
Abstract
The calcium homeostasis modulator 1 (CALHM1) gene codes for a novel cerebral calcium channel controlling Intracellular calcium homeostasis and amyloid-β (Aβ) peptide metabolism, a key event in the etiology of Alzheimer’s disease (AD). The P86L polymorphism in CALHM1 (rs2986017) initially was proposed to impair CALHM1 functionally and to lead to an increase in Aβ accumulation in vitro in cell lines. Recently, it was reported that CALHM1 P86L also may influence Aβ metabolism in vivo by increasing Aβ levels in human cerebrospinal fluid (CSF). Although the role of CALHM1 in AD risk remains uncertain, concordant data have now emerged showing that CALHM1 P86L is associated with an earlier age at onset of AD. Here, we have analyzed the association of CALHM1 P86L with CSF Aβ in samples from 203 AD cases and 46 young cognitively healthy individuals with a positive family history of AD. We failed to detect an association between the CALHM1 polymorphism and CSF Aβ levels in AD patients. Our data, however, revealed a significant association of CALHM1 P86L with elevated CSF Aβ42 and Aβ40 in the normal cohort at risk for AD. This work shows that CALHM1 modulates CSF Aβ levels in presymptomatic individuals, strengthening the notion that CALHM1 is involved in AD pathogenesis. These data further demonstrate the utility of endophenotype-based approaches focusing on CSF biomarkers for the identification or validation of risk factors for AD.
Similar content being viewed by others

Introduction
Alzheimer’s disease (AD) is a progressive neurodegenerative disorder characterized by the presence of senile plaques in different brain regions of the neocortex and hippocampus (1,2). Senile plaques result from the deposition of amyloid-β (Aβ), a series of peptides produced by sequential endoproteolysis of the amyloid precursor protein (APP) by β-secretase/BACE1 and γ-secretase (3,4). The etiology of the sporadic non-Mendelian forms of the disease, which represent nearly 99% of all the AD cases, is still poorly understood. Although there is clear evidence that genetic variation strongly influences the risk of developing sporadic AD, the only robust and unequivocally identified AD risk factor is the ε4 allele of the apolipoprotein E (APOE) gene (5,6). Meta-analyses and genome-wide association studies, however, have revealed recently that multiple independent loci show significant association with AD risk, indicating that other genes are involved in the disease etiology (7–10).
There is evidence suggesting that AD neuropathology may precede clinical symptoms by more than a decade (11–15). Future interventions may be targeted to those at increased risk, before clinical symptoms are manifested. The use of protein biomarkers from cerebrospinal fluid (CSF) as quantitative endophenotypes may be a helpful tool not only for identifying individuals at risk for AD but also for providing an unparalleled opportunity to increase the power of association studies to identify risk alleles (16–19). The use of quantitative endophenotype also may give important biological information in regards to when and by what mechanisms a given gene variant begins to exert a disease-associated impact. Additionally, in the future it may be prudent to follow CSF biomarkers in those at increased genetic risk to time future interventions.
It is well established that decreased Aβ42 in CSF is associated with AD (20–25), perhaps related to increased deposition of insoluble Aβ in brain parenchyma (26). In a sample composed of predominantly non-demented individuals, alterations in CSF levels of Aβ were associated with several putative genetic risk variants, supporting the further investigation of CSF Aβ as an early preclinical marker and endophenotype of AD for studying risk genes (17).
Altered calcium metabolism may be a critical component of the pathogenic process leading to the development of AD (27–32). Recently, our group identified calcium homeostasis modulator 1 (CALHM1) as a gene coding for a novel cerebral calcium channel component controlling cytosolic calcium homeostasis and Aβ metabolism (33). Increased CALHM1 expression in cell culture systems was found to enhance intracellular calcium concentration (33–35) and to reduce Aβ accumulation (33). The P86L polymorphism in the CALHM1 gene (rs2986017) has been associated with increased risk for late-onset AD in some (33,36–38), but not all studies (39–43). Three independent studies, in addition to our initial report (33), also have shown association between an earlier age at onset of AD and homozygosity of the rare allele in CALHM1 P86L (36,40) or a marker in the vicinity of the CALHM1 gene (44). A recent meta-analysis of available data from 24 centers in Europe and the United States of America by Lambert et al. concluded that while the P86L polymorphism may not be an independent risk factor for AD in the cohorts tested, it has a significant impact on the age at onset of AD (45), supporting the notion that CALHM1 controls AD pathogenesis.
