
Abstract
Background
Children < 5 years of age are at risk of developing an iron deficiency due to a low intake of bioavailable iron (FeBio). Few studies have estimated dietary FeBio in children at a national level in relation to sociodemographic characteristics. This study aimed to estimate FeBio intake and its association with sociodemographic factors among Mexican children aged 12–59 months.
Methods
A cross-sectional study was carried out. Information on serum ferritin and diet was obtained from a national survey and representative sample of 1012 Mexican children aged 12–59 months. We used a 24-h recall to estimate total iron, heme and non-heme iron, vitamin C, phytates, calcium, and meat intake. We calculated FeBio intake using an algorithm. Differences in FeBio intake were analyzed by area of residence (rural/urban), country region (north, center, south), and socioeconomic status (SES), using linear regression models by age subgroups (12–23 and 24–59 months) and total population, while adjusting for study design.
Results
Total iron intake was 9.2 ± 6.7 mg/d. The estimated average of total FeBio fluctuated between 0.74–0.81 mg/d, with a bioavailability of 9.15–12.03% of total iron. Children aged 12–23 months residing in rural areas consumed less FeBio than those in urban areas (β = − 0.276) (p < 0.05). Children aged 24–59 months with high SES consumed more FeBio (β = 0.158 mg/d) than those of a low SES (p < 0.05).
Conclusions
FeBio is low in Mexican preschoolers. Being from a rural area and having low SES were negatively associated with FeBio intake. These results can benefit interventions seeking to improve iron status.
Similar content being viewed by others


Introduction
Worldwide, 47% of children under the age of five have anemia, which is mainly attributed to iron deficiency [1]. In 2012, the national prevalence of iron deficiency in Mexican preschool children was 13.6%, while prevalence of anemia was 23.3% [2].
Iron deficiency in children < 2 years of age can result in long-term cognitive deficits and psychomotor impairment [3, 4]. In preschool children, iron deficiency is associated with a lower intelligence quotient, behavioral changes, and reduced capacity for physical activity [5, 6].
Iron-deficiency anemia is due to low iron intake and more specifically, low bioavailable iron (FeBio). Inflammation, parasitic diseases, and genetic disorders are other factors known to cause anemia [1]. Iron bioavailability refers to the proportion of iron ingested, absorbed and metabolized, is essential for a number of physiological functions [7], and should be considered in diet adequacy estimates [8, 9]. The mean iron bioavailability in the United States and Canada diets is estimated at 18% for children ≥1 year [10]. However, in Mexico iron bioavailability is lower, because the Mexican traditional diet is rich in plant-based foods such as grains and legumes, an important source of phytates, which inhibit non-heme iron absorption [8, 11].
There are two forms of dietary iron: 1) heme iron, which comes from hemoglobin and myoglobin in animal source foods, with uniform absorption, and could contribute ≥40% of total absorbed iron [12]. 2) non-heme iron found in plants, animal tissues and widely present in fortified foods, and supplement compounds, its bioavailability depends on body iron reserves, iron absorption enhancers, and absorption inhibitors consumed [13, 14]. Iron absorption is estimated using stable iron isotopes [15,16,17]; however, this method is not feasible in population studies. For this reason, algorithms have been designed to measure its bioavailability in populations [13, 14, 18]. In Mexico, estimates found a low bioavailability of iron (2.7–6.1%), as well as an elevated intake of phytates in preschoolers’ diets [13].
Dietary patterns vary with socioeconomic characteristics, which determine iron bioavailability. In Mexico, the probability of consuming fruits, vegetables, and red meat in important quantities, is greater in individuals with a high socioeconomic status (SES) and those who reside in urban areas [19]. In Mexico, the population of northern region consumes more processed meats than in the central region [19]. The southern region follows traditional dietary patterns, with a greater consumption of plant-based foods, which influences iron intake, absorption enhancers, and absorption inhibitors [8, 19]. In Mexico, mother’s educational level was also associated with children’s healthy diets (adequate in micronutrients) [20, 21].
To our knowledge, FeBio has not been recently estimated with national data in Mexico, nor has its relationship with sociodemographic characteristics been explored. The purpose of this study is to estimate FeBio and analyze its association with sociodemographic characteristics, such as area of residence (urban/rural), region and socioeconomic status in Mexican children from 12 to 59 months of age.
