
Abstract
Glucocorticoid (GC) sensitivity depends on glucocorticoid receptor (GR) and heat shock proteins (Hsps). We investigated whether common GR genes (ER22/23EK N363S, Bcl I, and 9β) and adrenocorticotropin receptor promoter polymorphisms influence susceptibility for unilateral adrenal incidentaloma (AI), plus GR and Hsp expression in tumorous (n = 19), peritumorous (n = 13) and normal adrenocortical (n = 11) tissues. Patients (n = 112), population-matched controls (n = 100) and tumor tissues (n = 32) were genotyped for these polymorphisms. Postdexamethasone serum cortisol was higher in patients (p < 0.001). GR gene variants, larger allele of Bcl I (odds ratio (OR) 2.9; 95% confidence interval (CI) 1.7–5.1; p < 0.001] and minor allele of 9β (OR 3.0; 95% CI 1.6–5.7; p < 0.001) were independent predictors of AI. In patients, the first allele is linked with larger tumors (p = 0.002) and the latter with higher postdexamethasone cortisol levels (p = 0.025). Both allele carriers had lesser waist circumference (p = 0.02), similar adrenocorticotropin and higher basal (p = 0.024) and postdexamethasone cortisol concentrations (p < 0.001). Tumorous and constitutional genotypes were similar. GR-D is the major receptor isoform in normal adrenal cortex by Western blotting. Loss of other receptor iso-forms, decrease in immunostaining for GR (p < 0.0001), underexpression of chaperones (p ≤ 0.01) and the presence of inducible Hsp70 were found in adenomas. In conclusion, GR gene variants, C allele of Bcl I and minor allele of 9β, are associated with Als. Their concurrent presence in patients reduces GC sensitivity. Normal adrenal cortex preferentially expresses GR-D. In adenomas, the lack of other GR isoforms and underexpression of heat shock proteins perhaps permanently impair GC signaling, which could promote dysregulated cortisol production and tumor growth. The innate GC sensitivity probably modifies these effects.
Similar content being viewed by others

Introduction
Adrenal tumors are common and reported in 3 –7% of autopsy and radiological series (1). Most of adrenal lesions found incidentally during imaging evaluation (so-called “incidentalomas” [AIs]) in patients with no known malignancy are presumed to be benign adenomas. The prevalence of adrenal masses increases from 3% in middle-age patients to as much as 10% in the elderly (2). Patients with functional adrenal tumors are offered surgery. The generally accepted recommendation regarding clinically nonfunctional masses is to excise lesions >6 cm, whereas masses <4 cm without suspect imaging are not generally resected (3). However, almost 10% of adrenocortical carcinomas lie within the size range of 3–5 cm (4). Most of adrenocortical masses are considered nonhypersecretory adenomas, although 5–25% of them secrete cortisol autonomously (5,6) and high incidence of obesity, diabetes and hypertension is detected among patients with these tumors (6,7).
Considerable interindividual variations in glucocorticoid (GC) sensitivity depend on glucocorticoid receptor (GR) gene polymorphisms, as demonstrated by a variable suppressive response to 0.25 mg dexamethasone (8). It is likely that GR provides feedback regulation of adrenocortical steroid production (9). Additionally, functional characteristics of GR depend on receptor-associated proteins including several mammalian heat shock proteins (Hsps) (10–13). So far, few studies have attempted to characterize GR expression in benign adrenocortical tumors (14,15), whereas there is no information regarding Hsp synthesis in these tumors. Clinical presentation of patients with Als could result from interaction between GC sensitivity determined by the hypothalamo-pituitary-adrenal (HPA) axis genotype and inappropriate cortisol secretion from an adrenocortical tumor.
We wanted to determine whether functional polymorphisms in GR and adrenocorticotropic hormone receptor (ACTHR) genes influence susceptibility for unilateral AI and GC sensitivity in these patients. We also investigate the expression of GR and molecular chaperons in the tissue samples of adrenocortical adenomas and corresponding adjacent and normal adrenal cortex.
Materials and Methods
Study Subjects
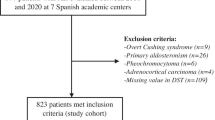
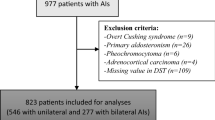
The study group consisted of 116 consecutive Caucasian patients referred to our unit (Department of Endocrine Oncology) from 2006 to 2007 for the presence of unilateral and incidentally discovered adrenal mass. However, after the exclusion of four patients with proven adrenocortical carcinoma, 112 patients (83 women, age 25–80 years) entered the study. The following were criteria for study inclusion: (a) incidental discovery of an adrenal mass by radiological investigation performed for unrelated reasons; (b) the absence of symptoms and signs of endocrine/neuroendocrine disease and hypokalemia (≤3.5 mmol/L), except for hypertension, disturbed glucose tolerance and obesity; (c) no abnormalities in 17-hydoxyprogesterone, mineralocorticoid (upright plasma renin activity and aldosterone), androgen (plasma total testosterone, androstenedione and dehydroepiandrosterone-sulfate) or 24-h urinary catecholamine concentrations; and (d) radiological features of nonmalignancy. Diagnosis of adrenal mass was confirmed by high-resolution imaging techniques such as computerized tomography or magnetic resonance imaging in all patients.