Given the evidence in vitro of a relationship between the presence of CALHM1 P86L and increased extracellular Aβ concentrations (33), investigation of CSF Aβ concentrations with respect to the CALHM1 genotypes is warranted. To date, two studies have analyzed the association of CSF Aβ concentrations with CALHM1 P86L. In a sample of subjects with AD and other cognitive disorders, no association was found between CALHM1 P86L and CSF Aβ concentrations (46). In contrast, in a mixed sample of subjects with and without AD, a statistically significant effect of the minor allele in CALHM1 P86L in the direction of increased CSF Aβ42 was detected (47). The current study was designed to reassess whether the CALHM1 P86L polymorphism modulates CSF Aβ concentrations in independent populations, and to test the hypothesis that this effect may be more apparent in presymptomatic individuals unaffected by the CSF Aβ42 drop observed during the disease process.
Materials and Methods
Study Population
Non-demented subjects (n = 46) were recruited to the Litwin-Zucker Research Center as part of a longitudinal study investigating CSF biomarkers in cognition and AD. The research was approved by the institutional review board, and all subjects provided informed consent. Nearly all of these subjects had a positive family history of AD (as defined by the presence of a first-degree relative with AD) and were enrolled for longitudinal follow up, but did not have cognitive complaints at the time of examination, and none met criteria for dementia. AD patients (n = 203) were recruited at the memory clinic of the Department of Psychiatry, University of Munich, Germany. Subjects diagnosed with AD-type dementia fulfilled the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) criteria (48).
CSF Sampling
After routine medical and physical assessments, lumbar puncture was performed in a sitting or lateral decubitus position. Following sterile preparation and local anesthesia with 4% lidocaine topical cream and 1% lidocaine subcutaneous injection, a 4-cm-long 20-gauge cutting-tip needle was used as an introducer in the L3–L4 or L4–L5 interspace. Next, a 25-gauge Whiteacre-point spinal needle was inserted through the introducer and placed in the thecal sac. After fluid return was established, the spinal catheter was connected to a 5- or 10-mL syringe via a polypropylene tube. Gentle negative pressure sufficient to remove CSF at a rate of approximately 2 mL/min was then applied by syringe and approximately 25–30 mL of clear spinal fluid was removed from each subject. CSF was then frozen and stored at −80°C. At the Munich center, samples of CSF were acquired via lumbar puncture between 9 am and 11 am according to a routine protocol.
Genotyping
APOE genotyping. Genetic variation at the APOE locus was determined by restriction isotyping using PCR amplification and subsequent digestion with HhaI (49). The PCR reaction was performed with 0.5 μmol/L primer F4 and F6 (49) and 1.5 mmol/L MgCl2 under the following cycle condition: 3 min denaturation at 95°C and 35 cycles with 1 min at 95°C, 1 min at 60°C, 1 min at 70°C and a final extension at 70°C for 10 min. PCR products were digested with HhaI overnight and the fragments separated on a 3% Metaphor agarose gel.
CALHM1 genotyping. The rs2986017 variant in CALHM1 was determined by sequencing CALHM1 exon 1. Exon 1 was amplified by PCR using FX1US and FX1DSa primers (33) in the presence of 1.5 mmol/L MgCl2 under the following amplification conditions: Initial denaturation for 3 min at 94°C and 35 cycles of 30 s at 94°C, annealing for 30 s at 54°C and extension for 1 min at 72°C for 35 cycles. PCR products were sequenced by GeneWiz (South Plainfield, NJ, USA).
Aβ ELISA
CSF Aβ1–40 and Aβ1–42 concentrations were determined by enzyme-linked immunosorbent assays (ELISAs) using kits from Covance (β-Amyloid 1–40 and β-Amyloid 1–42 ELISA; Princeton, NJ, USA) for the Manhasset samples or from Innogenetics (INNOTEST β-amyloid 1–42; Gent, Belgium) for the German samples, according to the manufacturers’ instructions. Please note that the use of different ELISA kits could potentially lead to inconsistencies between the results of the two kits in terms of the absolute values of measured Aβ levels and thus does not allow the comparison of the results obtained in the two centers. Our methodology, however, was designed to measure relative CSF Aβ level changes within diagnostic groups.
BACE1 Western Blot (WB) Analyses
BACE1 levels were analyzed by WB using ab2077 antibody (Abcam, San Francisco, CA, USA). Twenty microliters of a 1:100 dilution of CSF were analyzed by SDS-PAGE and WB. A standard ECL detection procedure was then used.