Methods
Design and population
The present study is cross-sectional. Information was obtained from the 2012 National Health and Nutrition Survey (2012 ENSANUT, by its Spanish acronym), which is a national, probabilistic survey, with state-level, regional, and urban/rural representation. The survey was carried out between October 2011 and May 2012 [22]. The purpose of this survey was to quantify the frequency, distribution, and patterns of the Mexican population’s health and nutrition status. The 2012 ENSANUT included 50,528 households. Information on diet was obtained in a subsample of 2655 children < 5 years [23, 24]. More details on the 2012 ENSANUT can be found in other documents [22,23,24].
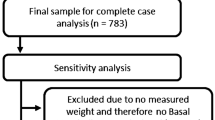
This study included preschool aged children that provided a blood sample and their parents completed a 24-h dietary recall questionnaire. Of the sample with valid diet information (n = 2113), children whose serum ferritin concentrations (SF) and C-reactive protein (CRP) levels could not be determined were excluded (n = 1101) (measures described below). The final sample included 1012 children (Fig. 1).

Study flowchart
The 2012 ENSANUT was approved by the research, biosecurity, and ethics committees at the National Institute of Public Health [Instituto Nacional de Salud Pública (INSP by its Spanish acronym)] in Cuernavaca, Morelos, Mexico. Informed consent was signed by the parents or guardians of the participating children [24].
Information on diet was obtained using a 24-h recall. The dietary information was provided by mothers or the person in charge of the child’s meals. Interviews were mostly carried out on weekday (75.1%), and a quarter took place during the weekend. A multi-step method was used in order to collect more precise information on diet [25]. This included 1) obtaining a quick or preliminary list of the foods and beverages consumed by the child, without specifying the order or time of consumption; 2) enquiring about commonly forgotten foods (predetermined list); 3) enquiring about meal time and the context in which the foods were eaten (place and activity during consumption); 4) recording detailed information about quantity and characteristics of the foods (food or beverage, consumed alone or along with other foods, ingredients used in preparation and quantities, preparation process); and finally, 5) carrying out a final revision and correcting information, if necessary.
The 24-h recall was carried out by trained personnel and standardized by researchers from INSP [24]. The 24-h recall software (multi-step methods, version 1.0, 2012; INSP) was developed and tested by INSP personnel for use in the 2012 ENSANUT.
Estimation of nutrient intake
Intake of vitamin C, total iron, heme iron, non-heme iron, calcium, and phytates (all in mg/d) and grams of red meat, poultry, fish, and seafood were estimated using the database on nutritional values developed by INSP [26]. Additionally, in order to estimate vitamin C and phytates losses by different cooking methods, retention factors for these dietary components were used [27, 28].
Cleaning process of diet information
A meat intake > + 3 SD was observed in 159 children and was considered implausible for the age group. For these children, we imputed mean meat consumption data by age and then recalculated the amount of heme iron, non- heme iron, and total iron consumed. A new estimate was made for the quantity of heme iron, non-heme iron, and total iron consumed. Children under 1 year of age were excluded from analyses (n = 411), as well as children who were partially breastfed (n = 107), due to the difficulty of estimating the quantity of breastmilk consumed. Values > + 3 SD or < − 3 SD of the logarithm distribution of the ratio between energy intake and energy requirement, were considered implausible and were excluded [24]. For nutrients, an upper boundary for plausible mineral intake was defined by multiplying the 99th percentile of the intake for each mineral by 1.5. When an intake value exceeded this upper boundary, we replaced it with a random value between the 95th percentile and the upper boundary value [8].
Biochemical indicators
A venous blood sample was obtained under fasting conditions by trained personnel and were handled according to recommended laboratory procedures for storage, preservation, and processing [23, 29]. Concentrations of SF and CRP were obtained using an automatic immunoassay analyzer (Abbott diagnostics, Wiesbaden, Germany) in the INSP nutrition laboratory. Children with CRP ≥5 mg/L (n = 275) were excluded from analyses, considering this was due to illness and could alter SF concentrations [30, 31].
Socioeconomic variables
Data on sex and age were obtained. As iron deficiency and its consequences are more severe in children < 2 years, children were classified in subgroups from 12 to 23 and 24–59 months [2, 4, 5]. Three geographical regions in Mexico were defined: North, Center and South. Rural areas were defined as having a population < 2500; the rest were considered as urban [22].
