
Abstract
Background
There exist contradictive views on whether the vitamin D has association with clinical outcome of in vitro fertilization (IVF) and/or intracytoplasmic sperm injection (ICSI). The present meta-analysis aim to establish whether vitamin D was associated with clinical outcomes of IVF/ICSI.
Methods
MEDLINE, Google Scholar and the Cochrane Library from database inception to March 2017 were searched. Clinical studies, which evaluated the association of vitamin D level and the clinical outcomes after IVF/ICSI, were included. The Main Outcome Measures were clinical pregnancy, ongoing pregnancy, and live birth.
Results
In the analysis of clinical pregnancy, 9 cohort studies were included. Of which, 2 studies and 3 studies were identified in analyzing ongoing pregnancy and live birth, respectively. Meta-analysis showed trends toward lower clinical pregnancy [RR 0.91, (95% CI 0.77–1.07)] and higher ongoing pregnancy [RR 1.06, (95% CI 0.95–1.19)] for women with deficient level of vitamin D. The probability of live birth for women with deficient level of vitamin D was significantly lower than cases with sufficient level of vitamin D [RR 0.74, (95% CI 0.58–0.90)].
Conclusions
Deficient vitamin D was associated with decreased probability of live birth after IVF/ICSI. So vitamin D should be supplied to women with deficient level vitamin D.
Similar content being viewed by others


Background
As a steroid hormone, Vitamin D exerts effect by binding with vitamin D receptor, which is a member of the nuclear receptors families [1, 2]. It was established that many tissues have vitamin D receptor, such as ovarian, endometrium, fallopian tube epithelial cells, placenta, decidual cells, hypothalamus, and pituitary [3,4,5,6]. Vitamin D plays critical role in the system of female reproduction, such as oocyte development, production of anti-Mullerian (AMH), ovarian steroidogrnrsis, endometrial receptivity, et al. It was supposed that vitamin D is associated with clinical pregnancy outcome of IVF/ICSI cycles.
So far, there were myriads of studies evaluating the association between vitamin D level and the clinical outcomes after ART. Some studies have indicated that deficient vitamin D was associated with pregnancy rate [7,8,9,10,11,12,13]. In contrast, some researchers found no association between vitamin D statuses with outcomes after IVF/ICSI cycles [14,15,16,17,18].
At present, two meta-analysis studies have evaluated the association between vitamin D level and outcomes of IVF/ICSI. One was done by Vanni et al., including three studies with 353 women. The study only compared the one outcome that is--clinical pregnancy rate, and found that deficient vitamin D was associated with lower probability of clinical pregnancy without statistically significance compared with vitamin D sufficient women [19]. The other meta-analysis, including five studies with 1238 women, compared both clinical pregnancy rate and live birth rate. The results displayed that deficient vitamin D was uncorrelated with clinical pregnancy rate, but related to decreased probability of live birth [20]. Although the design of the previous meta-analysis was suitable, the samples size of some studies was small.
So, it is necessary to conduct a systematic review and meta-analysis including more suitable studies to evaluated further whether deficient level vitamin D have effect on clinical pregnancy, ongoing pregnancy, and live birth after IVF/ICSI.
Methods
Identification of the literature
MEDLINE, Google Scholar and the Cochrane Library from inception until March 2017 were searched. The terms used to search literatures were as follows: one including terms on vitamin D (vitamin D, 25-hydroxy vitamin D, 25(OH) D, 1,25-(OH)2D), the other one including terms on reproductive techniques (in vitro fertilization, IVF, intracytoplasmic sperm injection, ICSI, assisted reproduction technologies, ART). Related citations were generated by combining the above terms with “AND”. Only papers fully published in English were covered. These included papers were reviewed by two investigators independently, and group discussion was needed if there was any discrepancies.
Study selection and data extraction
Studies evaluated the association between serum vitamin D levels and clinical outcomes after ART were selected. The primary outcomes of interest were clinical pregnancy and/or ongoing pregnancy, and /or live birth. For studies to be eligible, outcome data (with pregnancy rate and/or ongoing pregnancy rate and/or live birth rate in women with deficient or sufficient vitamin D levels) were extracted in 2 × 2 tables. We also recorded the study design, treatment protocol, threshold for deficient vitamin D, number of pregnant / live birth cycles with deficient or sufficient vitamin D levels. Newcastle–Ottawa Quality Assessment Scales was used to evaluate the quality of the observational studies [21]. Two reviewers completed the quality assessment, Group discussion was needed when there was any disagreements about inclusion.