To assess 24-h cortisol rhythm, determinations for morning cortisol at 0900 h and night cortisol at 2000 h and 2400 h were performed in all patients. Plasma concentration of adrenocorticotropin hormone (ACTH) was available for all patients; all patients underwent suppression testing with 1 mg overnight dexamethasone. Adrenocortical adenoma was found in 40 of 44 surgical patients and adrenocortical carcinoma in 4 of 44 surgical patients. Adenomatous tissue samples with or without surrounding adrenocortical tissue could be obtained from 32 of the 40 patients with adrenocortical adenoma. The control group consisted of 100 age-, sex- and body mass index (BMI)-matched healthy control subjects (65 women; age 28–76 years). They entered the study after the exclusion of the presence of adrenal mass by ultrasonography. All subjects gave informed written consent to participate in the study. Clinical characteristics of patients and control subjects are given in Table 1.
Biochemical and Hormonal Analyses
Plasma glucose was determined by the glucose oxidase method (Beckman Glucose Auto-Analyzer, Fullerton, CA, USA). Serum cholesterol and triglycerides concentrations were measured by using commercial enzymatic methods.
Insulin concentration was determined by radioimmunoassay (RIA) (Institute for the Application of Nuclear Energy [INEP], Zemun, Serbia); lower limit of sensitivity was 3.0 mU/L, whereas intra-and interassay coefficients of variations (CVs) were <10.0%. Cortisol concentration was measured by RIA (CORT-CT2; CIS Bio International, Gif-Sur-Yvette Cedex, France). Minimum detectible concentration was 4.6 nmol/L; intra- and interassay CVs were 5.4% and 7.3%, respectively. ACTH was measured by immunoradiometric assay (CIS Bio International); sensitivity of the method was 5 pg/mL, with intra- and interassay CVs ranging from 3.1% to 8.9%.
DNA Extraction and Genotyping
Genomic DNA was extracted from peripheral blood leukocytes of patients and control subjects plus from the tumor tissue samples (n = 32) by using the proteinase K and phenol-chloroform technique.
Characterization of two GR gene polymorphisms, intronic BclI (rs41423247) and ER22/23EK (rs6189 and rs6190) in exon 2, was performed by polymerase chain reaction (PCR) with restriction fragment-length polymorphism (RFLP) analysis. The PCR fragments were digested with 4 U BclI or MnlI restriction enzyme (Fermentas UAB; Thermo Fisher Scientific, Vilnius, Lithuania). We used an allele-specific PCR method for the detection of N363S (rs6195) polymorphism in exon 2 of the GR gene. Products of this reaction were control fragment of 357 bp in each tube and a specific fragment of 306 bp in tubes where the allele corresponding to the specific primer (363M or 363W) was present. To detect the presence or absence of polymorphism within the transcription initiation site of the ACTHR promoter, we used PCR and RFLP reaction. PCR products were digested with 4 U SacI restriction enzyme (Fermentas UAB; Thermo Fisher Scientific). Fragments obtained by RFLP and allele-specific PCR were separated by 3.5% agarose gel electrophoresis and visualized by ethidium-bromide.
Single nucleotide polymorphism A3669G (rs6198) located in the 3′ end of exon 9β of GRβ was characterized by DNA sequencing after PCR amplification. Results obtained by RFLP or allelespecific PCR analysis for all GR and ACTHR gene polymorphisms were confirmed by sequencing on an automated ABI PRISM 3130 Genetic Analyzer (Applied Biosystems; Life Technologies, Carlsbad, CA, USA) and analyzed with AB DNA Sequencing Analysis Software (v5.2) by using the Big Dye Terminator v3.1 and v1.1 Ready Reaction Cycle Sequencing Kit, respectively. Primers used in PCR with PCR ingredients, thermocycler and RFLP conditions for detection of each polymorphism are available on request.
Tissue Preparation
Tissue samples of 19 adrenocortical adenomas with 13 corresponding surrounding tissue samples of adrenal cortex were obtained from patients who underwent adrenalectomy. Tissue samples of normal human adult adrenal gland were provided from 11 patients who underwent nephrectomy because of renal cell carcinoma, tumor stage 1. After taking a small part for DNA extraction, each sample was divided into approximately equal parts for standard microscopy, including immunohistochemistry and Western blot analysis. Tissue samples for Western blot analysis were immediately frozen in liquid nitrogen and stored at −80°C until use.
Immunohistochemistry
A total of 19 paraffin-embedded adrenal cortical adenomas with 13 corresponding adjacent peritumoral tissue samples were studied by immunohistochemistry, and 11 frozen or formalin-fixed paraffin-embedded, normal human adrenal tissues were used as positive controls in immunohistochemistry.
The GR immunoreactivity (GR-ir) was evaluated by using rabbit polyclonal antibody raised against a peptide mapping at the N-terminus of murine GR (GR M-20; 1:300; Santa Cruz Biotechnology, Santa Cruz, CA, USA) and strepta-vidin-biotin complex method (DAKOLSAB+/Peroxidase Labeling kit, K0690; DAKO, Copenhagen, Denmark). The GR (M-20) antibody recognizes both α and β isoforms of human GR. The same technique of immunostaining was used with rabbit polyclonal antibody specifically raised against GRβ (PA3-514; Thermo Fisher Scientific Inc., Waltham, MA, USA).
Immunohistochemistry was performed on 5-µm serial sections from each specimen. After deparaffinization, the sections were heated for 2 min in a pressure cooker in 10 mmol/L citrate buffer (pH 6.0) for epitope retrieval. Endogenous peroxidase activity was blocked with 0.3% hydrogen peroxide in methanol. After that, tissue sections were incubated with anti-GR antibody (60 min, room temperature), washed with phosphatebuffered saline (pH 7.4) and incubated with biotinylated anti-mouse, anti-rabbit and anti-goat immunoglobulins for 30 min and with peroxidase-conjugated streptavidin-biotin for another 30 min. Antigen-antibody complexes were visualized with 3,3′-diamino-benzidine substrate solution (Liquid DAB+ Substrate Chromogen System, ready-to-use, K3468; DAKO Cytomation). Finally, the cell nuclei were counterstained with Mayer’s hematoxylin. Both omission of the primary antiserum and replacement of the first layer of antibody by specific blocking peptide (Santa Cruz, sc-1004P) were used as negative controls.
