
Abstract
Background: 18-F-fluorodeoxyglucose positron emission tomography (FDG-PET) is valuable in staging of esophageal cancer. However, FDG-PET may falsely upstage patients leading to incorrect exclusion from surgical treatment. This study was performed to determine the false-positive rate and possible causes.
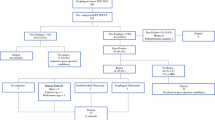
Methods: The rate of false-positive lesions on FDG-PET was documented in 86 out of a group of 98 patients. Lesions were defined as false positive when pathological examination was negative or as absence of tumor activity within 6 months of follow-up. To evaluate the influence of a learning curve on the false-positive rate, the PET scans were revised recently.
Results: False-positive lesions were found in 13 patients (13 of 86; 15%). FDG-PET incorrectly revealed only locoregional node metastases in 5 patients in whom surgery with curative intent was performed. Ten lesions in the other 8 patients were classified as distant organ or as nonregional node metastases (M1a/1b). Finally, 5 patients upstaged to M1a/1b underwent a curative resection. The number of false-positive lesions decreased from 16 to 5 (6%) after revision.
Conclusions: Proper interpretation of FDG-PET in staging esophageal cancer is impeded by false-positive results. Even after completion of the learning curve, positive FDG-PET findings still have to be confirmed by additional investigations.
Similar content being viewed by others


REFERENCES
Rice TW. Clinical staging of esophageal carcinoma: CT, EUS, and PET. Chest Surg Clin N Am 2000;10:471–85.
Block MI, Patterson GA, Sundaresan RS, et al. Improvement in staging of esophageal cancer with the addition of positron emission tomography. Ann Thorac Surg 1997;64:770–6.
Flamen P, Lerut A, Van Cutsem E, et al. Utility of positron emission tomography for the staging of patients with potentially operable esophageal carcinoma. J Clin Oncol 2000;18:3202–10.
Flanagan FL, Dehdashti F, Siegel BA, et al. Staging of esophageal cancer with 18F-fluorodeoxyglucose positron emission tomography. Am J Roentgenol 1997;168:417–24.
Kole AC, Plukker JT, Nieweg OE, Vaalburg W. Positron emission tomography for staging of oesophageal and gastroesophageal malignancy. Br J Cancer 1998;78:521–7.
Luketich JD, Schauer PR, Meltzer CC, et al. Role of positron emission tomography in staging esophageal cancer. Ann Thorac Surg 1997;64:765–9.
Meltzer CC, Luketich JD, Friedman D, et al. Whole-body FDG positron emission tomographic imaging for staging esophageal cancer comparison with computed tomography. Clin Nucl Med 2000;25:882–7.
Wallace MB, Nietert PJ, Earle C, et al. An analysis of multiple staging management strategies for carcinoma of the esophagus: computed tomography, endoscopic ultrasound, positron emission tomography, and thoracoscopy/laparoscopy. Ann Thorac Surg 2002;74:1026–32.
Wren SM, Stijns P, Srinivas S. Positron emission tomography in the initial staging of esophageal cancer. Arch Surg 2002;137:1001–7.
Choi JY, Lee KH, Shim YM, et al. Improved detection of individual nodal involvement in squamous cell carcinoma of the esophagus by FDG PET. J Nucl Med 2000;41:808–15.
Zhuang H, Pourdehnad M, Lambright ES, et al. Dual time point 18F-FDG PET imaging for differentiating malignant from inflammatory processes. J Nucl Med 2001;42:1412–7.
Duarte PS, Zhuang H, Castellucci P, Alavi A. The receiver operating characteristic curve for the standard uptake value in a group of patients with bone marrow metastasis. Mol Imag Biol 2003;4:157–60.
Nguyen AT, Akhurst T, Larson SM, Coit DG, Brady MS. PET Scanning with 18F 2-Fluoro-2-Deoxy-D-glucose (FDG) in patients with melanoma: benefits and limitations. Clin Pos Imag 2003;2:93–8.
Hamacher K, Coenen HH, Stocklin G. Efficient stereospecific synthesis of no-carrier-added 2-[18F]-fluoro-2- deoxy-D-glucose using aminopolyether supported nucleophilic substitution. J Nucl Med 1986;27:235–8.
Shreve PD, Anzai Y, Wahl RL. Pitfalls in oncologic diagnosis with FDG PET imaging: physiologic and benign variants. Radiographics 1999;19:61–77.
Kato H, Kuwano H, Nakajima M, et al. Comparison between positron emission tomography and computed tomography in the use of the assessment of esophageal carcinoma. Cancer 2002;94:921–8.
Kim K, Park SJ, Kim BT, Lee KS, Shim YM. Evaluation of lymph node metastases in squamous cell carcinoma of the esophagus with positron emission tomography. Ann Thorac Surg 2001;71:290–4.
Czernin J, Phelps ME. Positron emission tomography scanning: current and future applications. Annu Rev Med 2002;53:89–112.
Phay JE, Hussain HB, Moley JF. Strategy for identification of novel glucose transporter family members by using internet-based genomic databases. Surgery 2000;128:946–51.
Ishimori T, Saga T, Mamede M, et al. Increased (18)F-FDG uptake in a model of inflammation: concanavalin A–mediated lymphocyte activation. J Nucl Med 2002;43:658–63.
Kubota R, Yamada S, Kubota K, Ishiwata K, Tamahashi N, Ido T. Intratumoral distribution of fluorine-18-fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation tissues studied by microautoradiography. J Nucl Med 1992;33:1972–80.
Strauss LG. Fluorine-18 deoxyglucose and false-positive results: a major problem in the diagnostics of oncological patients. Eur J Nucl Med 1996;23:1409–15.
Yamada S, Kubota K, Kubota R, Ido T, Tamahashi N. High accumulation of fluorine-18-fluorodeoxyglucose in turpentine- induced inflammatory tissue. J Nucl Med 1995;36:1301–6.
Cremerius U, Wildberger JE, Borchers H, et al. Does positron emission tomography using 18-fluoro-2-deoxyglucose improve clinical staging of testicular cancer? Results in a study of 50 patients. Urology 1999;54:900–4.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
van Westreenen, H.L., Heeren, P.A.M., Jager, P.L. et al. Pitfalls of Positive Findings in Staging Esophageal Cancer With F-18-Fluorodeoxyglucose Positron Emission Tomography. Ann Surg Oncol 10, 1100–1105 (2003). https://doi.org/10.1245/ASO.2003.03.005
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1245/ASO.2003.03.005