
Abstract
The increasing proportion of elderly persons in the global population, and the implications of this trend in terms of increasing rates of chronic diseases such as type 2 diabetes mellitus, continue to be a cause for concern for clinicians and healthcare policy makers. The diagnosis and treatment of type 2 diabetes in the elderly is challenging, as age-related changes alter the clinical presentation of diabetic symptoms. Once type 2 diabetes is diagnosed, the principles of its management are similar to those in younger patients, but with special considerations linked to the increased prevalence of co-morbidities and relative inability to tolerate the adverse effects of medication and hypoglycaemia. In addition, there are many underappreciated factors complicating diabetes care in the elderly, including cognitive disorders, physical disability and geriatric syndromes, such as frailty, urinary incontinence and pain. Available oral antihyperglycaemic drugs include insulin secretagogues (meglitinides and sulfonylureas), biguanides (metformin), α-glucosidase inhibitors and thiazolidinediones. Unfortunately, as type 2 diabetes progresses in older persons, polypharmacy intensification is required to achieve adequate glycaemic control with the attendant increased risk of adverse effects as a result of age-related changes in drug metabolism. The recent introduction of the incretins, a group of intestinal peptides that enhance insulin secretion after ingestion of food, as novel oral antihyperglycaemic treatments may prove significant in older persons. The two main categories of incretin therapy currently available are: glucagon-like peptide-1 (GLP-1) analogues and inhibitors of GLP-1 degrading enzyme dipeptidyl peptidase-4 (DPP-4). The present review discusses the effect of aging on metabolic control in elderly patients with type 2 diabetes, the current treatments used to treat this population and some of the more recent advances in the field of geriatric type 2 diabetes. In particular, we highlight the efficacy and safety of GLP-1 and DPP-4 inhibitors, administered as monotherapy or in combination with other oral antihyperglycaemic agents, especially when the relevant clinical trials included older persons. There is strong evidence that use of incretin therapy, in particular, the DPP-4 inhibitors, could offer significant advantages in older persons. Clinical evidence suggests that the DPP-4 inhibitors vildagliptin and sitagliptin are particularly suitable for frail and debilitated elderly patients because of their excellent tolerability profiles. Importantly, these agents lack the gastrointestinal effects seen with metformin and α-glucosidase inhibitors taken alone, and have a low risk of the hypoglycaemic events commonly seen with agents that directly lower blood glucose levels.
Similar content being viewed by others


During the 20th century, the proportion of elderly persons comprising the populations of both developed and developing countries increased dramatically.[1] The population of persons aged ≥65 years in the US grew from around 3 million in 1900 to just over 37 million in 2006, with data from the American Community Survey showing that this age group constituted an estimated 12.5% of the population in that year.[2]
In parallel with this increase, there has been a rise in the prevalence of diabetes mellitus as the population has aged. The rate of occurrence of diabetes increases from 1% to 2% among persons aged 20–39 years to up to around 20% in those aged 60–74 years.[3] Most patients with diabetes have the type 2, or non-insulin-dependent, form of this disorder, and nearly half of all persons with type 2 diabetes are aged >65 years.[4] This association between an aging population and an increasing prevalence of type 2 diabetes gives rise to particular cause for concern when the costs to society are considered: the American Diabetes Association estimated that the direct and indirect medical expenditures attributable to diabetes in 2002 amounted to $US132 billion.[5] Direct medical expenditures amounted to $US91.8 billion, of which 51.8% was consumed by persons aged >65 years.
In this review we outline the effects of aging on metabolic control in patients with type 2 diabetes, and the difficulties faced by prescribers in choosing the most appropriate antihyperglycaemic treatments. We describe some of the antihyperglycaemic agents used in older persons, and focus on newer drugs with innovative mechanisms of action, most notably the dipeptidyl peptidase-4 [DPP-4] inhibitors sitagliptin and vildagliptin. We discuss the metabolic and clinical advantages of DPP-4 inhibition as reported in the literature and the potential for tolerability and quality-of-life benefits that may accrue from use of novel agents with physiologically based mechanisms of action in older persons who are likely to be frail or debilitated and who are likely to present with co-morbidities in addition to diabetes.
1. Particular Aspects of Type 2 Diabetes Mellitus in the Elderly
The diagnosis and treatment of type 2 diabetes in older persons poses unique challenges. Many age-related physiological changes can alter the clinical presentation of diabetes and make its diagnosis problematic. The onset of type 2 diabetes in the elderly is often slow and insidious, and symptoms typical of hyperglycaemia such as polyuria, polydipsia and polyphagia may be masked.[6] This is because the renal threshold for glucose increases with advancing age, and glucosuria may not be detected.[7] Polydipsia may be absent, the initial symptoms instead being dehydration with altered thirst perception and delayed fluid supplementation. Patients will often complain of changes such as dry eyes, dry mouth, confusion, urinary incontinence or more generalized symptoms such as weight loss or fatigue. Sometimes, type 2 diabetes may be discovered as a result of observing skin or genitourinary tract infections that are slow to heal. In many cases, however, type 2 diabetes will be diagnosed only through investigations of the better recognized micro- and macrovascular complications of the disease.[1]
Once type 2 diabetes is diagnosed in those aged ≥65 years, it is important to assess the patient’s overall health profile. There are a number of interacting and overlapping conditions common in the elderly that complicate the management of diabetes in this group. Apart from the obvious microvascular and macrovasular complications, there are also a number of underappreciated factors such as cognitive disorders, physical disabilities and geriatric syndromes as well as multi-morbidity and polypharmacy problems.
Both neuropathy and nephropathy are frequent in older patients with type 2 diabetes, and microalbuminuria may serve as an indication of increased mortality in this age group.[8] Diabetic retinopathy is also highly prevalent (around 40.3%) among middle-aged and older adults in the US and the risk of blindness in those aged >65 years is further increased by glaucoma, cataracts and macular degeneration.[9,10] In terms of macrovascular complications, elderly patients with type 2 diabetes frequently experience accelerated atherosclerosis leading to coronary artery disease, peripheral vascular disease and cerebrovascular accidents.[11,12] Indeed, recent research has even suggested that insulin resistance is itself an independent risk factor for congestive heart failure in those aged ≥70 years.[13]
Underappreciated factors complicating diabetes care in the elderly include cognitive disorders, physical disabilities such as impaired mobility and tremor, and geriatric syndromes such as frailty, urinary incontinence and pain. Although cognitive faculties commonly deteriorate in non-diabetic persons as they age, several studies have concluded that diabetes is uniquely associated with cognitive decline and doubles the risk of dementia among the elderly.[14–19] This has been linked to neurophysiological and structural changes in the brain that occur under conditions of poor glycaemic control and interfere with cognition.[20,21] In one community-based study, the ability of elderly diabetic patients to perform cognitive tests declined significantly over a 4-year period compared with age-matched healthy individuals.[17] Depression is also a cause for concern. Almost 20% of older adults in the primary care setting experience depression, and the rate of this disorder in those with diabetes is twice that observed in non-diabetic patients.[22] Such impairments have implications for the management of type 2 diabetes in older patients because they may result in confusion or forgetfulness that may interfere with the administration of medication and/or the following of dietary instructions.
