Abstract
Background
Hypertriglyceridemia (HTG) is one of the most common etiologies of acute pancreatitis (AP). Variants in five genes involved in the regulation of plasma lipid metabolism, namely LPL, APOA5, APOC2, GPIHBP1 and LMF1, have been frequently reported to cause or predispose to HTG.
Methods
A Han Chinese patient with HTG-induced AP was assessed for genetic variants by Sanger sequencing of the entire coding and flanking sequences of the above five genes.
Results
The patient was a 32-year-old man with severe obesity (Body Mass Index = 35) and heavy smoking (ten cigarettes per day for more than ten years). At the onset of AP, his serum triglyceride concentration was elevated to 1450.52 mg/dL. We sequenced the entire coding and flanking sequences of the LPL, APOC2, APOA5, GBIHBP1 and LMF1 genes in the patient. We found no putative deleterious variants, with the exception of a novel and heterozygous nonsense variant, c.1024C > T (p.Arg342*; rs776584760), in exon 7 of the LMF1 gene.
Conclusions
This is the first time that a heterozygous LMF1 nonsense variant was found in a HTG-AP patient with severe obesity and heavy smoking, highlighting an important interplay between genetic and lifestyle factors in the etiology of HTG.
Similar content being viewed by others


Background
Hypertriglyceridemia-induced acute pancreatitis (HTG-AP) usually refers to acute pancreatitis (AP) occurred in subjects with fasting serum triglyceride (TG) levels of > 1000 mg/dL (> 11.3 mmol/L) or > 500 mg/dL (> 5.65 mmol/L) with coincidentally detected milky serum and in the absence of other etiologic factors. Hypertriglyceridemia (HTG) is responsible for 2–5% of AP patients in Western countries [1] but the corresponding figure is 7.8–25.6% and tends to increase in China [2,3,4], demonstrating a marked ethnic difference in the etiology of AP. HTG-AP is more often associated with greater severity and higher recurrence and complication rates as compared with other etiologies of AP. This is particularly true in patients with primary severe HTG.
Variants in five genes involved in the regulation of plasma lipid metabolism, namely LPL (encoding lipoprotein lipase, which catalyzes hydrolysis of TG-rich lipoproteins [5]), APOA5 (encoding apolipoprotein A-V, which stabilizes the lipoprotein–LPL complex [6]), APOC2 (encoding apolipoprotein C-II, which acts as an essential LPL activator [7]), GPIHBP1 (encoding glycosylphosphatidylinositol-anchored high density lipoprotein-binding protein 1, which mediates the transmembrane transport and binding of LPL [8]), and LMF1 (encoding lipase maturation factor 1, which is involved in the folding and expression of LPL [9]), have been frequently reported to cause or predispose to HTG. HTG may be of monogenic origin in some patients, for example, those with the autosomal recessive inherited familial hyperchylomicronemia syndrome. However, the etiology of HTG in most cases is complex and likely involves gene-gene and/or gene-lifestyle interactions [10].
Herein, we describe a case with HTG-AP that appeared to be predisposed by a combination of genetic susceptibility and exposure to harmful lifestyle factors.
Materials and methods
Patient
The patient was a 32-year-old man with severe obesity (Body Mass Index (BMI) = 35) and heavy smoking (ten cigarettes per day for more than ten years). He was diagnosed to have moderate HTG (fasting serum TG concentration, ~ 500 mg/dL (~ 5.65 mmol/L)) three years ago (at the age of 29) but had not taken lipid-lowering drugs. His father had diabetes mellitus, his mother was healthy, and there was no known history of HTG in the family.
He was hospitalized elsewhere due to severe abdominal pain associated with nausea and vomiting on June 5, 2017. He was transferred to our Surgical Intensive Care Unit for further treatment on June 11, 2017. The study was performed in accordance with the Helsinki Declaration and was approved by the Ethics Committee of Jingling Hospital, Nanjing University. Bio-samples were obtained after written informed consent.
