
Abstract
The element chromium apparently has a role in maintaining proper carbohydrate and lipid metabolism in mammals. As this role probably involves potentiation of insulin signalling, chromium dietary supplementation has been postulated to potentially have effects on body composition, including reducing fat mass and increasing lean body mass. Because the supplement is absorbed better than dietary chromium, most studies have focused on the use of chromium picolinate [Cr(pic)3]. Cr(pic)3 has been amazingly popular with the general public, especially with athletes who may have exercise-induced increased urinary chromium loss; however, its effectiveness in manifesting body composition changes has been an area of intense debate in the last decade. Additionally, claims have appeared that the supplement might give rise to deleterious effects.
However, over a decade of human studies with Cr(pic)3 indicate that the supplement has not demonstrated effects on the body composition of healthy individuals, even when taken in combination with an exercise training programme. Recent cell culture and in vivo rat studies have indicated that Cr(pic)3 probably generates oxidative damage of DNA and lipids and is mutagenic, although the significance of these results on humans taking the supplement for prolonged periods of time is unknown and should be a focus for future investigations. Given that in vitro studies suggest that other forms of chromium used as nutritional supplements, such as chromium chloride, are unlikely to be susceptible to generating this type of oxidative damage, the use of these compounds, rather than Cr(pic)3, would appear warranted. Potential neurological effects (both beneficial and deleterious) from Cr(pic)3 supplementation require further study.
Similar content being viewed by others


1. Chromium
1.1 Evidence for an Essential Role
Chromium (Cr), in the form of the ion Cr3+, is believed to be an essential trace element for mammals. This evidence has recently been reviewed.[1] The case for Cr being essential is not definitive however.[2] The evidence can be summarised as follows:[1]
-
Rats fed a low Cr diet (33ng Cr/kg diet) require more insulin than rats on a healthy diet (>100ng Cr/kg diet) to metabolise glucose in glucose tolerance tests,[3] suggesting the development of tissue insulin resistance.
-
Cr deficiency has been developed by a limited number of patients on total parenteral nutrition, resulting in symptoms suggestive of adult-onset diabetes mellitus; [4] the symptoms of this condition are reversed by chromium supplementation and not insulin administration. However, the number of cases is extremely small (actually four or five depending on how they are counted), and the symptoms varied in the patients.
-
Cr absorption is inversely proportional to intake in humans.[5] This suggests that humans regulate Cr intake; this regulation in turn suggests essentialness. However, this does not appear to be the case in all mammals, e.g. rats.[6]
-
Increases in blood serum glucose concentrations result in increases in urinary Cr excretion.[7] Conditions that alter glucose metabolism (including adult-onset diabetes and exercise) alter urinary Cr output.[8] Thus, changes in glucose metabolism result in changes in how Cr is handled, suggesting a direct link between the two.
-
Studies with a naturally occurring biological molecule named chromodulin suggest that a possible explanation at a molecular level exists, which might explain the effects of Cr as described above.
These results suggest an essential relationship between Cr and proper glucose metabolism, probably associated with insulin action. As insulin, in combination with other hormones, is responsible for regulating fat storage and protein synthesis, changes in levels of insulin action could in theory bring about changes in body composition. Fortunately, generating Cr deficiency is difficult,[3] although this suggests that dietary Cr supplements should be of limited value. Conditions such as adult-onset diabetes with long-term increases in urinary Cr loss[9] may generate marginal Cr deficiency that potentially could be alleviated by supplementation; however, this has yet to be demonstrated convincingly.[1] The effects of Cr on corticosteroid-induced diabetes is an area of current research interest, yielding intriguing results.[10] Exercise also increases Cr excretion;[11] this has lead to the suggestion that athletes could be susceptible to Cr depletion and that supplementation of the diet of athletes with Cr could be beneficial.
1.2 Dietary Intake
The US Food and Nutrition Board of the National Academy of Sciences established in 2001 that the daily adequate intake (AI) of chromium was 35µg for adult males and 25µg for adult females [12]. Insufficient data existed for establishing a recommended daily allowance (RDA) [AI is used when an RDA cannot be determined and is the recommended intake value based on approximations or estimates of nutrient intake by healthy people who are assumed to have an adequate diet. The RDA is the average daily dietary intake that is sufficient to meet the nutrient requirements of nearly all (97–98%) healthy individuals[12]]. Thus, a healthy person consuming these amounts of chromium daily (25 or 35µg is assumed to receive an adequate intake to remain healthy. In 1985, Anderson and Kozlovsky[5] reported the Cr content of self-selected diets of 32 American men and women. The average daily Cr intake for men was 33µg; the average for women was 25µg Diets ranged in content from 13–48µg, with the mean Cr intake per 1000 cal being ∼15µg. One study has shown that humans consuming 35µg of Cr daily are Cr sufficient;[13] thus, humans consuming a reasonable diet are not likely to be Cr deficient and should receive little if any benefit from Cr supplementation.
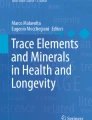
This concept is readily shown in figure 1. At very low levels of dietary intake, a sufficient amount of an essential element for life is not obtained, and the individual dies. As the amount is increased, the person experiences the symptoms of deficiency. After a certain amount is consumed, the individual is healthy; the benefit is maximal. Notice that this part of the figure is essentially a plateau; additional intake of the essential element has very little if any effect. However, as the amount continues to increase, eventually the intake is so great that toxic effects are produced, generating illness. As the amount continues to be increased, death occurs. For chromium, the width of the plateau (i.e., the amounts of dietary chromium that leads to the full beneficial effect) is extraordinarily broad. For individuals consuming a reasonable diet, the amount of Cr places one on the plateau. For dietary Cr, the intake at which chromium becomes harmful or toxic is so high that it currently can only be estimated.[14,15]

Dependence of beneficial biological effect on the intake of an essential element.
The key issue to consider here is that this is for forms of chromium normally found in the diet. Synthetic complexes of Cr, such as chromium picolinate [Cr(pic)3], could be more, or less, toxic than dietary Cr. Currently available nutrition supplements containing Cr(pic)3 generally provide 200–6OOµg of Cr per day, roughly 10- to 20-fold more than suggested AI. Cr(pic)3 is also more efficiently absorbed (2–5%) than dietary chromium (0.5–2%),[16,17] Thus, individuals on the supplement could be absorbing approximately 100-fold more Cr than individuals on a self-selected diet. The potential positive and negative effects of the intake of Cr(pic)3 at these levels have been examined numerous times since 1989 and will form the basis of this review (table I).

Effects of Cr(pic)3 a on body mass or composition
2. Chromium Picolinate: Effects on Body Mass and Body Composition?
2.1 Initial Reports
The field of Cr(pic)3 supplementation and its use as a weight loss/muscle development agent started with the publication of a paper by Evans[21] in 1989. The history leading to this publication has been excellently summarised by Neilsen:[43]
“Actually this story begins with the study of factors that could facilitate the absorption of zinc. It was found in the early 1980s that zinc complexes to picolinate, compared with zinc sulphate, improved zinc assimilation in children with acrodermatitis enteropathica, a genetic disorder that results in the inability to absorb zinc from cow’s milk. Subsequently it was found that other metal picolinates were better absorbed than mineral salt forms. Shortly thereafter, Dr Gary Evans, then employed by the Grand Forks Human Nutrition Research Center of the US Department of Agriculture (USDA) decided to patent the process of synthesizing coordination complexes of picolinic acid.”