The term ‘physical disability’ is wide ranging and, in the elderly, can encompass decreased mobility, blindness, arthritis, hand tremor and disability arising from falls and fractures. Type 2 diabetes is consistently reported as one of the strongest correlates of poor lower extremity performance, and older persons with the disease are at greater risk of loss of independence. The risk of developing poor physical function and severe disability is significantly higher in older persons with type 2 diabetes than in non-diabetic individuals even after adjustment for pre-existing complications.[23,24] A study in African Americans clearly showed that older diabetic men and women had an excessively high rate of disability compared with control individuals.[24] In particular, those with diabetes reported more falls and falls with injury.[24] This is in agreement with the results of several other studies showing that older diabetic women were at increased risk of falls and hip fractures compared with non-diabetic women.[25–27] With respect to other physical disabilities, research has shown that elderly persons with type 2 diabetes are two to three times less able to walk 400 m, prepare meals or do housework than their age- and sex-matched non-diabetic counterparts.[28]
The biological mechanisms by which diabetes is associated with a decline in lower extremity function may be linked to increased inflammatory states, reduced metabolic control and motor neuropathy, which in turn lead to disability through micro- and macrovascular complications and significant reductions in muscle mass. From a clinical perspective it is important to recognize that these factors may affect the individual’s ability to self-manage their diabetes in terms of medication use, performance of foot checks, preparation of suitable meals and exercise.
Common geriatric syndromes affecting older patients with type 2 diabetes include frailty, urinary incontinence and pain. Urinary incontinence was found to occur on a weekly basis in approximately 33% of women with diabetes or impaired glucose tolerance in the US National Health and Nutrition Examination Survey (NHANES).[29] Musculoskeletal pain also appears to be widespread among diabetic women and is independently associated with an increased likelihood of recurrent falls.[27] Frailty, however, is a more complex issue. Although there is currently no standard definition of age-related frailty, there is general agreement that it is a complex and multi-factorial condition characterized by the notion of risk due to instability.[30,31] In older persons with type 2 diabetes, the downward spiral of frailty is activated more quickly, but this syndrome is nevertheless reversible with appropriate interventions if it is tackled before it is allowed to progress beyond a certain level of severity.[32] The hazard for geriatric patients with type 2 diabetes is that frailty may compound some of the complications that are already associated with or caused by their diabetes. Frailty is in itself associated with cognitive impairment, reduced ability to perform activities of daily living and increased expression of inflammatory and coagulation markers (even after adjustment for cardiovascular disease and diabetes) that may contribute to the adverse microvascular effects of diabetes.[32–34]
A new category of obesity in older persons, sarcopenic obesity, has also been identified and is correlated with frailty.[35] Sarcopenic obesity is defined as a combination of excess weight and reduced muscle mass or strength due to age-related changes in body composition, as well as the increased prevalence of obesity, in the elderly.[35] Despite the increase in body fat and obesity that occurs with aging, there is a linear decrease in food intake over the life span that is related to decreased physical activity and altered metabolism. Thus, older frail persons, whether they be lean or obese, may fail to regulate food intake appropriately. This in turn has been linked to altered hormonal and neurotransmitter regulation and may increase the difficulties inherent in the control of type 2 diabetes.
The role of various co-morbidities and polypharmacy must also be considered before deciding how to treat elderly patients with type 2 diabetes: up to 70% of patients with type 2 diabetes have two or more co-morbidities.[36] Some conditions such as hypertension may exacerbate and accelerate diabetic complications (e.g. nephropathy and retinopathy). Multiple medical conditions require the simultaneous administration of multiple drugs and elderly patients may be more susceptible to hypoglycaemia caused by compromised renal function and altered drug elimination than younger patients. There is also a risk of adverse drug interactions: patients receiving five or more agents concurrently appear to be more susceptible to hypoglycaemia than those receiving fewer medications.[37]
2. Treatment of Type 2 Diabetes in the Elderly
As can be seen in section 1, the elderly population with type 2 diabetes is extremely heterogeneous, and there can be a number of complex factors to consider before deciding on a treatment plan. Treatment goals should focus not only on lowering hyperglycaemia but also on how to achieve maximum longevity in combination with optimal quality of life. The patient’s life expectancy, co-existing medical conditions or psychiatric disorders and willingness and ability to comply with the proposed treatment are important considerations. A stepwise approach that includes initial dietary and lifestyle changes is not usually successful in older persons; the majority will ultimately require drug therapy shortly after a diagnosis of diabetes.