Statistical analysis
We applied the meta-analysis method to complete the comparisons of study-by-study with the risk ratios (RRs) of the individual 2 × 2 tables. Forest plots were used to evaluate the heterogeneity of the included studies and the l2 value quantified heterogeneity between studies. Mantel- Haenszel Random effect models were implied according to the heterogeneity to calculate an overall RR and its 95% CI. A P-value of 0.10 rather than conventional level of 0.05 was considered to have statistical significance because of the low power of the X2 test for heterogeneity when studies have small sample size. The meta-analysis was conducted with RevMan 5.0 (Cochrane Collaboration, Oxford, UK).
Results
Studies selection and characteristics
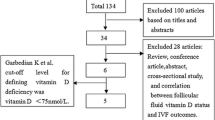
The search strategy yielded 52 citations, 17 of which are excluded after reviewing the titles and abstracts. Five of the 35 remaining publications were not suitable because either pregnancy or live birth data were not reported, and three papers were excluded because a 2 × 2 table was not extracted from the results. The remained 18 papers were reviews, meta-analysis or animal experiments. (Fig. 1).

Flow chart showing study selection process
The total number of eligible trails included in the present study was 9 (three IVF study, one ICSI study, three IVF/ICSI studies, and two oocyte donation studies) comprising 2254 couples reported clinical pregnancy rate after IVF/ICSI with 1112 pregnant cycles. 2 papers involved 784 couples also reported ongoing pregnancy rate and 3 studies involved 655 pregnant women with 238 live birth cycles.
The characteristics of included studies were depicted in Table 1. Of these 9 studies, 5 were retrospective studies and 4 were prospective studies. All the studies evaluated the vitamin D level in the serum, one study by Firouzabadi et al. [14] also examined the follicular fluid. The threshold for deficient vitamin D was 20 ng/ml in seven studies, 10 ng/ml in one study and 75 nmol/l in another study.
Meta-analysis
The present meta-analysis included 9 studies to evaluate the association between deficient level vitamin D and the clinical pregnancy outcomes after ART treatments. We found that there was a trend (without significance) toward lower in clinical pregnancy in women with deficient level of vitamin D compared with those with sufficient level of vitamin D. As the Q statistic P-value was below 0.1, there were heterogeneity of the studies (I2 = 68%, P = 0.002). The random effects model was implied and the combined RR was 0.91 (95% CI, 0.77, 1.07; P = 0.26) (Fig. 2).

Forest plot showing the results of meta-analysis of studies comparing the effect of deficient vitamin D and sufficient vitamin D on clinical pregnancy after IVF/ICSI
Among these studies, 2 papers evaluated the association between deficient vitamin D and on ongoing pregnancy at the same time. The results indicated that a similar ongoing pregnancy rate in patients with deficient and sufficient level vitamin D. The Q statistic P-value was above 0.1, indicating homogeneity of the studies (l2 = 0%, P = 0.39). The fixed effects model was implied and the combined RR was 1.06 (95% CI, 0.95, 1.19; P = 0.32) (Fig. 3).

Forest plot showing the results of meta-analysis of studies comparing the effect of deficient vitamin D and sufficient vitamin D on ongoing pregnancy after IVF/ICSI
Additionally, live birth rate was also evaluated and 3 studies were included. The results of meta-analysis showed a significantly lower live birth rate in women with deficient level vitamin D compared with ones with sufficient level vitamin. There was little heterogeneity in the results (l2 = 0%, P = 0.74). The fixed effects model combined RR was 0.72 (95% CI, 0.58, 0.90; P = 0.004) (Fig. 4).