Quantification of nuclear and cytoplasmic GR expression was performed by using Analysis Pro 3.2 software. Immunoreactive cells were counted in five representative zones of each specimen of cortical adenoma, peritumoral and normal adrenocortical tissue. The results were expressed as a number of positive per 1,000 cells and as an intensity of immunostaining (weak 1+, moderate 2+ and strong 3+). Total score of immunostaining intensity was obtained by assessing 1,000 cells for each category of intensity. Only the cells with intensive immunostaining of nuclei and cytoplasm were considered positive. The range of counted cells in different zones was 529 to 1,086 in cortical adenomas, 500 to 963 in peritumoral area and 1,117 to 1,403 in normal cortex.
Western Blot Analysis
Tumor, peritumorous and normal adrenocortical tissue lysates were prepared by homogenization of fresh, frozen tissue samples in lysis buffer containing 0.1% Triton X-100 (Sigma-Aldrich, St. Louis, MO, USA) and triple protease inhibitor (Roche Applied Science, Mannheim, Germany). The samples were denatured (70°C for 10 min) before elec-trophoresis on precast 4–12% Bis-Tris gels (Invitrogen; Life Technologies). Separated proteins were transferred to Hybond ECL nitrocellulose membranes (GE Healthcare, Piscataway, NJ, USA). The membranes were washed in Tris-buffered saline with 0.1% Tween 20 (TBST) and subsequently blocked in TBST containing 5% (wt/vol) nonfat dry milk powder for 1 h at room temperature. Blots were then probed with GR (clone 4H2, NCL-GCR; Novocastra; Leica Biosystems Newcastle Ltd, Newcastle upon Tyne, UK) at 1:100 overnight at 4°C. After washing in TBST, the blots were probed with peroxidaseconjugated goat anti-mouse secondary antibody (1:5,000) for 1 h at room temperature. The Amersham ECL Plus Western blotting detection reagents (GE Healthcare) were used to visualize the detected proteins. Protein loading was normalized to β-actin by AC-15 antibody (Sigma-Aldrich). Protein lysates were derived from MCF-7 cells, and human lymphocytes served as positive controls for GR expression.
For determination of Hsp70 and Hsp90 concentrations in tissue lysates, proteins were separated by 4–12% sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) and electrotransferred to nitrocellulose membranes, and the membranes were incubated with SPA-820 (Stressgen) and CA (SC-13119) (Santa Cruz Biotechnology) primary antibodies, respectively. After visualization of the immunoreactive bands, the membranes were stripped with 0.2 mol/L NaOH, blocked and probed for β-actin by AC-15 antibody (Sigma-Aldrich).
Densitometry
Immunoreactive bands were visualized by an enhanced chemifluorescence reaction (ECF) (Amersham Pharmacia Biotech, Little Chalfont, Amersham, UK) and their relative optical densities were measured by the STORM scanner (Amersham). Quantitative analysis was done by ImageQuant software. β Actin was used as an equal load control.
Statistics
We used the homeostasis model assessment-insulin resistance (HOMA-IR) to assess insulin resistance (16). Depending on the variable type used in comparisons, differences among the groups were determined with Pearson χ2 test or one-way analysis of variance. Only comparisons in GR-ir between tissue samples (cortical adenoma, peritumoral and normal cortex) were assessed by the Kruskal-Wallis test. To test deviations from the Hardy-Weinberg principle, we applied the χ2 test by using the observed genotype frequencies obtained from the data and the expected genotype frequencies obtained by using the Hardy-Weinberg principle. Crude odd ratios (ORs), as estimates of the relative risk for adrenocortical tumor, were calculated with 95% confidence intervals (CIs) and accordingly expressed with lower and upper bounds. For all but the BclI polymorphism, ORs were calculated from the proportion of minor allele carriers in patients and controls. In the case where one frequency was 0, we added the minimal positive value (1) in each of four cells in a 2 × 2 table and calculated the OR and corresponding 95% CI after this operation. The haplotypes for the patients and control subjects were reconstructed by using the program Phase (version 2.1, Matthew Stephens Lab, University of Chicago, Chicago, IL, USA) (17). The presented p values are two-sided throughout, and p < 0.05 was considered statistically significant.
Results
Clinical Characteristics of Patients and Control Subjects
Anthropometric and biochemical characteristics of patients and control subjects are presented in Table 1. Although there was no difference in waist circumference between patients and controls, values >88 cm for women and >102 cm for men were significantly more frequent among patients. They also had higher values of blood pressure and glucose concentration but not HOMA-IR index. There was no difference in morning cortisol concentration between patients and control subjects, but postdexamethasone (post-Dex) values were significantly lower in controls. In patients, basal cortisol and insulin correlated positively (r = 0.19; p = 0.043), whereas post-Dex cortisol was in negative association with waist girth (r = −0.32; p = 0.001). Systolic and diastolic blood pressure levels correlated with BMI (r = 0.22; p = 0.019 and r = 0.21; p = 0.022) and waist girth (r = 0.22; p = 0.020 and r = 0.23; p = 0.017), and blood glucose correlated with basal insulin (r = 0.33; p < 0.001). In controls, basal cortisol was related to glucose (r = 0.31; p = 0.002) and ACTH (r = 0.30; p = 0.037) concentrations, and post-Dex cortisol was related to systolic blood pressure (r = 0.26; p = 0.013) and age (r = −0.43; p = 0.027). As in patients, systolic and diastolic blood pressure correlated with BMI (r = 0.20; p = 0.049 and r = 0.22; p = 0.031) and waist girth (r = 0.26; p = 0.010 and r = 0.28; p = 0.006).