Oral antihyperglycaemic agents available today include insulin secretagogues (meglitinides and sulfonylureas), biguanides (metformin), α-glucosidase inhibitors and thiazolidinediones. Although such agents have established short-term beneficial effects, none has successfully demonstrated a lasting effect on β-cell dysfunction. Unfortunately, as type 2 diabetes progresses, polypharmacy intensification is normally required to maintain adequate glycaemic control, carrying with it the increased risk of adverse events, especially in older persons. In addition, changes in the normal metabolism of drugs with age and the development of other pathologies in elderly patients make it important that these drugs are prescribed with care. A new direction in the treatment of type 2 diabetes is the utilization of incretin hormones as therapeutic agents, either in the form of subcutaneous injections of glucagon-like peptide-1 (GLP-1) receptor agonists or as orally administered inhibitors of DPP-4.[38,39]
3. Potential Role of Incretin Hormones in Elderly Patients with Type 2 Diabetes
It has long been known that the insulin response to oral glucose is greater than that for intravenous glucose at matching blood glucose levels.[40] This is known as the ‘incretin effect’. The gastrointestinal hormones responsible for evoking the insulin response are known as incretins, the most important of which are glucose-dependent insulinotropic peptide (GIP) and GLP-1. In healthy individuals, plasma levels of these incretins are low in the fasted state, but rise rapidly following the ingestion of food and then decrease just as rapidly due to degradation by the enzyme DPP-4.[41] At a cellular level, GIP binds to G-protein-coupled receptors on pancreatic β cells while GLP-1 binds to both α and β cells, thereby improving their sensitivity to glucose.[42] This stimulates insulin secretion within the β cells and attenuates glucagon secretion by the α cells during postprandial hyperglycaemia. Importantly, GLP-1 also stimulates β-cell proliferation, delays gastric emptying and promotes a sense of satiety, while both GIP and GLP-1 enhance β-cell survival by inhibiting apoptosis.[43–45]
In patients with type 2 diabetes, much of the insulinotropic potency of GIP is lost and GLP-1 secretion is impaired, while GLP-1 action remains relatively preserved.[46–48] It is this last factor that makes the incretin system a potential target for therapy in older individuals with type 2 diabetes. Infusion or subcutaneous injection of exogenous GLP-1 lowers blood glucose, improves insulin secretion and sensitivity and reduces glycosylated haemoglobin (HbA1c) levels in older patients with diabetes, but its effect is short-lived, and repeated administration is required to maintain these effects.[6,49–52] Because the effects of GLP-1 are glucose dependent, the counter-regulatory release of glucagon in response to hypoglycaemia is maintained.[53] Other potential benefits of GLP-1 for the elderly include positive cardiovascular effects such as increased myocardial uptake of glucose, improved ventricular function, enhanced myocardial reperfusion and enhanced endothelial function.[54–56] Preliminary data further suggest that learning and memory are improved by activating or upregulating GLP-1 receptors in the CNS.[57]
4. Incretin Therapy in Elderly Patients with Type 2 Diabetes
4.1 Glucagon-Like Peptide-1 Analogues
Two main categories of incretin therapy are currently available: GLP-1 analogues and DPP-4 inhibitors. GLP-1 analogues are synthetic peptides or proteins that are resistant to degradation by DPP-4 and have more favourable pharmacokinetic properties than exogenous GLP-1. Exenatide is currently the only GLP-1 analogue available in the US, although a new GLP-1 analogue, liraglutide, is expected to be launched within the next couple of years.
4.1.1 Exenatide
Exenatide is approved as an adjunctive treatment for patients with type 2 diabetes who have suboptimal glycaemic control despite taking a sulfonylurea and/or metformin. Unfortunately, few data regarding the efficacy of these agents specifically in elderly patients with type 2 diabetes have been published. Exenatide is a potent degradation-resistant agonist of the mammalian GLP-1 receptor with a circulating half-life of 60–90 minutes after subcutaneous injection.[58] All exenatide trials in patients already taking a sulfonylurea, metformin or both have so far been conducted in middle-aged patients (mean age 52–60 years), in whom twice-daily adjunctive therapy (at doses of 5 or 10 µg) improved glycaemic control and decreased bodyweight.[59–62] Exenatide was well tolerated, with the most common adverse events being gastrointestinal, usually mild-to-moderate nausea (most common), vomiting and diarrhoea.[59–61]
These placebo-controlled phase III studies of exenatide included between 336 and 733 patients, most of whom were overweight, with inadequate glycaemic control on their existing medication. Exenatide was self-administered by subcutaneous injection in the 15 minutes preceding morning and evening meals. After 30 weeks’ therapy, mean changes in the primary endpoint of HbA1c were consistently significantly better with exenatide than with placebo, with relative reductions of 9.4–10% documented in patients injecting 10 µg twice daily. Exenatide treatment was also associated with progressive and dose-dependent weight loss. In two further phase III studies of 26[63] or 52[64] weeks’ duration, exenatide had similar antihyperglycaemic efficacy to once-daily insulin glargine or twice-daily insulin aspart in patients with type 2 diabetes inadequately controlled by metformin plus a sulfonylurea.
4.1.2 Liraglutide
Research into liraglutide is still ongoing, and, while data from phase II and III trials show that this agent also improves plasma glucose and HbA1c without increasing the risk of hypoglycaemia, no substudies have evaluated its efficacy in older patients.[65–67] Like exenatide, liraglutide is a potent and degradation-resistant analogue of GLP-1 that is given by subcutaneous injection, but it has a prolonged half-life conferred by albumin binding and the formation of micellar-like aggregates in the subcutis.[68] These properties result in prolongation of absorption and elimination in addition to DPP-4 stability, thereby permitting once-daily administration.
While early phase II trials of liraglutide were conducted using dosages of up to 0.75 mg/day,[66,69,70] more recent studies have used weekly escalating dosage titration regimens of up to 2 mg/day. Data from a recent randomized, double-blind, parallel-group trial in 165 patients showed reductions in mean fasting plasma glucose levels of 2.7–3.4 mmol/L with liraglutide 0.65, 1.25 or 1.9 mg compared with placebo over 14 weeks.[67] Levels of HbA1c were reduced by up to 1.75%, together with prevention of weight gain or loss of bodyweight compared with placebo. Data pertaining to subgroups of patients such as the elderly are anticipated as clinical study programmes for exenatide and liraglutide progress.
4.2 Dipeptidyl Peptidase-4 Inhibitors
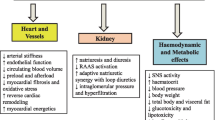
DPP-4 inhibitors increase endogenous GLP-1 levels by preventing enzymatic degradation of circulating GLP-1 (figure 1). There are three DPP-4 inhibitors in active phase III development or above: sitagliptin (the only launched product), vildagliptin and saxagliptin.

Effects of dipeptidyl peptidase-4 (DPP-4) inhibitors on plasma glucose levels (adapted from Unger[71]). ↑ indicates increased; ↓ indicates decreased.
4.2.1 Sitagliptin
Sitagliptin is an oral DPP-4 inhibitor that improves glycaemic control in patients with type 2 diabetes by inhibiting DPP-4 inactivation of GLP-1 and GIP.[72] This novel agent has been investigated as monotherapy and in combination with other antihyperglycaemic drugs in large, well designed, phase III trials, but as with the GLP-1 analogues, the majority of the data available for sitagliptin in type 2 diabetes involve middle-aged patients (mean age 54–57 years). No subgroup analyses in the elderly have been published, but in younger patients sitagliptin monotherapy is similar to placebo in its antihyperglycaemic effects and in the incidence of hypoglycaemia.[72]
Monotherapy with sitagliptin produces significant improvements in glycaemic control compared with placebo. In dose-ranging studies involving a total of 1295 patients, sitagliptin 10–100 mg/day produced dosage-dependent reductions in HbA1c of up to 0.8%, together with reductions in other markers of glycaemic control, after 12 weeks of therapy.[73,74] These encouraging results were supported by phase II data in 151 Japanese patients, which showed significantly greater reductions in mean HbA1c (–0.65% vs +0.41% with placebo) and 2-hour postprandial glucose (–3.8 vs +0.7 mmol/L with placebo) levels compared with baseline with sitagliptin 100 mg/day.[75] Two large phase III studies have assessed sitagliptin 100 or 200 mg/day for 18 weeks in 521 patients[76] or for 24 weeks in 741 patients,[77] and a 12-week trial has been carried out in 91 patients with renal impairment in addition to type 2 diabetes.[78] Sitagliptin was consistently associated with significantly better glycaemic control and higher rates of achievement of glycaemic control goals than placebo in all of these studies.
