
Abstract
Background
Evidence is mounting to suggest a causal relationship between the built environment and people’s physical activity behaviours, particularly active transport. The evidence base has been hindered to date by restricted consideration of cost and economic factors associated with built environment interventions, investigation of socioeconomic or ethnic differences in intervention effects, and an inability to isolate the effect of the built environment from other intervention types. The aims of this systematic review were to identify which environmental interventions increase physical activity in residents at the local level, and to build on the evidence base by considering intervention cost, and the differential effects of interventions by ethnicity and socioeconomic status.
Methods
A systematic database search was conducted in June 2015. Articles were eligible if they reported a quantitative empirical study (natural experiment or a prospective, retrospective, experimental, or longitudinal research) investigating the relationship between objectively measured built environment feature(s) and physical activity and/or travel behaviours in children or adults. Quality assessment was conducted and data on intervention cost and whether the effect of the built environment differed by ethnicity or socioeconomic status were extracted.
Results
Twenty-eight studies were included in the review. Findings showed a positive effect of walkability components, provision of quality parks and playgrounds, and installation of or improvements in active transport infrastructure on active transport, physical activity, and visits or use of settings. There was some indication that infrastructure improvements may predominantly benefit socioeconomically advantaged groups. Studies were commonly limited by selection bias and insufficient controlling for confounders. Heterogeneity in study design and reporting limited comparability across studies or any clear conclusions to be made regarding intervention cost.
Conclusions
Improving neighbourhood walkability, quality of parks and playgrounds, and providing adequate active transport infrastructure is likely to generate positive impacts on activity in children and adults. The possibility that the benefits of infrastructure improvements may be inequitably distributed requires further investigation. Opportunities to improve the quality of evidence exist, including strategies to improve response rates and representativeness, use of valid and reliable measurement tools, cost-benefit analyses, and adequate controlling for confounders.
Similar content being viewed by others


Background
Physical activity is fundamental to human health and wellbeing [1]. Insufficient physical activity is a major contributor to the occurrence of non-communicable diseases and is responsible for about 9% of premature mortality globally [2, 3]. Increasing focus is being placed on the role of the built environment in promoting physical activity, recognising the sustained nature and potential for broad reach of environmental interventions, and the potential to promote substantial changes in population-level physical activity [4]. Active transport also contributes to health-promoting levels of physical activity [5, 6]. In addition, replacing motorised trips with active forms of transportation also brings numerous co-benefits, such as reduced traffic congestion; improved air quality; and reduced fatalities due to traffic, air pollution, and inactivity [7,8,9]. Accordingly walking and cycling for transport are particular behaviours of interest for researchers and policy-makers alike.
A growing body of evidence shows clear associations between the neighbourhood built environment and physical activity behaviours [10, 11]. Specifically, systematic reviews of the literature have shown that environments characterised as more walkable (i.e., facilitating walking through higher destination accessibility, street connectivity, presence and quality of active transport infrastructure, etc.) are associated with physical activity accumulation for both children and adults [12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27].
McCormack et al. [12] systematically examined the relationship between physical activity and objectively-assessed built environment, improving on earlier reviews by only including cross-sectional studies that adjusted for self-selection, and quasi-experiments. Findings showed land use mix, connectivity and population density and overall neighbourhood design (i.e., walkability, neighbourhood type) were “important determinants of physical activity”. Similarly, Mayne et al. [14] systematically examined the impact of natural or quasi-experimental studies of built environment changes on physical activity. Findings showed greater impacts on physical activity of interventions that were designed to impact active transport. Stronger results were also reported in papers where specific activity constructs (e.g., walking or cycling, rather than total physical activity) were assessed.
Relationships may differ depending on the physical activity construct of interest (e.g., active transport, such as walking or cycling for transport, versus leisure time physical activity) and the type of intervention [12, 28, 29]. In particular, environmental features may be more closely related to active transportation than overall physical activity or recreational activity [12]. Indeed, reviews have consistently shown associations between active transport and built environments that are characterised as “walkable”, including aspects of active transport infrastructure [14, 16, 30, 31]. Less is known with regard to cycling. A systematic review showed cross-sectional associations between cycling and the presence of dedicated cycle routes or paths, separation of cycling from other traffic, high population density, short trip distance, and proximity of a cycle path or green space [18]. For children, an association has been demonstrated between cycling and the promotion of ‘safe routes to school’ [18]. Negative environmental factors were traffic danger, long trip distance, steep inclines and distance from cycle paths. This review also demonstrated some evidence for causality with statistically significant impacts of new cycle routes on cycling prevalence from a limited number of studies [18]. Similarly in their systematic review, Yang et al. [19] observed modest increases in cycling associated with high quality cycling infrastructure improvements.
Relationships may also differ by population group (e.g., children, adults) [15]. Associations for children seem more complex than for adults, with inconsistencies in relationships observed [32], although this may in part be due to the limited evidence base. In their systematic review and meta-analysis of built environments and physical activity in children and youth, McGrath et al. [15] reported adolescents’ physical activity was positively associated with walkability features, play facilities, parks and playgrounds, but these relationships were negative for younger children. Even less is known with regard to older adults, though one systematic review of quantitative and qualitative research reported environmental associates of physical activity in this population, including street lighting, destination accessibility, and pedestrian infrastructure [22].
The quality of the built environment may be an important contributor to health inequalities, especially by influencing opportunities for active transport. To the authors’ knowledge, only one systematic review published to date has considered the impact that sociodemographic factors may have on the efficacy of built environment interventions [25]. In their systematic review, Schüle et al. [25] included only studies that simultaneously considered at least one indicator of “neighbourhood socioeconomic position” (e.g., socioeconomic status, SES) and adjustment for at least one individual socioeconomic factor (ethnicity alone was not considered sufficient) in multilevel modelling of the relationship between the built environment and health outcomes. Almost all the studies in this review showed interactions between “neighbourhood socioeconomic position” and the built environment or individual characteristics, or between the built environment and individual characteristics (including “individual socioeconomic position”). However, substantial heterogeneity in study design and reporting of results hindered any ability to generate clear insights. Hopgood et al. [33] found that traffic calming intensity was more common around less deprived schools in Auckland, New Zealand, whereas Zhu et al. [34] found that schools in Austin, Texas with higher proportions of poor or Hispanic students had better sidewalks and walkability. Interventions to improve the built environment may also have important effects on health equity, for example, improved infrastructure may be used more often by residents with a higher educational or income level [35].