Plasma lipid profile analysis
Blood samples were collected after fasting for 12 h. Serum glucose (GLU), TG, total cholesterol (TC), high-density lipoprotein (HDL), low density lipoprotein (LDL), apolipoprotein A1 (APOA1), and apolipoprotein B (APOB) levels were measured enzymatically on an automatic analyzer (Hitachi High-Tech, 7600–120, Japan).
Mutational analysis of five HTG genes
Genomic DNA was extracted from the peripheral blood cells using a Gentra Puregene Blood kit (Qiagen, Dusseldorf, Germany) according to the manufacturer’s instructions. The entire coding and flanking sequences of LPL, APOA5, APOC2, LMF1, and GPIHBP1 were amplified by polymerase chain reaction (PCR) and subsequently sequenced using both forward and reverse primers (primer sequences available upon email request). Identified mutations were subjected to confirmation by independent PCR amplification and sequencing. Nomenclature for the description of the reported LMF1 mutation followed the Human Genome Variation Society (HGVS) recommendations [11]. GenBank accession number NM_022773.3 was used as the LMF1 mRNA reference sequence.
Results
Clinical features of the HTG-AP patient
When the patient was initially hospitalized elsewhere, his blood sample was milky, with the serum TG concentration being elevated to 1450.52 mg/dL (16.39 mmol/L). Moreover, his serum TC and GLU levels were elevated to 6.55 mmol/L and 20.35 mmol/L, respectively. The patient was diagnosed with severe AP with the complication of acute necrotic collection (Fig. 1) according to the 2012 Atlanta consensus report [12]. On admission in our hospital, physical examination of the patient revealed epigastric tenderness and distension without rebound tenderness or Murphy’s sign. Laboratory examination revealed elevations in amylase (274 U/L), white blood cell count (14.5 × 109/L) as well as inflammation markers C-reactive protein (CRP, 156.9 mg/L) and procalcitonin (PCT, 0.821 μg/L). Arterial blood gas analysis showed that pondus hydrogenii (PH) was 7.382 mmol/L, partial pressure of oxygen (PaO2) was 86.8 mmol/L, and fraction of inspiration oxygen (FiO2) was 33%. Renal and cardiovascular functions were normal.

Abdominal computed tomography (CT) showing the enlarged pancreas with adjacent water density shadow, disappearance of the space among peripancreatic adipose tissues in the patient. Left panel, plain CT scan. Right panel, enhanced CT scan. Blue, red and yellow arrowheads indicate acute necrotic collection, pancreatic edema and acute peripancreatic fluid collection, respectively
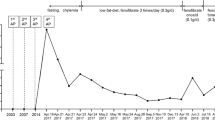
The patient was treated as illustrated in Fig. 2, in which the serum TG, TC, and GLU levels in different time points were also provided. Of particular note, after fasting for 6 days, the patient’s serum TG level plunged to 292.04 mg/dL (3.3 mmol/L). However, his TG level rose to 752.21 mg/dL (8.5 mmol/L) several days after general treatment and enteral nutrition intake. Consequently, he was given lipid-lowering drug Lipanthyl and his TG level decreased to 395.58 mg/dL (4.47 mmol/L). Before discharge on July 1, 2017, the patient’s TG level was 359.29 mg/dL (4.06 mmol/L). Thereafter, he was instructed to adhere to a low fat diet with prescription of Lipanthyl and metformin. A follow-up examination performed in September 2018 revealed a serum TG concentration of 353.98 mg/dL (4.0 mmol/L) (Fig. 2).

Flow-chart showing treatment procedure and serum TG, TC, and GLU levels in the patient. TG, triglyceride; TC, total cholesterol; GLU, glucose; EN, enteral nutrition
Genetic findings
We sequenced the entire coding and flanking sequences of the LPL, APOC2, APOA5, GBIHBP1 and LMF1 genes in the patient (sequencing data available in Additional file 1). We found no putative deleterious variants, with the exception of a heterozygous nonsense variant, c.1024 C > T (p.Arg342*; rs776584760), in exon 7 of the LMF1 gene (Fig. 3). This variant was absent in our other 131 HTG-AP patients, 85 AP patients without HTG, and 43 healthy controls (all subjects were Han Chinese). Unfortunately, no family members were available for genetic analysis.