In addition, an 8-week crossover trial[79] and two 24-week phase III studies[80,81] have demonstrated the efficacy of addition of sitagliptin to pioglitazone (n = 353) or metformin (n = 473) in patients with inadequate glycaemic control on their existing medication. Sitagliptin 100 mg/day has also been compared with glipizide (up to 20 mg/day) as additional therapy in 793 per-protocol patients inadequately controlled by metformin treatment in a 52-week study.[82] At the end of the two 24-week trials,[80,81] HbA1c levels were significantly lower with sitagliptin 100 mg once daily than with placebo when added to pioglitazone or metformin. Moreover, addition of sitagliptin to existing therapy approximately doubled the numbers of patients achieving glycaemic control goals. In the 52-week study,[82] sitagliptin was as effective as glipizide when added to existing metformin therapy. The 8-week crossover trial[79] showed that addition of sitagliptin 50 mg twice daily to ongoing metformin therapy improved 24-hour glycaemic control and β-cell function.
Although none of these trials of sitagliptin focused specifically on elderly patients (the mean age in the studies discussed ranged from 54 to 57 years), subgroup analyses in monotherapy trials indicated consistency of effect of sitagliptin whether patients were aged above or below 65 years.[76,77] Furthermore, the mean age of patients enrolled in the trial of patients with impaired renal function in addition to type 2 diabetes[78] was 68 years. In this study, sitagliptin was given at dosages of 50 and 25 mg/day in patients with moderate and severe renal impairment (including those with end-stage renal disease requiring haemodialysis), respectively. Improvements in glycaemic control in this trial (figure 2), which tended to recruit older persons, were similar to those seen in other trials involving patients without renal disease. Across all trials, sitagliptin was well tolerated, with neutral or beneficial effects on bodyweight.

Mean changes from baseline in glycosylated haemoglobin (HbA1c) and fasting plasma glucose (FPG) levels in a phase III study of 91 patients with type 2 diabetes mellitus and chronic renal disease.[78] Patients received sitagliptin 25 or 50 mg/day in this dosage-adjusted trial; results after 12 weeks’ treatment are shown pooled for both dosages.
4.2.2 Vildagliptin
Vildagliptin, a long-acting and potent orally administered DPP-4 inhibitor, has been found to significantly increase fasting and postprandial GLP-1 and GIP levels, improve the sensitivity of glucose to insulin and glucagon secretion and decrease both fasting and postprandial glucose in patients of any age with type 2 diabetes.[83,84] Clinical data in 107 patients with type 2 diabetes showed vildagliptin to be statistically significantly superior to placebo in improving glycaemic control in patients continuing on metformin therapy.[85] In this 12-week, randomized, double-blind, placebo-controlled study, vildagliptin 50 mg once daily was added to existing therapy with metformin 1.5–3 g/day. The mean HbA1c level decreased by 0.6% in patients randomized to vildagliptin, whereas those receiving placebo showed no mean change from baseline. Mean prandial glucose and fasting plasma glucose levels were also reduced significantly by vildagliptin treatment relative to placebo. The difference between vildagliptin and placebo was maintained for 1 year in an open-label extension to this study.[85] Other data have shown sustained efficacy with slight non-inferiority but better tolerability compared with metformin after 1 year of therapy with vildagliptin 50 mg twice daily or 100 mg once daily.[86] Vildagliptin was also as effective as rosiglitazone in a monotherapy study,[87] and produced significant reductions in HbA1c levels with potential mitigation of gastrointestinal adverse effects when administered in combination with metformin.[88] As with sitagliptin, these trials have shown vildagliptin to be well tolerated, with neutral or potentially beneficial effects on bodyweight.
Unlike other newer agents for use in patients with type 2 diabetes, recent information regarding the efficacy of vildagliptin in patients aged ≥65 years is available.[89–92] Pratley et al.[90] pooled data from five monotherapy studies that compared the efficacy and tolerability of vildagliptin (50 mg twice daily or 100 mg daily) with placebo over the course of 24 weeks. Relative to younger patients, older vildagliptin recipients experienced similar reductions in HbA1c, fasting plasma glucose and bodyweight (table I). Furthermore, vildagliptin was well tolerated and hypoglycaemic events were rare (table II). Baron et al.[92] pooled data to investigate the effects of vildagliptin in treatment-naive elderly patients in 174 participants who were administered vildagliptin monotherapy for either 24 or 52 weeks. Following treatment, mean HbA1c levels were reduced by approximately 1% from baseline levels, similar to changes observed in patients aged <65 years. As with the previous analysis, the incidence of hypoglycaemia was below 1%.[92]

Efficacy of treatment with vildagliptin for 24 weeks in older versus younger patients with type 2 diabetes mellitus[89]

Tolerability of treatment with vildagliptin for 24 weeks in older versus younger patients with type 2 diabetes mellitus[89] a
4.2.3 Other Dipeptidyl Peptidase-4 Inhibitors
Other DPP-4 inhibitors in clinical development include saxagliptin[93] and denagliptin.[94] Saxagliptin is currently under consideration by the US FDA as well as the European Medicines Agency for approval, while denagliptin is undergoing phase II and phase III clinical trials at the time of writing. Clinical data specific to the elderly are not available at this early stage for these drugs.
