
Abstract
Background
Intrauterine contraceptive device is the most common method of reversible contraception in women. The intrauterine contraceptive device can perforate the uterus and can also migrate into pelvic or abdominal organs. Perforation of the urinary bladder by an intrauterine contraceptive device is not common. In West Africa, intravesical migration of an intrauterine contraceptive device has been rarely reported. In this report, we present a case of an intrauterine contraceptive device migration into the urinary bladder of a 33 year old African woman at the Komfo Anokye Teaching Hospital, Kumasi, Ghana.
Case report
A 33 year old African woman presented with persistent urinary tract infection of 7 months duration despite appropriate antibiotic treatments. An abdominal ultrasonography revealed a urinary bladder calculus which was found to be an intrauterine contraceptive device on removal at cystoscopy. She got pregnant whilst having the intrauterine contraceptive device in place and delivered at term.
Conclusion
The presence of recurrent or persistent urinary tract infection in any woman with an intrauterine contraceptive device should raise the suspicion of intravesical migration of the intrauterine contraceptive device.
Similar content being viewed by others


Background
Intrauterine contraceptive device (IUCD) is the most common method for reversible contraception in women because it is effective, safe, and cost effective [1]. One of the major complications of IUCD is perforation of the uterus and the migration of the device into pelvic or abdominal organs [2]. However, intravesical migration of IUCD is not common. IUCD insertion is routinely performed in Komfo Anokye Teaching Hospital (KATH), the second largest teaching hospital in Ghana. There has been no report of intravesical migration of IUCD in Ghana and same has rarely been reported in the West African sub-region. In Nigeria, Eke et al. reported a case of intravesical migration of IUCD [3].
We present the case of a 33-year-old African woman with persistent Escherichia coli (E. coli) urinary tract infection (UTI) due to intravesical migration of an IUCD appearing as a bladder calculus on ultrasonography.
Case presentation
A 33-year-old African woman, para 4 with one spontaneous abortion was referred to the Urology clinic with complaints of dysuria, strangury, frequency of micturition, urgency, nocturia and severe lower abdominal pain. These symptoms had persisted for 7 months despite repeated treatment for E. coli isolated urinary tract infections by her attending gynaecologist. She used an IUCD for contraception for 2 years after the birth of her second child. The IUCD was removed before her third pregnancy. Forty (40) days after her third delivery, a copper T IUCD was inserted by her gynaecologist.
The patient reported after 21 months post IUCD insertion with symptoms of pregnancy. Further evaluation revealed she was 5 months pregnant. The IUCD strings were not visible on gynaecologic examination and transvaginal ultrasonography by the gynaecologist failed to detect the IUCD. Thus, the IUCD was assumed to have fallen out, permitting the patient to have her fourth pregnancy. She had an uneventful pregnancy and was delivered by a lower uterine segment caesarean section at term on account of two previous caesarean sections.
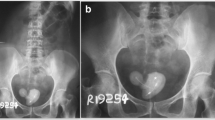
She started experiencing lower urinary tract symptoms 15 months post delivery. Urine culture persistently isolated E. coli despite appropriate antibiotic treatments by the attending gynaecologist. She was therefore referred to the urologist for further evaluation and management. An abdominal ultrasonography by the radiologist revealed a urinary bladder calculus (Fig. 1). This turned out to be a copper T IUCD at cystoscopic removal. The patient’s urinary tract symptoms resolved completely after the removal of the IUCD.

Abdominal ultrasonography showing the intrauterine contraceptive device as a bladder calculus (arrowed)
Discussion
Intrauterine contraceptive device (IUCD) is the most common method for reversible contraception in women because it is safe, inexpensive and readily available [1]. Uterine perforation and migration of the IUCD into abdominal or pelvic organs is a major complication of IUCD insertion [2] with an incidence of 1.9–3.6 per 1000 insertions [4]. Factors influencing the risk of perforation include the type of IUCD used, the time of insertion, the insertion technique, and anatomy of the cervix and uterus [4]. The exact mode of uterine perforation and IUCD migration is unclear [5]. However, it is believed that perforation mostly occurs at the time of insertion but may also occur spontaneously at a later time or during puerperium [6].
The presence of pain and bleeding per vaginam after IUCD insertion suggests that uterine perforation may have occurred at the time of insertion [7]. Secondary perforation may be due to slow migration through the myometrium which may be enhanced by spontaneous uterine contractions [8]. When a pregnancy occurs in a patient with an IUCD, there must be a high suspicion of uterine perforation and possible migration [1]. IUCDs which migrate to the urinary bladder are either located in the bladder wall or within the bladder lumen [1].
Most patients with intravesical migration of IUCD are symptomatic [8] with UTI being the most common presentation [9]. The patient in this case presented with persistent UTI.
Transvaginal ultrasonography is the investigation of choice for locating the intravesical IUCD [8]. However, in this case a transabdominal ultrasonography by the radiologist showed the intravesical IUCD as a bladder calculus. Ultrasonography is operator-dependent and this may have accounted for the failure to detect the IUCD by the gynaecologist.