An index of socioeconomic status (SES) was created through the analysis of principal components, including household characteristics (number of rooms, exclusive kitchen, bathroom, use of firewood or coal as fuel, and floor material), goods and services at home (color television, microwave, washing machine, computer, motor vehicle, stereo, Internet access, cell phone, telephone line). A continuous variable was obtained and categorized in terciles (low, medium, high) [32]. Maternal education level was estimated by using the highest level of schooling, categorized as: 1) elementary school, 2) middle school, 3) high school, 4) bachelor’s degree or above.
Estimation of bioavailable iron
The percentage of FeBio was estimated with the algorithm created by Armah et al. [14], given it had previously been used with data from nationally representative surveys in preschoolers and considered individual body iron storage. The percentage of total bioavailability was estimated along with food consumption for all meals throughout the day. Consumption of black tea was low in the study population, so this inhibiting factor was not included in the algorithm [13]. As a first step, bioavailability of non-heme iron was estimated considering absorption enhancers (vitamin C and meats), absorption inhibitors of non-heme iron (phytates and calcium), and the concentration of SF per individual using the following equation:
Equation I. Estimation of percentage of non-heme iron bioavailability
Where: SF corresponded to serum ferritin (μg/L); VC to vitamin C (mg/d); M to meats (gr/d); Ph to phytates (mg/d); Ca to calcium (mg/d), and NHI to non-heme iron (mg/d).
Next, bioavailability of heme iron (HI) was estimated. According to body iron stores, two categories were defined: 1) adequate iron reserve (SF ≥12 μg/L), assuming a conservative bioavailability value of 25% for HI and 2) depleted iron reserve (SF < 12 μg/L), considering a HI bioavailability of 35% [16, 18].
As a second part of the algorithm, total iron bioavailability was estimated from the sum of the fraction of bioavailable NHI and HI with the following formula:
Equation II. Estimation of percentage of total iron bioavailability
Where: Bioavailability NHI corresponded to the percentage of bioavailability of non-heme iron estimated in the first formula I; proportion NHI to the proportion from total iron in the diet (non-heme iron); bioavailability HI to the bioavailability of heme iron (conservative value of 25–35%) and proportion HI to the proportion from total iron (heme iron).
Finally, once the bioavailability of non-heme iron was obtained with the algorithm created by Armah et al. [14], FeBio was estimated in relation to dietary intake of total iron with the following formula:
Equation III. Estimation of bioavailable iron (in mg)
Where: Bioavailability NHI corresponded to the percentage of bioavailability of non-heme iron estimated from the formula I; NHI to non-heme dietary iron (mg/d); bioavailability HI to heme iron bioavailability (conservative value of 25–35%), and HI to heme dietary iron (mg/d).
Statistical analysis
General characteristics of the study population are shown in proportions with confidence intervals (CI) at 95%. Using chi-square tests, statistically significant differences (p < 0.05) between sociodemographic factors (SES, maternal education level, area, and geographic region) by groups of age (12–23 and 24–59 months) were calculated.
Nutrient intake, concentration of serum ferritin, bioavailability of total iron and non-heme iron, heme FeBio, non-heme FeBio, and total FeBio are shown in mean ± SD, and medians. To determine mean differences in nutrient intake, statistical significance was set at p < 0.05, and the Bonferroni method was used to adjust for multiple comparisons [33]. To study the association between FeBio and sociodemographic factors, robust multiple linear regression modeling techniques were employed. FeBio was considered a dependent variable and SES, area, and geographic as covariates. A model was run for all children aged 12–59 months and two separate models for the groups 12–23 and 24–59 months old. The northern region, urban area, and low SES were the reference categories. We verified the normality and homogeneity of residual variance, in addition to multicollinearity between independent variables in the models. We excluded the variable mother’s education due to collinearity with SES. Analyses were performed using the logarithmic transformation of FeBio. Results were similar to the untransformed variable. To facilitate the interpretation of results, we used the untransformed variable. We used the STATA software, version 14.0, (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP.), and adjusted by sampling design of the survey, with SVY module.
Results
We analyzed information from 1012 children between 12 and 59 months of age who had data on diet and body iron storage indicators. Approximately half were male (48.9%), most lived in urban areas (66.2%) and in the central region and Mexico City (41.8%), 40% had a middle SES, followed by those with low SES (36.2%).