Identification of a novel and heterozygous nonsense variant in the LMF1 gene. Sequencing electropherograms of the wild-type sequence from a healthy control and the heterozygous LMF1 c.1024C > T (p.Arg342*) variant from the patient are shown. The affected codon 342 (in exon 7 of the LMF1 gene) is underlined in the context of the wild-type sequence
Discussion
In this study, we identified a heterozygous LMF1 nonsense mutation, c.1024C > T (p.Arg342*), in a Han Chinese patient with HTG-AP. To our best knowledge, this variant has not been previously reported to be associated with HTG in the literature. Moreover, this variant was also absent in the ClinVar database (https://www.ncbi.nlm.nih.gov/clinvar/; as of November 8, 2018). Further, survey of the Genome Aggregation Database (genomAD, http://gnomad.broadinstitute.org/; as of November 8, 2018) revealed that the c.1024 C > T variant was present at an average allele frequency of 0.00002857 (7 of 244,974) in all populations combined; and its allele frequency in the East Asian population was 0.0002238 (4 of 17,876). In short, the LMF1 c.1024 C > T variant is extremely rare in normal populations.
The human LMF1 gene encodes a 567 amino acid protein. Recently, Serveaux Dancer and colleagues assessed the functionality of two LMF1 nonsense variants, p.Tyr439* and p.Trp464*, by means of an in vitro assay. Specifically, they co-transfected HEK293T cells with the wild-type LPL expression vector and the LMF1 mutant expression vector of interest; and then measured the LPL activity in the culture media of the co-transfected HEK-293 T cells. As such, Serveaux Dancer and colleagues found that both the LMF1 p.Tyr439* and p.Trp464* nonsense variants caused an almost complete loss of the LPL activity [13]. The LMF1 c.1024C > T (p.Arg342*) variant reported here, which removes ~ 100 more residues from the C terminus of the protein as compared to p.Tyr439* and p.Trp464*, can be reasonably concluded to cause a complete functional loss of the affected LMF1 allele.
A particularly interesting finding of the Serveaux Dancer study is that in one of their subjects with severe HTG, their mutational analysis of the LPL, APOC2, APOA5, GBIHBP1 and LMF1 genes identified only a single and heterozygous deleterious variant, LMF1 p.Trp464* (N.B. one of the aforementioned loss-of-function LMF1 nonsense mutations) [13]. Prior to their report, all heterozygous carriers of nonsense LMF1 variants had been described to have either normal or at most borderline HTG. Thus, our patient represents the second heterozygous carrier of a LMF1 nonsense variant who had severe HTG. This notwithstanding, it is pertinent to emphasize an important difference between the two relevant severe HTG patients in terms of their underlying etiological factors. In the Serveaux Dancer study, the two other heterozygous carriers of the LMF1 p.Trp464* variant had normal TG concentration; and the 8-month-old proband with the heterozygous LMF1 p.Trp464* variant exhibited severe HTG (1860 mg/dL (21 mmol/L)) on an episode of severe acute gastroenteritis (a condition known to be associated with moderate HTG) without AP. In our study, we were not able to analyze the patient’s parents but neither of them was known to have HTG. Notably, our patient had two harmful lifestyle factors, severe obesity and heavy tobacco abuse. Obesity, producing more TG, is not only associated with primary HTG [14] but also is a risk factor for secondary HTG [15]. Tobacco can influence the lipometabolism of liver, thereby increasing free fatty acid delivery into plasma that can in turn triggers a rise in TG level due to the defective lipolytic system [16]. In addition, tobacco has also been reported to be a risk factor for AP development [17]. In short, whereas the two severe HTG patients had LMF1 variants of similar functional effects, they had quite different secondary HTG-predisposing factors.
