
Abstract
OBJECTIVES: In 2009, due to increasing congenital syphilis rates, prenatal syphilis tests (PST) at both mid-gestation and delivery were added to first trimester prenatal screening in the province of Alberta. We sought to determine the proportion of mothers who had all three recommended PSTs during this period and to identify factors associated with incomplete PST.
METHODS: A cohort of all pregnancies resulting in a live or stillborn infant in Alberta for 2010 and 2011 was developed from Vital Statistics and linked with prenatal screening data to determine the number and timing of PSTs for pregnant women. The proportion of women who had PSTs at the three recommended time points in pregnancy and associated correlates were identified using basic statistics and logistic regressions.
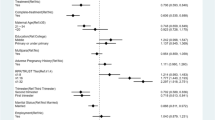
RESULTS: Of 99,609 pregnancies, 20.7% had all three PSTs at the recommended time points. Overall, 98.5% (98,162) had at least one PST, 1.5% only had PST at delivery and 1.5% had no PST performed. Independent risk factors for not having the three recommended PSTs included First Nations status (adjusted odds ratio [AOR]: 1.78 [95% CI: 1.62–1.96]), rural remote residence (AOR 3.61 [95% CI: 3.10–4.20]) and sole use of a midwife for prenatal care (AOR 13.70 [95% CI: 9.20–20.39]).
CONCLUSIONS: Nearly all pregnant women in Alberta received a PST at least once during their pregnancy, however far fewer received PSTs at the recommended time points. Interventions that target those who are less likely to be prenatally screened may help to ensure that pregnant women get early and appropriate care for syphilis during pregnancy.
Résumé
OBJECTIFS : En 2009, la hausse des taux de syphilis congénitale a poussé la province de l’Alberta à ajouter aux dépistages systématiques du premier trimestre des tests prénatals pour la syphilis (TPS) au milieu de la grossesse et à l’accouchement. Nous avons cherché à déterminer la proportion des mères ayant subi les trois TPS recommandés durant la grossesse et l’accouchement et à cerner les facteurs associés aux TPS incomplets.
MÉTHODE : À l’aide des statistiques de l’état civil, nous avons créé une cohorte de toutes les grossesses ayant donné lieu à un enfant vivant ou mort-né en Alberta en 2010 et en 2011 et nous l’avons liée aux données de dépistage prénatal afin de déterminer le nombre et le moment des TPS administrés aux femmes enceintes. La proportion des femmes ayant subi des TPS aux trois points recommandés durant leur grossesse, et les corrélats associés, ont été déterminés à l’aide de statistiques élémentaires et de régressions logistiques.
RÉSULTATS : Sur 99 609 grossesses, 20,7 % de femmes avaient subi les trois TPS aux points recommandés dans le temps. Dans l’ensemble, 98,5 % des femmes enceintes (98 162) avaient subi au moins un TPS, 1,5 % n’avaient subi qu’un TPS à l’accouchement et 1,5 % n’en avaient subi aucun. Les facteurs de risque indépendants pour n’avoir pas subi les trois TPS recommandés étaient le statut de membre d’une Première Nation (rapport de cotes ajusté [RCa]: 1,78 [IC de 95 %: 1,62–1,96]), le fait de résider en région rurale éloignée (RCa 3,61 [IC de 95 %: 3,10–4,20]) et le recours exclusif à une sage-femme pour les soins prénatals (RCa 13,70 [IC de 95 %: 9,20–20,39]).
CONCLUSIONS : Presque toutes les femmes enceintes en Alberta ont subi un TPS au moins une fois durant leur grossesse, mais elles sont beaucoup moins nombreuses à avoir subi les TPS aux points recommandés dans le temps. Des interventions ciblant les femmes moins susceptibles de subir un dépistage prénatal pourraient contribuer à faire en sorte que les femmes enceintes reçoivent des soins précoces et appropriés pour la syphilis durant la grossesse.
Similar content being viewed by others


References
Fiumara NJ, Fleming WL, Downing JG, Good, FL. The incidence of prenatal syphilis at the Boston City Hospital. N Engl J Med 1952;247:48–52. PMID: 14941281. doi: 10.1056/NEJM195207102470203.
Finelli L, Berman SM, Koumans EH, Levine, WC. Congenital syphilis. Bull World Health Organ 1998;76(Suppl 2):126–28. PMID: 10063689.