Transport infrastructure is expensive but given the substantial economic burden caused by physical inactivity [3], built environment interventions that help people get active and stay active may be attractive options from a cost-benefit perspective. In terms of benefit:cost ratios, active transport interventions tend to compare well to other major transport investments, such as new roads or public transport [36, 37]. Studies in this field use a range of methodologies and processes to describe and evaluate infrastructural interventions and to model economic outcomes. Even so, findings from a 2008 systematic review reported large positive benefit:cost ratios for walking and cycling infrastructure interventions, with median magnitudes of 5:1 [24]. An updated systematic review reported benefit:cost ratios ranging between −39:1 to 59:1, with positive ratios reported by 26 of the 32 studies included (81%) [27]. More information is needed about specific infrastructural factors at a local level to guide specific investment and planning decisions.
Often, changes in the built environment, experienced either by changing residential location or by intervention in a familiar setting, do not occur in isolation. For example, infrastructural interventions may have associated social media campaigns or supplementary programmes to support behaviour change [38]. It is challenging, yet important, to tease out the effect of built environment changes on physical activity behaviours to enable effective decision making for planning and resourcing environmental change interventions. In one systematic review all included studies that combined built environment and physical activity promotion interventions were reported as being effective in increasing activity, while only half of the built environment intervention only studies showed a positive impact on activity [13]. Only one study in this review was concerned solely with physical activity promotion, limiting comparability between the intervention types.
Notwithstanding frequent calls for research to understand causality [19, 21, 28, 39], until recently, the evidence base has remained predominantly cross-sectional. Likewise, despite calls for studies to improve specificity by examining behaviour-specific environmental attributes and improve objectivity in environmental measures [19, 39], numerous gaps still remain. The lack of evidence has been attributed to gaps in collaboration between disciplines (e.g., research, urban planning) [40], cost of conducting quality research [41], and complexities in evaluating interventions [42] and modelling their effectiveness across population groups [43]. These are substantial barriers, but there has recently been an increase in studies utilising objective and behaviour-specific measures where causality can be inferred (e.g., longitudinal studies, controlled trials).
Some of the difficulties faced in assessing this broad evidence base include variable study quality, insufficient (or no) quality assessment of articles included in reviews [41], a narrow focus on specific population groups or behaviours of interest (restricting understanding from a broader population health perspective), and the predominance of cross-sectional studies (reducing ability to understand causality). There is a dearth of systematic reviews that: (a) consider cost and economic factors associated with built environment interventions, (b) describe socioeconomic or ethnic differences in intervention effects, or (c) where the ability to isolate the effect of the built environment from other intervention types is assessed.
For these reasons, we believe it is timely to re-examine the evidence base, with a focus on updating and improving on previous reviews, by: (1) only including studies where causality can be implied, (2) considering intervention cost, (3) examining whether intervention effects differ by ethnicity or SES, (4) conducting rigorous article quality assessment, (5) including all age groups and physical activity behaviours, and (6) attempting to isolate the effect of the built environment from other interventions occurring in studies. Our aims are to: (1) conduct a new systematic review to identify which environmental interventions increase physical activity in residents at the local level, with the goal of informing future policy and practice in community design; and (2) to build on the limited evidence base on the effectiveness of built environment interventions for influencing health inequalities by systematically exploring the effectiveness of these interventions by ethnicity and SES.
Methods
The review protocol was prepared following the PROSPERO International prospective register of systematic reviews protocols [https://www.crd.york.ac.uk/prospero/] and published on figshare [44].
Eligibility criteria
Articles were eligible if they reported a quantitative empirical study (natural experiment or a prospective, retrospective, experimental, or longitudinal research (including repeated cross-sectional surveys)) investigating the relationship between objectively measured built environment feature(s) and physical activity and/or travel behaviours in children or adults. Qualitative studies, or those that did not measure change in both the independent and dependent variables were excluded. For trials, no control group was required for the study to be included in the review.
Information sources
A systematic search of Scopus, Ovid (all journals), ProQuest Science, ProQuest Social Science, and the Transport Research International Documentation database (comprising the US Transportation Research Board’s Transport Research Information Services database and the Organisation for Economic Co-operation and Development Joint Transport Research Centre’s International Transport Research Documentation database), was conducted by the lead author (MS) in June 2015. Databases were identified in consultation with a subject-specific librarian, and the wider research team comprising specialists in transport, built environments, physical activity, active transport, epidemiology, and health. We acknowledge the value of grey literature in some circumstances but did not include studies reported in this form in this study. We sought the most robust evidence available, ensuring our methods were as robust and replicable as possible [45], and reducing the risk of bias in outcome reporting that may occur in the grey literature, for instance in settings where funding for infrastructural work is at stake. Bibliographies of included articles were also searched for possible relevant articles (using the article title).
Search strategy
Keyword searches of article abstracts and titles were conducted using three categories: 1) environments, 2) physical activity or travel modes, and 3) natural experiments, or prospective, retrospective, experimental, or longitudinal. Search terms were identified from MeSH subject headings in PubMed, previous similar reviews [5, 12, 46], and the knowledge and expertise of the research team. Test searches were conducted to gauge the sensitivity and specificity of the search terms, and amendments were made accordingly. Searches were limited to English-language articles that were published or in press, with no date restrictions. The final search strategy is outlined in Additional file 1.
Study selection
Titles and abstracts of articles were screened by the lead author and included if they met the eligibility criteria. Where it was unclear whether articles met the inclusion and exclusion criteria from the abstract and title, full-text articles were sourced. Where bibliography searches identified article titles as possibly relevant, article abstracts were sourced and screened using the above criteria. All processes (i.e., identification of articles, data extraction, quality assessment) were duplicated by a co-author (JH) with a random selection of 10% of each dataset [47, 48]. Any disagreement was resolved through discussion, and any necessary amendments made to each process.
For the purposes of this examination, a relatively broad definition of built environment was used, with the aim of identifying and understanding the range of modifiable factors in the external neighbourhood environment that may impact people’s physical activity or travel behaviours. Accordingly, ‘built environment’ encompassed either interventions or changes occurring at the individual level (e.g., due to moving), or at the local, neighbourhood, or town scale. Measures were all objective and included geographic information systems-derived variables (e.g., dwelling density, distance to destinations), community infrastructural or streetscape intervention typologies (e.g., shared spaces, naked streets), natural or built aesthetic factors in the neighbourhood environment (e.g., tree planting, signage, wayfinding), and measures of other relevant environmental supports for physical activity or active travel (e.g., playground features). Recognising the contribution that public transport use can make to physical activity accumulation [49, 50], studies assessing changes in access to public transport (e.g., distance to closest public transport stop, park-and-ride interventions) were also eligible. As the focus was on being able to isolate the effect of built environment features or interventions, studies investigating aggregate measures (e.g., walkability, walk score), or studies combining infrastructural and “soft” (e.g., awareness programmes, social media, organised programmes) interventions where the effect of the infrastructural intervention could not be isolated were not included. Conversely, studies that included infrastructural and soft interventions but where findings enabled the effect of the infrastructural intervention to be isolated were included.