“In the patent, it is explained that these complexes are more available for absorption by the body. [44] In other words, contrary to what many advertisements touting chromium picolinate lead many to believe, the USDA patent is not specific to chromium, nor does it mention that chromium picolinate has any beneficial effects claimed for this form of chromium supplement. In 1986, a supplement company (Nutrition 21) licensed the patent from USDA. This authorized them to continue the development of chromium picolinate. Although the government collects an annual “maintenance” fee and royalties on all sales covered by the license, USDA does not make any claims or guarantees for the products covered by the patent. Research supported by Nutrition 21, in which Dr. Evans was heavily involved after leaving the Grand Forks Human Nutrition Research Center, resulted in the reports in 1989 that generated the publicity that probably was the major impetus leading to the popularity of chromium picolinate as a nutritional supplement.
The contents of this 1989 work by Evans[21] need to be examined in detail. Two of the studies, both appearing in Evans,[21] are of interest here (table I). In the first, 10 males between 18–21 years of age were involved. Half the students received a supplement containing 200µg Cr as Cr(pic)3 for 40 days; the other half received a placebo. The participants engaged in 40-minute exercise periods twice a week. By measuring the thickness of skin folds and biceps and calf circumferences, body composition was estimated. Participants on the supplement gained 2.2kg of body mass on average, had no significant change in percentage body fat and gained 1.6kg of lean body mass. In contrast, participants on the placebo on average gained 1.25kg of body mass, had an increase in body fat of 1.1% and increased their lean body mass by 0.04 kg. The increase in lean body mass for the participants receiving chromium was said to be statistically greater than that for the control (or placebo) group (p = 0.019).[21]
In the second study,[21] 31 (of an initial 40) college football players completed a 42-day programme. Half of the players were given 200µg Cr as Cr(pic)3, while the other half received a placebo. The participants exercised 1 hour per day for 4 days per week. Body composition was estimated by measuring thigh, abdomen, chest skin folds, and thigh, biceps and calf circumference. After 14 days, participants receiving Cr on average lost 2.7% of their body fat and had an increase of lean body mass of 1.8kg, while no changes were observed in the control group. After 6 weeks, the chromium group on average lost 1.2kg, lost 3.6% (or 3.4kg) of their body fat and had an increase in lean body mass of 2.6kg, while the control group had a loss of lkg of body fat and experienced a 1.8kg increase in lean body mass. Both the loss of body fat and the increase in lean body mass were said to be significantly greater for the chromium group (p = 0.001 and p = 0.031, respectively).
These results were rapidly challenged.[45–48] A major concern was that the article was a non-refereed review.[45,46] Body composition by skin fold measurements and circumference measurements is only an indirect estimation, especially in young males; [46] more accurate techniques such as underwater weighing were available in 1989. These measurements can give rise to values that are “statistically different yet functionally meaningless”. [47] No method to determine compliance of participants was indicated, and the standard deviation of the data was not presented.
2.2 Subsequent Studies
The next study to investigate the effects of Cr(pic)3 on body composition was reported by Press et al.[22] in 1990. The study had a double-blinded, crossover design. Groups received supplements or placebos for 42 days, then received neither for 14 days and finally received, for 42 days, the opposite (placebo or supplement) from that in the original 42 days. Participants varying from 25–80 years in age were enrolled. Compliance was monitored by capsule count. While the study was designed to look at serum cholesterol and apolipoprotein levels, body mass data were also collected. Cr(pic)3 supplementation, 200µg per day, had no effect on body mass.
In 1992, Hasten et al.[23] reported a larger study on the effects of Cr(pic)3 supplementation. College students ranging from 18–36 years of age were involved in the 12-week study; 37 males and 22 females completed the study. Students were not involved in physical training 2 years prior to the study or during the study outside of the conditioning class. Students were in 40-minute exercise classes 3 days a week. The study was double-blind with the supplement group receiving 200µg Cr a day as Cr(pic)3. Compliance was determined by capsule count. Body composition was determined by skin fold and circumference measurements. For male participants, Cr(pic)3 had no effect on strength, body measurements or body mass. For females, no effect was observed on strength or body measurements; however, females increased body mass on average by 2.5kg compared with the control, a significant change (p = 0.0048). Approximations of lean body mass and percentage body fat were not significantly different. In this work, the same concerns about estimating body compositions from skin fold measurements mentioned above still hold, although the authors were careful to refer to the approximate nature of the calculations. The authors also suggested that the increase in body mass in females was probably primarily from lean body mass increases; the increase in the latter was almost statistically significant.
Also in 1992, Kaats et al.[18] reported the effects of a diet supplemented with a high-fibre cookie and a capsule containing Cr(pic)3 and L-carnitine. Some positive effects on body composition were noted, but as the participants received numerous vitamins and minerals, fibre and carnitine in addition to Cr(pic)3, it is impossible to determine the effect of Cr(pic)3.
The following year, Evans and Pouchnik[24] reported a study of the effects of Cr(pic)3 on body composition. Twelve males and 12 females were involved in a weekly aerobics class. Participants were 25–36 years of age. Males received 400µg Cr per day as Cr(pic)3 or 400µg of Cr as chromium nicotinate. Females received half as much of either Cr source. Lean body mass was measured by resistivity. Data were presented with standard errors. For males receiving Cr(pic)3, the lean body mass increased 2.1 kg and was statistically equivalent to the initial value and to the values of the group receiving chromium nicotinate. For females, the lean body mass increased 1.8kg and was statistically equivalent to the initial value and to those of the group receiving chromium nicotinate. However, Evans and Pouchnik[24] claimed that despite this the change in lean body mass for both males and females on Cr(pic)3 was significant (p < 0.01). The statistical analysis that indicated that while final and initial values were equivalent the difference between them was significant failed to incorporate the error in both the initial and final values in the calculation of the error of the difference. This study has been criticised by Lefavi[49] who stated:
“It is likely that reviewers well-read in exercise physiology would find the notion of a 4.6-lb lean body mass (LBM) increase in males and a 4.0-lb LBM increase in females resulting from 12 weeks of a weekly aerobics class preposterous. A LBM increase that dramatic is not typically seen in participants who are weight-training three times per week for 12 weeks, no matter what they are taking.
... Investigators familiar with this type of research would suggest either (a) that was one great aerobics class, or (b) people in Bemidji, MN, respond in a highly unusual manner to aerobic exercise and/or are extremely chromium deficient, or (c) Dr. Evan’s group is consistently having difficulty accurately measuring LBM.
Subsequent research of body composition studies has generally used underwater weighting, dual Xray absorptiometry or magnetic resonance imaging to measure the fat and lean body content, and consequently is more accurate than these initial studies. Curiously, none of the studies described above reported a source of funding; funding sources are presented so that readers can note any potential conflicts of interest.