Forest plot showing the results of meta-analysis of studies comparing the effect of deficient vitamin D and sufficient vitamin D on live birth after IVF/ICSI
The studies got high score on the Newcastle-Ottawa Quality Assessment Scale (not shown). The funnel plots of meta-analysis evaluating the association between vitamin D levels and the ongoing pregnancy and live birth after IVF/ICSI showed symmetrical shapes, indicating no publication bias (Additional file 1: Figure S1 and Additional file 2: Figure S2). However, a modest publication bias was seen when the clinical pregnancy was evaluated (Additional file 3: Figure S3).
Discussion
So far, only two systematic reviews and meta-analyses have evaluated the association between vitamin D level and the clinical outcomes of IVF/ICSI cycles. To our knowledge, the present study is the largest in regard to sample size with 3693 IVF/ICSI cycles. In the present review, 9 studies, 2 studies and 3 studies were included to evaluate the association between vitamin D and clinical pregnancy, ongoing pregnancy and live birth, respectively. Vitamin D level was statistically associated with live birth (RR 0.74; 95%CI 0.58–0.90) and was not related to clinical pregnancy (RR 0.91; 95% CI 0.77–1.07) and ongoing pregnancy (RR 1.06; 95% CI 0.95–1.19). The three RR value demonstrated that deficient vitamin D was associated with a decreased chance of live birth, while had similar probability in clinical pregnancy and ongoing pregnancy with women with sufficient vitamin D. The conclusion was agreement with the systematic reviews by Valeria et al. and Lv et al. [19, 20], but we included additional several publications and evaluated not only clinical pregnancy but also ongoing pregnancy and live birth after IVF/ICSI.
As mentioned above, Vitamin D plays an important role in the female reproductive system [3, 6]. Therefore, a woman’s vitamin D level is supposed to be related to reproductive health and pregnant outcomes. The effect of deficient vitamin D level on reproduction has been investigated since the 1970s. Some studies believed that deficient vitamin D might have detrimental effect on the women infertility and pregnant outcomes of IVF [7,8,9,10]. However, other studies found that vitamin D deficiency did not play a critical role in the outcome of ART [14,15,16]. These discrepancies may be attributed to differences in patients’ mean age, ethnicity, race, BMI, countries, social economic status, the season, exposure categorization, analysis methods, and study design [22].
Although the discrepancies between studies, the combined results indicated that vitamin D deficiency may bring negative effect on the outcome of ART. The possible mechanism may be as follows:
Firstly, it was reported that vitamin D might have effect on the development of follicle and embryo. Mice, in which the VDR genes have been knocked out, showed damaged folliculogenesis and underdevelopment of uterine in a previous animal experiments [23]. Vitamin D brought beneficial effect on the ovarian steroidogenesis and stimulated the production of Insulin-like growth factor-binding protein-1 (IGFBP-1) in ovary. Vitamin D promotes the production of estradiol, estrone, and progesterone [24]. Vitamin D level of reproductive age women was correlated with their serum AMH levels [25], so vitamin D may involved in the production of AMH in adults.
Secondly, Vitamin D was identified with influence upon endometrial receptivity. It was identified that vitamin D receptor was expressed in the endometrium of mice [26], whereas vitamin D receptor mutant female mice have an underdeveloped uterus and were infertile [27]. One study demonstrated the 1,25(OH) 2D3 administration could up-regulate the expression of HOXA10 mRNA and protein by combining with its receptor in the endometrial stromal cells, and HOXA10 is essential for female fertility and embryo implantation [28]. This view was further supported by a vitro cell experiments with human endometrial cells lines, indicating that the 1a–hydroxylase enzyme was up-regulated in the endometrial stromal cells of early pregnancy [29]. In an oocyte donor study, adjusted clinical pregnancy rates and live birth rate were lower in VD-deficient recipients than those of vitamin D sufficient recipients. This study suggested that vitamin D might affect the reproduction through mediating the endometrium, not the follicular or oocytes [11].
Thirdly, recent researches demonstrated that vitamin D is significant not only for embryo implantation but also for gestation as well. Clinical studies have shown that pregnant women with deficient vitamin D are more likely to be with preeclampsia, gestational diabetes, and cesarean section [30,31,32]. Varying levels expression of vitamin D and HOXA10 were tested in the endometrium, decidua and placenta throughout pregnancy [33]. Therefore, it was suggested that vitamin D plays a crucial role in keeping healthy pregnancy [34]. These may be the possible explanations for higher ongoing pregnancy rate while lower live birth rate.