Likewise, a broad approach was taken to defining physical activity for this review – encompassing all types and dimensions of self-reported or objectively assessed physical activity (e.g., recreational walking, habitual physical activity, moderate-to-vigorous physical activity). Physical activity could be assessed retrospectively, prospectively, using repeated cross-sectional surveys or direct observation, or before and after an intervention. While acknowledging the limitations of recall, well-designed retrospective studies offer a “plausible alternative to prospective longitudinal data collection” [51] due to time efficiency, lack of panel attrition, cost effectiveness, and quality of survey instruments (as earlier measures may be obsolete).
Data extraction and quality assessment
A study-specific data extraction form (available in Additional file 2) was generated from a previous systematic review of health impacts of new roads [52] and the Effective Practice and Organisation of Care data collection form [53]. Data were extracted for all included articles across seven categories: general information, population and setting, methods, participants, intervention groups, outcome measures, and results. In addition, data were extracted on whether the effect of the built environment differed by ethnicity or SES. Studies were eligible for the latter if they reported effect estimates stratified by ethnicity or SES, or examined effect modification/interactions between the intervention or exposure variable and ethnicity or SES. Eligible measures of ethnicity included self-reported or objectively assigned ethnicity or race. Eligible measures of SES included income, educational level, occupation and home ownership, as well as composite indices such as those for deprivation. SES could be measured at an individual or area level. Area-level SES measures were only eligible if the SES variable was calculated for a smaller area than the study/intervention area (e.g., meshblock-level deprivation [54] calculated in a community-wide project that included multiple meshblocks).
Strength of evidence was determined using the Evaluation of Public Health Practice Projects Quality Assessment Tool (EPHPP) as employed in previous similar reviews [5, 46], and adapted to improve the suitability for assessing articles included in this review [46] as outlined in Additional file 3. EPHPP scoring criteria are provided in Additional file 4. Adaptations were made as a consequence of the duplicate quality assessment process whereby the reviewers identified a number of necessary clarifications to facilitate consistency in scoring. These changes did not impact the final quality assessment scores.
Summary measures, synthesis of results and quality assessment/risk of bias across studies
The key outcomes of interest were physical activity (self-reported, observed, or objectively assessed), active transport (self-reported or observed), and visitation to or use of a setting (e.g., counts of riders on new cycleways; counts of playground users). Findings were collated for each of these outcome measures and considered separately by population subgroups (children, adults). Findings were also summarised in the context of study quality to gauge risk of bias and understand the strength of evidence provided.
Results
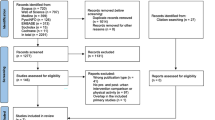
Figure 1 provides the flow diagram of articles included and excluded from the review [55]. Of the 12,082 articles identified, 2282 were duplicates, 9757 were excluded at title or abstract stage, and 43 were assessed at full text stage. In total, 28 articles met the inclusion criteria for this review.

Pathway of articles included and excluded in review
Study characteristics
Key characteristics of studies included are provided in Table 1. The majority of studies were controlled repeat cross-sectional examinations (n = 8), followed by uncontrolled repeat cross-sectional studies and uncontrolled longitudinal studies (both n = 6). Almost three-quarters (71%) of studies were conducted in the USA, with the remainder from Australia (n = 4), and Belgium, England, Scotland, and New Zealand (all n = 1). A majority of studies focused on all age groups (n = 13) or adults only (n = 12). Three (11%) focused on children and no studies focused specifically on older adults. Intervention types varied widely, but predominantly involved infrastructural interventions for facilitating walking and cycling (e.g., bicycle boulevards, installation of cycle lanes, improving sidewalks, etc.). Park and playground improvements or development also featured regularly. Walking for leisure or transport was assessed in seven studies, cycling in two, and overall active transport in six studies. Where observation of active transport occurred, two studies directly observed cyclist counts only, and two undertook counts of pedestrians and cyclists.
Quality assessment
Study quality assessment results are provided in Table 2. Using the EPHPP criteria, only one study was rated as strong (i.e., having no components with a weak rating), and a majority (75%) were rated as weak. No studies rated as moderate or strong assessed walking or cycling separately from each other. Selection bias was the quality component most frequently rated as weak. In many cases this was a consequence of undertaking direct observation of park users, where no measures of representativeness could be ascertained. In general, studies lacked robust means of ensuring generalisability. The use of direct observation made it difficult to fully control for confounders. Relevant information on traffic and street type was also frequently missing in studies that assessed the effectiveness of streetscape interventions. Of the studies where it was appropriate (i.e., where there was a control/comparison group or site), 28% reported on consistency between treatment conditions. Five studies noted distance between treatment sites, but no studies measured contamination directly. Cost of the intervention was reported in seven studies, all of which were conducted in the US. These ranged from US$45,000 per park for implementation of fitness zones to US$5.5 million for two major playfield renovations.
Differential effects by ethnicity or socio-economic status
Four studies investigated whether built environment effects differed by ethnicity/race or SES, using a range of different approaches. The iConnect CBA study of new walking and cycling routes in three UK municipalities over two years found no significant interaction between the intervention and education, income or employment when using walking and cycling as the outcome [56]. When examining use of the infrastructure, lower educational level and income, but not ethnicity, were associated with less use. Compared with an annual income of >£40,000, an income of <£20,000 was associated with a 23% lower likelihood of infrastructure use. Having less than tertiary-level educational level, compared with tertiary education, was associated with a 10–20% lower likelihood of infrastructure use, though the effect was only statistically significant at one-year (not two-year) follow-up. People who were not working, who were retired or were students (compared with working people) were less likely to use the infrastructure at two-year follow-up. Students were particularly unlikely to use the infrastructure (relative ratio = 0.20) [35].
A randomized controlled trial of the effects of Los Angeles park improvements informed by community engagement found a significant increase in the number of white park users, but no significant changes for black, Hispanic or other users [57]. Installation of a one-mile bike lane in New Orleans was associated with increases in mean daily cycling counts on the intervention street for both whites (from 48.9 to 192.9/day) and blacks (from 22.8 to 61.3/day; results for other racial/ethnic groups not reported), while cycle counts on adjacent control streets dropped post-intervention. The interaction of intervention, time and race/ethnicity was not statistically significant [58]. In a longitudinal study across several US cities, the effect of change in neighbourhood recreational facility density on change in recreational physical activity (mean follow-up 3.2 years) did not differ significantly by income or race/ethnicity [59].
