
Abstract
Background
Common etiological agents of neonatal meningitis include group B Streptococcus, Escherichia coli, and Staphylococcus aureus. Here we report a rare pathogen – Streptococcus bovis – causing meningitis in a premature neonate with Down syndrome.
Case presentation
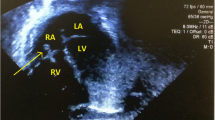
A 26-day-old Asian male neonate with Down syndrome presented with a history of high-grade fever, poor sucking, poor cry, and reduced activity. On admission, he was febrile and had features of circulatory collapse. A cerebrospinal fluid examination confirmed bacterial meningitis and blood culture isolated the causative organism: group D Streptococcus, which was verified as Streptococcus bovis biotype 2. An echocardiogram did not show evidence of infective endocarditis.
Conclusions
This is probably the first report of neonatal meningitis due to Streptococcus bovis in a child with Down syndrome. Although our patient did not show features of overt immunodeficiency, subtle abnormalities in his immune system would have predisposed him to infection with this unusual organism. This case highlights the need for considering unusual pathogens when managing serious infections in children with Down syndrome.
Similar content being viewed by others


Background
Neonatal meningitis is a serious infection of the central nervous system which results in significant morbidity and mortality [1]. Common etiological agents are Streptococcus agalactiae (group B Streptococcus), Staphylococcus aureus, and Escherichia coli worldwide. Rare pathogens that cause neonatal meningitis include coagulase-negative Staphylococci, Pseudomonas, Klebsiella, Enterococcus, and Listeria monocytogenes; however, they are mostly seen in neonates with congenital or acquired immunodeficiency [2]. Here we report a rare pathogen – Streptococcus bovis – causing meningitis in a premature neonate with Down syndrome. This case highlights the importance of considering rare and unusual pathogens when encountered with severe infections in children with Down syndrome.
Case presentation
A 26-day-old Asian male neonate with Down syndrome presented with a history of high-grade fever, poor sucking, poor cry, and reduced activity of 1-day duration. He was born by emergency lower segmental cesarean section to a 43-year-old primigravida mother at 34 weeks of gestation with a birth weight of 1.68 kg. Antenatal history was complicated with pregnancy-induced hypertension and reversed diastolic flow in umbilical arteries during third trimester. The baby had been exclusively breast-fed since birth and did not have vomiting or diarrhea.
On examination, he was febrile, 38.3 °C (101 °F), and had mottled skin. His pulse rate was 170 beats per minute, with prolonged capillary refilling time and cold peripheries; his blood pressure was 89/53 mmHg. Precordial evaluation revealed dual rhythm and a grade 3 ejection systolic murmur at the pulmonary area. His respiratory rate was 50/minute with signs of moderate respiratory distress. His anterior fontanel was flat, both pupils were equally reactive to light, and examinations of spine and extremities were normal. A provisional diagnosis of septic shock was made and initial resuscitation with supplementary oxygen and normal saline bolus was carried out; intravenously administered flucloxacillin and cefotaxime were commenced.
A complete blood count revealed total leukocytes 6500/mm3 (neutrophils 72%, lymphocytes 17%, and monocytes 9%), hemoglobin 13.2 g/dl, and platelet count 349,000/mm3. Random blood glucose was 123 mg/dl and C-reactive protein level was 38.6 mg/L. A lumbar puncture was performed 4 hours after the first dose of antibiotics and cerebrospinal fluid (CSF) analysis revealed: leukocytes 11/mm3 (ten polymorphonuclear cells and one lymphocytes), protein 124 mg/dL, and glucose 52 mg/dL. Blood culture yielded growth of group D Streptococcus, which was verified as Streptococcus bovis biotype 2 by manual analysis (demonstrating growth in MacConkey broth agar and Bile Esculin agar and absent growth in 6.5% sodium chloride medium) and by the automated bacterial identification technology. The organism was sensitive to penicillin and ampicillin; therefore, flucloxacillin was replaced by intravenously administered benzylpenicillin. CSF Gram stain demonstrated no organisms and cultures of CSF were negative probably due to antibiotic administration prior to lumbar puncture. Two-dimensional echocardiography revealed a small ostium secundum atrial septal defect without evidence of infective endocarditis. Karyotype confirmed trisomy 21.
Intravenously administered benzylpenicillin and cefotaxime were continued for 21 days during which the baby showed complete recovery. There were no neurological complications during acute or convalescent periods. The follow-up after 6 months confirmed normal neurological examination except for hypotonia due to Down syndrome and normal occipitofrontal circumference.
Discussion
Streptococcus bovis is a Gram-positive, Lancefield group D Streptococcus which is found in the pharynx, nose, and gastrointestinal tract of healthy humans [3]. It is an unusual etiology of human diseases; however, it is known to cause infective endocarditis in hosts with predisposing cardiac defects [4]. Meningitis due Streptococcus bovis is rare and is reported in patients with immunodeficiency, cancer, or colon diseases [5,6,7].