A high proportion of mothers had a middle school education level (43.1%). The sociodemographic variables (area, region, SES, and mother’s education level) were not different between the two age groups (Table 1).
In the total sample, consumption of total iron and calcium was lower and consumption of phytates were higher in rural areas (compared to urban areas), and among children from low SES (compared with high SES) (p < 0.05). On the other hand, children from high SES had a higher intake of vitamin C than those from low and medium SES (p < 0.05), and children residing in urban areas had higher meat consumption (p < 0.05). No differences were observed for the intake of absorption enhancers (vitamin C and meats) or non-heme iron absorption inhibitors (phytates and calcium) between regions of residence (Table 2). Vitamin C and phytates intake were slightly higher when losses by cooking method were not considered (80 mg and 700 mg/d of vitamin C and phytates, respectively) (data not showed in table).
In children aged 12–23 months, no differences were observed in the mean intake of enhancers or inhibitors of non-heme iron absorption between sociodemographic characteristics.
Children aged 24–59 months from rural areas with low SES consumed less total iron, vitamin C, and calcium and had a higher consumption of phytates, while the highest meat consumption was in children with a high SES (p < 0.05) (Table 2).
The mean intake of total iron by age group was 7.48 and 9.47 mg/d in children aged 12–23 months and 24–59 months, respectively (Table 3). The total estimated FeBio was 0.75 ± 0.73 mg/d in the total sample, corresponding to a bioavailability of 9.15 ± 5.36%. The main source of FeBio was non-heme iron (0.68 ± 0.70 mg/d), with a bioavailability of 8.33 ± 5.08%. In children aged 24–59 months, total intake of FeBio was 0.74 ± 0.71 mg/d, corresponding to a bioavailability of 8.74 ± 4.83%, which was similar to the estimated bioavailability in the total sample.
In children aged 12–23 months, bioavailability tended to be higher (12.03 ± 7.83%), as did FeBio (0.81 ± 0.76 mg/d) (Table 3).
Country regions were not associated with FeBio consumption in any of the three regression models. In 12 to 23-month-old children, we only found differences in the intake of FeBio by area of residence, with 0.276 mg/d less FeBio intake in rural areas versus children in urban areas (p < 0.05). In addition, this negative association was also observed in the total population, with 0.113 mg/d less FeBio intake in children from rural areas compared to urban areas (p < 0.05) (Table 4).
In the total population, children with a middle SES consumed 0.123 mg/d and children with a high SES consumed 0.173 mg/d more FeBio than low SES (p < 0.05). In 24 to 59-month-old children, only differences in children with high SES were observed, with a greater intake of 0.158 mg/d FeBio in comparison to low SES (p < 0.05) (Table 4).
Discussion
In this study, we found that the estimated intake of FeBio in Mexican children between 12 and 59 months of age was low (less than 1 mg/d) and was negatively associated with a low SES and residing in a rural area. We also found that dietary iron bioavailability was less than 10%. These results are due the following: 1) the majority of iron consumed in our population was non-heme, for which the bioavailability is much lower than heme iron; 2) there is a high consumption of iron absorption inhibitors, phytates and calcium, and low consumption of meat, which promotes iron absorption.
When the fraction of bioavailable heme and non-heme iron were added, a total bioavailability of 9.15 ± 5.36% was obtained, which differs from the estimated bioavailability in the United States population (15.1%) [11]. The bioavailability of iron is important to correctly estimate requirements for this nutrient. When assuming a low iron bioavailability (5.5% in children aged 1–3 years and 7.5% in children aged 4–5), estimates done with data from the Mexican National Nutrition Survey (ENN) 1999), the prevalence of iron deficiency in Mexican preschoolers was 52% [8, 34]. However, assuming a bioavailability of 18% (recommended in United States and Canada), the prevalence of iron deficiency is underestimated by 5% [8, 10]. We found that the prevalence of iron deficiency, considering the bioavailability in the present study, is 45%.