Additionally, vitamin D affects the implantation and early pregnancy by involving the immune-modulating effect. Some studies showed that vitamin D may inhibit the activity of decidual T-cell and reduce the production of some cytokines such as interleukin 1 (IL-1), IL-6 and TNF-a, which are considered to be essential for embryo implantation and endometrial receptivity [29, 35]. The vitamin leads to a transition from T helper 1(TH-1) to the more tolerant TH-2. Endometrial cells produce 1a hydroxylase, which activates 25-OH vitamin D and is up-regulated by IL-1β produced by the blastocyst. Lower level of vitamin D has a tendency to increase the percentage of B cells, INF-a producing Th cells and NK cytotoxicity, all of these were factors for RM [36].
With regard to strength, the present study leads to a more accurate evaluation with the pooled RRs rather than individual study. The pooled results of included studies indicated that deficient vitamin D was associated with decreased chance of live birth after IVF/ICSI cycles. While evaluating the association between vitamin D and clinical pregnancy and ongoing pregnancy, the combined RRs showed a decreased trend in clinical pregnancy [RR 0.91; 95% CI 0.77–1.07] and an increased trend in ongoing pregnancy [RR 1.06; 95% CI 0.94–1.19] but the differences had no significances.
Certainly, the present meta-analysis still has its limitations. A major limitation was the obvious heterogeneity among these included studies’ characteristics, including varied study designs (retrospective/retrospective studies), different ovarian stimulation protocols (GnRH-a long or short protocol/GnRH-ant protocol), different treatment types (IVF / ICSI) and different threshold for deficient vitamin D level (20 ng/ml, 10 ng/ml or 75 nmol/L). In addition, small sample size of some included studies and short of meaningful confounders adjustment were also the limitations of the present study. In spite of these shortcomings, the present systematic review and meta-analysis reviewed and summarized the results of relative publications with valuable summary.
Conclusion
This systematic review showed that deficient vitamin D has negative effect on the pregnancy after IVF/ICSI treatment. As the sample sizes of some studies were small and the study characteristics were different, further random cohort studies are needed to observe the effect of vitamin D supplementation and explore the possible effect mechanisms.
Abbreviations
- ART:
-
Assisted reproductive technology
- CI:
-
Confidence interval
- ICSI:
-
Intracytoplasmic sperm injection
- IR:
-
Implantation rate
- IVF:
-
In vitro fertilization
- OR:
-
Odds ratio
- PR:
-
Pregnancy rate
References
Halloran BP, DeLuca HF. Effect of vitamin D deficiency on fertility and reproductive capacity in the female rat. J Nutr. 1980;110:1573–80.
Johnson LE, HF DL. Vitamin D receptor null mutant mice fed high levels of calcium are fertile. J Nutr. 2001;131:1787–91.
Kinuta K, Tanaka H, Moriwake T, Aya K, Kato S, Seino Y. Vitamin D is an important factor in estrogen biosynthesis of both female and male gonads. Endocrinology. 2000;141:1317–24.
Hurley WL, Doane RM. Recent developments in the roles of vitamins and minerals in reproduction. J Dairy Sci. 1989;72:784–804.
Halhali A, Acker GM, Garabedian M. 1,25-Dihydroxyvitamin D3 induces in vivo the decidualization of rat endometrial cells. J Reprod Fertil. 1991;91:59–64.
Harkness LS, Bonny AE. Calcium and vitamin D status in the adolescent: key roles for bone, body weight, glucose tolerance, and estrogen biosynthesis. J Pediatr Adolesc Gynecol. 2005;18:305–11.
Ozkan S, Jindal S, Greenseid K, Shu J, Zeitlian G, Hickmon C, et al. Replete vitamin D stores predict reproductive success following in vitro fertilization. Fertil Steril. 2010;94:1314–9.
Anifandis GM, Dafopoulos K, Messini CI, Chalvatzas N, Liakos N, Pournaras S, et al. Prognostic value of follicular fluid 25-OH vitamin D and glucose levels in the IVF outcome. Reprod Biol Endocrinol. 2010;8:91.