Impact of built environment on physical activity, active transport, or visitation/use of settings
Table 3 summarises the key findings in relation to the impact of the built environment on physical activity, active transport, and visits or use of settings. With the exception of two studies showing no significant impact [60, 61], and one finding a negative impact [62], all others reported a significant positive impact on the outcomes of interest. For those studies rated higher quality (i.e., moderate or strong ranking using the EPHPP criteria), significant positive impacts were found for the following:
-
Interventions involving multiple streetscape improvements on active transport in children, and on physical activity in adults [63, 64]
-
Installation of park or playground equipment and active transport and physical activity in adults [57, 63]
-
Multiple component park renovations on children’s physical activity (for children of lower body size only) [65]
-
Temporary road closures and provision of play equipment on children’s physical activity [66]
-
Increased density of recreation facilities in the neighbourhood on physical activity in adults [59]
Discussion
The aims of this systematic review were to provide an update on the evidence for the impact of the built environment on physical activity behaviours, and to systematically explore the effectiveness of these interventions by ethnicity and SES. Drawing from best practice, we took a systematic approach to identifying and screening literature, data extraction, and quality assessment of relevant literature.
Findings showed a consistent positive effect of walkability components, provision of quality parks and playgrounds, and installation of or improvements in active transport infrastructure on active transport, physical activity, and visits or use of settings. Impacts on activity dimensions were observed in line with expectations (e.g., walkability components were related to active transport) [14]. Additionally, some interesting patterns emerged whereby improvements in non-specific activity dimensions occurred, such as installation of fitness or playground equipment increasing active transport to that setting, and improving the streetscape for walking and cycling increasing physical activity behaviours beyond active transport. Positive impacts were observed for children and adults alike, although there was a paucity of research including older adults. Taken together, these findings provide new evidence for the substantial promise that built environment interventions hold for improving physical activity behaviours across a population and are in keeping with previous systematic reviews [12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27]. There remains a substantial gap in understanding relationships with cycling behaviours. None of the studies rated as strong or moderate quality assessed cycling independently of other active transport modes.
Most analyses found no statistically significant differences in intervention effect by ethnicity or SES. However, one study found that new walking and cycling routes were used more by people with higher incomes, higher educational level and by people who were currently employed. Another study of park improvements found increased number of white users, but no significant change for black, Hispanic or other park users. Although these two studies provide a limited basis from which to draw inferences, the possibility that infrastructure improvements may predominantly benefit socioeconomically advantaged groups warrants further exploration in future evaluations.
As identified in previous reviews, there was substantial variability in the methodology, measures, and analytical processes used to evaluate the impact of environmental interventions. Overall, this made comparisons between studies and intervention delivery approaches difficult. In part, this variability may be a by-product of the significant differences in intervention typologies and associated research designs. There remains, however, a need for improved study quality, which may mitigate this somewhat (e.g., consistent application of objective assessment of physical activity, including appropriate control conditions, employment of strategies to improve response rates, adequate consideration of confounders, etc.). Our quality assessment rated three-quarters of included studies as weak. Studies were frequently limited by lack of representativeness and generalisability.
In most cases, blinding was not described in studies. Following the scoring protocol of the EPHPP, this earned a “Moderate” rating. It is worth noting there are ethical issues to be considered with participant blinding (such as informed consent), and that these can sometimes conflict with quality assessment criteria, where blinding is desirable to reduce bias associated with participant self-report or reactivity [67]. We chose to retain this category for consistency with the EPHPP and previous research that has used this tool. An indepth consideration of the issues surrounding the evaluation of blinding in quality assessment is beyond the scope of this review, but should be taken into account in future reviews in this field.
Few studies comprehensively controlled for confounders. While sex and age were commonly controlled or stratified for in analyses, only some included robust measures of SES or ethnicity. Depending on study design, area-level SES (and ethnicity characteristics) may suffice in order to mitigate challenges around collecting these data at the individual level. In their systematic review, Schule et al. [25] recommended the use of comparable characteristics of neighbourhood-level SES in studies of the built environment, recognising the need to “disentangle health impacts and identify vulnerable neighbourhoods and population groups”.
Issues around contamination and consistency across intervention sites were rarely considered and were not controlled for in any analyses. Future studies would also benefit from considering neighbourhood self-selection as a possible confounder. In their systematic review, McCormack et al. [12] reported “an attenuation in associations between built environment characteristics and physical activity after accounting for neighbourhood self-selection”. Likewise, baseline activity was rarely controlled for in analyses. One recent study to consider this factor revealed that existing cycling behaviour, as well as distance to the intervention site, was associated with increased use of a new bike path in Australian adults [68].
Overall, there was a lack of research specific to children or older adults. It is possible that the adult-centric approach to characterising built environments may not be sufficiently capturing environments that matter to younger populations. For example, in their earlier review, Sugiyama et al. [29] found no link between route safety and traffic features and adults’ utilitarian and recreational walking, while these factors have previously been linked with children’s active transport [32]. A recent systematic review showed that where youth physical activity was geo-located (i.e., with global positioning systems devices and geographic information systems), greater proportions of activity took place in streets and urban venues than in green spaces [15].
In keeping with Hunter et al. [13], reporting of intervention costs was uncommon in the studies included in this review. The lack of clear and consistent reporting of intervention cost limited any ability to determine whether a relationship existed between expenditure and behaviour change, and whether costs differed significantly between intervention types. This may also lead to bias in studies of benefit:cost analyses for built environment interventions because only a small portion of evidence is presented, and it is not clear why some studies report costs and other don’t [24, 27]. Moreover, the low quality of evidence found overall negatively impacts confidence in estimations of cost-effectiveness of built environment interventions [41]. Given that the costs of included interventions varied widely (ranging from USD45,000 to USD5.5 million in the current study), it is essential that clear reporting of intervention costs occurs, and that intervention studies also include a cost-benefit component.
Compared with infrastructural interventions, relocation studies are less hindered by infrastructural cost. RESIDE is perhaps the first study of its kind – a natural experiment involving longitudinal data collection with new residents of new housing developments [69]. The study commenced in 2003 prior to participants moving, with follow-up data collection occurring with participants approximately 12 months after their baseline (pre-moving) survey. Improvements in walkability (specifically, objectively-assessed destination accessibility, residential density, street connectivity, and access to/availability of public transit) were associated with increases in physical activity and use of active transport [69,70,71]. This important study demonstrates the value of well-designed residential relocation studies.
The substantial inconsistency in timing and number of follow-up measures post exposure (i.e., through intervention or moving) limits a clear understanding of the impact of the built environment on physical activity. In their systematic review of natural or quasi-experiments, Mayne et al. [14] found that stronger impacts on physical activity were found where studies included longer follow-up times. This phenomenon was observed in the iConnect study, in which no effect on behaviour was observed one year after a major environmental intervention, but significant changes were found at the two-year follow-up [56]. Pragmatic and economic factors may limit the feasibility of repeated and longer-term follow-up periods in this research field, but where possible this should be encouraged.
