
Abstract
Hypophysitis is an inflammatory disease of the pituitary gland that clinically and radiologically mimics pituitary tumors. We report here a case of xanthogranulomatous hypophysitis mimicking a pituitary neoplasm.
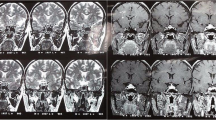
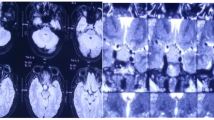
A 65-yr-old woman presented with weight loss, fatigue, and visual disturbance. Computed tomography demonstrated a round cystic low-density mass with calcification in the sella. A T1-weighted magnetic resonance imaging scan showed most of the mass as hyperintense. The capsule of the mass was strongly enhanced by gadolinium. Endocrinologic examination revealed hypocorticism and hypothyroidism. Diabetes insipidus (DI) developed after the administration of hydrocortisone. The patient also had hallucination and delusions of persecution.
Transsphenoidal surgery was performed. Histologic examination of the removed tissue showed central necrosis surrounded by accumulation of foamy cells and epithelioid cells. Several multinucleated giant cells were also seen. The foamy cells and epithelioid cells were immunopositive for Kp-1, a marker of macrophages. The patient made an uneventful postoperative recovery. Although DI and hypofunction of adenohypophysis persisted, the visual disturbance and psychiatric disorder were resolved.
We have described an unusual inflammatory lesion of the pituitary in the sellar region that was mimicking neoplasm. A high level of clinical suspicion of inflammatory disorders is necessary for correct diagnosis and optimal management.
Similar content being viewed by others

References
Deodhare SS, Bilbao JM, Kovacs K, et al. Xanthomatous hypophysitis: a novel entity obscure etiology. Endocr Pathol 10:237–241, 1999.
Folkerth RD, Price DL, Jr, Schwartz M, Black PM, De Girolami U. Xanthomatous hypophysitis. Am J Surg Pathol 22:736–741, 1998.
Scanarini M, d’Avella D, Rotilio A, Kitromilis N, Mingrino S. Giant-cell granulomatous hypophysitis: a distinct clinicopathological entity. J Neurosurg 71:681–686, 1989.
Cheung CC, Ezzat S, Smyth HS, Asa SL. The spectrum and significance of primary hypophysitis. J Clin Endocrinol Metab 86:1048–1053, 2001.
Hashimoto K, Takao T, Makino S. Lymphocytic adenohypophysitis and lymphocytic infundibuloneurohypophysitis. Endocr J 44:1–10, 1997.
Honegger J, Fahlbusch R, Bornemann A, et al. Lymphocytic and granulomatous hypophysitis: experience with nine cases. Neurosurgery 40:713–722, 1997.
Tashiro T, Sano T, Xu B, et al. Spectrum of different types of hypophysitis: a clinicopathologic study of hypophysitis in 31 cases. Endocr Pathol 13:183–195, 2002.
Saeger W. Tumor-like lesions of the sellar region. In: Thapar K, Kovacs K, Scheithauer BW, Lloyd RV, eds. Diagnosis and management of pituitary tumors. Totowa, NJ: Humana Press, 2001; 449–460.
Goudie RB, Pinkerton PH. Anterior hypophysitis and Hashimoto’s disease in a young woman. J Pathol Bacteriol 83:584–585, 1962.
Imura H, Nakao K, Shimatsu A, et al. Lymphocytic infundibuloneurohypophysitis as a cause of central diabetes insipidus. N Engl J Med 329:683–689, 1993.
Hama S, Arita K, Tominaga A, et al. Symptomatic Rathke’s cleft cyst coexisting with central diabetes insipidus and hypophysitis: case report. Endocr J 46:187–192, 1999.
Emery D, Kucharczyk W. Imaging of pituitary tumors. In: Thapar K, Kovacs K, Scheithauer BW, Lloyd RV, eds. Diagnosis and management of pituitary tumors. Totowa, NJ: Humana Press, 2001; 201–217.
Asa SL. Tumor-like lesions of the sella turcica. In: Tumors of the pituitary gland. Washington, DC: Armed Forces Institute of Pathology, 1998; 191–210.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yokoyama, S., Sano, T., Tajitsu, K. et al. Xanthogranulomatous hypophysitis mimicking a pituitary neoplasm. Endocr Pathol 15, 351–357 (2004). https://doi.org/10.1385/EP:15:4:351
Issue Date:
DOI: https://doi.org/10.1385/EP:15:4:351