
Abstract
BACKGROUND
The current trend in the management of low risk differentiated thyroid carcinoma is to follow less aggressive strategies.
OBJECTIVE
To assess the long-term morbidity and mortality outcomes of low-risk papillary thyroid carcinoma (PTC) patients undergoing minimal intervention.
DESIGN
We retrospectively analyzed 137 patients with low-risk PTC (stage I: n=77; stage II: n=60). Of these patients, 107 (Group 1) had macro-PTC and underwent near-total thyroidectomy and received postoperatively 50mCi RAI. The remaining 30 patients (Group 2) had micro-PTC (<1cm) and were treated only by means of near-total thyroidectomy.
RESULTS
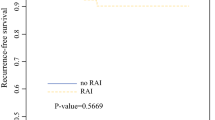
The median follow-up for Group 1 patients was 10 years (range: 3–30). At 1-year evaluation, 8 patients of Group 1 had indeterminate or incomplete biochemical response, of whom 4 had also incomplete structural response to initial therapy. Only 1 of 4 patients with structural incomplete response underwent cervical lymph node dissection and then received an additional dose of 100mCi RAI. The remaining 7 patients received only an additional dose of 100mCi RAI. These patients have been continuously followed till the present time with no recurrences or deaths (median follow-up: 17.5 years; 3–30 years). At 15 years, 2 patients of Group 1 experienced biochemical recurrence and they received 100mCi RAI. Three patients of Group 2 experienced recurrence, with 2 receiving 50mCi RAI and 1 undergoing cervical lymph node dissection with 50mCi RAI.
CONCLUSIONS
Patients with low-risk macro-PTC treated by means of near-total thyroidectomy without PCCLND and receiving postoperatively a low dose of 50mCi RAI have excellent long-term prognosis.
Article PDF
Similar content being viewed by others


References
Jonklaas J, Sarlis NJ, Litofsky D, et al, 2006 Outcomes of patients with differentiated thyroid carcinoma following initial therapy. Thyroid 16: 1229–1242.
Kim SJ, Myong JP, Suh H, Lee KE, Youn YK, 2015 Optimal cutoff age for predicting mortality associated with differentiated thyroid cancer. PloS one 10: e0130848.
Qubain SW, Nakano S, Baba M, Takao S, Aikou T, 2002 Distribution of lymph node micrometastasis in pn0 well-differentiated thyroid carcinoma. Surgery 131: 249–256.
Arturi F, Russo D, Giuffrida D, et al, 1997 Early diagnosis by genetic analysis of differentiated thyroid cancer metastases in small lymph nodes. J Clin Endocrinol Metab 82: 1638–1641.
Randolph GW, Duh QY, Heller KS, et al, American Thyroid Association Surgical Affairs Committee’s Taskforce on Thyroid Cancer Nodal Surgery, 2012 The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid 22: 1144–1152.
American Thyroid Association Surgery Working Group, American Association of Endocrine Surgeos, American Academy of Otolaryngology Head and Neck Surgery, American Head and Neck Society, Carty SE, Cooper DS, Doherty GM, et al, 2009 Consensus statement on the terminology and classification of central neck dissection for thyroid cancer. Thyroid 19: 1153–1158.
Haugen BRM, Alexander EK, Bible KC, et al, 2015 american thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid 26: 1–133.
Alpert EH, Wenig BM, Dewey EH, Su HK, Dos Reis L, Urken ML, 2015 Size distribution of metastatic lymph nodes with extranodal extension in patients with papillary thyroid cancer: A pilot study. Thyroid 25: 238–241.
Leboulleux S, Rubino C, Baudin E, et al, 2005 Prognostic factors for persistent or recurrent disease of papillary thyroid carcinoma with neck lymph node metastases and/or tumor extension beyond the thyroid capsule at initial diagnosis. J Clin Endocrinol Metab 90: 5723–5729.
Robenshtok E, Fish S, Bach A, Dominguez JM, Shaha A, Turtle RM, 2012 Suspicious cervical lymph nodes detected after thyroidectomy for papillary thyroid cancer usually remain stable over years in properly selected patients. J Clin Endocrinol Metab 97: 2706–2713.
Adam MA, Pura J, Goffredo P, et al, 2015 Presence and number of lymph node metastases are associated with compromised survival for patients younger than age 45 years with papillary thyroid cancer. J Clin Oncol 33: 2370–2375.