Finally, it is possible that publication bias affected the balance of studies included in this review. In general, registration or public release in other forms of study protocols prior to the publication of findings provides a check on selective reporting of study results.
Strengths and limitations
This systematic review focused on physical activity behaviours and use or visitation of settings, and did not include more distal health measures such as body size [72]. While these outcomes are unquestionably important, this approach was taken recognising that: (a) a substantial period of time exists between sustained activity behaviours and manifestation of associated health outcomes, and (b) studies in this field rarely examine effects of the built environment on activity behaviours for a sufficient period of time to expect meaningful changes in health outcomes that are downstream from improved physical activity behaviours.
The broad inclusion criteria used here are a strength, drawing on studies across all quality assessment categories as well as considering findings in light of study quality. However, the exclusion of grey literature could have been a limiting factor, in that it is possible that significant new lines of inquiry might have been overlooked.
While acknowledging the important role of perceptions on the relationship between the built environment and activity behaviours [73, 74], this review focused only on objectively assessed built environment features. The association between the built environment and activity varies, depending on whether perceived or objective measures are used [73, 75,76,77]. Moreover these differences are not consistent, and vary along with individual factors such as education level, income, body size, and physical activity [74, 78]. Individuals who are more physically active may be more familiar with their local environment, and more aware of both positive and negative features, than those who are less active [79]. In the interest of providing clear and direct information to inform policy and practice that was not complicated or hindered by individual perceptions, we chose to focus on objective measures of the environment. Future reviews may consider replicating the current study with a focus on perceived environmental features only, while others may undertake the task of considering both objective and subjectively-assessed environments. There is an emerging body of research that simultaneously considers both objective and subjective measures of the environment in relation to physical activity [76]; offering challenges and opportunities for future reviews in this area.
Our focus was on being able to isolate the effect of specific built environment features or interventions, thus studies that employed aggregate measures (e.g., neighbourhood walkbability) were excluded from this review. A range of robust studies exist in the field that have utilized aggregate measures [80, 81]. The exclusion of this research limits an understanding of the combination of features that encompass a pedestrian or cyclist friendly environment. However, this approach was taken in the interest of generating specific findings that could be translated into policy and practice. Measures that combine variables may be difficult to interpret, if it is not possible to determine which components are most effective. Future reviews with differing aims could consider including aggregate scores, and might extend this to broader aggregate concepts such as obesogenic environments [82].
There have been calls for more systematic approaches in reviews in this field [83]. This study employed robust systematic procedures following best practice, and improved on existing reviews by conducting quality assessment of articles, considering article quality when summarising results, including literature for children and adults, excluding cross-sectional studies, and attempting to isolate the effect of the built environment from other interventions occurring in studies. With the intent of providing evidence from the most robust evidence possible and undertaking a process that was as replicable as possible, as well as drawing from existing high quality reviews in this field [12, 14, 16, 30, 31, 46], this review did not include grey literature or involve forwards citation searches. Future reviews may undertake these processes to capture an evidence base that is as broad and up-to-date as possible [45, 84]. Although our global quality assessment score does not include measures of study contamination, consistency, health equity, or intervention cost, these factors were systematically considered and presented in the context of understanding the overall quality of studies presented in this review.
Conclusion
The systematic and comprehensive approach to examining study quality and contextualising findings in light of study quality in this review adds strength to the evidence base for the positive impact of built environments on physical activity behaviours, active transport, and visits to/use of activity settings. Improving neighbourhood walkability, quality of parks and playgrounds, and providing adequate active transport infrastructure is likely to generate positive impacts on activity in children and adults. Specifically, findings from the current review suggest that the following show promise for increasing active transport and physical activity levels in children and adults: multiple streetscape components for walking or cycling (including two or more of: crosswalk and sidewalk improvements, improved and covered bike parking, installation of traffic calming features (raised platforms, zebra crossings) and parking bays; creating safe places to walk); bike boulevard/lane installation; new greenways; traffic free bridges and boardwalks; installation of fitness/playground equipment; multiple park renovations (including two or more of: new equipment, walking tracks, fencing, landscaping, surfaces, lights); removal of park/playground seating; retrofitting existing spaces into pocket parks; temporary road closures and play equipment; access to and availability of public transport; higher residential, destination, and recreation density; increased street connectivity; and increased land use mix. The strongest evidence existed for multiple streetscape components (adult PA, child AT), installation of fitness equipment (adult PA and AT), temporary road closures and play equipment (child PA), and recreation facility density (adult PA).
Numerous limitations in the evidence base exist. In particular, the possibility that the benefits of infrastructure improvements may be inequitably distributed requires further investigation. Notwithstanding the significant challenges in terms of research design, many opportunities to improve the quality of evidence are clear, including strategies to improve response rates and representativeness, use of valid and reliable measurement tools, cost-benefit analyses, and adequate controlling for confounders.
Abbreviations
- EPHPP:
-
Evaluation of Public Health Practice Projects Quality Assessment Tool
- SES:
-
Socioeconomic status
- UK:
-
United Kingdom
- US:
-
United States
- USD:
-
United States dollars
References
World Health Organization. Global recommendations on physical activity for health. Geneva; 2010.
Lee I-M, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Lancet physical activity series working group: effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380:219–29.
Ding D, Lawson KD, Kolbe-Alexander TL, Finkelstein EA, Katzmarzyk PT, van Mechelen W, Pratt M. Lancet physical activity series 2 executive C: the economic burden of physical inactivity: a global analysis of major non-communicable diseases. Lancet. 2016;388:1311–24.
Sallis JF, Floyd MF, Rodriguez DA, Saelens BE. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation. 2012;125:729–37.
Saunders LE, Green JM, Petticrew MP, Steinbach R, Roberts H. What are the health benefits of active travel? A systematic review of trials and cohort studies. PLoS One. 2013;8:e69912.
Oliver M, Parker K, Witten K, Mavoa S, Badland H, Donovan P, Chaudhury M, Kearns RA. Children’s out-of-school independently mobile trips, active travel, and physical activity: a cross-sectional examination from the kids in the City study. JPAH. 2016;13:318–24.
Rojas-Rueda D, de Nazelle A, Andersen ZJ, Braun-Fahrlander C, Bruha J, Bruhova-Foltynova H, Desqueyroux H, Praznoczy C, Ragettli MS, Tainio M, Nieuwenhuijsen MJ. Health impacts of active transportation in Europe. PLoS One. 2016;11:e0149990.