In 1994, Clarkson and colleagues[25] followed 36 college football players for 9 weeks. Twenty-one completed all or most of the study. Half the players received 200µg Cr as Cr(pic)3. The players trained the first and last 4-week periods of the study with spring break in the middle; each week’s training consisted of weightlifting on 4 days and running on 2 days. Compliance was monitored. Body composition was determined using underwater weighing; skin fold and circumference measurements were also performed. No changes in body composition or strength were found to result from Cr supplementation. The source of funding was not given. In 1995, Trent and Thieding-Cancel[26] studied Navy personnel (79 men, 16 women) with a mean age of 30.3 years. Participants received 400µg Cr(pic)3 or placebo daily [the authors probably meant 400µg of Cr as Cr(pic)3]. A conditioning programme consisting of exercise (at least 30 minutes) three times a week (average 4.5 hours per week) was employed; compliance was monitored. Body composition was estimated by circumference measurements. No statistically significant changes from Cr supplementation were found for body mass, percentage body fat or lean body mass. Funding was provided by the Navy and Nutrition 21.
Five studies [19,27–30] of relevance appeared in 1996. Hallmark et al. [27] followed 16 untrained males (23 ± 4 years of age) through a 12-week resistive training programme consisting of training 3 days a week. Half received 200µg Cr per day as Cr(pic)3. Underwater weighing was used to determine body composition. While the strength of individuals increased on average over the course of the study, Cr(pic)3 had no effect on body mass, strength, percentage body fat, lean body mass or skin fold thicknesses. Compliance was monitored; Cr(pic)3 was denoted by Nutrition 21. Krieder et al.[19] examined the effects of 800µg of Cr as Cr(pic)3 as the commercial product GainersFuel™1. While the study was well designed and body composition was determined by x-ray absorptiometry, no changes arose from the product versus the control in participants on a resistance-training programme. Drawing conclusions specifically on the effect of the Cr(pic)3 cannot be done as it is conceivable that some ingredient in the product could have cancelled any beneficial effects from Cr(pic)3. Thirty-six men aged 19-26 years participated in a study by Lukaski et al. [28] Participants received a placebo or 172µg Cr as Cr(pic)3 for 8 weeks. Participants exercised 5 days a week, and compliance was monitored. Body composition was measured by dual x-ray absorptiometry; skin fold thicknesses, body mass and height were measured. No effects on body composition, body mass, skin fold or strength were found from supplementation. Nutrition 21 provided the supplements. Interestingly, Lukaski et al.[28] found that urinary Cr loss increased for control participants during weeks 2, 3, 5, 7 and 8 of the exercise programme. However, whether Cr absorption changed as a result of increased losses is not known. Thus, homeostatic adaptation could take place, preventing the increased urinary Cr loss from changing the Cr status of the body.
Kaats et al.[29] examined 154 free-living (no constraints on diet or exercise) participants who received a placebo or 200 or 400µg Cr daily as Cr(pic)3 in a protein/carbohydrate nutritional drink. Two hundred and eighteen participants started the study which was 72 days in length. Body composition was determined using underwater weighing. The significance of this study is difficult to determine as the authors described their results in terms of a calculated ‘body composition improvement’ (BCI) index, rather than on measured parameters. The BCI index was calculated by adding “losses in body fat and increases in [free fat mass] as positive changes and increases in body fat and decreases in [free fat mass] as negative changes”.[29] The BCI of patients on either dose of Cr(pic)3 improved significantly while the extent of improvement was equivalent for both quantities. In terms of changes in measured parameters, non-significant changes were observed in non-fat mass. The group receiving 400µg Cr, but not 200µg had a lower body mass. Fat weight and percentage body fat also appeared to drop significantly with supplementation. The statistical treatment was based on comparing changes, rather than comparing initial values against final values; indeed, the changes were quite small. The post-study values were not presented with their standard deviations, preventing further statistical analysis. Lukaski[50] has criticised the design of this study because of a lack of control of Cr intake and failure to maintain constant energy intake and expenditure. Participants were not asked about their diet or exercise during the study, only about how much of the drink they consumed each day. The study was funded in part by Nutrition 21.
Bulbulian et al.[30] reported the effects of 400µg Cr, as Cr(pic)3, daily for 24 weeks on 20 male and 20 female swimmers. Using hydrodensitometry, supplementation after 24 weeks led to decreased fat mass and percentage fat mass and increased lean body mass, with greater magnitude changes in women than men. No significant effects were observed after 12 weeks. Unfortunately, the work was only presented in an abstract, so the same scrutiny given other studies reviewed here is not possible. For example, the actual mass changes, standard deviation, compliance measures, etc. were not reported; therefore, this preliminary report will not be considered further.
In 1997, four studies appeared [20,31–33]. Grant et al.[31] examined female participants with obesity ranging from 18–35 years of age. Over 9 weeks, the participants received either two placebo capsules or two capsules each containing 200µg of Cr as Cr(pic)3 per day. Compliance was monitored by counting returned capsules. Participants consuming Cr(pic)3 and involved in cross training had no changes in body mass, percentage body fat, fat mass or fat free mass compared with those consuming placebos and exercising. However, participants consuming the supplement, but not exercising, gained body mass when compared with a control group not exercising, while no effects were observed on percentage body fat, fat mass or fat free mass. Body composition was determined by underwater weighing. Funding was provided by Shaklee, USA, Inc., who also provided the supplements. Campbell et al. [32] have examined the effects of Cr(pic)3 on moderately overweight men. Eighteen men aged 56–69 years participated in the 12-week study. All were involved in a twice-weekly resistance-training programme, while half received 1000µg Cr as Cr(pic)3 daily. Compliance was monitored by counting returned capsules. The supplement had no effect on body mass or strength. The study was supported in part by Nutrition 21.
Bahadori et al.[33] examined 21 participants with obesity. The average age of the participants was 44 years. Participants consumed a very low calorie diet for 8 weeks followed by an 18-week maintenance period and received either a placebo or 200µg Cr as Cr(pic)3 or Cr-enhanced yeast daily. Body composition was unfortunately measured by skin fold thickness. Cr(pic)3 had significantly increased lean body mass compared with that of the other groups (p < 0.029). Body mass and percentage fat mass were not significantly affected by Cr(pic)3. However, use of skin fold measurements places these results in question. Pasman et al.[20] examined the effects of Cr(pic)3 on 33 female participants with obesity. Unfortunately, in terms of analysis of the effects of Cr(pic)3, fibre and caffeine were used in conjunction with 200µg of Cr(pic)3 daily. The supplement had no effect on body mass or body composition (estimated from circumference measurements). Novartis Nutrition Ltd. provided funding.
Studies of the effects of Cr(pic)3 continued to appear at a brisk pace in 1998 (3 studies)[34–36] and 1999 (3 studies)[37–39]. Walker et al.[34] followed wrestlers with an average age of 20 years. In a double-blind, placebo-controlled study, the wrestlers consumed 200µg Cr as Cr(pic)3 daily for 14 weeks. Compliance was monitored and body composition was determined from underwater weighing; skin folds and circumferences were also measured. No effects from Cr(pic)3 were found on body mass, lean body mass, percentage body fat, fat mass or strength. Funding was provided by the Gatorade Sports Institute. Kaats et al.[35] examined 17 men and 105 women averaging 42.3 years of age. Participants received either a placebo or 400µg Cr(pic)3 daily for 90 days. Body composition was determined by x-ray absorptiometry. Compliance was monitored by having participants keep a notebook and by interview. No significant changes from supplementation were found for body mass, percentage body fat or fat-free mass. The loss of fat mass was significantly larger (p = 0.023) for the Cr(pic)3 group, although concerns about how the statistics for differences were calculated holds again for this work as with the earlier work by Kaats et al.[29] The authors also indicated that when the data were corrected for physical activity and caloric intake, changes in body mass, percentage body fat and fat mass (but not free-fat mass) all became significantly greater for the supplemented group (p < 0.001). The validity of this ‘correction’ is highly questionable. It is also significant to note that the data were not corrected this time for BCI as in the previous report in 1996 by Kaats et al.[29] The lack of statistical changes in measurable variables, with the exception of fat mass with supplementation, directly contradicted the results of their work in 1996. The study was funded by Nutrition 21. Boyd et al.[36] studied 35 students for 13 weeks. The students received either a placebo or 1000µg Cr(pic)3 [probably meant to indicate 1000µg Cr as Cr(pic)3] daily. Students also underwent a 50-minute exercise class twice a week. Circumferences were measured, and unfortunately skin folds were measured to estimate body composition. No significant changes in strength or lean body mass were noted, either from the exercise programme or from the programme in combination with supplementation. Cr(pic)3 was provided by Nutrition 21.