The estimated FeBio intake (0.74–0.81 mg/d) is slightly higher than previous estimates in Mexican preschool children, with data from the 1999 ENN (0.14–0.37 mg/d) [13]. Diverse factors could be contributing to the differences between estimates: 1) the instrument and methodology used for data collection were different, as in the present study a multi-step method was used, allowing for a better record of consumed foods [8, 24, 25]; 2) the algorithm applied included the concentration of SF per individual [14], whereas in 1999, three different scenarios of iron reserves were used because a ferritin measurement was not available [13]; 3) a possible change in iron intake in the past 13 years could be due to a greater consumption of fortified foods [8, 35, 36]; 4) the implementation of government programs, such as the Liconsa milk supply program (milk fortified with iron and other micronutrients), could be contributing to an improved iron status in children [36,37,38].
Despite increases in iron bioavailability, FeBio continues to be low, given that only 4.6% of total dietary iron is heme iron, while, in other populations, heme iron represents > 10% of total dietary iron [8, 14, 16]. It is because in 2012, 31% of households had food insecurity, which limited meat consumption within other expensive food groups [39]. There was no difference in FeBio intake between different regions in Mexico, which is largely explained by the fact that consumption of meats, vitamin C, phytates, and calcium is not different between age groups. Similar to previous studies, consumption of total iron, phytates, and vitamin C were not significantly associated with SF concentration [40].
In our analyses, there were no significant differences in FeBio intake by sex (data not shown). Children iron deficiency is reported to be attributed to factors such as muscle and blood volume increase due to rapid growth, a diet low in high available iron (heme), elevated consumption of cow’s milk, and loss of intestinal blood from parasitism, in both boys and girls [41]. Furthermore, conditions such as inflammation, vitamin deficiency, obesity, and genetic factors contribute to differences in iron absorption among individuals [12].
As our findings in the total sample suggest, living in a rural area and having a low SES are negatively associated with FeBio. In rural areas of Mexico, the traditional diet, rich in cereals and legumes, is largely consumed, representing an important source of iron and of iron absorption inhibitors [7, 8, 42]. FeBio is lower in individuals from the lowest SES terciles, which could be due to a lower mean consumption of iron absorption enhancers (meat and vitamin C) in these groups. Other studies indicated a lower consumption of fruits, vegetables (an important source of vitamin C), and red meats in individuals with a low SES, in addition to a higher consumption of energy-dense foods with low nutritional quality [20, 43].
Some strategies to increase bioavailable iron are: combination of beans or other legumes in the same meal with foods that facilitate iron absorption (citrus fruit, 100% natural juices and vegetables) [44]. Appropriate cooking methods (fermentation, sourdough preparation, soaking, and discarding soaking water) has also been effective to reduce content of phytates in whole foods [12, 45].
Our study presents some limitations. First, we performed a secondary analysis from the 2012 ENSANUT data. However, unlike clinical studies, our results can be extrapolated to the general population and provide information for health and nutrition policies. Second, the use of only a 24-h recall and a possible overestimation of the prevalence of iron deficiency. Nonetheless, the 24-h multi-step recall method minimizes omission of forgotten foods and improves diet estimates [25]. Third, not adjusting the calcium and iron intake for losses for cooking methods. However, we consider that the lack of adjustment for losses of these two minerals does not change the direction of the results, since the highest cooking losses for calcium and iron are found in vegetables ~ 24% of the total losses, and a high proportion of Mexican children < 48 months do not consume vegetables (80%) [43]. For iron, losses by cooking oscillate between 5 and 10% in the different food [27, 46]. Fourth, information on dietary supplements was not collected in this sample of children, which would have been useful to have a better estimate of the iron intake.
The strengths of the study include the use of an algorithm developed with national data, proved useful for estimating iron bioavailability in population groups [11]. Another strength is the estimation of vitamin C and phytates intakes by adjusting for losses in relation to the different cooking methods used. This adjustment provided a better estimate of the total bioavailable iron [28]. Furthermore, to the best of our knowledge, few studies have estimated FeBio in preschool children’s overall diet at a national level, in a representative manner.
Conclusions
In conclusion, the estimated FeBio in Mexican children was low. Rural areas and low SES were negatively associated with FeBio intake. From a public health standpoint, identifying dietary factors that hinder or promote iron bioavailability in groups with certain sociodemographic characteristics will allow for the design of targeted interventions to improve consumption of bioavailable iron. In light of the present findings, future studies should review iron intake recommendations in the Mexican population.
Availability of data and materials
The dataset used for analysis is available from the corresponding author on reasonable request.