Genotyping
Table 2 includes the frequency of different alleles in the tested populations. We identified three BclI sites around exon 2 of the GR gene: one in intron 1 and two in intron 2. The polymorphic site in intron 2 (647 bp from the exon/intron junction) produced the fragment sizes of 3.9 kb in the absence and 2.2 kb in the presence of the BclI site. Sequence analysis confirmed G-to-C transition 646 bp downstream of exon 2, which abolished the BclI restriction site (TGATCA → TCATCA) as reported previously (18). The obtained fragment sizes (3.9 and 2.2 kb) were slightly different from those originally reported (4.5 kb and 2.2 kb) (19). The frequency of larger C allele carriers of the BclI polymorphism and the prevalence of a naturally occurring ATTTA to GTTTA single nucleotide polymorphism located in the 3′ end of exon 9β in the GR gene were significantly higher among patients than in control subjects. These two alleles of the GR gene are in linkage disequilibrium (D′ = 0.172). There was no difference in the frequencies of N363S and ER22/23EK gene variants of GR between patients and controls. We did not detect homozygous individuals for N363S and ER22/23EK polymorphisms in the GR gene in studied subjects. There was no difference in the frequency of the ACTHR gene promoter polymorphism between patients and controls. Carriers of the C allele of BclI or minor allele of the 9β GR gene polymorphisms are at higher risk to develop AI (Table 2). Identical genotypes of GR and ACTHR were obtained from the tumorous and constitutive DNA. Figure 1 presents reconstructed haplotypes with relative positions of GR gene polymorphisms. The frequencies of haplotypes were significantly different in patients and control subjects (p = 0.01). All examined allele frequencies were in the Hardy-Weinberg equilibrium.

Polymorphisms in the glucocorticoid receptor gene and reconstructed haplotypes. Position of the polymorphisms is indicated in relation to the gene (top), and the haplotypes with their frequencies are shown (bottom). The number of observed haplotypes is shown in parentheses.
Relationship Between Gene Variants and Phenotypes
GR gene polymorphisms that were present with higher frequency among patients and their effects on clinical characteristics are presented in Table 3. Because of the small number of subjects homozygous for all assessed GR and ACTHR gene polymorphisms, these cases were merged with the heterozygotes to compare carriers with noncarriers. Carriers of the C allele of the BclI gene variant had larger tumors; however, attendance of the 3669G polymorphism apparently attenuates the effect on tumor size (Table 4). Patients carrying the minor G allele of the 9β polymorphism had lower values of BMI, fasting glucose and post-Dex cortisol concentration compared to noncarriers, indicating lower sensitivity to GCs. These patients also tended to have higher basal cortisol levels and lower waist circumferences, but these levels did not reach statistical significance. This effect of 9β polymorphism is potentiated by the presence of the C allele of the BclI polymorphism, since patients carrying both of these alleles at the same time had significantly higher concentrations of morning and post-Dex cortisol concentrations for the same ACTH level, as well as lower values of waist circumference and BMI compared to noncarriers (see Table 4). In carriers of these two polymorphisms, post-Dex cortisol concentration was in negative correlation with BMI (r = −0.64; p = 0.002), waist circumference (r = −0.63; p = 0.003) and ACTH concentration (r = −0.43; p = 0.049), whereas glycemia correlated with BMI and waist girth (r = 0.44; p = 0.047 for both), systolic and diastolic blood pressure (r = 0.50; p = 0.022 and r = 0.57; p = 0.007) and basal insulin (r = 0.44; p = 0.048). Basal insulin was in positive association with post-Dex cortisol concentration (r = 0.28; p = 0.009) and glycemia (r = 0.32; p = 0.003), whereas systolic blood pressure correlated only with glycemia (r = 0.28; p = 0.009) in patients noncarriers of the two alleles.
Regional and Intracellular Distribution of GR
GR-ir was moderately expressed in the adrenal cortex of the normal human adrenal gland, with the strongest staining within the zona reticularis (Figure 2A) using an antibody that recognizes both isoforms of the receptor protein (anti-GRα/β) and in zona glomerulosa when anti-GRβ was applied (Figure 2B). Immunoreactivity for both isoforms of GR was present in adenomatous and periadenomatous tissue (Figures 2C, F). Cellular localization of the GR in examined tissues was nuclear and cytoplasmic. The number of immunostained cells was significantly lower in adenomatous tissue than in normal adrenal cortex (Figure 3A). Total immunostaining score for GR was reduced in examined adrenocortical adenomas compared with control adrenal cortex or peritumorous tissue, regardless of antibody used (Figure 3B); this result is in line with lower expression of both α and β isoforms of the receptor protein in these tumors. A decrease in total immunostaining score in peritumorous tissue was obtained with anti-GRα/β, but not with anti-GRβ, suggesting underexpression only of GRα in peritumorous tissue. This result was confirmed with reduced nuclear (Figure 3C) and cytoplasmic (Figure 3D) scores, which follow a similar pattern of total immunostaining score, suggesting underexpression of both GRα and GRβ in tumorous tissue, but only GRα in peritu-morous tissue. Nuclear score was significantly higher than cytoplasmic for GRβ in all examined tissues confirming dominant nuclear localization of GRβ.