Campbell et al.[37] also found that Cr(pic)3 had no effect on fat free mass, whole body muscle mass and muscle strength in a 13-week study with men aged between 50–75 years. However, one type of muscle power increased in the placebo group and not in the Cr(pic)3 group. This could be equally well restated as Cr(pic)3 appeared to prevent muscle power increase in one case. Each man received a placebo or 924µg Cr per day. Compliance was monitored, and body composition was determined by underwater weighing. Participants were also involved in a twice-weekly resistance-training programme. The research was funded by the National Institutes of Health and independently by Nutrition 21. Many of these same researchers were involved in another study which appeared at about the same time.[38] Thirty-five men and women aged 54–71 years were given a placebo or 924µg Cr as Cr(pic)3 daily. Participants were involved in resistance training twice a week for 12 weeks. Body composition was determined by underwater weighing. No effects from Cr(pic)3 were observed on body mass, percentage body fat, fat-free mass or strength. The research was funded by the same sources. Thus, in these two studies, 53 participants were given large 924µg quantities of Cr daily for 12–13 weeks without effect. Also in 1999, Cefalu et al.[39] examined 14 men and 15 women who received 1000µg of Cr daily as Cr(pic)3 for 8 months. Compliance was monitored and body composition was determined by magnetic resonance imaging. No effect was observed on body mass, abdominal fat distribution or body mass index. No funding source was indicated.
In the last 2 years, four other reports appeared; [40–42,51] none reported any effects from Cr(pic)3 supplementation on body mass or composition. Davis et al.[51] examined the time taken for eight men to become fatigued during high-shuttle running. The men consumed flavoured water, a drink containing carbohydrates and electrolytes or a drink containing these ingredients, and 400µg Cr as Cr(pic)3. The men then underwent an exercise programme before being tested for fatigue. While the drink had beneficial effects, the addition of Cr had no effect. No source of support was indicated. Amato et al.[40] examined nine women and ten men between the ages of 63–77 years. Nine of the participants received 1000µg per Cr(pic)3 [probably meant to be 1000µg Cr as Cr(pic)3]. Compliance was monitored and body composition was determined by dual-energy x-ray absorptiometry. No change in body mass index or body composition was found from supplementation. Cr(pic)3 was provided by Nutrition 21. Female softball athletes were investigated in a study by Livolsi et al.[41] The women, between 17–21 years of age, received 500µg Cr as Cr(pic)3 or a placebo for 6 weeks. During this time the women trained for 2 hours on 3 days a week. Body composition was determined by underwater weighing. No effect was observed from Cr on muscular strength, body mass, percentage body fat or lean body mass. Nutrition [2] provided the Cr(pic)3. Finally, Volpe et al.[42] examined the effects of 400µg Cr as Cr(pic)3 on moderately obese women. Forty-four women aged 27–51 years received the supplement or a placebo for 12 weeks. During this time, the women participated in weight training 2 days a week. Body composition was determined by underwater weighing. No change was found from the Cr(pic)3 on body mass, body mass index, waist or hip circumferences, percentage body fat, lean body mass or fat mass. The project was supported by Nutrition 21.
2.3 Reviews
The increase in the number of studies in the midto-late 1990s was accompanied by a sudden plethora of published review articles. The themes of the reviews were similar. Nielsen[43] stated:
“To summarise, the data related to chromium changing lean body mass, strength gain, and athletic performance are mostly negative ... in other words, the findings to indicate that the use of large amounts of chromium supplements, including the picolinate form, will not bring forth the over zealously touted propitious effects on muscle accretion, strength gain, or athletic performance.” (p. 229). “In summary, there are no data from well-controlled studies to support the astonishing weight-loss claims with the use of chromium picolinate supplements. Thus, a high intake of chromium picolinate is unlikely to lead to significant weight loss.” (p. 229).
Clarkson[52] reported that “the preponderance of evidence shows that chromium supplements will not increase lean body mass or decrease fat mass, despite the widespread hype to the contrary ... the prudent course for athletes should be to ingest foods rich in chromium”. Similarly, according to Anderson:[53]
“In our studies during the past 20 years of daily supplementation of 200 µg as Cr chloride and up to 1000 µg in the form of Cr picolinate ranging from 5 weeks to 4 months of supplementation, we have been unable to detect an effect of supplemental Cr on bodyweight .... If Cr is to have any effect on body composition and over all weight, it is likely to be a long-term small effect and not a quick fix or panacea.”
Hellerstein[54] commented: “To an outsider reviewing literature on chromium and diabetes/obesity, the field is most striking for two features: its nearly complete lack of biomedical or clinical understanding and its high degree of polarisation .... As in all fields with more heat than light, the reason has been the incomplete ability to measure and test key factors .... The high degree of politicisation and polarisation in this field is characterised by unproven claims and counterclaims and suspicion among investigators. Concerns about possible commercial bias and potential conflict of interest have naturally emerged. Reports of benefits of supplementation (e.g. that lean tissue is increased and fat decreased by chromium in athletes in training) that were not confirmed by several subsequent studies have furthered these concerns.”
According to Kreider;[55] “It appears clear from these studies that short-term chromium supplementation (i.e. chromium 200 to 800 mg/day, as chromium picolinate, for 4 to 12 weeks) does not promote muscle growth in healthy resistance-trained individuals. Consequently, in my view, chromium supplementation should not be recommended to athletes as a method of promoting muscle growth or fat loss.”
Lukaski[50] stated: “CrPic supplementation with an exercise training programme does not facilitate a preferential loss of FM [fat mass]. Thus, CrPic per se does not promote beneficial changes in body composition of humans.” Lukaski[56] also commented in another review: “Thus, the limited studies to date indicate that chromium supplements do not promote general muscle gain and fat loss, as determined by various methods of body-composition assessment, nor do they facilitate regional or wholebody strength gain during resistance training.” Kobla and Volpe[57] concluded that “chromium supplements have gained popularity due to the belief that they may increase LBM and reduce percent body fat .... Chromium supplementation does not appear to increase LBM or decrease fat mass, even when combined with resistive training.” Perhaps most notable of all is that the US Federal Trade Commission in 1997 concluded that no basis existed for claims that Cr(pic)3 promotes body mass loss and fat loss in humans.[58]
2.4 Summary
In summary, the results of well-designed and performed studies indicate that Cr(pic)3 supplementation has no significant effect on body composition when given up to 1000µg Cr as Cr(pic)3 daily, regardless of whether an exercise programme is involved or not. Occasionally in these studies, changes in the group supplemented with Cr(pic)– are statistically distinct from changes in the control group. However, no pattern is present in these changes from study to study. In a recent review,[1] a meta-analysis has demonstrated that data summarised from randomised clinical trials [most using Cr(pic)3] showed no effect of supplemental Cr and glucose or insulin concentrations in healthy participants.[59] Thus, Cr(pic)– supplementation does not affect body composition or glucose or insulin responses in healthy individuals.
