
Abstract
Background
Intracorporeal anastomosis after totally laparoscopic total gastrectomy (TLTG) has been increasingly applied.1–7 We assessed the intracorporeal isoperistaltic jejunum-later-cut overlap method (IJOM) for esophagojejunostomy anastomosis (EA).
Methods
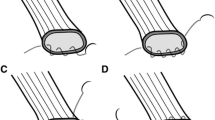
From January to June 2014, a total of 19 patients with resectable gastric cancer (cT1–T4aNOM0) underwent TLTG. IJOM was performed by creating side-to-side stapled anastomosis through enterotomies proximal to the left esophageal resection margin and on the antimesenteric jejunal border, 30 cm distal to the Trietz ligament. Conjoined enterotomies were sutured closed. The IJOM reduces jejunal motion and controls the EA direction. The biliary jejunal limb was transected ≤5 cm proximal to anastomosis, and a gastrografin esophagram was performed 5–7 days after the operation to diagnose anastomotic leakage. Follow-ups were performed every 3 months from the date of surgery to last follow-up by esophagram or computed tomography.
Results
For the 19 patients, the esophagojejunostomy time was 26 min, and blood loss was 50 ml (interquartile ranges [IQRs] 22–31 and 50–60, respectively). There were no conversions to open surgery. Liquid intake and soft diet were initiated on days 4 and 7, respectively, for 37 and 53% of patients (n = 7 and 10; IQRs 4–5 and 7–8, respectively). One patient with abdominal infection had delayed oral intake (day 11). Hospitalization duration was 12 days (IQR 11–16), and no patients experienced anastomosis-related complications (i.e. anastomotic leakage, stricture, hemorrhage, dysphagia, or dilation) or recurrence at anastomosis during follow-up (19 months; IQR 18–20).
Conclusions
IJOM for EA after TLTG is feasible. These early results do not reveal a high complication rate but additional outcome monitoring is needed.
Similar content being viewed by others


References
Okabe H, Obama K, Tsunoda S, Tanaka E, Sakai Y. Advantage of completely laparoscopic gastrectomy with linear stapled reconstruction a long-term follow-up study. Ann Surg. 2014;259(1): 109–16.
Kim HS, Kim MG, Kim BS, et al. Comparison of totally laparoscopic total gastrectomy and laparoscopic-assisted total gastrectomy methods for the surgical treatment of early gastric cancer near the gastroesophageal junction. J Laparoendosc Adv Surg Tech A. 2013;23(3):204–10.
Kim HS, Kim BS, Lee IS, Lee S, Yook JH, Kim BS. Comparison of totally laparoscopic total gastrectomy and open total gastrectomy for gastric cancer. J Laparoendosc Adv Surg Tech A. 2013;23(4):323–31.
Tsunoda S, Okabe H, Obama K, et al. Short-term outcomes of totally laparoscopic total gastrectomy: experience with the first consecutive 112 cases. World J Surg. 2014;38(10):2662–7.
Kim HS, Kim MG, Kim BS, Yook JH, Kim BS. Totally laparoscopic total gastrectomy using endoscopic linear stapler: early experiences at one institute. J Laparoendosc Adv Surg Tech A. 2012;22(9):889–97.
Bracale U, Marzano E, Nastro P, et al. Side-to-side esophagojejunostomy during totally laparoscopic total gastrectomy for malignant disease: a multicenter study. Surg Endosc. 2010t;24(10): 2475–9.
Matsui H, Okamoto Y, Nabeshima K, et al. Endoscopy-assisted anastomosis: a modified technique for laparoscopic side-to-side esophagojejunostomy following a total gastrectomy. Asian J Endosc Surg. 2011;4(3):107–11.
Funding
This work was supported by the National Key Clinical Specialty Discipline Construction Program of China (No. [2012]649) and the Key Project of Science and Technology Plan of Fujian Province, China (No. 2-14Y0025).
Author Contributions
Ze-Ning Huang and Chang-Ming Huang conceived the study, analyzed the data, drafted the manuscript, and recorded the video; Chao-Hui Zheng, Ping Li, Jian-Wei Xie, and Jia-Bin Wang critically revised the manuscript for important intellectual content; and Jian-Xian Lin, Jun Lu, Qi-Yue Chen, Long–Long Cao, Mi Lin, and Ru-Hong Tu collected the data and designed the study. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Video 1 (MP4 223072 kb)
Rights and permissions
About this article

Cite this article
Huang, CM., Huang, ZN., Zheng, CH. et al. An Isoperistaltic Jejunum-Later-Cut Overlap Method for Esophagojejunostomy Anastomosis After Totally Laparoscopic Total Gastrectomy: A Safe and Feasible Technique. Ann Surg Oncol 24, 1019–1020 (2017). https://doi.org/10.1245/s10434-016-5658-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5658-5