Xia T, Zhang Y, Crabb S, Shah P. Cobenefits of replacing car trips with alternative transportation: a review of evidence and methodological issues. J Environ Public Health. 2013;2013:797312.
Lindsay G, Macmillan A, Woodward A. Moving urban trips from cars to bicycles: impact on health and emissions. Moving urban trips from cars to bicycles: impact on health and emissions. 2011;35:54–60.
Giles-Corti B, Kelty S, Zubrick S, Villanueva K. Encouraging walking for transport and physical activity in children and adolescents: how important is the built environment? Sports Med. 2009;39:995–1009.
Sallis JF, Cerin E, Conway TL, Adams MA, Frank LD, Pratt M, Salvo D, Schipperijn J, Smith G, Cain KL, et al. Physical activity in relation to urban environments in 14 cities worldwide: a cross-sectional study. Physical activity in relation to urban environments in 14 cities worldwide: a cross-sectional study. 2016. Online First.
McCormack GR, Shiell A. Search of causality: a systematic review of the relationship between the built environment and physical activity among adults. Int J Behav Nutr Phys Act. 2011;8:125.
Hunter RF, Christian H, Veitch J, Astell-Burt T, Hipp JA, Schipperijn J. The impact of interventions to promote physical activity in urban green space: a systematic review and recommendations for future research. Soc Sci Med. 2015;124:246–56.
Mayne SL, Auchincloss AH, Michael YL. Impact of policy and built environment changes on obesity-related outcomes: a systematic review of naturally occurring experiments. Obes Rev. 2015;16:362–75.
McGrath LJ, Hopkins WG, Hinckson EA. Associations of objectively measured built-environment attributes with youth moderate-vigorous physical activity: a systematic review and meta-analysis. Sports Med. 2015;45:841–65.
Grasser G, Van Dyck D, Titze S, Stronegger W. Objectively measured walkability and active transport and weight-related outcomes in adults: a systematic review. Int J Public Health. 2013;58:615–25.
Durand CP, Andalib M, Dunton GF, Wolch J, Pentz MA. A systematic review of built environment factors related to physical activity and obesity risk: implications for smart growth urban planning. Obes Rev. 2011;12:e173–82.
Fraser SD, Lock K. Cycling for transport and public health: a systematic review of the effect of the environment on cycling. Eur J Pub Health. 2011;21:738–43.
Yang L, Sahlqvist S, McMinn A, Griffin SJ, Ogilvie D. Interventions to promote cycling: systematic review. BMJ. 2010;341:c5293.
Casagrande SS, Whitt-Glover MC, Lancaster KJ, Odoms-Young AM, Gary TL. Built environment and health behaviors among African Americans: a systematic review. Am J Prev Med. 2009;36:174–81.
Wendel-Vos W, Droomers M, Kremers S, Brug J, van Lenthe F. Potential environmental determinants of physical activity in adults: a systematic review. Obes Rev. 2007;8:425–40.
Annear M, Keeling S, Wilkinson T, Cushman G, Gidlow B, Hopkins H. Environmental influences on healthy and active ageing: a systematic review. Ageing Soc. 2014;34:590–622.
Laine J, Kuvaja-Kollner V, Pietila E, Koivuneva M, Valtonen H, Kankaanpaa E. Cost-effectiveness of population-level physical activity interventions: a systematic review. Am J Health Promot. 2014;29:71–80.
Cavill N, Kahlmeier S, Rutter H, Racioppi F, Oja P. Economic analyses of transport infrastructure and policies including health effects related to cycling and walking: a systematic review. Transp Policy. 2008;15:291–304.
Schule SA, Bolte G. Interactive and independent associations between the socioeconomic and objective built environment on the neighbourhood level and individual health: a systematic review of multilevel studies. PLoS One. 2015;10:e0123456.
Oliveira AF, Moreira C, Abreu S, Mota J, Santos R. Environmental determinants of physical activity in children: a systematic review. Archives of Exercise in Health and Disease. 2014;4:254–61.
Brown V, Diomedi BZ, Moodie M, Veerman JL, Carter R. A systematic review of economic analyses of active transport interventions that include physical activity benefits. Transp Policy. 2016;45:190–208.
Owen N, Humpel N, Leslie E, Bauman A, Sallis JF. Understanding environmental influences on walking; review and research agenda. Am J Prev Med. 2004;27:67–76.
Sugiyama T, Neuhaus M, Cole R, Giles-Corti B, Owen N. Destination and route attributes associated with adults' walking: a review. Med Sci Sports Exerc. 2012;44:1275–86.
Saelens BE, Sallis JF, Frank LD. Environmental correlates of walking and cycling: findings from the transportation, urban design, and planning literatures. Ann Behav Med. 2003;25:80–91.
Saelens BE, Handy SL. Built environment correlates of walking: a review. Med Sci Sports Exerc. 2008;40:S550–S66.
Oliver M, Mavoa S, Badland H, Parker K, Donovan P, Kearns RA, Lin E-Y, Witten K. Associations between the neighbourhood built environment and out of school physical activity and active travel: an examination from the kids in the City study. Health & Place. 2015;36:57–64.
Hopgood T, Percival T, Stewart J, Ameratunga S. A tale of two cities: paradoxical intensity of traffic calming around Auckland schools. N Z Med J. 2013;126:22–8.
Zhu X, Lee C. Walkability and safety around elementary schools. Economic and ethnic disparities. Am J Prev Med. 2008;34:282–90.
Goodman A, Sahlqvist S, Ogilvie D. iConnect c: who uses new walking and cycling infrastructure and how? Longitudinal results from the UK iConnect study. Prev Med. 2013;57:518–24.
Macmillan A, Connor J, Witten K, Kearns R, Rees D, Woodward A. The societal costs and benefits of commuter bicycling: simulating the effects of specific policies using system dynamics modeling. The societal costs and benefits of commuter bicycling: simulating the effects of specific policies using system dynamics modeling. 2014;122:335–44.
Davis A: Value for money: an economic assessment of Investment in Walking and Cycling. United Kingdom; 2010.
Pucher J, Dill J, Handy S. Infrastructure, programs, and policies to increase bicycling: an international review. Prev Med. 2010;50(Suppl 1):S106–25.
McCormack G, Giles-Corti B, Lange A, Smith T, Martin K, Pikora TJ. An update of recent evidence of the relationship between objective and self-report measures of the physical enviornment and physical activity behaviours. An update of recent evidence of the relationship between objective and self-report measures of the physical enviornment and physical activity behaviours. 2004;7:81–91.
Glanz K, Handy S, Henderson KE, Slater SJ, Davis EL, Powell LM. Built environment assessment: multidisciplinary perspectives. SSM - Population Health. 2016;2:24–31.