Yet, Cr(pic)– has clearly been shown to have one effect on humans: increased urinary output of Cr.[60] Comparing urinary Cr loss with intake suggests a second effect; Cr accumulates in tissues. The potential significance of this accumulation and other in vivo effects from Cr(pic)3 supplementation will be the next topic of discussion.
3. Toxic Effects of Chromium Picolinate
3.1 Generation of Reactive Oxygen Species
In 1995, questions arose about the safety of Cr(pic)3 as a dietary supplement as Steams et al.[61] showed that the compound caused clastogenic damage (i.e., cleavage of chromosomes) in Chinese hamster ovary (CHO) cells. When intracellular Cr levels generated using CrCl3 or Cr nicotinate were comparable to those generated using Cr(pic)3, no chromosome aberrations were found. Unfortunately, these studies used high, non-physiological concentrations of Cr (0.05–1mM) and used Cr(pic)3 that had not been purified, casting doubt on the interpretation of these findings. Bagchi et al.[62] have subsequently observed DNA fragmentation in another type of cultured cell treated with Cr(pic)3, although the Cr concentrations were also non-physiological. In 2002, Steams et al.[63] reported that Cr(pic)3 is mutagenic at the hypoxanthine phosphoribosyltransferase locus in CHO cells; yet, these studies still used the same concentrations of Cr(pic)3 (0.2–1 mM), although the material was purified before use. In a related study, this group has also shown that Cr(pic)3 also leads to mitochondrial damage and apoptosis in CHO cells.[64] Wetterhahn and colleagues[65] have suggested from pharmacokinetic modelling studies that taking Cr(pic)3 supplements for 5 years could result in Cr(pic)3 concentrations as high as 13µM in liver tissue.
In an in vitro study,[66] physiologically relevant concentrations of Cr as Cr(pic)3 (as low as 120nM) and of biological reductants, such as ascorbate and thiols (5mM, the approximate ascorbate concentration in cells), resulted in catalytic production of reactive oxygen species (ROS), such as hydroxyl radicals, that can cleave DNA. This ability apparently stems from the combination of Cr and picolinate;[67] neither the picolinate nor the Cr3+ catalyse this separately. The picolinate ligands shift the redox potential of the chromic centre such that it is susceptible to reduction. The reduced chromous species could interact with dioxygen to produce ROS. These findings are consistent with earlier results that showed mutagenic forms of Cr3+ possessed chelating ligands containing pyridine-type nitrogens coordinated to the metal, and damage required the presence of dioxygen.[68]
Recent studies have also shown that Cr(pic)3 is remarkably stable in buffered aqueous solution,[66,69] similar to the pH of body fluids, and in synthetic gastric fluid and passes unhindered through the jejunum.[70] Consequently when Cr(pic)3 is taken orally, the supplement probably enters cells intact, i.e. in the potentially harmful form. Cr(pic)3 possesses a lifetime of less than 24 hours in vivo in rats.[71] Thus, the form that accumulates in rats.[71] is not Cr(pic)3. However, these in vivo and in vitro studies also suggest that Cr(pic)3 must enter cells intact to be subsequently degraded, the degradation being rapid in the cell. Within liver cells, Cr3+ from the supplement (given intravenously daily to rats for 2 weeks) resides mainly in the cytosol; little of the metal ion is in the nucleus.[72] A study of the transport of Cr(pic)3 in rats during the first 24 hours after intravenous injection (5µg Cr) demonstrated that Cr enters hepatocyte nuclei rapidly, reaching a maximum concentration 1 hour after injection; Cr levels decreased rapidly thereafter.[73] Behaviour in mitochondria was similar. Fortunately, the supplement has little propensity to bind to isolated DNA.[72] Kareus et al.[74] have demonstrated in vitro that microsomal hepatocyte enzymes can degrade picolinate from Cr(pic)3 efficiently. Furthermore, Anderson et al.[75] have shown that Cr(pic)3 is not acutely toxic. Four-week old rats were fed diets containing up to 100mg Cr as Cr(pic)3 per kg diet for 24 weeks. No effects were seen from supplementation on body mass, organ mass or numerous blood variables. Histological evaluation of liver and kidney tissues revealed no effects from the supplement; however, Cr concentrations in the liver and kidney increased linearly with the amount of Cr in the food.[75] While it was not the focus of this study, it should be pointed out that the rats consumed up to 15mg Cr per kg body mass per day for 24 weeks which resulted in no change in body composition. For a 50kg human, this would be equivalent to 750mg Cr per day, 1000-fold the amount used in the human studies (table I) reviewed above (for a review of effects of Cr(pic)3 administration on body composition in rats see Vincent[1]).
Isolated incidents of deleterious effects of Cr(pic)3 supplementation of humans have been reported: weight loss, anaemia, thrombocytopenia, liver dysfunction and renal failure;[76] renal failure;[77] rhabdomyolysis;[78] dermatitis;[79] acute, short-lasting cognitive, perceptual and motor changes;[80] exanthematous pustulosis;[81] and hypoglycaemia.[82] The significance of these isolated incidents is difficult to ascertain.
Studies have been performed to look for the effects of potential Cr(pic)3-generated ROS on DNA. No effect on 5-hydroxymethyl uracil, a product of oxidative DNA damage, levels was observed in a study of ten women with obesity given 400µg Cr(pic)3 per day for 8 weeks.[83] In a preliminary report, rats were given a single oral dose of Cr(pic)3 up to 2000mg complex per kg body mass; chromosomes from bone marrow cells of femurs removed 18 or 42 hours after the dose showed no increase in damage versus controls.[84] However, the significance of a study using a single dose of Cr(pic)3 is difficult to assess. Similarly in a preliminary report, Esber et al.[85] provided rats (the method of administration was not reported) with a single dose of up to 246mg Cr/kg (body mass presumably) as Cr(pic)3; no induction of chromosomal damage resulted (although what exactly was measured and how was not reported). The same abstract[85] reported that the supplement was not mutagenic at a level of 5 mg/ plate in the Ames assay.
Studies observing oxidative damage from the supplement in vivo are just appearing. Intravenous injection of rats with Cr(pic)3 (5µg ∼20-fold the amount a human taking commercial supplements receives on a per kg body mass basis) daily for 60 days resulted in significant increases (p < 0.002) in urinary 8-hydroxydeoxyguanosine (8-OHdG) a product of oxidative DNA damage, in urine commencing after 32 days of treatment.[72] At the end of the 60 days, 8-OHdG levels were significantly greater in liver and kidney tissue (p < 0.002). Additionally, levels of lipid peroxidation in the tissues were significantly increased (p < 0.002). In addition to the oxidative damage, this lipid peroxidation can in turn lead to DNA and chromosome damage[86] of the type observed by Steams et al.[61] in 1995. The failure to observe an effect on 5-hydroxymethyl uracil levels in women given the supplement for 56 days, as in the rat study, may be the result of the difference in dosage; rats given proportionally more of the supplement required 30 days of administration before significant levels of oxidative damage were observed. To truly establish the safety of Cr(pic)3, a long-term human study will be necessary. Additionally, Cr(pic)3 when added to the food of fruit flies at levels comparable to those of human diet supplementation has been shown to lead to increases in lethal mutations (Vincent J, unpublished observations).