(A) Normal adrenal cortex displayed positive focal immunostaining for glucocorticoid receptor (GR) by using an antibody that recognizes α and β isoforms of the receptor (anti-GRβα/β) in the zona reticularis (zr). (B) β Isoform of GR is expressed predominantly in the zona glomerulosa (zg) of normal adrenal cortex. (C) Tumorous (at) and peritumorous (pt) tissue stained with anti-GRα/β. Both tissues show immunoreactivity. (D) Immunoreactivity for GRβ is seen in the tumor (at) and in adjacent peritumorous tissue (pt). Focal and weak staining with anti-GRα/β (E) and with anti-GRβ (F) are demonstrated in adenomatous tissue. Cellular localization of GR is nuclear and/or cytoplasmic. Magnifications are presented in the lower right-hand corner of each photograph.

Regional and subcellular distribution of GR. (A) The number of immunostained cells in adenomatous tissue is reduced compared to normal human adrenal cortex. Similar results were obtained by using antibody that recognizes both a and β isoforms of GR (anti-GRα/β) or by anti-GRβ. (B) Total immunostaining intensity score is reduced in adenomatous tissue compared to control or peritumorous tissue, regardless of antibody used. The decrease in immunostaining score in peritumorous tissue was detected only when anti-GRα/β was applied, suggesting GRα underexpression. Nuclear (C) and cytoplasmic (D) scores follow similar pattern of total immunostaining intensity score; GRβ is predominantly located within nuclei of all examined tissues. *p < 0.001 versus normal or adjacent tissue and normal or adenomatous tissue.
Western Blot Analysis: GR and Heat Shock Proteins
Western blot analysis of GR isoforms in lysates of normal human adrenal cortex, periadenomatous and adenomatous tissues revealed dominant and similar expression of the 53- to 56-kDa receptor protein. Other N-terminal isoforms of GR were detected only in nontumorous tissue, and these isoforms lacked 17 of 19 analyzed tumorous tissues (Figure 4). The 73-kDa constitutive heat shock cognate protein (Hsc70) and Hsp90 were detected in tumorous, peritumorous and normal adrenocortical tissues (Figures 5A, C), but the stress-inducible 72-kDa Hsp70 was expressed only in the tumor tissue (Figure 5A). The expression of Hsp70 and Hsp90 in peritumorous and tumorous tissues were reduced in comparison to normal adrenal cortex (Figures 5B, D).

Representative Western blot for GR. (A) The MCF-7 cells and human lymphocytes (Ly) were used as positive controls. Monoclonal anti-GR antibody, which recognizes the α and β transcriptional isoforms of GR, reveals the presence of bands of about 100 kDa; however, the dominant 53- to 56-kDa receptor isoform that corresponds to GR-D is detected in normal adrenal cortex (AC) and periadenomatous (PT) tissue. In the majority of tumor samples (T), GR-D is the only isoform that can be seen. (B) GR-D expression was similar in normal adrenal cortex, peritumorous and tumorous tissues.

Western blot analysis of the whole-cell lysate for heat shock proteins. (A) Inducible form of Hsp70 (the lower band) was expressed only in the tumor tissue (T). (B) The expression of total Hsp70 in the tumor (the sum of two protein isoforms) and adjacent normal tissue (PT) was reduced compared to the normal adrenal cortex (AC). (C) The expression of Hsp90 in control adrenal cortex, adenomatous and adjacent tissue. (D) Relative expression of Hsp90 is reduced in adrenocortical adenomas and adjacent peritumorous tissue compared to normal adrenal cortex. *p ≤ 0.01 versus control tissue.
Discussion
We have shown that GR gene variants associated with unilateral AI in a Serbian Caucasian population also reduce sensitivity to GCs. For the first time, we show that normal human adrenal cortex, among multiple N-terminal isoforms of GR, preferentially expresses GR-D. The vast majority of AIs are adrenocortical adenomas characterized by the absence of other receptor isoforms except GR-D accompanied by reduced expression of molecular chaperones. Genotypes of GR and ACTHR from these tumors and constitutional DNA were alike.
In the present study, the majority of patients were women in the sixth decade of life. Although both patients and control subjects had similar morning cortisol, basal insulin and BMI values, only patients were showing increased visceral fat and higher blood glucose concentration and blood pressure, suggesting the coexistence of insulin resistance and metabolic syndrome (6,7). The relationship between cortisol action, visceral fat, insulin resistance and hypertension in simple obesity, which can be reminiscent of exposure to chronic stress, was demonstrated previously (20,21). Circulating cortisol may not reflect its activity in target tissues. Increased visceral fat in our patients could be related to 11β-hydroxysteroid dehydrogenase type 1 (11β-HSD1) activity, which converts inactive circulating 11-keto steroids into active GCs, amplifying local GC action. Overexpression of 11β-HSD1 in all adipose tissues of transgenic mice and visceral adipose expanding are related to increased expression of GRα (22). Higher blood pressure in patients could be linked with increased portal-venous supply of free fatty acids or other adipokines from visceral fat due to insulin resistance, which activate sympathetic system and serve as a secretagogue for aldosterone (23).