Abbreviations
- CRP:
-
C-reactive protein
- ENN:
-
National Nutrition Survey
- ENSANUT:
-
National Health and Nutrition Survey
- FeBio:
-
Bioavailable iron
- HI:
-
Heme iron
- INSP:
-
National Institute of Public Health (Instituto Nacional de Salud Publica)
- M:
-
Meat
- NHI:
-
Non-heme iron
- Ph:
-
Phytates
- SES:
-
Socioeconomic status
- SF:
-
Serum ferritin
- VC:
-
Vitamin C
References
WHO. The global prevalence of anaemia in 2011. Geneva: World Health Organization; 2015.
Villalpando S, De la Cruz-Góngora V, Shamah-levy T, Rebollar R, Contreras-Manzano A. Nutritional status of iron , vitamin B12 , folate , retinol and anemia in children 1 to 11 years old . Results of the Ensanut 2012. Salud Publica Mex. 2015;57(5):372–84.
Lozoff B. Iron deficiency and child development. Food Nutr Bull. 2007;28(4):s560–9.
Lozoff B, Beard J, Connor J, Barbara F, Georgieff M, Schallert T. Long-lasting neural and behavioral effects of irondeficiency in infancy. Nutr Rev. 2006;64(5 Pt 2):S34–91.
Beard JL, Murray-Kolb LE, Haas JD, Lawrence F. Iron absorption prediction equations lack agreement and underestimate iron absorption. J Nutr. 2007;137(7):1741–6.
Grantham-McGregor S, Ani C. A review of studies on the effect of iron deficiency on cognitive development in children. J Nutr. 2001;131(2):649S–68S.
Fairweather-Tait SJ. Bioavailability of trace elements. A review. Food Chemistry. 1992;43:213–7.
Sanchez-Pimienta TG, Lopez-Olmedo N, Rodriguez-Ramirez S, Garcia-Guerra A, Rivera JA, Carriquiry AL, et al. High prevalence of inadequate calcium and iron intakes by mexican population groups as assessed by 24-hour recalls. J Nutr. 2016;146(9):1874S–80S.
De Carli E, Dias GC, Morimoto JM, Marchioni DML, Colli C. Dietary iron bioavailability: agreement between estimation methods and association with serum ferritin concentrations in women of childbearing age. Nutrients. 2018;10(5):650.
Institute of Medicine (US) Panel on Micronutrients. Dietary Reference Intakes for Iron and Zinc. Washington: National Academies Press (US); 2001.
Armah SM, Carriquiry AL, Reddy MB. Total iron bioavailability from the US diet is lower than the current estimate. J Nutr. 2015;145(11):2617–21.
Hurrell R, Egli I. Iron bioavailability and dietary reference values. Am J Clin Nutr. 2010;91(5):1461S–7S.
Rodríguez SC, Hotz C, Rivera JA. Bioavailable dietary iron is associated with hemoglobin concentration in mexican preschool children. J Nutr. 2007;137(10):2304–10.
Armah SM, Carriquiry A, Sullivan D, Cook JD, Reddy MB. A complete diet-based algorithm for predicting nonheme iron absorption in adults. J Nutr. 2013;143(7):1136–40.
Gleerup A, Rossander-Hulthén L, Gramatkovski E, Hallberg L. Iron absorption from the whole diet: comparison of the effect of two different distributions of daily calcium intake. Am J Clin Nutr. 1995;61(1):97–104.
Hallberg L, Hulthén L. Prediction of dietary iron absorption: an algorithm for calculating absorption and bioavailability. Am J Clin Nutr. 2000;71(5):1147–60.
Tetens I, Larsen TM, Kristensen MB, Hels O, Jensen M, Morberg CM, et al. The importance of dietary composition for efficacy of iron absorption measured in a whole diet that includes rye bread fortified with ferrous fumerate: a radioisotope study in young women. Br J Nutr. 2005;94(5):720–6.
Bhargava A, Bouis HE, Scrimshaw NS. Community and international nutrition dietary intakes and socioeconomic factors are associated with the hemoglobin concentration of bangladeshi women. J Nutr. 2001;131(3):758–64.
Batis C, Aburto TC, Sánchez-Pimienta TG, Pedraza LS, Rivera JA. Adherence to dietary recommendations for food group intakes is low in the Mexican population. J Nutr. 2016;146(9):1897S–906S.
