
Abstract
Background
Canavan disease is a devastating autosomal recessive leukodystrophy leading to spongiform degeneration of the white matter. There is no cure or treatment for Canavan disease, and disease progression is poorly understood.
Results
We report a new presentation of a patient found to have Canavan disease; brain magnetic resonance imaging (MRI) revealed white matter cytotoxic edema, indicative of an acute active destructive process. We performed a comprehensive review of published cases of Canavan disease reporting brain MRI findings, and found that cytotoxic brain edema is frequently reported in early Canavan disease.
Conclusions
Our results and the literature review support the notion of an acute phase in Canavan disease progression. These findings suggest that there is a window available for therapeutic intervention and support the need for early identification of patients with Canavan disease.
Similar content being viewed by others

Background
Canavan disease is a devastating autosomal recessive leukodystrophy leading to spongiform degeneration of the white matter [1]. Deficient aspartoacylase activity from mutations in ASPA lead to accumulation of N-acetylaspartic acid (NAA) in the brain, myelin loss [2, 3], and NAA acidemia with elevated levels of NAA present in cerebrospinal fluid, blood, and urine [4]. Patients with Canavan disease typically present with developmental delay, focal neurological signs, macrocephaly, and even neurological deterioration in the first year of life [5]. There is no cure or treatment for Canavan disease, and disease progression is poorly understood. Magnetic resonance imaging (MRI) of the brain can be diagnostic, based on the presence of diffuse symmetric T2 hyperintense signal in the cortical white matter and basal ganglia with an accompanying elevated NAA peak seen on magnetic resonance spectroscopy (MRS) [6, 7].
We report a patient presenting with brain MRI white matter cytotoxic edema, indicative of an acute active destructive process, who was found to have Canavan disease. Review of the literature suggests that cytotoxic edema is a common finding in early Canavan disease, and supports the potential for a therapeutic window of intervention.
Methods
A ten-week old boy presented with episodes of right pendular horizontal nystagmus lasting two to three seconds. He had been born full term following an uncomplicated pregnancy to nonconsanguineous Caucasian parents. Vitals and general physical exam were unremarkable and head circumference was at the 63rd percentile. Neurologic examination was notable for a lack of visual tracking, central hypotonia, limb hyperreflexia, and choreiform limb movements.
We conducted PubMed searches for the terms “Canavan” and “MRI” or “Canavan” and “diffusion” to identify potential relevant publications. Identified publications were reviewed for relevant cases involving cytotoxic edema on brain MRI and data were extracted (STM and JLB).
Results
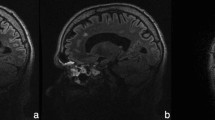
Brain MRI performed at presentation revealed extensive diffusion restriction symmetrically in the subcortical white matter of both cerebral hemispheres, extending inferiorly in the corticospinal tracts and into the brainstem including the dorsal and ventral pons, with T2 hyperintensity and T1 hypointensity of the white matter (Fig. 1 a-h). Single voxel magnetic resonance spectroscopy (MRS) of the white matter of the posterior left hemisphere demonstrated an elevated peak at 2.02 ppm indicating increased NAA (Fig. 1i). The short echo-time (TE) spectrum N-acetylaspartic acid/creatine (NAA/CR) ratio was elevated at 2.45 (normal for age 1.71) [8]. Urine organic acids had elevated NAA excretion (>750 mmol NAA/mol creatinine), consistent with Canavan disease. Sequencing of the ASPA gene demonstrated a homozygous p.Ala305Glu (c.914 C > A) point mutation confirming the diagnosis.

a-h Axial MRIs. a DWI shows hyperintensity in the internal capsule and subcortical white matter; B) ADC demonstrates corresponding hypointensities; c T2 FLAIR image; d T1 image. e DWI with hyperintensities in the subcortical white matter; f Corresponding ADC hypointensities; g T2 image; d T1 image. i Single voxel MRS demonstrates increased NAA (arrow, peak at 2.02 ppm; choline, asterisk, 3.2 ppm; creatine, arrowhead, 3 ppm); inset shows area of analysis in the posterior left hemisphere
To determine if cytotoxic edema with diffusion restriction was a common pathophysiological feature of Canavan disease we reviewed cases using PubMed. We identified 81 potentially relevant publications; including our own report there were 13 Canavan disease patients in whom cytotoxic edema and diffusion restriction was reported (Table 1). The median age of presentation was 12 months (average age 32 months; range 0.8 to 171 months). For the eleven patients in whom gender was reported, ten were male. Of nine cases reporting head size, one patient was microcephalic, five were normocephalic, and four were macrocephalic.
