. Hypertension 51(3), 712–718.
Burrell, L.M., Risvanis, J., Kubota, E. et al. (2005) Myocardial infarction increases ACE2 expression in rat and humans. Eur Heart J 26(4), 369–375.
Goulter, A.B., Goddard, M.J., Allen, J.C, and Clark, K.L. (2004) ACE2 gene expression is up-regulated in the human failing heart. BMC Med 2, 19.
Zisman, L.S., Keller, R.S., Weaver, B. et al. (2003) Increased angiotensin-(1-7)-forming activity in failing human heart ventricles: evidence for upregulation of the angiotensin-converting enzyme Homologue ACE2. Circulation 108(14), 1707–1712.
Epelman, S., Tang, W.H., Chen, S.Y., Van, L.F., Francis, G.S., and Sen, S. (2008) Detection of soluble angiotensin-converting enzyme 2 in heart failure: insights into the endogenous counter-regulatory pathway of the renin-angiotensin-aldosterone system. J Am Coll Cardiol 52(9), 750–754.
Lambert, D.W., Yarski, M., Warner, F.J. et al. (2005) Tumor necrosis factor-alpha convertase (ADAM17) mediates regulated ectodomain shedding of the severe-acute respiratory syndrome-coronavirus (SARS-CoV) receptor, angiotensin-converting enzyme-2 (ACE2). J Biol Chem 280(34), 30113–30119.
Fedak, P.W., Moravec, C.S., McCarthy, P.M. et al. (2006) Altered expression of disintegrin metalloproteinases and their inhibitor in human dilated cardiomyopathy. Circulation 113(2), 238–245.
Lew, R.A., Warner, F.J., Hanchapola, I. et al. (2008) Angiotensin-converting enzyme 2 catalytic activity in human plasma is masked by an endogenous inhibitor. Exp Physiol 93(5), 685–693.
Li, W., Moore, M.J, Vasilieva, N. et al. (2003) Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 426(6965), 450–454.
Campbell, D.J., and Habener, J.F. (1986) Angiotensinogen gene is expressed and differentially regulated in multiple tissues of the rat. J Clin Invest 78(1), 31–39.
Campbell, D.J. (1987) Circulating and tissue angiotensin systems. J Clin Invest 79(1), 1–6.
Danser, A.H., and Schalekamp, M.A. (1996) Is there an internal cardiac renin-angiotensin system? Heart 76(3 Suppl 3), 28–32.
Danser, A.H., van Kats, J.P., Verdouw, P.D., and Schalekamp, M.A. (1997) Evidence for the existence of a functional cardiac renin-angiotensin system in humans. Circulation 96(10), 3795–3796.
Danser, A.H., Saris, J.J., Schuijt, M.P., and van Kats, J.P. (1999) Is there a local renin-angiotensin system in the heart? Cardiovasc Res 44(2), 252–265.
Danser, A.H., van Kats, J.P., Admiraal, P.J. et al. (1994) Cardiac renin and angiotensins. Uptake from plasma versus in situ synthesis. Hypertension 24(1), 37–48.
Mackins, C.J., Kano, S., Seyedi, N. et al. (2006) Cardiac mast cell-derived renin promotes local angiotensin formation, norepinephrine release, and arrhythmias in ischemia/reperfusion. J Clin Invest 116(4), 1063–1070.
Ichihara, A., Hayashi, M., Kaneshiro, Y. et al. (2004) Inhibition of diabetic nephropathy by a decoy peptide corresponding to the "handle" region for nonproteolytic activation of prorenin. J Clin Invest 114(8), 1128–1135.
Ichihara, A., Kaneshiro, Y., and Suzuki, F. (2006) Prorenin receptor blockers: effects on cardiovascular complications of diabetes and hypertension. Expert Opin Investig Drugs 15(10), 1137–1139.
Ichihara, A., Kaneshiro, Y., Takemitsu, T. et al. (2006) Contribution of nonproteolytically activated prorenin in glomeruli to hypertensive renal damage. J Am Soc Nephrol 17(9), 2495–2503.
Nagata, S., Kato, J., Sasaki, K., Minamino, N., Eto, T., and Kitamura, K. (2006) Isolation and identification of proangiotensin-12, a possible component of the renin-angiotensin system. Biochem Biophys Res Commun 350(4), 1026–1031.
Jessup, J.A., Trask, A.J., Chappell, M.C. et al. (2008) Localization of the novel angiotensin peptide, angiotensin-(1-12), in heart and kidney of hypertensive and normotensive rats. Am J Physiol Heart Circ Physiol 294(6), H2614–H2618.
Trask, A.J., Jessup, J.A., Chappell, M.C., and Ferrario, C.M. (2008) Angiotensin-(1-12) is an alternate substrate for angiotensin peptide production in the heart. Am J Physiol Heart Circ Physiol 294(5), H2242–H2247.
Re, R. (2007) Intracellular renin-angiotensin system: the tip of the intracrine physiology iceberg. Am J Physiol Heart Circ Physiol 293(2), H905–H906.
Re, R.N. (2004) Mechanisms of disease: local renin-angiotensin-aldosterone systems and the pathogenesis and treatment of cardiovascular disease. Nat Clin Pract Cardiovasc Med 1(1), 42–47.
Re, R.N., and Cook, J.L. (2006) The intracrine hypothesis: an update. Regul Pept 133(1–3), 1–9.
Re, R.N., and Cook, J.L. (2007) Mechanisms of disease: intracrine physiology in the cardiovascular system. Nat Clin Pract Cardiovasc Med 4(10), 549–557.
Ferrario, C.M., Trask, A.J, and Jessup, J.A. (2005) Advances in biochemical and functional roles of angiotensin-converting enzyme 2 and angiotensin-(1-7) in regulation of cardiovascular function. Am J Physiol Heart Circ Physiol 289(6), H2281–H2290.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Humana Press, a part of Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Trask, A.J., Varagic, J., Ahmad, S., Ferrario, C.M. (2010). Angiotensin-(1-7), Angiotensin-Converting Enzyme 2, and New Components of the Renin Angiotensin System. In: DeMello, W., Frohlich, E. (eds) Renin Angiotensin System and Cardiovascular Disease. Contemporary Cardiology. Humana Press. https://doi.org/10.1007/978-1-60761-186-8_10
Download citation
DOI: https://doi.org/10.1007/978-1-60761-186-8_10
Published:
Publisher Name: Humana Press
Print ISBN: 978-1-60761-185-1
Online ISBN: 978-1-60761-186-8
eBook Packages: MedicineMedicine (R0)