
Abstract
Background
The overall survival with non-cardia gastric adenocarcinoma in the United States has remained poor and relatively unchanged over the past 2 decades. This brings into question the utilization and quality of gastrectomy and lymphadenectomy. We examined the trends, extent, and determinants of surgical treatment and the influence of gastrectomy and adequacy of lymphadenectomy (defined as collection of 15 or more lymph nodes) on non-cardia gastric cancer survival.
Methods
Data from Surveillance, Epidemiology, and End Results (SEER) registries was used to identify patients with non-cardia adenocarcinoma diagnosed during 1983–2002. Logistic regression was used to examine determinants of gastric resection and adequacy of lymphadenectomy. Cox proportional hazard (PH) models were used to examine determinants of mortality risk for patients treated surgically. All models examined year of diagnosis, age, race, gender, geographic region, and cancer spread.
Results
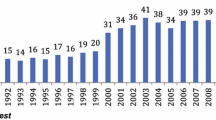
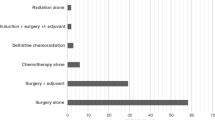
There were 16,846 patients with non-cardia gastric cancer of whom 10,534 (62.5%) underwent gastric resection. Approximately 77.9% with localized disease underwent resection. Resection for non-cardia gastric cancer declined 6% for all stages and 20% for local stages between 1983 and 2002. In multivariable models, gastrectomies were less likely to be performed between 1998–2002 (−37% compared to 1983–1987), for localized disease (−78% compared to regional disease), for patients older than 70 (−39% compared to patients younger than 40), and for patients from New Mexico (−45% compared to highest in Hawaii). Wide racial variability was also found (lowest for Whites [−54%] compared to Asians). Adequate LN sampling (15 or more LN) was recorded in only 25% overall and 20% of localized disease. Improvement in LN collection since 1997 has been modest, with only a 7% relative increase. The mortality risk of surgically treated non-cardia cancer patients has been unchanged for 15 years. Adequate lymphadenectomy was associated with a 19% decreased mortality risk in this group. Gender and racial differences in mortality risk were present (up to 13% higher in men compared to women and 22% higher in Whites compared Asians).
Conclusion
Gastrectomy for non-cardia gastric adenocarcinoma is underutilized, especially for localized disease. In the majority of operations for non-cardia gastric cancer, LN collection is inadequate. Racial and geographic variations with gastric resection and LN sampling are as significant as patient age and stage of the cancer. Disparities based on race and geographic region, as well as surgeon and facility factors need to be investigated and addressed to bring forth improvements in outcomes for non-cardia adenocarcinoma.


Similar content being viewed by others

References
Parkin DM, Bray FI, Devesa SS. Cancer burden in the year 2000. The global picture. Eur J Cancer 2001; 37:4–66
American Cancer Society. Cancer Facts and Figures 2005. Atlanta: American Cancer Society
Lau MK, Le AT, El-Serag HB. Non-cardia gastric cancer remains important and deadly in the United States: secular trends in incidence and survival. Am J Gastroenterol 2006; 101:2485–92
Borch K, Jonsson B, Tarpila E, et al. Changing pattern of histological type, location, stage and outcome of surgical treatment of gastric carcinoma. Br J Surg 2000; 87:618–26
de Gara CJ, Hanson J, Hamilton S. A population-based study of tumor-node relationship, resection margins, and surgeon volume on gastric cancer survival. Am J Surg 2003; 186:23–7
Hansson LE, Ekstrom AM, Bergstrom R, Nyren O. Surgery for stomach cancer in a defined Swedish population: current practices and operative results. Swedish Gastric Cancer Study Group. Eur J Surg 2000; 166:787–95
Msika S, Benhamiche AM, Jouve JL, Rat P, Faivre J. Prognostic factors after curative resection for gastric cancer: a population-based study. Eur J Cancer 2000; 36:390–6
Msika S, Benhamiche AM, Tazi MA, Rat P, Faivre J. Improvement of operative mortality after curative resection for gastric cancer: population-based study. World J Surg 2000; 24:1137–42
Wainess RM, Dimick JB, Upchurch GR Jr, Cowan JA, Mulholland MW. Epidemiology of surgically treated gastric cancer in the United States, 1988–2000. J Gastrointest Surg 2003; 7:879–83
Baxter NN, Tuttle TM. Inadequacy of lymph node staging in gastric cancer patients: a population-based study. Ann Surg Oncol 2005; 12:981–7
Smith DD, Schwarz RR, Schwarz RE. Impact of total lymph node count on staging and survival after gastrectomy for gastric cancer: data from a large US-population database. J Clin Oncol 2005; 23:7114–24
Sobin LH, Wittekind CH, editors. TNM Classification of Malignant Tumors. 5th ed. New York: John Wiley & Sons, 1997:59–62
MacDonald WC, MacDonald JB. Adenocarcinoma of the esophagus and/or gastric cardia. Cancer 1987; 60:1094–8
Ohno S, Tomisaki S, Oiwa H, et al. Clinicopathologic characteristics and outcome of adenocarcinoma of the human gastric cardia in comparison with carcinoma of other regions of the stomach. J Am Coll Surg 1995; 180:577–82
Kim MA, Lee HS, Yang HK, Kim WH. Clinicopathologic and protein expression differences between cardia carcinoma and noncardia carcinoma of the stomach. Cancer 2005; 103:1439–46
Yang PC, Davis S. Epidemiological characteristics of adenocarcinoma of the gastric cardia and distal stomach in the United States, 1973–1982. Int J Epidemiol 1988; 17:293–7
Hundahl SA, Phillips JL, Menck HR. The National Cancer Data Base Report on poor survival of US gastric carcinoma patients treated with gastrectomy: Fifth Edition American Joint Committee on Cancer staging, proximal disease, and the “different disease” hypothesis. Cancer 2000; 88:921–32
Trivers KF, De Roos AJ, Gammon MD, et al. Demographic and lifestyle predictors of survival in patients with esophageal or gastric cancers. Clin Gastroenterol Hepatol 2005; 3:225–30
Karpeh MS Jr. Should gastric cancer surgery be performed in community hospitals? Semin Oncol 2005; 32(6 Suppl 9):S94–6
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Le, A., Berger, D., Lau, M. et al. Secular Trends in the Use, Quality, and Outcomes of Gastrectomy for Noncardia Gastric Cancer in the United States. Ann Surg Oncol 14, 2519–2527 (2007). https://doi.org/10.1245/s10434-007-9386-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-007-9386-8