Discussion
We found that cytotoxic edema with corresponding diffusion restriction on brain MRI is more commonly observed in Canavan disease than previously appreciated. Besides our own case, we identified twelve other published reports of Canavan disease with diffusion restriction. It is difficult to assess the frequency of diffusion restriction in Canavan disease, since many published cases of Canavan disease do not include MRI reports, and diffusion restriction may only be present early in the disease course. Because diffusion restriction has not been considered as a presenting feature of Canavan disease, patients have sometimes first been evaluated for other non-leukodystrophy causes, e.g., stroke [9]. Further, it is increasing recognized that there is a broader phenotypic variability [5] with milder clinical courses in some patients [10] and even absence of features consider pathognomonic; for example the absence of macrocephaly [11].
Disease pathology in Canavan is related to NAA accumulation [2, 3]. In turn, the degree of ASPA impairment from different mutations correlates with clinical disease severity [12]. While NAA accumulation appears responsible for the spongiform myelin loss, NAA also has important roles in normal CNS function. Acetate derived from catabolism of NAA by ASPA is utilized by oligodendrocytes to synthesize the lipid component of the myelin sheath [1]. The ASPA enzyme is expressed widely in the body, but NAA is found exclusively in the brain [13, 14]. It has been shown that during neuronal development increased myelination correlates with increased ASPA activity [15]. NAA also appears to function as a molecular water pump in neurons [16]. These roles of NAA may contribute to the histopathology of Canavan disease, which includes astroglial swelling and intramyelinic edema [17, 18], and which may in turn be correlated with alterations in anisotropy and the diffusion coefficient seen on MRI. Diffuse brain edema with an increase in cerebral water content is also seen in other disorders (for example Congenital Muscular Dystrophy with Merosin Deficiency [19]), but without NAA accumulation, raising the possibility that NAA accumulation is not the primary cause of the edema.
Interest in improved understanding of the pathology and the early diagnosis of Canavan disease has arisen in part because of the potential for new treatments [20]. Gene therapy replacement of ASPA has been used successfully in a rodent Canavan model and appears safe in humans [21, 22]. Pharmacologic strategies to target osmotic pressure in Canavan also appear promising [23]. However, screening for Canavan disease is only recommended for high-risk groups [5], although advances in next-generation sequencing and in liquid chromatography-tandem mass spectrometry (e.g., [4]), suggest increased potential for broader newborn screening. The presence of cytotoxic edema, indicated by an increase in diffusion restriction [24], suggests that there is an acute neurotoxic process occurring. Because the diffusion restriction is abnormal for only approximately a week or less after damage, the presence of diffusion restriction shows that at least some of the disease pathology in Canavan disease is occurring post-natally. If a therapy was available it could be instituted as soon as the diagnosis was made, even if some disease progression had already occurred.
Conclusions
Our case and review of the literature show that cytotoxic edema with diffusion restriction on brain MRI is often observed in infant-onset Canavan disease, and if an infant presents with diffusion restriction Canavan disease should be considered in the differential. Our results support the notion of an acute phase in disease progression. Together with evidence that NAA levels are related to myelin degeneration [2, 3], that NAA levels rise during the first year of life in Canavan disease [25], and the possibility for potential treatments [20, 22, 23], these findings suggest that there is a window available for therapeutic intervention and support the need for early identification of patients with Canavan disease.
References
Moffett JR, Ross B, Arun P, Madhavarao CN, Namboodiri AM. N-Acetylaspartate in the CNS: from neurodiagnostics to neurobiology. Prog Neurobiol. 2007;81:89–131.
Maier H, Wang-Eckhardt L, Hartmann D, Gieselmann V, Eckhardt M. N-Acetylaspartate synthase deficiency corrects the myelin phenotype in a canavan disease mouse model but does not affect survival time. J Neurosci. 2015;35:14501–16.
Guo F, Bannerman P, Mills Ko E, Miers L, Xu J, Burns T, Li S, Freeman E, McDonough JA, Pleasure D. Ablating N-acetylaspartate prevents leukodystrophy in a Canavan disease model. Ann Neurol. 2015;77:884–8.
Al-Dirbashi OY, Rashed MS, Al-Qahtani K, Al-Mokhadab MA, Kurdi W, Al-Sayed MA. A quantification of N-acetylaspartic acid in urine by LC-MS/MS for the diagnosis of Canavan disease. J Inherit Metab Dis. 2007;30:612.
Matalon R, Michals-Matalon K. Canavan disease. 1999 Sep 16 [updated 2011 Aug 11]. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Fong CT, Mefford HC, Smith RJH, Stephens K, editors. GeneReviews [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2016. Available from: http://www.ncbi.nlm.nih.gov/books/NBK1234/. Accessed May 15, 2016.
Sener RN. Canavan disease: diffusion magnetic resonance imaging findings. J Comput Assist Tomogr. 2003;27:30–3.
Barkovich AJ, Patay Z. Metabolic, toxic, and inflammatory brain disorders. In: Barkovich AJ, Raybaud C, editors. Pediatric Neuroimaging. 5th ed. Philadelphia: Wolters Kluwer Health; 2012. p. 81–239.