The neonate described in this case report has Down syndrome; however, he did not show other features of primary or secondary immunodeficiency. He had an atrial septal defect but was neither predisposed to nor had infective endocarditis. To the best of our knowledge this is the first case report of neonatal meningitis due to Streptococcus bovis in a child with Down syndrome. Previous reports have shown that children with Down syndrome have intrinsic defects in the immune system and are at higher risk of developing infections due to streptococcal organisms [8, 9]. Abnormalities in the immune system associated with Down syndrome include reduced T lymphocyte and B lymphocyte counts, absence of normal lymphocyte expansion in infancy, impaired mitogen-induced T cell proliferation, reduced specific antibody responses to immunizations, and defects of neutrophil chemotaxis [10]. We believe that the presence of Down syndrome in this baby would have predisposed him to the severe infection with this unusual organism.
Alternatively, the infection by Streptococcus bovis could be related to the premature birth of this baby. Immune system components, both innate and adaptive, show distinct deficits in premature babies which include deficient skin barrier function, fewer commensals in intestinal microbiome, inefficient production of complement proteins, limited neutrophil storage pool, reduced expression of CD40 ligand, and inefficient class switching from IgM to other antibody isotypes [11]. These deficits may also have contributed to infection by Streptococcus bovis in this child.
Another important fact about Streptococcus bovis infection is its association with colorectal cancer. Particularly in adults, Streptococcus bovis bacteremia and endocarditis are associated with colon cancer, neoplastic colon polyps, and other gastrointestinal malignancies [12]. The significance of these associations is not yet known and it is not clear whether infections are causative factors or results of these malignancies. None of the reported cases of pediatric patients with Streptococcus bovis infections show associations with colonic diseases; therefore, this association may be limited to adults.
Conclusions
In conclusion, this case report adds to the medical literature of causative organisms of neonatal meningitis in an apparently immunocompetent child with Down syndrome. It also highlights the need for considering unusual pathogens when managing severe infections in children with Down syndrome.
References
Ogunlesi TA, Odigwe CC, Oladapo OT. Adjuvant corticosteroids for reducing death in neonatal bacterial meningitis. Cochrane Database Syst Rev. 2015;11:CD010435.
Furyk JS, Swann O, Molyneux E. Systematic review: neonatal meningitis in the developing world. Tropical Med Int Health. 2011;16(6):672–9.
Alvarez A, Jia Y, Garcia CJ, Rosas-Blum ED, Boman D, Zuckerman MJ. Streptococcus bovis Bacteremia in Neonates in a Predominantly Hispanic Population. Front Pediatr. 2015;3:92.
Vogkou CT, Vlachogiannis NI, Palaiodimos L, Kousoulis AA. The causative agents in infective endocarditis: a systematic review comprising 33,214 cases. Eur J Clin Microbiol Infect Dis. 2016;35(8):1227–45.
van Samkar A, Brouwer MC, Pannekoek Y, van der Ende A, van de Beek D. Streptococcus gallolyticus meningitis in adults: report of five cases and review of the literature. Clin Microbiol Infect. 2015;21(12):1077–83.
Beneteau A, Levy C, Foucaud P, Bechet S, Cohen R, Raymond J, Dommergues MA. Childhood meningitis caused by Streptococcus bovis group: clinical and biologic data during a 12-year period in France. Pediatr Infect Dis J. 2015;34(2):136–9.
Grant RJ, Whitehead TR, Orr JE. Streptococcus bovis meningitis in an infant. J Clin Microbiol. 2000;38(1):462–3.
Kusters MA, Verstegen RH, Gemen EF, de Vries E. Intrinsic defect of the immune system in children with Down syndrome: a review. Clin Exp Immunol. 2009;156(2):189–93.
Morais VM, Orsi AR, Maranhao FC, Castro TM, Castro KC, Silva DM. Prevalence of beta-hemolytic Streptococcus in children with special health care needs. Braz J Otorhinolaryngol. 2012;78(5):110–5.
Ram G, Chinen J. Infections and immunodeficiency in Down syndrome. Clin Exp Immunol. 2011;164(1):9–16.
Collins A, Weitkamp JH, Wynn JL. Why are preterm newborns at increased risk of infection? Arch Dis Child Fetal Neonatal Ed. 2018. doi: https://doi.org/10.1136/archdischild-2017-313595.
Abdulamir AS, Hafidh RR, Abu Bakar F. The association of Streptococcus bovis/gallolyticus with colorectal tumors: the nature and the underlying mechanisms of its etiological role. J Exp Clin Cancer Res. 2011;30:11.
Acknowledgements
Not applicable.
Funding
Not applicable.
Availability of data and materials
Not applicable.
Author information
Authors and Affiliations
Contributions
All authors contributed to the clinical management of the patient, writing of manuscript, and final approval of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient’s legal guardian(s) for publication of this case report. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Mettananda, S., Kamalanathan, P. & Dhananja Namalie, K. Streptococcus bovis – unusual etiology of meningitis in a neonate with Down syndrome: a case report. J Med Case Reports 12, 93 (2018). https://doi.org/10.1186/s13256-018-1634-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-018-1634-y