It should be noted that Preuss et al.[87] have also examined the effect of Cr(pic)3 on lipid peroxidation in rats. Spontaneously hypertensive rats were fed a diet containing 5 mg/kg Cr as Cr(pic)3 for 30 days. Subsequently, the diet was changed to laboratory rat chow for 30 days during which time the drinking water was replaced with 5% weight per weight sucrose solution. For another 14 days, the diet was maintained while the concentration of sucrose in the water was doubled. Hence, the rats received Cr(pic)3 for 30 days, but they were then off the supplement for 44 days prior to sacrifice and determination of lipid peroxidation levels. The researchers found that hepatic levels of thiobarbituric acid reactive substance (TBARS) in rats receiving Cr(pic)3 were significantly lower than those of the controls (although no numbers were presented), while renal levels of TBARS were not significantly affected. Given the short lifetime of Cr(pic)3 in the cells and the instability of peroxidised lipids, termination of the supplementation probably allowed for the repair/ replacement of any damaged cellular components.
Additionally, Witmer et al.[88] have examined the ability of CrC13 and Cr(pic)3 to promote the formation of ROS capable of generating oxidative damage in cultured human lung cells.[88] Using a dye that fluoresces when oxidised, CrC13 (200 µmol/L) was found to have no effect. Cr(pic)3 at the same concentration partially quenched the fluorescence. However, the Cr(pic)3 was added as a methanol solution to increase the solubility of the complex; alcohols are traps for ROS such as hydroxyl radicals, preventing any conclusions from being drawn from the study.
Recently, a potential beneficial effect of Cr(pic)3 on antidepressant pharmacotherapy for dysthymic disorder was reported.[19,90] Cr(pic)3 has also been reported to lower cortisol response to serotonin (i.e. 5-hydroxytryptamine) precursors.[91] These reports, in combination with the isolated report of Cr(pic)3 possibly causing perceptual and motor changes, may potentially be concerning. Picolinic acid/picolinate is a natural catabolite of the amino acid tryptophan, generated as an end product in the kynurenine pathway in the body.[92] Molecules generated along this pathway tend to have neurological effects.[93] This raises concerns about Cr(pic)3 in the body, as the Cr(pic)3 should deliver and release 3 picolinates (or its degradation products)[74] per Cr. Safety concerns regarding picolinic acid have arisen several times,[94–98] leading to suggestions that picolinic acid by itself should not be used as a dietary supplement. Thus, effects on perceptual and motor function and dysthymic disorder could potentially be related to picolinate released in the body; this is an area that requires more investigation.
3.3 Summary
In summary, recent studies suggest that potentially deleterious effects from Cr(pic)3 supplementation must be taken seriously. Further investigation into the effects of Cr(pic)3 on humans consuming 200mg or greater of Cr, as the supplement, daily for prolonged periods of time are urgently needed. Given that forms of Cr which do not generate the same type of oxidative damage as Cr(pic)3 are available for use in nutritional supplements (and in the case of CrCl3, for example, are substantially cheaper [even when differences in the percentage of Cr absorbed are considered]), the use of alternative forms of Cr3+ would seem warranted.
Cr(pic)3 is an amazingly popular nutritional supplement and weight loss agent; products containing the supplement generate nearly $US500 million (2000 values) annually, second only to calcium supplements.[99] Yet, overwhelming evidence indicates that Cr(pic)3 has no effects on body composition. The potential deleterious effects of the supplement, especially when recent reports of mutagenic effects are taken into account, outweigh the potential benefits, especially when alternative sources of Cr for dietary supplementation are available.
References
Vincent JB. The bioinorganic chemistry of chromium(III). Polyhedron 2001; 20: 1–26
Stearns DM. Is chromium a trace essential metal? Biofactors 2000; 11: 149–62
Striffler JS, Law JS, Polansky MM, et al. Chromium improves insulin response to glucose in rats. Metabolism 1995; 44: 1314–20
Anderson RA. Chromium in parenteral nutrition. Nutrition 1995; 11 (1 Suppl.): 83–6
Anderson RA, Kozlovsky AS. Chromium intake, absorption and excretion of subjects consuming self-selected diets. Am J Clin Nutr 1985; 41: 1177–83
Anderson RA, Polansky MM. Dietary and metabolite effects on trivalent chromium retention and distribution in rats. Biol Trace Elem Res 1995; 50: 97–108
Morris BW, MacNeil S, Stanley K, et al. The inter-relationship between insulin and chromium in hyperinsulinaemic euglycaemic clamps in healthy volunteers. J Endocrinol 1993; 139: 339–45
Kozlovsky AS, Moser PB, Reiser S, et al. Effects of diets high in simple sugars on urinary chromium losses. Metabolism 1986 Jun; 35(6): 515–8
Morris BW, MacNeil S, Hardisty CA, et al. Chromium homeostasis in patients with type II (NIDDM) diabetes. J Trace Elem Med Biol 1999; 13: 57–61
Kim DS, Kim TW, Park IK, et al. Effects of chromium picolinate supplementation on insulin sensitivity, serum lipids, and body weight in dexamethasone-treated rats. Metabolism 2002; 51: 589–94
Anderson RA, Bryden NA, Polansky MM, et al. Exercise effects on chromium excretion of trained and untrained men consuming a constant diet. J Appl Physiol 1988; 64: 249–52
Trumbo P, Yates AA, Schlicker S, et al. Dietary reference intakes: vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. J Am Diet Assoc 2001; 101: 294–301
Offenbacher EG, Spencer H, Dowling HJ, et al. Metabolic chromium balances in men. Am J Clin Nutr 1986; 44: 77–82
Jeejeebhoy KN. The role of chromium in nutrition and therapeutics and as a potential toxin. Nutr Rev 1999; 57: 329–35
Hathcock JN. Safety limits for nutrients. J Nutr 1996; 126: 2386S–9S
Olin KL, Stearns DM, Armstrong WH, et al. 51Chromium (51Cr) from 51Cr chloride, 51Cr nicotinate and 51Cr picolinate in a rat model. Trace Elem Electrolytes 1994; 11: 182–6
Anderson RA, Bryden NA, Polansky MM, et al. Dietary chromium effects on tissue chromium concentrations and chromium absorption in rats. J Trace Elem Exp Med 1996; 9: 11–25
Kaats GR, Wise JA, Blum K, et al. The short-term therapeutic efficacy of treating obesity with a plan of improved nutrition and moderate caloric restriction. Curr Ther Res 1992; 51: 261–74
Krieder RB, Klesges R, Harmon K, et al. Effects of ingesting supplements designed to promote lean tissue accretion on body composition during resistance training. Int J Sport Nutr 1996; 6: 234–46