Pouwels PJW, Brockmann K, Kruse B, Wilken B, Wick M, Hanefeld F, Frahm J. Regional age dependence of human brain metabolites from infancy to adulthood as detected by quantitative localized proton MRS. Pediatr Res. 1999;46:474.
Delaney KE, Kralik SF, Hainline BE, Golomb MR. An atypical case of canavan disease with stroke-like presentation. Pediatr Neurol. 2015;52:218–21.
Sarret C, Boespflug-Tanguy O, Rodriguez D. Atypical clinical and radiological course of a patient with Canavan disease. Metab Brain Dis. 2016;31:475–9.
Gowda VK, Bhat MD, Srinivasan VM, Prasad C, Benakappa A, Faruq M. A case of Canavan disease with microcephaly. Brain Dev. 2016;38:759–62.
Zano S, Wijayasinghe YS, Malik R, Smith J, Viola RE. Relationship between enzyme properties and disease progression in Canavan disease. J Inherit Metab Dis. 2013;36:1–6.
Tallan HH. Studies on the distribution of NAA in brain. J Biol Chem. 1957;224:41–5.
Kaul R, Gao GP, Balamurugan K, Matalon R. Cloning of the human aspartoacylase cDNA and a common missense mutation in Canavan disease. Nat Genet. 1993;5:118–23.
Bhakoo KK, Craig TJ, Styles P. Developmental and regional distribution of aspartoacylase in rat brain tissue. J Neurochem. 2001;79:211–20.
Baslow MH, Guilfoyle DN. Canavan disease, a rare early-onset human spongiform leukodystrophy: insights into its genesis and possible clinical interventions. Biochimie. 2013;95:946–56.
Towfighi J, Friedman Z, Maisels MJ. Spongy degeneration of the central nervous system (van Bogaert–Bertrand type?) in a newborn infant. Acta Neuropathol (Berl). 1977;37:267–70.
Harding BN, Surtees R. Metabolic and neurodegenerative diseases of childhood. In: Graham DI, Lantos PL, editors. Greenfield’s neuropathology, vol. 1. 7th ed. London: Arnold Publishers; 2002. p. 485–517.
Leite CC, Reed UC, Otaduy MC, Lacerda MT, Costa MO, Ferreira LG, Carvalho MS, Resende MB, Marie SK, Cerri GG. Congenital muscular dystrophy with merosin deficiency: 1H MR spectroscopy and diffusion-weighted MR imaging. Radiology. 2005;235:190–6.
Roscoe RB, Elliott C, Zarros A, Baillie GS. Non-genetic therapeutic approaches to Canavan disease. J Neurol Sci. 2016;366:116–24.
McPhee SW, Francis J, Janson CG, Serikawa T, Hyland K, Ong EO, Raghavan SS, Freese A, Leone P. Effects of AAV-2-mediated aspartoacylase gene transfer in the tremor rat model of Canavan disease. Brain Res Mol Brain Res. 2005;135:112–21.
Leone P, Shera D, McPhee SW, Francis JS, Kolodny EH, Bilaniuk LT, Wang DJ, Assadi M, Goldfarb O, Goldman HW, Freese A, Young D, During MJ, Samulski RJ, Janson CG. Long-term follow-up after gene therapy for canavan disease. Sci Transl Med. 2012;4:165ra163.
Assadi M, Janson C, Wang DJ, Goldfarb O, Suri N, Bilaniuk L, Leone P. Lithium citrate reduces excessive intra-cerebral N-acetyl aspartate in Canavan disease. Eur J Paediatr Neurol. 2010;14:354–9.
Schaefer PW, Grant PE, Gonzalez RG. Diffusion-weighted MR imaging of the brain. Radiology. 2000;217:331–45.
Janson CG, McPhee SW, Francis J, Shera D, Assadi M, Freese A, Hurh P, Haselgrove J, Wang DJ, Bilaniuk L, Leone P. Natural history of Canavan disease revealed by proton magnetic resonance spectroscopy (1H-MRS) and diffusion-weighted MRI. Neuropediatrics. 2006;37(4):209–21.
Acknowledgements
Not applicable.
Funding
The authors state they have no funding related to this project.
Availability of data and materials
Not applicable.
Authors’ contributions
STM and JLB analyzed and interpreted the patient data and other cases. All authors contributed to interepretation of the data, and read and approved the final manuscript.
Competing interests
The authors state that they have no competing interests.
Consent for publication
Consent for publication was provided by the parents, whom we thank for the help.
Ethics approval and consent to participate
The Institutional Review Boards of the University of Utah and Intermountain Healthcare (IH) approved this study.
Data sharing and supplemental materials
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study. There are no supplemental materials associated with this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Merrill, S.T., Nelson, G.R., Longo, N. et al. Cytotoxic edema and diffusion restriction as an early pathoradiologic marker in canavan disease: case report and review of the literature. Orphanet J Rare Dis 11, 169 (2016). https://doi.org/10.1186/s13023-016-0549-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-016-0549-1