World Health Organization, Department of Reproductive Health and Research. The Global Elimination of Congenital Syphilis: Rationale and Strategy for Action, 2007. Available at: http://www.who.int (Accessed May 5, 2016).
Mobley JA, McKeown RE, Jackson KL, Sy F, Parham JS, Brenner, ER. Risk factors for congenital syphilis in infants of women with syphilis in South Carolina. Am J Public Health 1998;88(4):597–602. PMID: 9551001. doi: 10.2105/AJPH.88.4.597.
Desenclos JC, Scaggs M, Wroten, JE. Characteristics of mothers of live infants with congenital syphilis in Florida, 1987–1989. Am J Epidemiol 1992;136(6):657–61. PMID: 1442732.
Caddy S, Lee B, Sutherland K, Robinson J, Plitt S, Read R, Singh, AE. Pregnancy and neonatal outcomes of women with reactive syphilis serology in Alberta, 2002–2006. J Obstet Gynaecol Can 2011;33:453–59. PMID: 21639965.
Singh AE, Sutherland K, Lee BE, Robinson JL, Wong T. Resurgence of early congenital syphilis in Alberta. CMAJ 2007;177(1):33–36. PMID: 17606936.
Warner L, Rochat RW, Fichtner RR, Stoll BJ, Nathan L, Toomey, KE. Missed opportunities for congenital syphilis prevention in an urban southeastern hospital. Sex Transm Dis 2001;28(2):92–98. PMID: 11234792.
Alberta Health. Interactive Health Data Application. Available at: http://www.ahw.gov.ab.ca (Accessed April 14, 2015).
Alberta Prenatal Screening Program for Selected Communicable Diseases. June 2006. Available at: http://www.health.alberta.ca (Accessed February 16, 2015).
Lee MC, Robinson JL, Lee BE, Singh A. An infant with seizures, rash, and hepatosplenomegaly. Clin Infect Dis 2008;46:451–52, 472–73. PMID: 18181743. doi: 10.1086/525533.
Alberta Perinatal Health Program. Alberta Perinatal Connection, 2009. Available at: http://www.aphp.ca (Accessed September 15, 2015).
Public Health Agency of Canada. Canadian Guidelines on Sexually Transmitted Infections, 2013 ed. Ottawa, ON: Her Majesty the Queen in Right of Canada, 2013. Available at: http://www.phac-aspc.gc.ca (Accessed December 10, 2014).
Schrag SJ, Arnold KE, Mohle-Boetani JC, Lynfield R, Zell ER, Stefonek K, et al. Prenatal screening for infectious diseases and opportunities for prevention. Obstet Gynecol 2003;102(4):753–60.
Alberta Health Services. ProvLab Laboratory Bulletin. Discontinuation of Second Trimester Syphilis Screening on Pregnant Women, 2012. Available at: http://www.provlab.ab.ca (Accessed April 17, 2016).
Wang F, Larke B, Gabos S, Hanrahan A, Schopflocher D. Potential factors that may affect the acceptance of routine prenatal HIV testing. Can J Public Health 2005;96(1):60–64. PMID: 15682699.
Guenter D, Kaczorowski J, Carroll J, Sellors J. Prenatal HIV tests: Routine testing or informed choice? Can Fam Physician 2003;49:1334–40. PMID: 14594102.
Bell CA, Simmonds KA, MacDonald, SE. Exploring the heterogeneity among partially vaccinated children in a population-based cohort. Vaccine 2015;33(36):4572–78. PMID: 26187259. doi: 10.1016/j.vaccine.2015.07.004.
Sahni V, Lai FY, MacDonald, SE. Neonatal vitamin K refusal and nonimmunization. Pediatrics 2014;134(3):497–503. PMID: 25136042. doi: 10.1542/peds.2014-1092.
Midwife Philosophy. Alberta Association of Midwives. Available at: http://www.alberta-midwives.com(Accessed April 30, 2015).
Dube E, Vivion M, Valderrama A, Sauvageau C. Knowledge and attitudes toward vaccination among midwives in Quebec. Sante Publique 2013;25(1):35–43. PMID: 23705333.
Author information
Authors and Affiliations
Corresponding author
Additional information
Conflict of Interest: None to declare.
Rights and permissions
About this article

Cite this article
Plitt, S.S., Osman, M., Sahni, V. et al. Examination of a prenatal syphilis screening program, Alberta, Canada: 2010–2011. Can J Public Health 107, e285–e290 (2016). https://doi.org/10.17269/CJPH.107.5320
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.17269/CJPH.107.5320