Lang BH, Ng SH, Lau LL, Cowling BJ, Wong KP, Wan KY, 2013 A systematic review and meta-analysis of prophylactic central neck dissection on short-term locoregional recurrence in papillary thyroid carcinoma after total thyroidectomy. Thyroid 23: 1087–1098.
Ywata de Carvalho A, Chulam TC, Kowalski LP, 2015 Long-term results of observation vs prophylactic selective level vi neck dissection for papillary thyroid carcinoma at a cancer center. JAMA Otolaryngol Head Neck Surg 141: 599–606.
Schlumberger M, Catargi B, Borget I, et al, Tumeurs de la Thyroide Refractaires Network for the Essai Stimulation Ablation Equivalence Trial, 2012 Strategies of radioiodine ablation in patients with low-risk thyroid cancer. N Engl J Med 366: 1663–1673.
Mallick U, Harmer C, Yap B, et al, 2012 Ablation with low-dose radioiodine and thyrotropin alfa in thyroid cancer. N Engl J Med 366: 1674–1685.
Sacks W, Fung CH, Chang JT, Waxman A, Braunstein GD, 2010 The effectiveness of radioactive iodine for treatment of low-risk thyroid cancer: A systematic analysis of the peer-reviewed literature from 1966 to april 2008. Thyroid 20: 1235–1245.
Sawka AM, Thephamongkhol K, Brouwers M, Thabane L, Browman G, Gerstein HC, 2004 Clinical review 170: A systematic review and metaanalysis of the effectiveness of radioactive iodine remnant ablation for well-differentiated thyroid cancer. J Clin Endocrinol Metab 89: 3668–3676.
Vaccarella S, Dal Maso L, Laversanne M, Bray F, Plummer M, Franceschi S, 2015 The impact of diagnostic changes on the rise in thyroid cancer incidence: A population-based study in selected high-resource countries. Thyroid 25: 1127–1136.
Adam MA, Pura J, Goffredo P, et al, 2015 Impact of extent of surgery on survival for papillary thyroid cancer patients younger than 45 years. J Clin Endocrinol Metab 100: 115–121.
Zaydfudim V, Feurer ID, Griffin MR, Phay JE, 2008 The impact of lymph node involvement on survival in patients with papillary and follicular thyroid carcinoma. Surgery 144: 1070–1077.
Podnos YD, Smith D, Wagman LD, Ellenhorn JD, 2005 The implication of lymph node metastasis on survival in patients with well-differentiated thyroid cancer. Am Surg 71: 731–734.
Viola D, Materazzi G, Valerio L, et al, 2015 Prophylactic central compartment lymph node dissection in papillary thyroid carcinoma: Clinical implications derived from the first prospective randomized controlled single institution study. J Clin Endocrinol Metab 100: 1316–1324.
Lee DY, Oh KH, Cho JG, et al, 2015 The benefits and risks of prophylactic central neck dissection for papillary thyroid carcinoma: Prospective cohort study. Int J Endocrinol 2015: 571480.
Sywak M, Cornford L, Roach P, Stalberg P, Sidhu S, Delbridge L, 2006 Routine ipsilateral level vi lymph-adenectomy reduces postoperative thyroglobulin levels in papillary thyroid cancer. Surgery 140: 1000–1007.
Klein Hesselink EN, Links TP, 2015 Radioiodine treatment and thyroid hormone suppression therapy for differentiated thyroid carcinoma: Adverse effects support the trend toward less aggressive treatment for low-risk patients. Eur Thyroid J 4: 82–92.
Schvartz C, Bonnetain F, Dabakuyo S, et al, 2012 Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients. J Clin Endocrinol Metab 97: 1526–1535.
Vaisman F, Shaha A, Fish S, Michael Turtle R, 2011 Initial therapy with either thyroid lobectomy or total thyroidectomy without radioactive iodine remnant ablation is associated with very low rates of structural disease recurrence in properly selected patients with differentiated thyroid cancer. Clin Endocrinol 75: 112–119.
Seo GH, Cho YY, Chung JH, Kim SW, 2015 Increased risk of leukemia after radioactive iodine therapy in patients with thyroid cancer: A nationwide, population-based study in korea. Thyroid 25: 927–934.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Michalaki, M., Bountouris, P., Roupas, N.D. et al. Low-risk papillary thyroid carcinoma patients who underwent near-total thyroidectomy without prophylactic central compartment lymph node dissection and were ablated with low-dose 50mCi RAI had excellent 10-year prognosis. Hormones 15, 511–517 (2016). https://doi.org/10.14310/horm.2002.1694
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.14310/horm.2002.1694