Statistical analysis
Normal cohort. We performed multiple linear regression to predict the level of each endophenotype (Aβ40 or Aβ42) with factors including APOE genotype (coded as a nominal variable with value ε4/4, ε3/4, ε3/3, ε2/4, or ε2/3); age of the patient at CSF collection time; gender; or BACE1 levels, and CALHM1 genotype coded to reflect the hypothesized transmission mechanism (that is, recessive model compares CC or CT versus TT; additive model codes the number of T allele(s): 0 for CC, 1 for CT, and 2 for TT; dominant model compares CC versus CT or TT). Reported P values were estimated with JMP version 8.01.
AD cohort. We performed multiple linear regression to predict the level of Aβ42 (adjusted for age of the patient at CSF collection time) and CALHM1 genotype coded to reflect the hypothesized transmission mechanism, as described above.
Results
The CALHM1 P86L Polymorphism (rs2986017) Shows Association with CSF Aβ Levels in Young Cognitively Healthy Individuals at Risk for AD, but Not in AD Patients
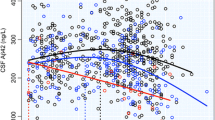
CSF samples from 46 cognitively healthy individuals with a positive family history of AD and 203 individuals with AD were collected. Patient characteristics and genotype distributions in each group are shown in Table 1. CSF concentrations (pg/mL) of Aβ1–40 (normal cohort) and Aβ1–42 (normal and AD cohorts) were measured and rs2986017 genotypes were determined in these patients (Table 1, Table 2).
Table 3 shows the results of test of associations between rs2986017 genotype and Aβ1–40 or Aβ1–42 in the normal cohort under the recessive, additive and dominant genetic transmission models (tests are performed with multiple regression and controls for several genetic and biological covariates, see Methods). These tests indicated that in the cognitively healthy cohort, CALHM1 genotype has a significant effect on Aβ1–42 levels under the additive (P = 0.0036) and dominant (P = 0.0099) models, and shows a trend effect under the recessive model (P = 0.0669, Table 3). A significant effect of CALHM1 genotype also was found for Aβ1–40 levels under the recessive (P = 0.0123) and additive models (P = 0.0237, Table 3).
Because CSF BACE1 levels and activity were found in several studies to be elevated in MCI (mild cognitive impairment) and AD patients (50,51), we also measured CSF BACE1 levels in the normal cohort to determine whether BACE1 levels could influence the effect of CALHM1 P86L on Aβ levels. Western blot and densitometry analyses were conducted to measure BACE1 levels (Figure 1). BACE1 levels were not associated with CALHM1 genotype (see Figure 1) and models fitted to Aβ levels that controlled for CSF BACE1 levels (Table 3) showed significant association between CALHM1 genotype and Aβ levels, indicating that the effect of CALHM1 genotype on Aβ levels could not be explained by changes in CSF BACE1 levels.
In contrast to the normal cohort, we found that levels of Aβ1–42 were not affected by rs2986017 genotype in the AD cohort. The additive model for a CALHM1 effect yielded a P value of 0.34.

CSF BACE1 levels by CALHM1 P86L genotype (rs2986017). CSF BACE1 levels in the normal cohort were analyzed by WB (A). Graph in (B) shows BACE1 level quantification by CALHM1 genotype (rs2986017) in the normal cohort.
Discussion
The use of quantitative endophenotypes such as CSF Aβ levels to evaluate candidate genes in late-onset AD has emerged recently as a promising approach (17,26,47,52–54). For instance, the APOE ε4 allele has been found to predict in some (55,56), but not all studies (57,58), changes in CSF Aβ concentrations in non-demented individuals, potentially as an early marker of evolving disease. Another example is the gene coding for angiotensin-converting enzyme (ACE), a protease involved in Aβ degradation (59), for which a haplotype associated with an increased risk of AD has been reported in association with elevated levels of CSF Aβ (60).