In our study, higher post-Dex cortisol levels were found in patients, while polymorphisms of the GR gene, larger allele of BclI or minor allele of 9β, were associated with the predisposition to develop AI. The first gene variant also influences tumor size, whereas the 9β polymorphism reduces the ability of dexamethasone to suppress cortisol, indicating its effect on GC sensitivity in patients. Along with their increased presence in patients, we also demonstrated association of the two alleles with anthropometric, endocrine and metabolic characteristics of patients. GC resistance is potentiated by the larger C allele of BclI polymorphism, since patients/carriers of both alleles had similar ACTH, higher morning and post-Dex cortisol concentrations and lower waist circumference and BMI values than noncarriers. Higher cortisol concentrations in these patients possibly result from the interaction between autonomous cortisol secretion from adrenal tumors and HPA axis genotype associated with reduced sensitivity to GCs at the same time. Various studies report that subjects carrying a larger allele of BclI polymorphism of GR gene have increased visceral obesity, higher systolic blood pressure, elevated cortisol concentrations after a standardized meal, reduced ability of 0.25 and 1.0 mg dexamethasone to suppress cortisol in elderly and elevated fasting insulin concentrations in obese perimenopausal women. On the contrary, the minor G allele is associated with lower cortisol after dexamethasone suppression and a tendency to lower lean body mass in the elderly, a higher blood pressure with adverse lipid profile in obese and an increased skeletal sensitivity to GCs in patients with AIs, as well as in individuals with endogenous GC excess (24–30). It has been shown that the 3669G allele of the GR gene polymorphism, located in an AUUUA motif of the 3’UTR (untranslated region) of exon 9β, is associated with a more favorable metabolic profile due to a greater stability of GRβ mRNA and increased synthesis of GRβ, which antagonize the action of hGRα (31–33). Our data suggest the functional importance of BclI alleles in linkage disequilibrium with other GR genetic variants (that is, C allele of BclI seems to enhance the effects of the minor allele of the 9β gene variant on GC sensitivity). Although the BclI polymorphism is intronic, its effect on GR gene activity may be indirect through selective effects on repressor or enhancer sites within the gene promoter. By interacting with either repressor or enhancer sites, GC sensitivity would be decreased or increased (34). There was no difference in the prevalence of the ACTHR promoter polymorphism or N363S and ER22/23EK gene variants of GR between patients and control subjects, although the last variant was associated with GC insensitivity (35). The existence of a specific link between GR genotypes and HPA axis-related phenotypes in patients suggests that innate GC sensitivity could be either a protective or vulnerability factor to cortisol actions.
Genotypes of GR obtained from tumorous and constitutional DNA samples were similar. We have shown dominant expression of GR isoforms corresponding to GR-D in normal adrenal cortex; however, other N-terminal isoforms were also present. This was not the case with majority of tumorous samples in which only the GR-D isoform was found by Western blotting. In vitro, the GRα-D exhibits weak transcriptional activity on a synthetic GRE-driven promoter compared to GRα-A. It resides primarily in the nucleus, irrespective of the presence or absence of ligand (36,37). Because GRα and GRβ mRNA differs only on their 3′ ends, it was proposed that multiple N-terminal isoforms may also exist for GRβ (38). Thus, dominant expression of the GR-D isoform seems to be tissue specific, and it could be responsible for the physiological resistance of adrenal cortex to GCs (39), since GR provides feedback regulation of adrenocortical steroid production (9). Selective expression of GR-D and the absence of other receptor isoforms in tumorous tissue are in line with reduced immunoreactivity for GR. Nuclear localization of GRβ in all examined tissues possibly indicates its active role in decreasing GRα transcriptional activity (33). Reduced synthesis of heat shock proteins within these tissues during surgery may be due to the impaired ability of anesthetics to activate and/or increase the ability of GR to inhibit heat shock transcription factor-1 (40,41). Our results are consistent with reports demonstrating GR in normal adrenal cortex of different species (42–48), the absence of GR mRNA and dexamethasone binding sites and reduced GR protein expression in cortisol-secreting adenomas and bilateral adrenal hyperplasia (14,48,49). However, overexpression of GR in benign cortisol-secreting adenomas and adrenocortical carcinomas have been shown as well (15,50), possibly reflecting different pathogenesis of these tumors. Altogether, our results suggest three independent mechanisms of GC resistance in clinically nonfunctioning adrenocortical adenomas exist: the constitutionally reduced sensitivity to GCs, selective expression of GR-D isoform and the decrease of Hsp synthesis (51,52). The first two mechanisms may operate in the normal adrenal cortex.
The inability of GR-D to downregulate the expression of GC-controlled prosurvival genes possibly influences the growth of adenoma (54,55), and this result could be potentiated by the lack of other N-terminal isoforms of receptors in adenomatous tissue. It appears that the observed effect of the C allele of the BclI polymorphism on tumor size cannot be mediated through tumorous GR, whereas the effect of 9β polymorphism of the GR gene on sensitivity to GCs can be obtained in tumorous and nontumorous tissues. Whether the loss of GC sensitivity might be the primary event in the pathogenesis of these tumors has yet to be elucidated (49).
Conclusion
GR gene variants C allele of BclI and minor allele of 9β are associated with unilateral AIs. These alleles, especially when present together, reduce sensitivity to GCs. Preferential expression of GR-D in normal adrenal cortex could mediate physiological resistance to GCs of the tissue. In adenomas, the absence of other isofoms except GR-D and underexpres-sion of heat shock proteins perhaps permanently impair GC signaling. The acquired intraadenomatous GC resistance could promote dysregulated cortisol production and tumor growth at the same time, whereas the innate sensitivity to GCs probably modifies these effects.
Disclosure
The authors declare that they have no competing interests as defined by Moleeular Medieine, or other interests that might be perceived to influence the results and discussion reported in this paper.
References
Angeli A, Osella G, Ali A, Terzolo M. (1997) Adrenal incidentaloma: an overview of clinical and epidemiological data from the National Italian Study Group. Horm. Res. 47:279–83.
Kloos RT, Gross MD, Francis IR, Korobkin M, Shapiro B. (1995) Incidentally discovered adrenal masses. Endocr. Rev. 16:460–84.
Mansmann G, et al. (2004) The clinically inapparent adrenal mass: update in diagnosis and management. Endocr. Rev. 25:309–40.
Dackiw APB, Lee JE, Gagel RF, Evans DB. (2001) Adrenal cortical carcinoma. World J. Surg. 25:914–26.
McLeod M, Thomuson N, Gross M, Bondeson A, Bondeson L. (1990) Sub-clinical Gushing’s syndrome in patients with adrenal gland incidentalomas: pitfalls in diagnosis and management. Am. Surgeon. 56:398–403.