Finally, we would like to make two points. First, the LMF1 protein expression level in the patient carrying the heterozygous LMF1 nonsense variant, c.1024C > T (p.Arg342*), is assumed to be half of that in health controls. We were not able to confirm this assumption due to the unavailability of pathophysiologically relevant tissue(s) from the patient. Second, “LPL is also expressed at high levels in certain regions of the brain. Why LPL is produced in neurons of the brain remains an enigma ….” [18]. Intriguingly, LMF1, which is involved in the folding and expression of LPL, is also highly expressed in the brain (see https://www.proteinatlas.org/search/lmf1).
Conclusions
In conclusion, we have for the first time discovered a novel and heterozygous LMF1 nonsense variant in a HTG-AP patient with severe obesity and heavy smoking, highlighting an important interplay between genetic and lifestyle factors in the etiology of HTG.
Abbreviations
- AP:
-
Acute pancreatitis
- APOA1:
-
Apo-protein A1
- APOA5:
-
Apolipoprotein A-V
- APOB:
-
Apo-protein B
- APOC2:
-
Apolipoprotein C-II
- BMI:
-
Body mass index
- CRP:
-
C-reactive protein
- EN:
-
Enteral nutrition
- FiO2 :
-
fraction of inspiration oxygen
- Glu:
-
Glucose
- GPIHBP1:
-
Glycosylphosphatidylinositol-anchored high-density lipoprotein binding protein 1
- HDL:
-
High density lipoprotein
- HTG:
-
Hypertriglyceridemia
- LDL:
-
Low density lipoprotein
- LMF1:
-
Lipase maturation factor 1
- LPL:
-
Lipoprotein lipase
- PaO2 :
-
Partial pressure of oxygen
- PCR:
-
Polymerase chain reaction
- PCT:
-
Procalcitonin
- PH:
-
Pondus hydrogenii
- TC:
-
Total cholesterol
- TG:
-
Triglyceridemia
References
Forsmark CE, Vege SS, Wilcox CM. Acute pancreatitis. N Engl J Med. 2016;375:1972–81.
Carr RA, Rejowski BJ, Cote GA, Pitt HA, Zyromski NJ. Systematic review of hypertriglyceridemia-induced acute pancreatitis: a more virulent etiology? Pancreatology. 2016;16:469–76.
Zheng Y, Zhou Z, Li H, Li J, Li A, Ma B, Zhang T, Liao Q, Ye Y, Zhang Z, Yang Y, Wang Z, Zhang Z, Yang J, Li F. A multicenter study on etiology of acute pancreatitis in Beijing during 5 years. Pancreas. 2015;44:409–14.
Zhu Y, Pan X, Zeng H, He W, Xia L, Liu P, Zhu Y, Chen Y, Lv N. A study on the etiology, severity, and mortality of 3260 patients with acute pancreatitis according to the revised Atlanta classification in Jiangxi, China over an 8-year period. Pancreas. 2017;46:504–9.
Ma Y, Henderson HE, Murthy V, Roederer G, Monsalve MV, Clarke LA, Normand T, Julien P, Gagné C, Lambert M, et al. A mutation in the human lipoprotein lipase gene as the most common cause of familial chylomicronemia in French Canadians. N Engl J Med. 1991;324:1761–6.
Pennacchio LA, Olivier M, Hubacek JA, Cohen JC, Cox DR, Fruchart JC, Krauss RM, Rubin EM. An apolipoprotein influencing triglycerides in humans and mice revealed by comparative sequencing. Science. 2001;294:169–73.
Breckenridge WC, Little JA, Steiner G, Chow A, Poapst M. Hypertriglyceridemia associated with deficiency of apolipoprotein C-II. N Engl J Med. 1978;298:1265–73.
Beigneux AP, Davies BS, Gin P, Weinstein MM, Farber E, Qiao X, Peale F, Bunting S, Walzem RL, Wong JS, Blaner WS, Ding ZM, Melford K, Wongsiriroj N, Shu X, de Sauvage F, Ryan RO, Fong LG, Bensadoun A, Young SG. Glycosylphosphatidylinositol-anchored high-density lipoprotein-binding protein 1 plays a critical role in the lipolytic processing of chylomicrons. Cell Metab. 2007;5:279–91.