Garbedian K, Boggild M, Moody J, Liu KE. Effect of vitamin D status on clinical pregnancy rates following in vitro fertilization. CMAJ Open. 2013;1:E77–82.
Rudick B, Ingles S, Chung K, Stanczyk F, Paulson R, Bendikson K. Characterizing the influence of vitamin D levels on IVF outcomes. Hum Reprod. 2012;27:3321–7.
Rudick BJ, Ingles SA, Chung K, Stanczyk FS, Paulson RJ, Bendikson KA. Influence of vitamin D levels on in vitro fertilization outcomes in donor-recipient cycles. Fertil Steril. 2014;101:447–52.
Paffoni A, Ferrari S, Vigano P, Pagliardini L, Papaleo E, Candiani M, Tirelli A, Fedele L, Somigliana E. Vitamin D deficiency and infertility insights from in vitro fertilization cycles. J Clin Endocrinol Metal. 2014;99:1–9.
Polyzos NP, Anckaert E, Guzman L, Schiettecatte J, Landuyt LV, Camus M, Smitz J, Tournaye H. Vitamin D deficiency and pregnancy rates in women undergoing single embryo, blastocyst stage, transfer (SET) for IVF/ICSI. Hum Reprod. 2014;29:2032–40.
Firouzabadi RD, Rahmani E, Rahsepar M, Firouzabadi MM. Value of follicular fluid vitamin D in predicting the pregnancy rate in an IVF program. Arch Gynecol Obstet. 2014;289:201–6.
Aleyasin A, Hosseini MA, Mahdavi A, Safdarian L, Fallahi P, Mohajeri MR, et al. Predictive value of the level of vitamin D in follicular fluid on the outcome of assisted reproductive technology. Eur J Obstet Gynecol Reprod Biol. 2011;159:132–7.
Van de Vijver A, Drakopoulos P, Van Landuyt L, Vaiarelli A, Blockeel C, Santos-Ribeiro S, et al. Vitamin D deficiency and pregnancy rates following frozen–thawed embryo transfer: a prospective cohort study. Hum Reprod. 2016;31:1749–54.
Fabris A, Pacheco A, Cruz M, Puente JM, Fatemi H, Garcia-Velasco JA. Impact of circulating levels of total and bioavailable serum vitamin D on pregnancy rate in egg donation recipients. Fertil Steril. 2014;102:1608–12.
Franasiak JM, Molinaro TA, Dubell EK, Scott KL, Ruiz AR, Forman EJ, et al. Vitamin D levels do not affect IVF outcomes following the transfer of euploid blastocysts. Am J Obstet Gynecol. 2015;212:315e1–6.
Vanni VS, Vigano P, Somigliana E, Papaleo E, Paffoni A, Pagliardini L, et al. Vitamin D and assisted reproduction technologies: current concepts. Reprod Biol Endocrinol. 2014;12:47.
Lv SS, Ji YW, Wang XQ, Wang Y, Yong X. Serum vitamin D status and in vitro fertilization outcomes: a systematic review and meta-analysis. Arch Gynecol Obstet. 2016;293:1339–45.
Wells G, SBOD. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of non-randomised Studies in Meta-analysis, Improving Quality and Impact. Oxford: Proceedings or the Third Symposium on Systematic Reviews beyond the Basics; 2000.
Nesby-O’Dell S, Scanlon KS, Cogswell ME, Gillespie C, Hollis BW, Looker AC, et al. Hypovitaminosis D prevalence and determinants among African American and white women of reproductive age: third National Health and nutrition examination survey, 1988-1994. Am J Clin Nutr. 2002;76:187–92.
Yoshizawa T, Handa Y, Uematsu Y, Takeda S, Sekine K, Yoshihara Y, et al. Mice lacking the vitamin D receptor exhibit impaired bone formation, uterine hypoplasia and growth retardation after weaning. Nat Genet. 1997;16:391–6.
Parikh G, Varadinova M, Suwandhi P, Araki T, Rosenwaks Z, Poretsky L, et al. Vitamin D regulates steroidogenesis and insulin-like growth factor binding protein-1 (IGFBP-1) production in human ovarian cells. Horm Metab Res. 2010;42:754.