Benton JS, Anderson J, Hunter RF, French DP. The effect of changing the built environment on physical activity: a quantitative review of the risk of bias in natural experiments. Int J Behav Nutr Phy. 2016;13
Coghill CL, Valaitis RK, Eyles JD. Built environment interventions aimed at improving physical activity levels in rural Ontario health units: a descriptive qualitative study. BMC Public Health. 2015;15
Mehdipanah R, Manzano A, Borrell C, Malmusi D, Rodriguez-Sanz M, Greenhalgh J, Muntaner C, Pawson R. Exploring complex causal pathways between urban renewal, health and health inequality using a theory-driven realist approach. Soc Sci Med. 2015;124:266–74.
Smith M. Systematic Review Protocol. figshare. 2017. Retrieved September 26, 2017. https://doi.org/10.17608/k6.auckland.5445586.v1.
Godin K, Stapleton J, Kirkpatrick SI, Hanning RM, Leatherdale ST. Applying systematic review search methods to the grey literature: a case study examining guidelines for school-based breakfast programs in Canada. Syst Rev. 2015;4:138.
Chillón P, Evenson KR, Vaughn A, Ward DS. A systematic review of interventions for promoting active transportation to school. Int J Behav Nutr Phys Act. 2011;8 doi:10.1186/479–5868–8-10.
Moher D, Tetzlaff J, Tricco AC, Sampson M, Altman DG. Epidemiology and reporting characteristics of systematic reviews. PLoS Med. 2007;4:e78.
Page MJ, Shamseer L, Altman DG, Tetzlaff J, Sampson M, Tricco AC, Catala-Lopez F, Li L, Reid EK, Sarkis-Onofre R, Moher D. Epidemiology and reporting characteristics of systematic reviews of biomedical research: a cross-sectional study. PLoS Med. 2016;13:e1002028.
Rissel C, Curac N, Greenaway M, Bauman A. Physical activity associated with public transport use--a review and modelling of potential benefits. Int J Environ Res Public Health. 2012;9:2454–78.
Brown BB, Werner CM. A new rail stop: tracking moderate physical activity bouts and ridership. Am J Prev Med. 2007;33:306–9.
Mayer KU. Retrospective longitudinal research: the German life history study. In: Handbook of Longitudinal Research: Design, Measurement, and Analysis. Edited by Menard S. Burlington, MA: Elsevier; 2008. p. 85–106.
Egan M, Petticrew M, Hamilton V, Ogilvie D. Health impacts of new roads: a systematic review. Am J Public Health. 2003;93:1463–71.
Data collection form. EPOC Resources for review authors. http://epoc.cochrane.org/epoc-specific-resources-review-authors.
Salmond CE, Crampton P. Development of New Zealand’s deprivation index (NZDep) and its uptake as a national policy tool. Can J Public Health. 2012;103:S7–S11.
Moher D, Liberati A, Tetzlaff J, Altman DG. The PRISMA group: preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi:10.1371/journal.pmed.
Goodman A, Sahlqvist S, Ogilvie D. New walking and cycling routes and increased physical activity: one- and 2-year findings from the UK iConnect study. Am J Public Health. 2014:e1–9.
Cohen D, Marsh T, Williamson S, Golinelli D, McKenzie TL. Impact and cost-effectiveness of family fitness zones: a natural experiment in urban public parks. Health Place. 2012;18:39–45.
Parker KM, Gustat J, Rice JC. Installation of bicycle lanes and increased ridership in an urban, mixed-income setting in New Orleans, Louisiana. J Phys Act Health. 2011;8(Suppl 1):S98–S102.
Ranchod YK, Roux AVD, Evenson KR, Sanchez BN, Moore K. Longitudinal associations between neighborhood recreational facilities and change in recreational physical activity in the multi-ethnic study of atherosclerosis, 2000-2007. Am J Epidemiol. 2014;179:335–43.
West ST, Shores KA. Does building a greenway promote physical activity among proximate residents? J Phys Act Health. 2015;12:52–7.
Clark S, Bungum T, Shan G, Meacham M, Coker L. The effect of a trail use intervention on urban trail use in southern Nevada. Prev Med. 2014;67:S17–20.
Dill J, McNeil N, Broach J, Ma L. Bicycle boulevards and changes in physical activity and active transportation: findings from a natural experiment. Prev Med. 2014;69(Suppl 1):S74–8.
Gustat J, Rice J, Parker KM, Becker AB, Farley TA. Effect of changes to the neighborhood built environment on physical activity in a low-income African American neighborhood. Prev Chronic Dis. 2012;9:E57.
McDonald NC, Yang YZ, Abbott SM, Bullock AN. Impact of the safe routes to school program on walking and biking: Eugene, Oregon study. Transp Policy. 2013;29:243–8.
Quigg R, Reeder AI, Gray A, Holt A, Waters D. The effectiveness of a community playground intervention. J Urban Health. 2012;89:171–84.
D'Haese S, Van Dyck D, De Bourdeaudhuij I, Deforche B, Cardon G. Organizing "play streets" during school vacations can increase physical activity and decrease sedentary time in children. Int J Behav Nutr Phys Act. 2015;12:14.
Boutron I, Guittet L, Estellat C, Moher D, Hrobjartsson A, Ravaud P. Reporting methods of blinding in randomized trials assessing nonpharmacological treatments. PLoS Med. 2007;4:e61.
Rissel C, Greaves S, Wen LM, Crane M, Standen C. Use of and short-term impacts of new cycling infrastructure in inner-Sydney, Australia: A quasi-experimental design. Int J Behav Nutr Phys Act. 2015;12:129.
Giles-Corti B, Bull F, Knuiman M, McCormack G, Van Niel K, Timperio A, Christian H, Foster S, Divitini M, Middleton N, Boruff B. The influence of urban design on neighbourhood walking following residential relocation: longitudinal results from the RESIDE study. Soc Sci Med. 2013;77:20–30.
Beenackers MA, Foster S, Kamphuis CB, Titze S, Divitini M, Knuiman M, van Lenthe FJ, Giles-Corti B. Taking up cycling after residential relocation: built environment factors. Am J Prev Med. 2012;42:610–5.
Knuiman MW, Christian HE, Divitini ML, Foster SA, Bull FC, Badland HM, Giles-Corti B. A longitudinal analysis of the influence of the neighborhood built environment on walking for transportation: the RESIDE study. Am J Epidemiol. 2014;180:453–61.