Pasman WJ, Westerterp-Plantenga MS, Saris WHM. The effectiveness of long-term supplementation of carbohydrate, chromium, fibre and caffeine on weight maintenance. Int J Obes Relat Metab Disord 1997; 21: 1143–51
Evans GW. The effect of chromium picolinate on insulin controlled parameters in humans. Int J Biosocial Med Res 1989; 11: 163–80
Press RI, Geller J, Evans GW. The effect of chromium picolinate on serum cholesterol and apolipoprotein fractions in human subjects. West J Med 1990; 152: 41–5
Hasten DL, Rome EP, Franks BD, et al. Effects of chromium picolinate on beginning weight training students. Int J Sport Nutr 1992; 2: 343–50
Evans GW, Pouchnik DJ. Composition and biological activity of chromium-pyridine carboxylate complexes. J Inorg Biochem 1993; 49: 177–87
Clancy SP, Clarkson PM, DeCheke ME, et al. Effects of chromium picolinate supplementation on body composition, strength, and urinary chromium loss in football players. Int J Sports Nutr 1994; 21: 142–53
Trent LK, Thieding-Canel D. Effects of chromium picolinate on body composition. J Sports Med Phys Fitness 1995; 35: 273–80
Hallmark MA, Reynolds TH, DeSouza CA, et al. Effects of chromium picolinate and resistance training on muscle strength and body composition. Med Sci Sports Exerc 1996; 28: 139–44
Lukaski HC, Bolonchuk WW, Siders WA, et al. Chromium supplementation and resistance training: effects on body composition, strength, and trace element status of men. Am J Clin Nutr 1996; 63: 954–65
Kaats GR, Blum K, Fisher JA, et al. Effects of chromium picolinate supplementation on body composition: a randomized, double-masked, placebo-controlled study. Curr Ther Res 1996; 57: 747–56
Bulbulian R, Pringle DD, Liddy MS. Chromium picolinate supplementation in male and female swimmers [abstract]. Med Sci Sports Exerc 1996; 28 (5 Suppl.): S111
Grant KE, Chandler RM, Castle AL, et al. Chromium and exercise training: effect on obese women. Med Sci Sports Exerc 1997; 29: 992–8
Campbell WW, Beard JL, Joseph LJ, et al. Chromium picolinate supplementation and resistive training by older men: effects on iron-status and hematologic indexes. Am J Clin Nutr 1997; 66: 944–9
Bahadori B, Wallner S, Schneider H, et al. Effects of chromium yeast and chromium picolinate on body composition in obese non-diabetic patients during and after a very-low-calorie diet [German]. Acta Med Austriaca 1997; 24: 185–7
Walker LS, Bemben MG, Bemben DA, et al. Chromium picolinate effects on body composition and muscular performance in wrestlers. Med Sci Sports Exerc 1998; 30: 1730–7
Kaats GR, Blum K, Pullin D, et al. A randomized, double-masked, placebo-controlled study of the effects of chromium picolinate supplementation on body composition: a replication and extension of an earlier study. Curr Ther Res 1998; 59: 379–88
Boyd SG, Boone BE, Smith AR, et al. Combined dietary chromium picolinate and an exercise program leads to a reduction of serum cholesterol and insulin in college-aged subjects. J Nutr Biochem 1998; 9: 471–5
Campbell WW, Joseph LJO, Davey SL, et al. Effects of resistance training and chromium picolinate on body composition and skeletal muscle in older men. J Appl Physiol 1999; 86: 29–39
Joseph LJO, Farrell PA, Davey SL, et al. Effect of resistance training with or without chromium picolinate supplementation on glucose metabolism in older men and women. Metabolism 1999; 48: 546–53
Cefalu WT, Bell-Farrow AD, Stegner J, et al. Effect of chromium picolinate on insulin sensitivity in vivo. J Trace Elem Exp Med 1999; 12: 71–85
Amato P, Morales AJ, Yen SSC. Effects of chromium picolinate supplementation on insulin sensitivity, serum lipids, and body composition in healthy, nonobese, older men and women. J Gerontology 2000; 55A: 14260–3
Livolsi JM, Adams GM, Laguna PL. The effect of chromium picolinate on muscular strength and body composition in women athletes. J Strength Cond Res 2001; 15: 161–6
Volpe SL, Huang HW, Larpadisorn K, et al. Effect of chromium supplementation and exercise on body composition, resting metabolic rate and selected biochemical parameters in moderately obese women following an exercise program. J Am Coll Nutr 2001; 20: 293–306
Nielsen FH. Controversial chromium: does the superstar mineral of the mountebanks receive appropriate attention from clinicians and nutritionists? Nutr Today 1996; 31: 226–33
Evans GW. Dietary supplementation with essential metal picolinates. US patent 4,315,927. 1982 Feb 16
Clarkson PM. Nutritional erogogenic aids: chromium, exercise, and muscle mass. Int J Sport Nutr 1991; 1: 289–93
Moore RJ, Friedl KE. Ergogenic aids: physiology of nutritional supplements: chromium picolinate and vanadyl sulfate. Nat Strength Conditioning Assoc J 1992; 14: 47–51
Lefavi RG, Anderson RA, Keith RE, et al. Efficacy of chromium supplementation in athletes: emphasis on anabolism. Int J Sport Nutr 1992; 2: 111–22
Whitmire D. Vitamins and minerals: a perspective in physical performance. In: Berning JR, Steen SN, editors. Sports nutrition for the 90s. Gaithersburg (MD): Aspen Publishers Inc, 1991: 129–51
Lefavi RG. Chromium picolinate is an efficacious and safe supplement: response [letter]. Int J Sport Nutr 1993; 3: 120–2
Lukaski HC. Chromium as a supplement. Annu Rev Nutr 1999; 19: 279–302
Davis JM, Welsh RS, Alderson NA. Effects of carbohydrate and chromium ingestion during intermittent high-intensity exercise to fatigue. Int J Sport Nutr Exerc Metab 2000; 10: 476–85
Clarkson PM. Effects of exercise on chromium levels: is supplementation required? Sports Med 1997; 23: 341–9
Anderson RA. Effects of chromium on body composition and weight loss. Nutr Rev 1998; 56: 266–70
Hellerstein MK. Is chromium supplementation effective in managing type II diabetes? Nutr Rev 1998; 56: 302–6
Kreider RB. Dietary supplements and the promotion of muscle growth with resistance exercise. Sports Med 1999; 27: 97–110
Lukaski HC. Magnesium, zinc, and chromium nutriture and physical activity. Am J Clin Nutr 2000; 72Suppl. 2: S585–93
Kobla HV, Volpe SL. Chromium, exercise, and body composition. Crit Rev Food Sci Nutr 2000; 40: 291–308
United States of America before Federal Trade Commission, Docket No. C-3758 [online]. Available from URL: www.ftc.gov/os/1997/9707/nutrit~l.htm and www.ftc.gov/os/1997/9707/nutrit~2.htm [Accessed 1997 Jul 18]
Althius MD, Jordan NE, Ludington EA, et al. Glucose and insulin responses to dietary chromium supplements: a metaanalysis. Am J Clin Nutr 2002; 76: 148–55