Rossi R, et al. (2000) Subclinical Cushing’;s syndrome in patients with adrenal incidentaloma: clinical and biochemical features. J. Clin. Endocrinol. Metab. 85:1440–8.
Terzolo M, et al. (2005) Midnight serum cortisol as a marker of increased cardiovascular risk in patients with a clinically inapparent adrenal adenoma. Eur. J. Endocrinol. 153:307–15.
Huizenga NATM, et al. (1998) A polymorphism in the glucocorticoid receptor gene may be associated with an increased sensitivity to glucocorticoids in vivo. J. Clin. Endocrinol. Metab. 83:144–51.
Gummow BM, Scheys JO, Cancelli VR, Hammer GD. (2006) Reciprocal regulation of a glucocorticoid receptor-steroidogenic factor-1 transcription complex on the Dax-1 promoter by glucocorticoids and adrenocorticotropic hormone in the adrenal cortex. Mol. Endocrinol. 20:2711–23.
Sanchez ER. (1992) Heat shock induces translocation to the nucleus of the unliganded glucocorticoid receptor. J. Biol. Chem. 267:17–20.
Shen P, Xie Z-J, Li H, Sanchez ER. (1993) Glucocorticoid receptor conversion to high affinity nuclear binding and transcription enhancement activity in Chinese hamster ovary cells subjected to heat and chemical stress. J. Steroid. Biochem. Mol. Biol. 47:55–64.
Liu W, Hillmann AG, Harmon JM. (1995) Hormone-independent repression of the AP-1-inducible collagenase promoter activity by glucocorticoid receptors. Mol. Cell. Biol. 15:1005–13.
Sivo J, Harmon JM, Vogel SN. (1996) Heat shock mimics glucocorticoid effects on IFN-γ-induced Fc γ RI and Ia messenger RNA expression in mouse peritoneal macrophages. J. Immunol. 156:3450–4.
Bourdeau I, et al. (2003) Primary pigmented nodular adrenocortical disease: paradoxical responses of cortisol secretion to dexamethasone occur in vitro and are associated with increased expression of the glucocorticoid receptor. J. Clin. Endocrinol. Metab. 88:3931–7.
Boyle B, et al. (2010) Expression of glucocorticoid receptor isoforms in human adrenocortical adenomas. Steroids. 75:695–700.
Matthews DR, et al. (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentration in men. Diabetologia. 28:412–9.
Stephens M, Smith NJ, Donnelly P. (2001) A new statistical method for haplotype reconstruction from population data. Am. J. Hum. Genet. 68:978–89.
Fleury I, et al. (2003) Characterisation of the BclI polymorphism in the glucocorticoid receptor gene. Clin. Chem. 49:1528–31.
Murray JC, Smith RF, Ardinger HA, Weinberger C. (1987) RFLP for the glucocorticoid receptor (GRL) located at 5q11-5q13. Nucl. Acids Res. 15:6765.
Rosmond R, Dallman MF, Bjorntorp P. (1998) Stress-related cortisol secretion in men: relationships with abdominal obesity and endocrine, metabolic and hemodynamic abnormalities. J. Clin. Endocrinol. Metab. 83:1853–9.
Bjorntorp P, Holm G, Rosmond R. (1999) Hypothalamic arousal, insulin resistance and type 2 diabetes mellitus. Diabet. Med. 16:373–83.
Tomlinson JW, et al. (2004) 11β-Hydroxysteroid dehydrogenase type 1: a tissue-specific regulator of glucocorticoid response. Endocr. Rev. 25:831–66.
Peppa M, Maria Krania M, Raptis SA. (2011) Hypertension and other morbidities with Cushing’s syndrome associated with corticosteroids: a review. Integr. Blood Press. Control. 4:7–16.
van Rossum EFC, et al. (2003) Identification of BclI polymorphism in the glucocorticoid receptor gene: association with sensitivity to glucocorticoids in vivo and body mass index. Clin. Endocrinol. 59:585–92.
Weaver JU, Hitman GA, Kopelman PG. (1992) An association between a Bcl1 restriction fragment length polymorphism of the glucocorticoid receptor locus and hyperinsulinaemia in obese women. J. Mol. Endocrinol. 9:295–300.
Rosmond R, et al. (2000) A polymorphism of the 50-flanking region of the glucocorticoid receptor gene locus is associated with basal cortisol secretion in men. Metabolism. 49:1197–9.
Buemann B, et al. (1997) Abdominal visceral fat is associated with a BclI restriction fragment length polymorphism at the glucocorticoid receptor gene locus. Obes. Res. 5:186–92.
Di Blasio AM, et al. (2003) The relation between two polymorphisms in the glucocorticoid receptor gene and body mass index, blood pressure and cholesterol in obese patients. Clin. Endocrinol. 59:68–74.
Szappanos Á, et al. (2009) BclI polymorphism of the glucocorticoid receptor gene is associated with decreased bone mineral density in patients with endogenous hypercortisolism. Clin. Endocrinol. 71:636–43.
Morelli V, et al. (2010) Role of glucocorticoid receptor polymorphism in adrenal incidentalomas. Eur. J. Clin. Invest. 40:803–11.
Syed AA, et al. (2006) Association of glucocorticoid receptor polymorphism A3669G in exon 9beta with reduced central adiposity in women. Obesity (Silver Spring). 14:759–64.
Trementino L, et al. (2012) Association of glucocorticoid receptor polymorphism A3669G with decreased risk of developing diabetes in patients with Cushing’s syndrome. Eur. J. Endocrinol. 166:35–42.