In this study, an association was observed between the CALHM1 P86L polymorphism and elevated levels of CSF Aβ42 and Aβ40 in a small sample of young, cognitively healthy individuals with a positive family history for AD. This association was not observed in individuals suffering from dementia, albeit in a large sample. Elevated levels of CSF Aβ were predicted in association with CALHM1 P86L based on its in vitro effects on Aβ metabolism. Indeed, CALHM1 was found to repress Aβ accumulation in a calcium-dependent manner in cell lines, and expression of mutated P86L-CALHM1 resulted in a partial loss of CALHM1 control on cytosolic calcium levels and Aβ repression, resulting in an elevation of extracellular Aβ levels (33). While the CALHM1 P86L polymorphism has not been established conclusively as an AD risk allele, its impact on the age at onset of AD has now been demonstrated in four independent studies (33,36,40,45) and may be related directly to its effect on Aβ metabolism (33). The association of CALHM1 P86L with CSF Aβ observed here in cognitively healthy individuals at risk for AD, but not in AD patients, may be related to the reduction in circulating Aβ42 that accompanies the presumed parenchymal deposition in AD (20–24). Thus, the effect of the CALHM1 P86L polymorphism on CSF Aβ may be the most apparent before the first clinical manifestations of the disease.
The design of the current study had several limitations. First, the sample size of the cognitively healthy cohort was small, limiting the power of the study. However, significant differences for both Aβ42 and Aβ40 levels were found within this group, suggesting that the effect of CALHM1 on CSF Aβ levels in young cognitively healthy individuals is large enough to be seen in a sample group of this size. Second, the study includes two independent cohorts. Longitudinal studies in normal cohorts will be required to determine whether CALHM1 P86L, co-occurring with early elevations in CSF Aβ levels, influences the disease onset.
In summary, we show that the CALHM1 P86L polymorphism is associated with elevated CSF Aβ in normal individuals at risk for AD, supporting previous reports suggesting that CALHM1 controls Aβ metabolism in vitro in cell lines (33) and in vivo in human CSF (47). These data further strengthen the notion that CALHM1 is involved in AD pathogenesis by modulating the age of disease onset (33,36,40,45), and this, via a mechanism implicating early deregulation in Aβ metabolism. Finally, this work provides support for the use of CSF Aβ measurements as a quantitative endophenotype for identifying or validating AD risk genes in populations of individuals with preclinical AD.
Disclosure
The authors declare that they have no competing interests as defined by Molecular Medicine, or other interests that might be perceived to influence the results and discussion reported in this paper.
References
Blennow K, de Leon MJ, Zetterberg H. (2006) Alzheimer’s disease. Lancet. 368:387–403.
Selkoe DJ. (2001) Alzheimer’s disease: genes, proteins, and therapy. Physiol. Rev. 81:741–66.
Marambaud P, Robakis NK. (2005) Genetic and molecular aspects of Alzheimer’s disease shed light on new mechanisms of transcriptional regulation. Genes Brain Behav. 4:134–46.
Querfurth HW, LaFerla FM. (2010) Alzheimer’s disease. N. Engl. J. Med. 362:329–44.
Lambert JC, Amouyel P. (2007) Genetic heterogeneity of Alzheimer’s disease: complexity and advances. Psychoneuroendocrinology. 32 Suppl 1: S62–70.
Rademakers R, Rovelet-Lecrux A. (2009) Recent insights into the molecular genetics of dementia. Trends Neurosci. 32:451–61.
Lambert JC, et al. (2009) Genome-wide association study identifies variants at CLU and CR1 associated with Alzheimer’s disease. Nat. Genet. 41:1094–9.
Harold D, et al. (2009) Genome-wide association study identifies variants at CLU and PICALM associated with Alzheimer’s disease. Nat. Genet. 41:1088–93.
Bertram L, McQueen MB, Mullin K, Blacker D, Tanzi RE. (2007) Systematic meta-analyses of Alzheimer disease genetic association studies: the AlzGene database. Nat. Genet. 39:17–23.
Hollingworth P, et al. (2011) Common variants at ABCA7, MS4A6A/MS4A4E, EPHA1, CD33 and CD2AP are associated with Alzheimer’s disease. Nat. Genet. 43:429–35.
Gomez-Isla T, et al. (1996) Profound loss of layer II entorhinal cortex neurons occurs in very mild Alzheimer’s disease. J. Neurosci. 16:4491–500.
Hulette CM, et al. (1998) Neuropathological and neuropsychological changes in “normal” aging: evidence for preclinical Alzheimer disease in cognitively normal individuals. J. Neuropathol. Exp. Neurol. 57:1168–74.
Markesbery WR, et al. (2006) Neuropathologic substrate of mild cognitive impairment. Arch. Neurol. 63:38–46.