5. Other Treatments that May Affect Incretins
The α-glucosidase inhibitors exert their antihyperglycaemic effects by inhibiting the breakdown of complex carbohydrates in the small bowel. However, these agents (which include acarbose and miglitol) have also been associated with exaggerated and sustained postprandial GLP-1 responses in healthy persons,[95,96] in patients with type 2 diabetes poorly controlled by dietary and sulfonylurea therapy[97] and in obese patients with controlled type 2 diabetes.[98] Miglitol and acarbose have also been associated with suppression of GIP secretion.[95,97–99] Data are not unequivocal, however: one study of ten patients with type 2 diabetes failed to demonstrate enhancement of GLP-1 release by acarbose.[99] Interestingly, the gastrointestinal lipase inhibitor orlistat, which has been used to promote weight loss and thereby improve glycaemic control in obese patients with type 2 diabetes,[100] has also been shown to increase postprandial GLP-1 release.[101]
Of particular interest in the present context are the results of a study conducted to determine the response of GLP-1 to acarbose in patients aged >65 years with type 2 diabetes.[102] In this study, 10 individuals were given a standardized test meal with or without acarbose 25, 50 or 100 mg. Under these experimental conditions, the peak antihyperglycaemic effect of acarbose was seen with the 25-mg dose. Serum postprandial insulin and triglyceride levels were not altered to any relevant extent by acarbose treatment. Postprandial serum GLP-1 levels rose significantly in two patients only, and only after treatment with acarbose 100 mg. No correlations were found between serum levels of GLP-1, insulin or glucose. The authors concluded that the antihyperglycaemic effect of acarbose could be maximized only with low doses in elderly patients with type 2 diabetes, and that GLP-1 is unlikely to contribute to the clinical efficacy of the drug in these persons. Moreover, the gastrointestinal adverse effects of the α-glucosidase inhibitors (which include flatulence, abdominal discomfort and diarrhoea) are usually significant and may be particularly problematic in the elderly.[1]
6. Conclusion
Until recently, all oral antihyperglycaemic agents have been directly aimed at correcting hyperglycaemia, while indirectly protecting against diabetic complications. Use of agents targeting the incretin hormones, in particular the DPP-4 inhibitors, with mechanisms of action that target clearly identified physiological pathways, could offer significant advantages in older persons who may be frail and therefore unable to tolerate more aggressive or poorly tolerated therapeutic approaches. Even though such drugs are currently relatively expensive, the implications of use of these agents in older persons suggest that their use would be highly rational in this context.
Importantly, evidence suggests that drugs such as vildagliptin and sitagliptin are particularly suitable for frail and debilitated elderly patients: these agents have excellent tolerability profiles and lack the gastrointestinal effects seen with metformin and the α-glucosidase inhibitors taken alone, and have a low risk of the hypoglycaemia that is commonly seen with agents that directly lower blood glucose levels. However, hypoglycaemic events may have a higher incidence when DPP-4 inhibitors are combined with glucose-lowering agents such as sulphonylureas at 100 mg/day.[103] Elderly patients may also be less inclined or less able than younger persons to undertake physical activity in order to minimize gains in bodyweight, and the neutral or beneficial effects in this respect that have been reported with the DPP-4 inhibitors to date are therefore of considerable interest. The good tolerability and efficacy of sitagliptin in patients with renal impairment are likely to be highly relevant in the elderly, and data relating specifically to the use of vildagliptin in this age group confirm the potential of this group of drugs in older patients. The GLP-1 analogues exenatide and liraglutide may also be capable of conferring similar benefits, but these agents are limited by their need for subcutaneous injection, and neither agent has been studied specifically in the elderly.
In light of these observations, future studies should focus on the benefits of DPP-4 inhibition that are additional to and likely to augment improvements in glycaemic control, and that are likely to lead to enhanced quality of life in elderly patients. Indeed, long-term treatment aimed at specific outcomes will determine the full potential of these agents, with their physiologically based mechanism of action, in older persons with type 2 diabetes, many of whom are overweight and/or frail with co-existing medical conditions.
References
Rosenstock J. Management of type 2 diabetes mellitus in the elderly: special considerations. Drugs Aging 2001; 18(1): 31–44
US Census Bureau. American FactFinder: United States S0101. Age and sex: data set: 2006 American Community Survey [online]. Available from URL: http://factfinder.census.gov/servlet/STTable?._bm=y&geo_id=01000US&qr_name=ACS_2006_EST_G00_S0101&ds_name=ACS_2006_EST_G00_&redoLog=false. [Accessed 2007 Oct 31]
Harris MI, Flegal KM, Cowie CC, et al. Prevalence of diabetes, impaired fasting glucose, and impaired glucose tolerance in U.S. adults: the third National Health and Nutrition Examination Survey, 1988–1994. Diabetes Care 1998; 21: 518–24
Gossain VV, Carella MJ, Rovner DR. Management of diabetes in the elderly: a clinical perspective. J Assoc Acad Minority Phys 1994; 5: 22–31
American Diabetes Association. Economic costs of diabetes in the U.S. in 2002. Diabetes Care 2003; 26: 917–32
Meneilly GS, Tessier D. Diabetes in elderly adults. J Gerontol A Biol Sci Med Sci 2001; 56(1): M5–13
Meneilly GS. Diabetes. In: Evans JG, Williams TF, Beattie BL, et al., editors. Oxford textbook of geriatric medicine. 2nd ed. New York: Oxford University Press, 2000: 210–7
Damsgaard EM, Froland A, Jorgensen OD, et al. Microalbumin-uria as a predictor of increased mortality in elderly people. BMJ 1990; 300: 297–8
