
Abstract
Background: Delayed coverage of pathogens including meticillin-resistant Staphylococcus aureus (MRSA) in pneumonia and bacteraemia has been associated with increased mortality and length of hospital stay (LOS). However, less is known about the impact of delayed appropriate coverage in complicated skin and skin-structure infections (cSSSIs).
Objective: To evaluate the clinical and economic outcomes associated with early versus late use of vancomycin in the management of patients hospitalized for cSSSIs.
Methods: Retrospective analysis was performed using an inpatient claims database of >500 US hospitals in 2005. Using prescription claims, patients with primary or secondary cSSSI admissions were classified into three groups: 1 = early vancomycinmonotherapy; 2 = early vancomycin combination therapy; 3 = late vancomycin therapy. Outcomes studied included LOS and inpatient hospital costs. One-way analysis of variance was used for unadjusted analysis and multivariate regression methods were used to control for co-variates.
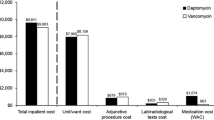
Results: A total of 34 942 patients (27.78% of all patients with cSSSIs) were treated with vancomycin. Mean age was 54.7 years and 54.3% of the patients were males. Mean unadjusted total LOS was 8.46, 9.44 and 13.2 days, and hospital costs in 2005 values were $US10 211.94, $US12 361.94 and $US18 344.00 for groups 1, 2 and 3, respectively. In-hospital mortality rate was highest in group 3 (4.18%) and lowest in group 1 (1.75%). Generalized linear models used to control for potential confounding variables between early versus late vancomycin use suggest that among cSSSI patients late vancomycin use is an independent predictor of higher LOS and costs.
Conclusion: In this large inpatient database, later vancomycin use in patients with cSSSIs appears to be significantly associated with higher LOS and total costs.





Similar content being viewed by others


References
Lee SY, Kuti JL, Nicolau DP. Antimicrobial management of complicated skin and skin structure infections in the era of emerging resistance. Surg Infect (Larchmt) 2005; 6 (3): 283–95
Moet GJ, Jones RN, Biedenbach DJ, et al. Contemporary causes of skin and soft tissue infections in North America, Latin America, and Europe: report from the SENTRY Antimicrobial Surveillance Program (1998–2004). Diagn Microbiol Infect Dis 2007; 57 (1): 7–13. Epub 2006 Oct 23
Frazee BW, Lynn J, Charlebois ED, et al. High prevalence of methicillin-resistant Staphylococcus aureus in emergency department skin and soft tissue infections. Ann Emerg Med 2005; 45 (3): 311–20
Jones ME, Karlowsky JA, Draghi DC, et al. Epidemiology and antibiotic susceptibility of bacteria causing skin and soft tissue infections in the USA and Europe: a guide to appropriate antimicrobial therapy. Int J Antimicrob Agents 2003; 22 (4): 406–19
Tiemersma EW, Bronzwaer SL, Lyytikäinen O, et al. Methicillin-resistant Staphylococcus aureus in Europe, 1999–2002. Emerg Infect Dis 2004; 10 (9): 1627–34
Fridkin SK, Hageman JC, Morrison M, et al. Methicillin-resistant Staphylococcus aureus disease in three communities. N Engl J Med 2005; 352 (14): 1436–44
Lodise Jr TP, McKinnon PS. Burden of methicillin-resistant Staphylococcus aureus: focus on clinical and economic outcomes. Pharmacotherapy 2007; 27 (7): 1001–12
Evans ME, Kortas KJ. Vancomycin use in a university medical center: comparison with hospital infection control practices advisory committee guidelines. Infect Control Hosp Epidemiol 1996; 17 (6): 356–9
Hamilton-Miller JM. Vancomycin-resistant Staphylococcus aureus: a real and present danger? Infection 2002; 30 (3): 118–24
Cosgrove SE, Qi Y, Kaye KS, et al. The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: mortality, length of stay, and hospital charges. Infect Control Hosp Epidemiol 2005; 26 (2): 166–74
Fraser A, Paul M, Almanasreh N, et al. Benefit of appropriate empirical antibiotic treatment: thirty-day mortality and duration of hospital stay. Am J Med 2006; 119 (11): 970–6
Frei CR, Restrepo MI, Mortensen EM, et al. Impact of guideline-concordant empiric antibiotic therapy in community-acquired pneumonia. Am J Med 2006; 119 (10): 865–71
Iregui M, Ward S, Sherman G, et al. Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator-associated pneumonia. Chest 2002; 122 (1): 262–8
Lodise TP, McKinnon PS. Clinical and economic impact of methicillin resistance in patients with Staphylococcus aureus bacteremia. Diagn Microbiol Infect Dis 2005; 52 (2): 113–22
Premier, Inc. [online]. Available from URL: http://www.premierinc.com/index.jsp [Accessed 2008 Feb 13]
Shah NP, Reddy P, Paladino JA, et al. Direct medical costs associated with using vancomycin in methicillin-resistant Staphylococcus aureus infections: an economic model. Curr Med Res Opin 2004; 20 (6): 779–90
Gemmell CG, Edwards DI, Fraise AP, et al. Guidelines for the prophylaxis and treatment of methicillin-resistant Staphylococcus aureus (MRSA) infections in the UK. J Antimicrob Chemother 2006; 57 (4): 589–608
Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis 2005; 41 (10): 1373–406
Graffunder EM, Venezia RA. Risk factors associated with nosocomial methicillin-resistant Staphylococcus aureus (MRSA) infection including previous use of antimicrobials. J Antimicrob Chemother 2002; 49 (6): 999–1005
Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med 2006; 355 (7): 666–74
Wunderink RG, Rello J, Cammarata SK, et al. Linezolid vs vancomycin: analysis of two double-blind studies of patients with methicillin-resistant Staphylococcus aureus nosocomial pneumonia. Chest 2003; 124 (5): 1789–97
Das I, O’Connell N, Lambert P. Epidemiology, clinical and laboratory characteristics of Staphylococcus aureus bacteraemia in a university hospital in UK. J Hosp Infect 2007; 65 (2): 117–23
Acknowledgements
The authors thank Hind T. Hatoum, PhD, for her assistance in writing this manuscript. Her assistance in manuscript development was supported by a contract funded by Johnson & Johnson Pharmaceuticals to Hind T. Hatoum & Company. This study was funded by Johnson & Johnson Pharmaceutical Services, L.L.C. Dr Itani did not receive compensation for his participation in this work. Drs Akhras, Quintana and Merchant and Mr Budd and Mr Stellhorn are employees of Johnson & Johnson and as such are eligible to receive stock options in the company. Dr Itani has previously received honoraria and/or research funding from Pfizer, Merck and Wyeth.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Itani, K.M.F., Akhras, K.S., Stellhorn, R. et al. Outcomes Associated with Initial versus Later Vancomycin Use in Patients with Complicated Skin and Skin-Structure Infections. Pharmacoeconomics 27, 421–430 (2009). https://doi.org/10.2165/00019053-200927050-00006
Published:
Issue Date:
DOI: https://doi.org/10.2165/00019053-200927050-00006