Aflatoonian A, Mashayekhy M, Mohamadian F, Moghaddam FM. The correlation between follicular fluid anti-mullerian hormone levels and fertilization and embryo quality in ART cycles. Iran J Reprod Med. 2010;8:157–60.
Zarnani AH, Shahbazi M, Salek-Moghaddam A, Zareie M, Tavakoli M, Ghasemi J, et al. Vitamin D(3) receptor is expressed in the endometrium of cycling mice throughout the estrous cycle. Fertil Steril. 2010;93:2738–43.
Johnson LE, Deluca HF. Vitamin D receptor null mutant mice fed high levels of calcium are fertile. J Nutrition. 2001;131:1787–91.
Lerchbaum E, Obermayer-Pietsch B. Mechanisms in endocrinology: vitamin D and fertility: a systematic review. Eur J Endocrinol. 2012;166:765–78.
Vigano P, Lattuada D, Mangioni S, Ermellino L, Vignali M, Caporizzo E, et al. Cycling and early pregnant endometrium as a site of regulated expression of the vitamin D system. J Mol Endocrinol. 2006;36:415–24.
Merewood A, Mehta SD, Chen TC, Bauchner H, Holick MF. Association between severe vitamin D deficiency and primary caesarean section. J Clin Endocrinol Metab. 2009;94:940–5.
Shand AW, Nassar N, Von Dadelszen P, Innis SM, Green TJ. Maternal vitamin D status in pregnancy and adverse pregnancy outcomes in a group at high risk for pre-eclampsia. BJOG. 2010;117:1593–8.
Soheilykhah S, Mojibian M, Rashidi M, Rahimi-Saghand S, Jafari F. Maternal vitamin D status in gestational diabetes mellitus. Nutr Clin Pract. 2010;25:524–7.
Evans KN, Nguyen L, Chan J, Innes BA, Bulmer JN, Kilby MD, et al. Effects of 25-hydroxyvitamin D3 and 1,25-dihydroxyvitamin D3 on cytokine production by human decidual cells. Biol Reprod. 2006;75:816–22.
Bodnar LM, Catov JM, Simhan HN, Holick MF, Powers RW, Roberts JM. Maternal vitamin D deficiency increases the risk of preeclampsia. J Clin Endocrinol Metab. 2007a;92:3517–22.
Pasco JA, Wark JD, Carlin JB, Ponsonby A-L, Vuillermin PJ, Morley R. Maternal vitamin D in pregnancy may influence not only offspring bone mass but other aspects of musculoskeletal health and adiposity. Med Hypothes. 2008;71:266–9.
Chen X, Yin B, Lian R-C, Zhang T, Zhang H-Z, Diao L-H, et al. Modulatory effects of vitamin D on peripheral cellular immunity in patiens with recurrent miscarriage. Am J Reprod Immunol. 2016;76:432–8.
Acknowledgments
Not applicable
Funding
This project was supported by the National Natural Science Foundation of China (Grant No. 81401269).
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article and its additional file.
Author information
Authors and Affiliations
Contributions
ZJ contributed to the study design and acquisition of data, article drafting and revising as well as organization of the final approval of the version to be published. HX contributed substantially to the interpretation of the data and helped with drafting and revision of the article. LY contributed to conception and design, acquisition of data and analysis and interpretation of data. YY and XB contributed significantly to the acquisition, analysis and interpretation of the data. ZQ helped with revision of the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1: Figure S1.
Funnel plot of analysis for the effect of vitamin D level on pregnancy, showing the results of Eggers to assess publication bias. (PDF 19 kb)
Additional file 2: Figure S2.
Funnel plot of analysis for the effect of vitamin D level on ongoing pregnancy, showing the results of Eggers to assess publication bias. (PDF 17 kb)
Additional file 3: Figure S3.
Funnel plot of analysis for the effect of vitamin D level on live birth, showing the results of Eggers to assess publication bias. (PDF 18 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Zhao, J., Huang, X., Xu, B. et al. Whether vitamin D was associated with clinical outcome after IVF/ICSI: a systematic review and meta-analysis. Reprod Biol Endocrinol 16, 13 (2018). https://doi.org/10.1186/s12958-018-0324-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12958-018-0324-3