Kempen JH, O’Colmain BJ, Leske MC, et al. The prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol 2004; 122(4): 522–63
Lee PP, Feldman ZW, Ostermann J, et al. Longitudinal prevalence of major eye diseases. Arch Ophthalmol 2003; 121(9): 1303–10
Cohen DL, Neil HAW, Thorogood M, et al. A population based study of the incidence of complications associated with type 2 diabetes in the elderly. Diabet Med 1991; 8: 928–33
Dornan TL, Peck GM, Dow JDC, et al. A community survey of diabetes in the elderly. Diabet Med 1992; 9: 860–5
Ingelsson E, Sundstrom J, Arnlov J, et al. Insulin resistance and risk of congestive heart failure. JAMA 2005; 294(3): 334–41
Gregg EW, Yaffe K, Cauley JA, et al. Is diabetes associated with cognitive impairment and cognitive decline among older women? Study of Osteoporotic Fractures Research Group. Arch Intern Med 2000 Jan 24; 160(2): 174–80
Haan MN, Shemanski L, Jagust WJ, et al. The role of APOE epsilon4 in modulating effects of other risk factors for cognitive decline in elderly persons. JAMA 1999; 282: 40–6
Knopman D, Boland LL, Mosley T, et al. Atherosclerosis Risk in Communities (ARIC) study investigators: cardiovascular risk factors and cognitive decline in middle-aged adults. Neurology 2001; 56: 42–8
Fontbonne A, Berr C, Ducimetiere P, et al. Changes in cognitive abilities over a 4-year period are unfavorably affected in elderly diabetic subjects: results of the Epidemiology of Vascular Aging Study. Diabetes Care 2001; 24: 366–70
Ott A, Stolk RP, Hofman A, et al. Association of diabetes mellitus and dementia: the Rotterdam Study. Diabetologia 1996; 39: 1392–7
Luchsinger JA, Tang M, Stern Y, et al. Diabetes mellitus and risk of Alzheimer’s disease and dementia with stroke in a multiethnic cohort. Am J Epidemiol 2001; 154: 635–41
Biessels GJ, van der Heide LP, Kamal A, et al. Ageing and diabetes: implications for brain function. Eur J Pharmacol 2002; 441(1–2): 1–14
Abbatecola AM, Rizzo MR, Barbieri M, et al. Postprandial plasma glucose excursions and cognitive functioning in aged type 2 diabetics. Neurology 2006; 67(2): 235–40
Feil D, Weinreb J, Sultzer D. Psychiatric disorders and psychotropic medication use in elderly persons with diabetes. Ann Long Term Care 2006; 14(7): 39–47
Maty SC, Fried LP, Volpato S, et al. Patterns of disability related to diabetes mellitus in older women. J Gerontol A Biol Sci Med Sci 2004; 59(2): 148–53
Miller DK, Lui LY, Perry 3rd HM, et al. Reported and measured physical functioning in older inner-city diabetic African Americans. J Gerontol A Biol Sci Med Sci 1999; 54(5): M230–6
Gregg EW, Mangione CM, Cauley JA, et al. Diabetes and incidence of functional disability in older women. Diabetes Care 2002; 25: 61–7
Schwartz AV, Sellmeyer DE, Ensrud KE, et al. Older women with diabetes have an increased risk of fracture: a prospective study. J Clin Endocrinol Metab 2001; 86: 32–8
Volpato S, Leveille SG, Blaum C, et al. Risk factors for falls in older disabled women with diabetes: the Women’s Health and Aging Study. J Gerontol A Biol Sci Med Sci 2005; 60(12): 1539–45
Gregg EW, Beckles GL, Williamson DF, et al. Diabetes and physical disability among U.S. adults. Diabetes Care 2000; 23: 1272–7
Brown JS, Vittinghoff E, Lin F, et al. Prevalence and risk factors for urinary incontinence in women with type 2 diabetes and impaired fasting glucose: findings from the National Health and Nutrition Examination Survey (NHANES) 2001–2002. Diabetes Care 2006; 29(6): 1307–12
Fried LP, Tangen CM, Walston J, et al. Cardiovascular Health Study Collaborative Research Group: frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56(3): M146–56
Rockwood K, Hogan DB, MacKnight C. Conceptualisation and measurement of frailty in elderly people. Drugs Aging 2000; 17(4): 295–302
Vanitallie TB. Frailty in the elderly: contributions of sarcopenia and visceral protein depletion. Metabolism 2003; 52 (10 Suppl. 2): 22–6
Cigolle CT, Langa KM, Kabeto MU, et al. Geriatric conditions and disability: the Health and Retirement Study. Ann Intern Med 2007; 147(3): 156–64
Walston J, McBurnie MA, Newman A, et al. Frailty and activation of the inflammation and coagulation systems with and without clinical comorbidities: results from the Cardiovascular Health Study. Arch Intern Med 2002; 162(20): 2333–41
Baumgartner RN, Wayne SJ, Waters DL, et al. Sarcopenic obesity predicts instrumental activities of daily living disability in the elderly. Obes Res 2004; 12(12): 1995–2004
Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med 2002; 162(20): 2269–76
Shorr RI, Ray WA, Daugherty JR, et al. Incidence and risk factors for serious hypoglycemia in older persons using insulin or sulfonylureas. Arch Intern Med 1997; 157: 1681–6
Inzucchi SE, McGuire DK. New drugs for the treatment of diabetes: part II. Incretin-based therapy and beyond. Circulation 2008 Jan 29; 117(4): 574–84
Mathieu C, Bollaerts K. Antihyperglycaemic therapy in elderly patients with type 2 diabetes: potential role of incretin mimetics and DPP-4 inhibitors. Int J Clin Pract Suppl Aug 2007; (154): 29–37
Gallwitz B. Glucagon-like peptide-1-based therapies for the treatment of type 2 diabetes mellitus. Treat Endocrinol 2005; 4(6): 361–70
Orskov C, Wettergren A, Holst JJ. Biological effects and metabolic rates of glucagon-like peptide-17-36 amide on glucagonlike peptide-1 7–37 in healthy subjects are indistinguishable. Diabetes 1993; 42: 658–61
Drucker DJ, Nauck M. The incretin system: glucagon-like pep-tide 1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet 2006; 368: 1696–705
MacDonald PE, El-Kholy W, Riedel MJ, et al. The multiple actions of GLP-1 on the process of glucose-stimulated insulin secretion. Diabetes 2002; 51Suppl. 3: S434–42
List JF, Gabener JF. Glucagon-like peptide 1 agonists and the development and growth of pancreatic beta cells. Am J Physiol Endocrinol Metab 2004; 266: E875–81
Brubaker PL, Drucker DJ. Minireview: glucagon-like peptides regulate cell proliferation and apoptosis in the pancreas, gut, and central nervous system. Endocrinology 2004; 145: 2653–9