Schaaf MJ, Cidlowski JA. (2002) AUUUA motifs in the 3′UTR of human glucocorticoid receptor alpha and beta mRNA destabilize mRNA and decrease receptor protein expression. Steroids. 67:627–36.
Panarelli M, et al. (1996) Glucocorticoid receptor polymorphism, skin vasoconstriction, and other metabolic intermediate phenotypes in normal human subjects. J. Clin. Endocrinol. Metab. 83:1846–52.
van Rossum EF, et al. (2004) The ER22/23EK polymorphism in the glucocorticoid receptor gene is associated with a beneficial body composition and muscle strength in young adults. J. Clin. Endocrinol. Metab. 89:4004–9.
Nick Z, Lu NZ, Cidlowski JA. (2005) Translational regulatory mechanisms generate N-terminal glucocorticoid receptor isoforms with unique transcriptional target genes. Mol. Cell. 18:331–42.
Duma D, Jewell CM, Cidlowski JA. (2006) Multiple glucocorticoid receptor isoforms and mechanisms of post-translational modification. J. Steroid. Biochem. Mol. Biol. 102:11–21.
Chrousos GP, Kino T. (2005) Intracellular glucocorticoid signaling: a formerly simple system turns stochastic. Sci. STKE. 2005:pe48.
Graybeal ML, Fang VS, Landau RI. (1985) Enhancement of adrenal cortisol secretion after intravenous high dose dexamethasone. J. Clin. Endocrinol. Metab. 61:607–11.
Wu GJ, et al. (2011) Effects of propofol on proliferation and anti-apoptosis of neuroblastoma SH-SY5Y cell line: new insights into neuroprotection. Brain Res. 1384:42–50.
Wadekar SA, Li D, Periyasamy S, Sánchez ER. (2001) Inhibition of heat shock transcription factor by GR. Mol. Endocrinol. 15:1396–410.
Cochet C, Job D, Dhien A, Chambaz EM. (1977) A soluble glucocorticoid binding protein in the bovine adrenal cortex. Arch. Biochem. Biophys. 180:1–9.
Loose DS, Do YS, Chen TL, Feldman D. (1980) Demonstration of glucocorticoid receptors in the adrenal cortex: evidence for a direct dexamethasone suppressive effect on the rat adrenal gland. Endocrinology. 107:137–46.
Yang K, Challis JR. (1989) Fetal and adult sheep adrenal cortical cells contain glucocorticoid receptors. Biochem. Biophys. Res. Commun. 162:604–11.
Root B, Abrassart J, Myers DA, Monau T, Ducsay CA. (2008) Expression and distribution of glucocorticoid receptors in the ovine fetal adrenal cortex: effect of long-term hypoxia. Reprod. Sci. 15:517–28.
Jiang X, Wang J, Luo T, Li Q. (2009) Impaired hypothalamic-pituitary-adrenal axis and its feedback regulation in serotonin transporter knockout mice. Psychoneuroendocrinology. 34:317–31.
Paust HJ, et al. (2006) Expression of the glucocorticoid receptor in the human adrenal cortex. Exp. Clin. Endocrinol. Diabetes. 114:6–10.
Kontula K, Pomoell UM, Gunsalus GL, Pelkonen R. (1985) Glucocorticoid receptors and responsiveness of normal and neoplastic human adrenal cortex. J. Clin. Endocrinol. Metab. 60:283–9.
Bouligand J, et al. (2010) Familial glucocorticoid receptor haploinsufficiency by non-sense mediated mRNA decay, adrenal hyperplasia and apparent mineralocorticoid excess. PLoS One. 5:e13563.
Tacon LJ, et al. (2009) The glucocorticoid receptor is overexpressed in malignant adrenocortical tumors. J. Clin. Endocrinol. Metab. 94:4591–9.
Vanderbilt JN, Miesfeld R, Maler BA, Yamamoto KR. (1987) Intracellular receptor concentration limits glucocorticoid-dependent enhancer activity. Mol. Endocrinol.1:68–74.
Kojika S, et al. (1996) Mechanisms of glucocorticoid resistance in human leukemic cells: implication of abnormal 90 and 70 kDa heat shock proteins. Leukemia. 10:994–9.
Tsagarakis S, et al. (1998) The low-dose dexamethasone suppression test in patients with adrenal incidentalomas: comparisons with clinically euadrenal subjects and patients with Cushing’s syndrome. Clin. Endocrinol. 48:627–33.
Bernini GP, et al. (2002) Apoptosis control and proliferation marker in human normal and neoplastic adrenocortical tissues. Br. J. Cancer. 86:1561–5.
Gross KL, Okley RH, Scoltock AB, Jewell CM, Cidlowski JA. (2011) Glucocorticoid receptor α isoform-selective regulation of antiapoptotic genes in osteosarcoma cells: a new mechanism for glucocorticoid resistance. Mol. Endocrinol. 25:1087–99.
Acknowledgments
The authors are indebted to Neda Drndarevic and Zoran Sinadinovic for technical assistance and hormonal measurements. This study was supported by the Ministry of Science and Technological Development of Serbia (grant III41009).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, and provide a link to the Creative Commons license. You do not have permission under this license to share adapted material derived from this article or parts of it.
The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
To view a copy of this license, visit (https://doi.org/creativecommons.org/licenses/by-nc-nd/4.0/)
About this article
Cite this article
Damjanovic, S.S., Antic, J.A., Ilic, B.B. et al. Glucocorticoid Receptor and Molecular Chaperones in the Pathogenesis of Adrenal Incidentalomas: Potential Role of Reduced Sensitivity to Glucocorticoids. Mol Med 18, 1456–1465 (2012). https://doi.org/10.2119/molmed.2012.00261
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.2119/molmed.2012.00261