Cystoscopy is another means of visualising the intravesical IUCD and is helpful for its removal [8].
All IUCDs which have migrated into the urinary bladder must be removed even if they are asymptomatic. This is to prevent complications such as calculus formation and bladder rupture [1].
An IUCD which has migrated into the urinary bladder is treated by cystoscopic removal or by open suprapubic cystotomy [10].
Cystoscopic removal is preferred because it has a low morbidity and is highly effective [11]. In this case, cystoscopic removal was done successfully. Open surgery is currently restricted to centres without cystoscopic facilities and also for the removal of IUCDs with calculus formation that are not amenable to cystoscopic removal [7]. Laparoscopic removal, a minimally invasive alternative to open surgery can also be used [5].
Conclusion
The presence of recurrent or persistent UTI in any woman who gets pregnant despite having had an IUCD inserted should raise the suspicion of intravesical migration of the IUCD. Early ultrasonography for the cause of recurrent or persistent UTI is recommended.
Abbreviations
- IUCD:
-
intrauterine contraceptive device
- KATH:
-
Komfo Anokye Teaching Hospital
- UTI:
-
urinary tract infection
- E. coli :
-
Escherichia coli
References
Kandirali E, Mehmet AT, Atilla S, Ahmet M. Double intrauterine device: presented with protruding stone. Marmara Med J. 2008;21(1):061–3.
Nitke S, Rabinerson D, Dekel A, Sheiner E, Kaplan B, Hackmon R. Lost levonorgestrel IUD: diagnosis and therapy. Contraception. 2004;69(4):289–93.
Eke N, Okpani AO. Extrauterine translocated contraceptive device: a presentation of five cases and revisit of the enigmatic issues of iatrogenic perforation and migration. Afr J Reprod Health. 2003;7(3):117–23.
Farmer M, Webb A. Intrauterine device insertion-related complications: can they be predicted? J Fam Plan Reprod Health Care R Coll Obstet Gynaecol. 2003;29(4):227–31.
Tosun M, Celik H, Yavuz E, Cetinkaya MB. Intravesical migration of an intrauterine device detected in a pregnant woman. Can Urol Assoc J. 2010;4(5):E141–3.
Markovitch O, Klein Z, Gidoni Y, Holzinger M, Beyth Y. Extrauterine mislocated IUD: is surgical removal mandatory? Contraception. 2002;66(2):105–8.
Mascarenhas MP, Tiraboschi RB, Paschoalin VP, Costa EAP, Suzuki Bellucci CH, Bessa Junior J, et al. Exercise-induced hematuria as the main manifestation of migration of intrauterine contraceptive device into the bladder. Case Rep Urol Case Rep Urol. 2012;2012:e736426.
Priyadarshi V, Singh M, Kumar V, Tiwari R, Gupta SK, Sehgal N. An unusual cause of bladder stones in a female: a migrant intrauterine contraceptive device. UroToday Int J [Internet]. 2012 [cited 2015 Aug 24];05(06). http://www.urotoday.com/index.php?option=com_content&Itemid=230&catid=1356&id=54877&lang=en&view=article.
Dietrick DD, Issa MM, Kabalin JN, Bassett JB. Intravesical migration of intrauterine device. J Urol. 1992;147(1):132–4.
Hick EJ, Hernández J, Yordán R, Morey AF, Avilés R, García CR. Bladder calculus resulting from the migration of an intrauterine contraceptive device. J Urol. 2004;172(5 Pt 1):1903.
Vagholkar S, Vagholkar K. Secondary vesical calculus resulting from migration of an intrauterine contraceptive device. Case Rep Obstet Gynecol. 2012;2012:603193.
Authors’ contributions
CKG-S contributed to conception and design of this study and he was involved in drafting the manuscript and revising it critically for important intellectual content. PM contributed to conception and design of this study and he was involved in drafting the manuscript and revising it critically for important intellectual content. EM contributed to the design of this study and he was involved in drafting the manuscript and revising it critically for important intellectual content. KA contributed to the design of this study and he was involved in drafting the manuscript and revising it critically for important intellectual content. RA participated in the design of this study and helped to draft the manuscript. KAAA participated in the design of this study and helped to draft the manuscript. GA helped to draft the manuscript and contributed in revising it for intellectual content. KB-N helped to draft the manuscript and contributed in revising it for intellectual content. KO-B helped to draft the manuscript and contributed to revising it for intellectual content. DA helped to draft the manuscript and contributed to revising it for intellectual content. BF-T helped with the literature search and drafting of the manuscript. IA helped with the literature search and drafting of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
We thank Professor Francis Abantanga who critically revised the manuscript to improve the style of written English.
Competing interests
The authors declare that they have no competing interests.
Informed consent
Written informed consent was obtained from the patient for publication of this Case Report and the accompanying image.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Gyasi-Sarpong, C.K., Maison, P.O.M., Morhe, E. et al. Intravesical migration of an intrauterine device. BMC Res Notes 9, 4 (2016). https://doi.org/10.1186/s13104-015-1792-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13104-015-1792-6