Anderson RA, Bryden NA, Polansky MM, et al. Effects of carbohydrate loading and underwater exercise on circulating Cortisol, insulin, and urinary losses of chromium and zinc. Eur J Appl Physiol 1991; 63: 146–50
Stearns DM, Wise Sr JP, Patierno SR, et al. Chromium(III) picolinate produces chromosome damage in Chinese hamster ovary cells. FASEB J 1995; 9: 1643–8
Bagchi D, Bagchi M, Balmoori J, et al. Comparative induction of oxidative stress in cultured J774A: 1 macrophage cells by chromium picolinate and chromium nicotinate. Res Commun Mol Pathol Pharmacol 1997; 97: 335–46
Stearns DM, Silveira SM, Wolf KK, et al. Chromium(III) tris(picolinate) is mutagenic at the hypoxanthine (guanine) phopshoribosyl transferase locus in Chinese hamster ovary cells. Mutat Res 2002; 513: 135–42
Manygoats KR, Yazzie M, Stearns DM. Ultrastructural damage in chromium picolinate-treated cells: a TEM study. J Biol Inorg Chem 2002 Sep; 7(7–8): 791–8
Stearns DM, Beibruno JJ, Wetterhahn KE. A prediction of chromium(III) accumulation in humans from chromium dietary supplements. FASEB J 1995; 9: 1650–7
Speetjens JK, Collins RA, Vincent JB, et al. The nutritional supplement chromium(III) tris(picolinate) cleaves DNA. Chem Res Toxicol 1999; 12: 483–7
Sun Y, Ramirez J, Woski SA, et al. The binding of trivalent chromium to low-molecular-weight chromium-binding substance (LMWCr) and the transfer of chromium from transferrin and Cr(pic)3 to LMWCr. J Biol Inorg Chem 2000; 5: 129–36
Sugden KD, Geer RD, Rogers SG. Oxygen radical-mediated DNA damage by redox-active Cr(III) complexes. Biochemistry 1992; 31: 11626–31
Chakov NE, Collins RA, Vincent JB. Re-examining the electronic spectra of chromium(III) picolinate complexes and high yield synthesis and characterization of Cr2(μ-OH)2(pic)4.5H2O (Hpic = picolinic acid). Polyhedron 1999; 18: 2891–7
Gammelgaard B, Jensen K, Steffansen B. In vitro metabolism and permeation studies in rat jejunum: organic chromium compared to inorganic chromium. J Trace Elem Med Biol 1999; 13: 82–8
Hepburn DDD, Vincent JB. The in vivo distribution of chromium from chromium picolinate in rats and implications for the safety of the dietary supplement. Chem Res Toxicol 2002; 15: 93–100
Hepburn DDD, Burney JM, Woski SA, et al. The nutritional supplement chromium picolinate generates oxidative DNA damage and peroxidized lipids in vivo. Polyhedron. In press
Hepburn DDD, Vincent JB. The tissue and subcellular distribution of chromium picolinate with time after entering the bloodstream: the potential for deleterious effects from the dietary supplement. J Inorg Biochem. In press
Kareus SA, Kelley C, Walton HS, et al. Release of Cr(III) from Cr(III) picolinate upon metabolic activation. J Hazard Mater 2001; B84: 163–74
Anderson RA, Bryden NA, Polansky MM. Lack of toxicity of chromium chloride and chromium picolinate in rats. J Am Coll Nutr 1997; 16: 273–9
Cerulli J, Grabe DW, Gauthier I, et al. Chromium picolinate toxicity. Ann Pharmacother 1998; 32: 428–31
Wasser WG, D’Agati VD. Chronic renal failure after ingestion of over-the-counter chromium picolinate [letter]. Ann Intern Med 1997; 126: 410
Martin WR, Fuller RE. Suspected chromium picolinate-induced rhabdomyolysis. Pharmacotherapy 1998; 18: 860–2
Fowler Jr JF. Systemic contact dermatitis caused by oral chromium picolinate. Cutis 2000; 65: 116
Huszonek J. Over-the-counter chromium picolinate [letter]. Am J Pyschiatry 1993; 150: 1560–1
Young PC, Turiansky GW, Bonner MW, et al. Acute generalized exanthematous postulosis induced by chromium picolinate. J Am Acad Dermatol 1999; 41: 820–3
Bunner SP, McGinnis R. Chromium-induced hypoglycemia [letter]. Psychosomatics 1998; 39: 298–9
Kato I, Vogelman JH, Dilman V, et al. Effect of supplementation with chromium picolinate on antibody titers to 5-hydroxymethyl uracil. Eur J Epidemology 1998; 14: 621–6
Komorowski JR, Loveday K. Rat chromosomes are unharmed by orally administered chromium picolinate [abstract]. J Am Coll Nutr 1999; 18: 527
Esber HJ, Moreno V, Loveday KS. Evaluation of chromium picolinate in the Ames and the rat in vivo chromosomal aberration assays [abstract]. Mutat Res 1997; 379 (1 Suppl.): S89
Ringden D, Lee SH, Nakajima M, et al. Formation of a substituted l,N-etheno-2′-deoxyadenosine adduct by lipid hydroperoxide-mediated generation of 4-oxo-2-nonenal. Chem Res Toxicol 2000; 13: 846–52
Preuss HG, Grojec PL, Lieberman S, et al. Effects of different chromium compounds on blood pressure and peroxidation in spontaneously hypertensive rats. Clin Nephrol 1997; 47: 325–30
Witmer C, Faria E, Park HS, et al. In vivo effects of chromium. Environ Health Perspect 1994; 102 (3 Suppl.): 169–76
McLeod MN, Gaynes BN, Golden RN. Chromium potentiation of antidepressant pharmocotherapy for dysthymic disorder in 5 patients. J Clin Psychiatry 1999; 60: 237–40
McLeod MN, Golden RN. Chromium treatment of depression. Int J Neuropsychopharmacol 2000; 3: 311–4
Attenburrow MJ, Odontiadis J, Murray BJ, et al. Chromium treatment decreases the sensitivity of 5-HT2A receptors. Psychopharmacology 2002; 159: 432–6
Mehler AH. Formation of picolinic acid and quinolinic acids following enzymatic oxidation of 3-hydroxyanthranilic acid. J Biol Chem 1956; 218: 241–53
Boegman RJ, Jhamandas K, Beninger RJ. Neurotoxicity of tryptophan metabolites. Ann N Y Acad Sci 1990; 585: 261–73
Lonnerdal B, Keen CL, Hurley LS. Zinc binding ligands and complexes in zinc metabolism. Adv Nutr Res 1984; 6: 139–65
DiSilvestro RA, Cousins RJ. Physiological ligands for copper and zinc. Annu Rev Nutr 1983; 3: 261–88
Fernandez-Pol J. Morphological changes induced by picolinic acid in cultured mammalian cells. Exp Mol Pathol 1978; 29: 348–57
Etzel KR, Cortez JE, Johnson DA. The addition of picolinic acid to low protein diets: a word of caution. Nutr Res 1988; 8: 1391–401
Seal CJ. Influence of dietary picolinic acid on mineral metabolism in the rat. Ann Nutr Metab 1988; 32: 186–91
Mirasol F. Chromium picolinate market sees robust growth and high demand [online]. Available from URL: http://www.chemicalmarketreporter.com. Chem Market Rep 2000 Feb 14; 257
Acknowledgements
Research on chromium biochemistry in the author’s laboratory is supported by the American Diabetes Association and the National Institutes of Health.The authors have provided no information on conflicts of interest directly relevant to the content of this review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vincent, J.B. The Potential Value and Toxicity of Chromium Picolinate as a Nutritional Supplement, Weight Loss Agent and Muscle Development Agent. Sports Med 33, 213–230 (2003). https://doi.org/10.2165/00007256-200333030-00004
Published:
Issue Date:
DOI: https://doi.org/10.2165/00007256-200333030-00004