Morris JC, Price AL. (2001) Pathologic correlates of nondemented aging, mild cognitive impairment, and early-stage Alzheimer’s disease. J. Mol. Neurosci. 17:101–18.
Price JL, et al. (2001) Neuron number in the entorhinal cortex and CA1 in preclinical Alzheimer disease. Arch. Neurol. 58:1395–402.
Gottesman II, Gould TD. (2003) The endophenotype concept in psychiatry: etymology and strategic intentions. Am. J. Psychiatry. 160:636–45.
Kauwe JS, et al. (2009) Alzheimer’s disease risk variants show association with cerebrospinal fluid amyloid beta. Neurogenetics. 10:13–7.
De Meyer G, et al. (2010) Diagnosis-independent Alzheimer disease biomarker signature in cognitively normal elderly people. Arch. Neurol. 67:949–56.
Dubois B, et al. (2010) Revising the definition of Alzheimer’s disease: a new lexicon. Lancet Neurol. 9:1118–27.
Galasko D, et al. (1998) High cerebrospinal fluid tau and low amyloid beta42 levels in the clinical diagnosis of Alzheimer disease and relation to apolipoprotein E genotype. Arch. Neurol. 55:937–45.
Hampel H, et al. (2004) Value of CSF beta-amyloid1–42 and tau as predictors of Alzheimer’s disease in patients with mild cognitive impairment. Mol. Psychiatry. 9:705–10.
Mehta PD, et al. (2000) Plasma and cerebrospinal fluid levels of amyloid beta proteins 1–40 and 1–42 in Alzheimer disease. Arch. Neurol. 57:100–5.
Motter R, et al. (1995) Reduction of beta-amyloid peptide42 in the cerebrospinal fluid of patients with Alzheimer’s disease. Ann. Neurol. 38:643–8.
Sunderland T, et al. (2003) Decreased beta-amyloid1–42 and increased tau levels in cerebrospinal fluid of patients with Alzheimer disease. JAMA. 289:2094–103.
Mattsson N, et al. (2009) CSF biomarkers and incipient Alzheimer disease in patients with mild cognitive impairment. JAMA. 302:385–93.
Fagan AM, et al. (2006) Inverse relation between in vivo amyloid imaging load and cerebrospinal fluid Abeta42 in humans. Ann. Neurol. 59:512–9.
Demuro A, Parker I, Stutzmann GE. (2010) Calcium signaling and amyloid toxicity in Alzheimer disease. J. Biol. Chem. 285:12463–8.
Marambaud P, Dreses-Werringloer U, Vingtdeux V. (2009) Calcium signaling in neurodegeneration. Mol. Neurodegener. 4:20.
Supnet C, Bezprozvanny I. (2010) The dysregulation of intracellular calcium in Alzheimer disease. Cell Calcium. 47:183–9.
Green KN, LaFerla FM. (2008) Linking calcium to Abeta and Alzheimer’s disease. Neuron. 59:190–4.
Mattson MP. (2010) ER calcium and Alzheimer’s disease: in a state of flux. Sci. Signal. 3:pe10.
Foskett JK. (2010) Inositol trisphosphate receptor Ca2+ release channels in neurological diseases. Pflugers Arch. 460:481–94.
Dreses-Werringloer U, et al. (2008) A polymorphism in CALHM1 influences Ca2+ homeostasis, Abeta levels, and Alzheimer’s disease risk. Cell. 133:1149–61.
Moreno-Ortega AJ, Ruiz-Nuno A, Garcia AG, Cano-Abad MF. (2010) Mitochondria sense with different kinetics the calcium entering into HeLa cells through calcium channels CALHM1 and mutated P86L-CALHM1. Biochem. Biophys. Res. Commun. 391:722–6.
Gallego-Sandin S, Alonso MT, Garcia-Sancho J. (2011) Calcium homeostasis modulator 1 (CALHM1) reduces the calcium content of the endoplasmic reticulum (ER) and triggers ER stress. Biochem. J. 437:469–75.
Boada M, et al. (2010) CALHM1 P86L polymorphism is associated with late-onset Alzheimer’s disease in a recessive model. J. Alzheimers Dis. 20:247–51.
Cui PJ, et al. (2010) CALHM1 P86L polymorphism is a risk factor for Alzheimer’s disease in the Chinese population. J. Alzheimers Dis. 19:31–5.
Campagne F, et al. (2008) Response: CALHM1 Association with Alzheimer’s Disease Risk. Cell. 135:994–6.
