
Abstract
Background
Recent data support the use of post-mastectomy radiation therapy (PMRT) in women with one to three positive lymph nodes; however, the benefit of PMRT in patients with micrometastatic nodal disease (N1mi) is unknown. We evaluated the survival impact of PMRT in patients with N1mi within the National Cancer Database.
Methods
The pattern of care and survival benefit of PMRT was examined in women with pT1-2N1mi breast cancer who underwent mastectomy without neoadjuvant chemotherapy. Univariable and multivariable Cox proportional hazard models were employed for survival analysis, and subanalyses of high-risk patients and a propensity score-matched (PSM) cohort were completed.
Results
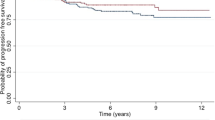
From 2004 to 2014, we identified 14,019 patients who fitted the study criteria. PMRT was delivered in 18.5% of patients and its use increased over the study period. Patients treated with PMRT were younger, had better performance status and larger primaries, were estrogen receptor (ER)-negative, had higher grade, lymphovascular invasion and positive surgical margins, and more often received systemic therapy. PMRT was significantly associated with overall survival (OS) in univariable analysis (hazard ratio [HR] 0.75 [0.64–0.89]), but was not significant in multivariable analysis (adjusted HR 1.01 [0.84–1.20]). There was no survival benefit to PMRT in ER-negative, high-grade, and/or young patients. There were 2 (0.9%) death events in the sentinel lymph node biopsy (SLNB) + PMRT group versus 21 (2.9%) in the SLNB-alone group (log-rank p = 0.053), and 8 (3.9%) death events in the axillary lymph node biopsy (ALNB) + PMRT group versus 27 (3.6%) in the axillary lymph node dissection-alone group (p = 0.82). There was no significant association between PMRT and OS within the PSM subgroup.
Conclusion
In this largest reported retrospective study, no OS differences were associated with PMRT, which suggests that PMRT may not benefit every patient with microscopic nodal disease.


Similar content being viewed by others


References
Recht A, Comen EA, Fine RE, Fleming GF, Hardenbergh PH, Ho A, et al. Postmastectomy radiotherapy: an American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology focused guideline update. Practical Radiation Oncology. 2016;6(6):e219–e234.
McGale P, Taylor C, Correa C, Cutter D, Duane F, Ewertz M, et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet. 2014;383(9935):2127–35.
Poortmans PM, Collette S, Kirkove C, Van Limbergen E, Budach V, Struikmans H, et al. Internal mammary and medial supraclavicular irradiation in breast cancer. New England Journal of Medicine. 2015;373(4):317–27.
McCready DR, Yong WS, Ng AK, Miller N, Done S, Youngson B. Influence of the new AJCC breast cancer staging system on sentinel lymph node positivity and false-negative rates. Journal of the National Cancer Institute. 2004;96(11):873–75.
Hieken TJ, and Boughey JC. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases: commentary on the IBCSG 23-01 Trial. Gland Surgery. 2013;2(3):128–32.
Galimberti V, Cole BF, Zurrida S, Viale G, Luini A, Veronesi P, et al. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23–01): a phase 3 randomised controlled trial. The Lancet Oncology. 2013;14(4):297–305.
Jagsi R, Chadha M, Moni J, Ballman K, Laurie F, Buchholz TA, et al. Radiation field design in the ACOSOG Z0011 (Alliance) Trial. Journal of Clinical Oncology. 2014;32(32):3600–6.
Schemper M, Smith TL. A note on quantifying follow-up in studies of failure time. Control Clin Trials. 1996;17(4):343–6.
Giuliano AE, Hunt KK, Ballman KV, Beitsch PD, Whitworth PW, Blumencranz PW, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA. 2011; 305(6):569–75.
Solá M, Alberro JA, Fraile M, Santesteban P, Ramos M, Fabregas R, et al. Complete axillary lymph node dissection versus clinical follow-up in breast cancer patients with sentinel node micrometastasis: final results from the multicenter clinical trial AATRM 048/13/2000. Ann Surg Oncol. 2013;20(1):120–7.
Sávolt Á, Péley G, Polgár C, Udvarhelyi N, Rubovszky G, Kovács E, et al. Eight-year follow up result of the OTOASOR trial: The optimal treatment of the axilla–surgery or radiotherapy after positive sentinel lymph node biopsy in early-stage breast cancer: A randomized, single centre, phase III, non-inferiority trial. Eur J Surg Oncol. 2017;43(4):672–9.
Donker M, van Tienhoven G, Straver ME, Meijnen P, van de Velde CJ, Mansel RE, et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): a randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol. 2014;15(12):1303–10.
Mamtani A, Patil S, Stempel M, Morrow M. Axillary Micrometastases and Isolated Tumor Cells Are Not an Indication for Post-mastectomy Radiotherapy in Stage 1 and 2 Breast Cancer. Annals of Surgical Oncology. 2017;24(8):2182–88.
FitzSullivan E, Bassett RL, Kuerer HM, Mittendorf EA, Yi M, Hunt KK, et al. Outcomes of sentinel lymph node-positive breast cancer patients treated with mastectomy without axillary therapy. Ann Surg Oncol. 2017;24(3):652–59.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
S Peter Wu, Moses Tam, Fauzia Shaikh, Anna Lee, Jennifer Chun, Freya Schnabel, Amber Guth, Sylvia Adams, David Schreiber, Cheonguen Oh, and Naamit K. Gerber have no actual or potential conflicts of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Wu, S.P., Tam, M., Shaikh, F. et al. Post-mastectomy Radiation Therapy in Breast Cancer Patients with Nodal Micrometastases. Ann Surg Oncol 25, 2620–2631 (2018). https://doi.org/10.1245/s10434-018-6632-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-018-6632-1