Meier JJ, Hucking K, Holst JJ, et al. Reduced insulinotropic effect of gastric inhibitory polypeptide in first-degree relatives of patients with type 2 diabetes. Diabetes 2001; 50: 2497–504
Gutniak M, Orskov C, Holst JJ, et al. Antidiabetogenic effect of glucagon-like peptide-1 [7–36]amide in normal subjects and patients with diabetes mellitus. New Engl J Med 1992; 326: 1316–22
Nathan DM, Schreiber E, Fogel H, et al. Insulinotropic action of glucagon-like peptide I-[7–37] in diabetic and nondiabetic subjects. Diabetes Care 1992; 15: 270–6
Meneilly GS, Greig N, Tidesley H, et al. Effects of 3 months of continuous subcutaneous administration of glucagon-like peptide 1 in elderly patients with type 2 diabetes. Diabetes Care 2003; 26: 2835–41
Meneilly GS, Mcintosh CH, Pederson RA, et al. Effect of glucagon-like peptide 1 on non-insulin-mediated glucose uptake in the elderly patient with diabetes. Diabetes Care 2001; 24: 1951–6
Meneilly GS, Mcintosh CH, Pederson RA, et al. Glucagon-like peptide-1 [7–37] augments insulin release in elderly patients with diabetes. Diabetes Care 2001; 24: 964–5
Meneilly GS, Mcintosh CH, Pederson RA, et al. Glucagon-like peptide-1 [7–37] augments insulin-mediated glucose uptake in elderly patients with diabetes. J Gerontol A Biol Sci Med Sci 2001; 56: M681–5
Nauck MA, Heimesaat MM, Behle K, et al. Effects of glucagon-like peptide 1 on counterregulatory hormone responses, cognitive functions and insulin secretion during hyperinsulinemic, stepped hypoglycemic clamp experiments in healthy volunteers. J Clin Endocrinol Metab 2002; 87: 1239–46
Nikolaidis LA, Elahi D, Hentosz T, et al. Recombinant glucagon-like peptide-1 increases myocardial glucose uptake and improves left ventricular performance in conscious dogs with pacing-induced dilated cardiomyopathy. Circulation 2004; 110: 955–61
Nikolaidis LA, Doverspike A, Hentosz T, et al. Glucagon-like peptide-1 limits myocardial stunning following brief coronary occlusion and reperfusion in conscious canines. J Pharmacol Exp Ther 2005; 312(1): 303–8
Nystrom T, Gutniak MK, Zhang Q, et al. Effects of glucagon-like peptide-1 on endothelial function in type 2 diabetes patients with stable coronary artery disease. Am J Physiol Endocrinol Metab 2004; 287: E1209–15
During MJ, Lei C, Zuzga DS, et al. Glucagon-like peptide-1 receptor is involved in learning and neuroprotection. Nat Med 2003; 9(9): 1173–9
Kolterman OG, Kim DD, Shen L, et al. Pharmacokinetics, pharmacodynamics, and safety of exenatide in patients with type 2 diabetes mellitus. Am J Health Syst Pharm 2005; 62: 173–81
Buse JB, Henry RR, Han J, et al. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes. Diabetes Care 2004; 27(11): 2628–35
DeFronzo RA, Ratner RE, Han J, et al. Effects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in patients with type 2 diabetes. Diabetes Care 2005; 28(5): 1092–100
Kendall DM, Riddle MC, Rosenstock J, et al. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in patients with type 2 diabetes treated with metformin and a sulfonylurea. Diabetes Care 2005; 28(5): 1083–91
Cvetković RS, Plosker GL. Exenatide: a review of its use in patients with type 2 diabetes mellitus (as an adjunct to metformin and/or a sulfonylurea). Drugs 2007; 67(6): 935–54
Heine RJ, Van Gaal LF, Johns D, et al. Exenatide versus insulin glargine in patients with suboptimally controlled type 2 diabetes: a randomized trial. Ann Intern Med 2005; 143: 559–69
Nauck MA, Duran S, Kim D, et al. A comparison of twice-daily exenatide and biphasic insulin aspart in patients with type 2 diabetes who were suboptimally controlled with sulfonylurea and metformin: a non-inferiority study. Diabetologia 2007; 50: 259–67
Degn KB, Juhl CB, Sturis J, et al. One week’s treatment with the long-acting glucagon-like peptide 1 derivative liraglutide (NN2211) markedly improves 24-h glycemia and α- and α-cell function and release in patients with type 2 diabetes. Diabetes 2004; 53(5): 1187–94
Madsbad S, Schmitz O, Ranstam J, et al. Improved glycemic control with no weight increase in patients with type 2 diabetes after once-daily treatment with the long-acting glucagon-like peptide 1 analog liraglutide (NN2211): a 12-week, doubleblind, randomized, controlled trial. Diabetes Care 2004; 27(6): 1335–42
Visbøll T, Zdravkovic M, Le-Thi T, et al. Liraglutide significantly improves glycemic control and lowers body weight without risk of either major or minor hypoglycemic episodes in subjects with type 2 diabetes [abstract no. 115-OR]. Diabetes 2006; 55Suppl. 1: 27–8
Vilsbøll T. Liraglutide: a once-daily GLP-1 analogue for the treatment of type 2 diabetes mellitus. Expert Opin Investig Drugs 2007; 16: 231–7
Feinglos MN, Saad MF, Pi-Sunyer FX, et al. Effects of liraglutide (NN2211), a long-acting GLP-1 analogue, on glycemic control and bodyweight in subjects with type 2 diabetes. Diabet Med 2005; 22: 1016–23
Harder H, Nielsen L, Tu DT, et al. The effect of liraglutide, a long-acting glucagon-like peptide 1 derivative, on glycemic control, body composition, and 24-h energy expenditure in patients with type 2 diabetes. Diabetes Care 2004; 27: 1915–21
Unger RH. Alpha- and beta-cell interrelationships in health and disease. Metabolism 1974; 23: 581–93
Lyseng-Williamson KA. Sitagliptin. Drugs 2007; 67(4): 587–97
Hanefeld M, Herman G, Mickel C, et al. Effect of MK-0431, a dipeptidyl peptidase IV inhibitor, on glycemic control after 12 weeks in patients with type 2 diabetes [abstract no. 791]. Diabetologia 2005; 48Suppl. 1: A287
Scott R, Wu M, Sanchez M, et al. Efficacy and tolerability of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy over 12 weeks in patients with type 2 diabetes. Int J Clin Pract 2007; 61: 171–80
Nonaka K, Kakikawa T, Sato A, et al. Twelve-week efficacy and tolerability of sitagliptin, a dipeptidyl peptidase-4 inhibitor (DPP-4), in Japanese patients with type 2 diabetes [abstract no. 0038]. Diabetologia 2006; 49Suppl. 1: 25–6
Raz I, Hanefeld M, Xu L, et al. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy in patients with type 2 diabetes mellitus. Diabetologia 2006; 49: 2564–71