Bertram L, et al. (2008) No association between CALHM1 and Alzheimer’s disease risk. Cell. 135:993,4; author reply 994–6.
Minster RL, Demirci FY, DeKosky ST, Kamboh MI. (2009) No association between CALHM1 variation and risk of Alzheimer disease. Hum. Mutat. 30: E566–9.
Sleegers K, et al. (2009) No association between CALHM1 and risk for Alzheimer dementia in a Belgian population. Hum. Mutat. 30: E570–4.
Beecham GW, Schnetz-Boutaud N, Haines JL, Pericak-Vance MA. (2009) CALHM1 polymorphism is not associated with late-onset Alzheimer disease. Ann. Hum. Genet. 73:379–81.
Nacmias B, et al. (2010) Lack of implication for CALHM1 P86L common variation in Italian patients with early and late onset Alzheimer’s disease. J. Alzheimers Dis. 20:37–41.
Li H, et al. (2008) Candidate single-nucleotide polymorphisms from a genomewide association study of Alzheimer disease. Arch. Neurol. 65:45–53.
Lambert JC, et al. (2010) The CALHM1 P86L polymorphism is a genetic modifier of age at onset in Alzheimer’s disease: a meta-analysis study. J. Alzheimers Dis. 22:247–55.
Giedraitis V, et al. (2010) CALHM1 P86L polymorphism does not alter amyloid-beta or tau in cerebrospinal fluid. Neurosci. Lett. 469:265–7.
Kauwe JS, et al. (2010) Validating predicted biological effects of Alzheimer’s disease associated SNPs using CSF biomarker levels. J. Alzheimers Dis. 21:833–42.
McKhann G, et al. (1984) Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 34:939–44.
Hixson JE, Vernier DT. (1990) Restriction isotyping of human apolipoprotein E by gene amplification and cleavage with HhaI. J. Lipid Res. 31:545–8.
Ewers M, et al. (2011) Increased CSF-BACE1 activity associated with decreased hippocampus volume in Alzheimer’s disease. J. Alzheimers Dis. 25:373–81.
Holsinger RM, McLean CA, Collins SJ, Masters CL, Evin G. (2004) Increased beta-Secretase activity in cerebrospinal fluid of Alzheimer’s disease subjects. Ann. Neurol. 55:898–9.
Fagan AM, et al. (2007) Cerebrospinal fluid tau/beta-amyloid(42) ratio as a prediction of cognitive decline in nondemented older adults. Arch. Neurol. 64:343–9.
Kauwe JS, et al. (2007) Extreme cerebrospinal fluid amyloid beta levels identify family with late-onset Alzheimer’s disease presenilin 1 mutation. Ann. Neurol. 61:446–53.
Han MR, Schellenberg GD, Wang LS, Alzheimer’s Disease Neuroimaging Initiative. (2010) Genome-wide association reveals genetic effects on human Abeta42 and tau protein levels in cerebrospinal fluids: a case control study. BMC Neurol. 10:90.
Prince JA, Zetterberg H, Andreasen N, Marcusson J, Blennow K. (2004) APOE epsilon4 allele is associated with reduced cerebrospinal fluid levels of Abeta42. Neurology. 62:2116–8.
Sunderland T, et al. (2004) Cerebrospinal fluid beta-amyloid1–42 and tau in control subjects at risk for Alzheimer’s disease: the effect of APOE epsilon4 allele. Biol. Psychiatry. 56:670–6.
Glodzik-Sobanska L, et al. (2009) The effects of normal aging and ApoE genotype on the levels of CSF biomarkers for Alzheimer’s disease. Neurobiol. Aging. 30:672–81.
Vuletic S, et al. (2008) Apolipoprotein E highly correlates with AbetaPP- and tau-related markers in human cerebrospinal fluid. J. Alzheimers Dis. 15:409–17.
Miners JS, et al. (2008) Abeta-degrading enzymes in Alzheimer’s disease. Brain Pathol. 18:240–52.
Kehoe PG, et al. (2003) Haplotypes extending across ACE are associated with Alzheimer’s disease. Hum. Mol. Genet. 12:859–67.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Koppel, J., Campagne, F., Vingtdeux, V. et al. CALHM1 P86L Polymorphism Modulates CSF Aβ Levels in Cognitively Healthy Individuals at Risk for Alzheimer’s Disease. Mol Med 17, 974–979 (2011). https://doi.org/10.2119/molmed.2011.00154
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.2119/molmed.2011.00154