Chiu M, Rezai MR, Maclagan LC, Austin PC, Shah BR, Redelmeier DA, JV T. Moving to a highly walkable neighborhood and incidence of hypertension: a propensity-score matched cohort study. Environ Health Perspect. 2015;
Hoehner CM, Ramirez LKB, Elliott MB, Handy SL, Brownson RC. Perceived and objective environmental measures and physical activity among urban adults. Am J Prev Med. 2005;28:105–16.
Jauregui A, Salvo D, Lamadrid-Figueroa H, Hernandez B, Rivera-Dommarco JA, Pratt M. Perceived and objective measures of neighborhood environment for physical activity among Mexican adults, 2011. Prev Chronic Dis. 2016;13
Gebel K, Bauman AE, Sugiyama T, Owen N. Mismatch between perceived and objectively assessed neighborhood walkability attributes: prospective relationships with walking and weight gain. Health Place. 2011;17:519–24.
Hinckson E, Cerin E, Mavoa S, Oliver M, Badland H, Stewart T, Duncan S, Schofield G. Associations of the perceived and objective neighborhood environment with physical activity and sedentary time in New Zealand adolescents. Int J Behav Nutr Phys Act. in submission
Orstad SL, McDonough MH, Stapleton S, Altincekic C, Troped PJ. A systematic review of agreement between perceived and objective neighborhood environment measures and associations with physical activity outcomes. A systematic review of agreement between perceived and objective neighborhood environment measures and associations with physical activity outcomes. 2017;49:904–32.
Gebel K, Bauman A, Owen N. Correlates of non-concordance between perceived and objective measures of walkability. Ann Behav Med. 2009;37:228–38.
Adams MA, Ryan S, Kerr J, Sallis JF, Patrick K, Frank LD, Norman GJ. Validation of the neighborhood environment walkability scale (NEWS) items using geographic information systems. J Phys Act Health. 2009;6:S113–S23.
Krizek K. Pretest-posttest strategy for researching neighborhood-scale urban form and travel behavior. Trans Res Rec. 1722;2000:48–55.
Krizek KJ. Residential relocation and changes in urban travel: does neighborhood-scale urban form matter? JAPA. 2003;69:265–81.
Mackenbach JD, Rutter H, Compernolle S, Glonti K, Oppert J-M, Charreire H, De Bourdeaudhuij I, Brug J, Nijpels G, Lakerveld J. Obesogenic environments: a systematic review of the association between the physical environment and adult weight status, the SPOTLIGHT project. BMC Public Health. 2014;14:233.
Gebel K, Ding D, Foster C, Bauman AE, Sallis JF. Improving current practice in reviews of the built environment and physical activity. Improving current practice in reviews of the built environment and physical activity. 2015;45:297–302.
Kuper H, Nicholson A, Hemingway H. Searching for observational studies: what does citation tracking add to PubMed? A case study in depression and coronary heart disease. BMC Med Res Methodol. 2006;6:4.
Boarnet MG, Day K, Anderson C, McMillan T, Alfonzo M. California’s safe routes to school program. J Am Plan Assoc. 2005;71:301–17.
Brown BB, Werner CM. Before and after a new light rail stop: resident attitudes, travel behavior, and obesity. J Am Plan Assoc. 2008;75:5–12.
Cohen DA, Marsh T, Williamson S, Han B, Derose KP, Golinelli D, McKenzie TL. The potential for pocket parks to increase physical activity. Am J Health Prom. 2014;28:S19–26.
Cohen DA, Han B, Isacoff J, Shulaker B, Williamson S, Marsh T, McKenzie TL, Weir M, Bhatia R. Impact of park renovations on park use and park-based physical activity. J Phys Act Health. 2015;12:289–95.
Fitzhugh EC, Bassett DR, Jr., Evans MF: Urban trails and physical activity: a natural experiment. Am J Prev Med 2010;39:259–262.
Harduar-Morano L, Price JR, Parker D, Blackmore C. PACE EH post project assessment of quality of life changes in a Florida community related to infrastructure improvements. J Environ Health. 2008;70:40–6.
Lott DF, Tardiff T. Evaluation by experienced riders of a new bicycle lane in an established bikeway system. Transp Res Rec. 1979;683:40–6.
Morrison DS, Thomson H, Petticrew M. Evaluation of the health effects of a neighbourhood traffic calming scheme. J Epidemiol Community Health. 2004;58:837–40.
Parker KM, Rice J, Gustat J, Ruley J, Spriggs A, Johnson C. Effect of bike lane infrastructure improvements on ridership in one New Orleans neighborhood. Ann Behav Med. 2013;45(Suppl 1):S101–7.
Roemmich JN, Beeler JE, Johnson L. A microenvironment approach to reducing sedentary time and increasing physical activity of children and adults at a playground. Prev Med. 2014;62:108–12.
Shu S, Quiros DC, Wang R, Zhu YF. Changes of street use and on-road air quality before and after complete street retrofit: an exploratory case study in Santa Monica, California. Transport Res D-Tr E. 2014;32:387–96.
Tester J, Baker R. Making the playfields even: evaluating the impact of an environmental intervention on park use and physical activity. Prev Med. 2009;48:316–20.
Veitch J, Ball K, Crawford D, Abbott GR, Salmon J. Park improvements and park activity: a natural experiment. Am J Prev Med. 2012;42:616–9.
West ST, Shores KA. The impacts of building a greenway on proximate residents' physical activity. J Phys Act Health. 2011;8:1092–7.
Acknowledgements
Not applicable.
Funding
This research was funded by the New Zealand Ministry for Business, Innovation and Employment (grant number 29898). MS is supported by a Health Research Council of New Zealand Sir Charles Hercus Research Fellowship (grant number 17–013). The funding bodies had no role in the design of the study; collection, analysis, or interpretation of data; or writing the manuscript.
Availability of data and materials
The dataset used and analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
All authors conceived the idea, contributed to the search strategy employed, and read, contributed to, and approved the final manuscript. MS conducted the literature search, quality assessment, data extraction and analysis, and wrote the draft manuscript. JH undertook the 10% replication of data sourcing, extraction, and quality assessment; and conducted the equality assessment (data extraction, analysis, and write-up, with MS conducting 10% replication of data extraction).
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Search terms. (DOCX 11 kb)
Additional file 2:
Data extraction form. (DOCX 13 kb)
Additional file 3:
Adaptations made to the Evaluation of Public Health Practice Projects Quality Assessment Tool (EPHPP) scoring criteria. (DOCX 25 kb)
Additional file 4:
Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies - Component Ratings of Study. (DOCX 12 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Smith, M., Hosking, J., Woodward, A. et al. Systematic literature review of built environment effects on physical activity and active transport – an update and new findings on health equity. Int J Behav Nutr Phys Act 14, 158 (2017). https://doi.org/10.1186/s12966-017-0613-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-017-0613-9