Péterfy M, Ben-Zeev O, Mao HZ, Weissglas-Volkov D, Aouizerat BE, Pullinger CR, Frost PH, Kane JP, Malloy MJ, Reue K, Pajukanta P, Doolittle MH. Mutations in LMF1 cause combined lipase deficiency and severe hypertriglyceridemia. Nat Genet. 2007;39:1483–7.
Hegele RA, Ginsberg HN, Chapman MJ, Nordestgaard BG, Kuivenhoven JA, Averna M, Borén J, Bruckert E, Catapano AL, Descamps OS, Hovingh GK, Humphries SE, Kovanen PT, Masana L, Pajukanta P, Parhofer KG, Raal FJ, Ray KK, Santos RD, Stalenhoef AF, Stroes E, Taskinen MR, Tybjærg-Hansen A, Watts GF, Wiklund O. European atherosclerosis society consensus panel. The polygenic nature of hypertriglyceridaemia: implications for definition, diagnosis, and management. Lancet Diabetes Endocrinol. 2014;2:655–66.
den Dunnen JT, Dalgleish R, Maglott DR, Hart RK, Greenblatt MS, McGowan-Jordan J, Roux AF, Smith T, Antonarakis SE, Taschner PE. HGVS recommendations for the description of sequence variants: 2016 update. Hum Mutat. 2016;37:564–9.
Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS. Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–11.
Serveaux Dancer M, Di Filippo M, Marmontel O, Valéro R, Piombo Rivarola MDC, Peretti N, Caussy C, Krempf M, Vergès B, Mahl M, Marçais C, Moulin P, Charrière S. New rare genetic variants of LMF1 gene identified in severe hypertriglyceridemia. J Clin Lipidol. 2018;12:1244–52.
Shah AS, Wilson DP. Primary hypertriglyceridemia in children and adolescents. J Clin Lipidol. 2015;9:S20–8.
Blackett PR, Wilson DP, McNeal CJ. Secondary hypertriglyceridemia in children and adolescents. J Clin Lipidol. 2015;9:S29–40.
Athyros VG, Katsiki N, Doumas M, Karagiannis A, Mikhailidis DP. Effect of tobacco smoking and smoking cessation on plasma lipoproteins and associated major cardiovascular risk factors: a narrative review. Curr Med Res Opin. 2013;29:1263–74.
Sun X, Huang X, Zhao R, Chen B, Xie Q. Meta-analysis: tobacco smoking may enhance the risk of acute pancreatitis. Pancreatology. 2015;15:286–94.
Brown WV, Goldberg IJ, Young SG. JCL roundtable: hypertriglyceridemia due to defects in lipoprotein lipase function. J Clin Lipidol. 2015;9:274–80.
Acknowledgements
The authors are indebted to all doctors, nurses and researchers for the follow-up assessment and data collection in the Severe Acute Pancreatitis Center of Jinling Hospital.
Funding
This research was funded by National Natural Science Foundation of China (No. 81570584 and No. 81670588); Social Development Project of Jiangsu Province (No. BE2015685 and No. BE2016749); Natural Science Foundation of Yangzhou City (No. YZ2017106); Postdoctoral Science Foundation of China (No. 2018 M632260) and Postdoctoral Science Foundation of Jiangsu Province (No. 1701047C).
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its Additional file 1].
Author information
Authors and Affiliations
Contributions
Conceptualization, WWC and QY; Investigation, NP; Formal Analysis, XYL and XLS; Writing – Original Draft Preparation, WWC and QY; Writing – Review & Editing, JMC, GTL and ZHT; Supervision, WQL. All authors have read and approved the final version of this manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethics committee of the Jinling Hospital, Medical School of Nanjing University. Written informed consent was obtained from each participant.
Consent for publication
Consent for publication was obtained from the patient.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Sequencing data. (DOCX 22 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chen, WW., Yang, Q., Li, XY. et al. Identification of a novel and heterozygous LMF1 nonsense mutation in an acute pancreatitis patient with severe hypertriglyceridemia, severe obesity and heavy smoking. Lipids Health Dis 18, 68 (2019). https://doi.org/10.1186/s12944-019-1012-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-019-1012-9