Aschner P, Kipnes MS, Lunceford JK, et al. Effect of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy on glycemic control in patients with type 2 diabetes. Diabetes Care 2006; 29: 2632–7
Chan JC, Scott R, Arjona Ferreira JC, et al. Safety and efficacy of sitagliptin in patients with type 2 diabetes and chronic renal insufficiency. Diabetes Obes Metab 2008; 10(7): 545–55
Brazg R, Xu L, Dalla Man C, et al. Effect of adding sitagliptin, a dipeptidyl peptidase-4 inhibitor, to metformin on 24-h glycemic control and β-cell function in patients with type 2 diabetes. Diabetes Obes Metab 2007; 9: 186–93
Rosenstock J, Brazg R, Andryuk PJ, et al. Efficacy and safety of the dipeptidyl dipeptidase-4 inhibitor sitagliptin added to ongoing pioglitazone therapy in patients with type 2 diabetes: a 24-week, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Clin Ther 2006; 28: 1556–68
Charbonnel B, Karasik A, Liu J, et al. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin added to ongoing metformin therapy in patients with type 2 diabetes inadequately controlled with metformin alone. Diabetes Care 2006; 29: 2638–43
Nauck MA, Meininger G, Sheng D, et al. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, compared with the sulfonylurea, glipizide, in patients with type 2 diabetes inadequately controlled on metformin alone: a randomized, double-blind, non-inferiority trial. Diabetes Obes Metab 2007; 9: 194–205
Kleppinger EL, Helms K. The role of vildagliptin in the management of type 2 diabetes. Ann Pharmacother 2007; 41: 82432
Balas B, Baig MR, Watson C, et al. The dipeptidyl peptidase IV inhibitor vildagliptin suppresses endogenous glucose production and enhances islet function after single-dose administration in type 2 diabetic patients. J Clin Endocrinol Metab 2007; 92(4): 1249–55
Ahren B, Gomis R, Standl E, et al. Twelve- and 52-week efficacy of the dipeptidyl peptidase IV inhibitor LAF237 in metformin-treated patients with type 2 diabetes. Diabetes Care 2004; 27: 2874–80
Dejager S, Lebeaut A, Couturier A, et al. Sustained reduction in HbA1c during one-year treatment with vildagliptin in patients with type 2 diabetes (T2DM) [abstract no. 120-OR]. Diabetes 2006; 55Suppl. 1: 29
Rosenstock J, Baron MA, Schweizer A, et al. Vildagliptin is as effective as rosiglitazone in lowering HbA1c but without weight gain in drug-naive patients with type 2 diabetes (T2DM) [abstract no. 557-P]. Diabetes 2006; 55Suppl. 1: 133
Garber A, Camisasca RP, Ehrsam E, et al. Vildagliptin added to metformin improves glycemic control and may mitigate metformin-induced GI side effects in patients with type 2 diabetes (T2DM) [abstract no. 121-OR]. Diabetes 2006; 55Suppl. 1: 29
Pratley RE, Rosenstock J, Pi-Sunyer F-X, et al. Management of type 2 diabetes in treatment naive elderly patients: benefits and risks of vildagliptin monotherapy. Diabetes Care 2007; 30(12): 3017–22
Pratley RE, Rosenstock J, Pi-Sunyer FX, et al. Benefit/risk assessment of vildagliptin in the elderly: pooled analysis of 5 monotherapy studies [abstract]. Diabetes 2007; 56Suppl. 1: A135
He Y-L, Sabo R, Campestrini J, et al. The effect of age, gender, and body mass index on the pharmacokinetics and pharmacodynamics of vildagliptin in healthy volunteers. Br J Clin Pharmacol 2008; 65(3): 338–46
Baron MA, Schweizer A, Couturier A, et al. Efficacy and tolerability of the DPP-4 inhibitor vildagliptin in drug naive patients with type 2 diabetes aged 65 years and older. J Am Geriatr Soc 2007; 55 Suppl.: 25–6
Augeri DJ, Robl JA, Betebenner DA, et al. Discovery and preclinical profile of saxagliptin (BMS-477118): a highly potent, long-acting, orally active dipeptidyl peptidase IV inhibitor for the treatment of type 2 diabetes. J Med Chem 2005; 48: 5025–37
Demuth HU, McIntosh CH, Pederson RA. Type 2 diabetes: therapy with dipeptidyl peptidase IV inhibitors. Biochim Biophys Acta 2005; 1751: 33–44
Qualmann C, Nauck MA, Holst JJ, et al. Glucagon-like peptide 1 [7-36 amide] secretion in response to luminal sucrose from the upper and lower gut: a study using alpha-glucosidase inhibition (acarbose). Scand J Gastroenterol 1995; 30: 892–6
Enç FY, Imeryüz N, Akin L, et al. Inhibition of gastric emptying by acarbose is correlated with GLP-1 response and accompanied by CCK release. Am J Physiol Gastrointest Liver Physiol 2001; 281: G752–63
Seifarth C, Bergmann J, Holst JJ, et al. Prolonged and enhanced secretion of glucagon-like peptide 1 [7-36 amide] after oral sucrose due to alpha-glucosidase inhibition (acarbose) in type 2 diabetic patients. Diabet Med 1998; 15: 485–91
Lee A, Patrick P, Wishart J, et al. The effects of miglitol on glucagon-like peptide-1 secretion and appetite sensations in obese type 2 diabetics. Diabetes Obes Metab 2002; 4: 329–35
Hücking K, Kostic Z, Pox C, et al. α-Glucosidase inhibition (acarbose) fails to enhance secretion of glucagon-like peptide 1 [7–36 amide] and to delay gastric emptying in type 2 diabetic patients. Diabet Metab 2005; 22: 470–6
Hollander PA, Elbein SC, Hirsch IB, et al. Role of orlistat in the treatment of obese patients with type 2 diabetes: a 1-year randomized double-blind study. Diabetes Care 1998; 21: 1288–94
Damci T, Yalin S, Balci H, et al. Orlistat augments postprandial increases in glucagon-like peptide 1 in obese type 2 diabetic patients. Diabetes Care 2004; 27: 1077–80
DeLeon MJ, Chandurkar V, Albert SG, et al. Glucagon-like peptide-1 response to acarbose in elderly type 2 diabetic subjects. Diabetes Res Clin Pract 2002; 56: 101–6
Garber AJ, Foley JE, Banerji MA, et al. Effects of vildagliptin on glucose control in patients with type 2 diabetes inadequately controlled with suphonylurea. Diabetes Obes Metab. Epub 2008 Feb 18
Acknowledgements
No sources of funding were used to assist in the preparation of this review. The authors have no conflicts of interest that are directly relevant to the content of this review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Abbatecola, A.M., Maggi, S. & Paolisso, G. New Approaches to Treating Type 2 Diabetes Mellitus in the Elderly. Drugs Aging 25, 913–925 (2008). https://doi.org/10.2165/0002512-200825110-00002
Published:
Issue Date:
DOI: https://doi.org/10.2165/0002512-200825110-00002