Leroy JL, Habicht J-P. González de Cossío T, Ruel MT. maternal education mitigates the negative effects of higher income on the double burden of child stunting and maternal overweight in rural Mexico. J Nutr. 2014;144(5):765–70.
Gonzalez de Cosio T, Escobar-Zaragoza L, Gonzalez-Castell D, Rivera-Dommarco JA. Prácticas de alimentación infantil y deterioro de la lactancia materna en México. [infant feeding practices and deterioration of breastfeeding in Mexico]. Salud Publica Mex. 2013;55(2):S170–9.
Gutierrez J, Rivera-Dommarco J, Shamah-Levy T, Villalpando S, Franco-Núñez A, Cuevas-Nasu L, et al. Encuesta Nacional de Salud y Nutrición 2012. Resultados Nacionales. [National Health and nutrition survey 2012. National Results] Cuernavaca, México; 2012.
Romero-Martínez M, Shamah-Levy T, Franco-Núñez A, Villalpando S, Cuevas-Nasu L, Pablo Gutiérrez J, et al. Encuesta nacional de salud y nutrición 2012: diseño y cobertura. [National Health and nutrition survey 2012: design and coverage]. Salud Publica Mex. 2013;55(2):S332–40 (in Spanish).
Lopez-Olmedo N, Carriquiry AL, Rodriguez-Ramirez S, Ramirez-Silva I, Espinosa-Montero J, Hernandez-Barrera L, et al. Usual intake of added sugars and saturated fats is high while dietary fiber is low in the Mexican population. J Nutr. 2016;146(9):1856S–65S.
Conway J, Ingwersen L, Moshfegh A. Effectiveness of the USDA 5-step multiple-pass method to assess food intake in obese and non-obese women. Am J Clin Nutr. 2003;77(11):71–8.
Instituto Nacional de Salud Publica. Base de datos de valor nutritivo de los alimentos. [National Institute of public health. Food composition table.]. Cuernavaca: Compilación del Instituto Nacional de Salud Publica [National Institute of Public Health]; 2012.
USDA. USDA table of nutrient retention factors release 6; 2007. Available from: https://data.nal.usda.gov/dataset/usda-table-nutrient-retention-factors-release-6-2007.
Gupta RK, Gangoliya SS, Singh NK. Reduction of phytic acid and enhancement of bioavailable micronutrients in food grains. J Food Sci Technol. 2015;52(2):676–84.
Shamah-Levy T, Villalpando-Hernández S, Rivera-Dommarco JA. Manual de procedimientos Para proyectos de nutrición. Centro de Investigación en Nutrición y Salud, Instituto Nacional de Salud Pública / 2006. [procedures manual for nutrition projects]. Cuernavaca: Nutrition and Health Research Center, National Institute of Publica Health]; 2006.
Thurnham DI, McCabe LD, Haldar S, Wieringa FT, Northrop-Clewes CA, McCabe GP. Adjusting plasma ferritin concentrations to remove the effects of subclinical inflammation in the assessment of iron deficiency: a meta-analysis. Am J Clin Nutr. 2010;92(3):546–55.
WHO, CDC. Assessing the iron status of populations. Annex 2: indicators of the iron status of populations: ferritin. Geneva: World Health Organization; Centers for Disease Control and Prevention; 2007.
Gutiérrez JP. Clasificación socioeconómica de los hogares en la ENSANUT 2012. [socioeconomic classification of households in ENSANUT 2012]. Salud Publica Mex. 2013;55:S341–6.
Bland JM, Altman DG. Multiple significance tests: the Bonferroni method. BMJ. 1995;310(6973):170.
Rivera-Dommarco JÁ, Hotz C, Rodriguez-Ramirez S, Garcia-Guerra A, Perez-Exposito A, Martinez H. Hierro. In: Recomendaciones de ingestión de nutrimentos Para la población mexicana [recommendations of intake of nutrients for the Mexican population]. México: Editorial Medica panamericana; 2005. p. 247–64.
Mundo-Rosas V, Rodríguez-Ramírez S, Shamah-Levy T. Energy and nutrient intake in Mexican children 1 to 4 years old: results from the Mexican National Health and nutrition survey 2006. Salud Publica Mex. 2009;51:S530–9.
Shamah-Levy T, Méndez-Gómez-Humarán I, Gaona-Pineda EB, Cuevas-Nasu L, Villalpando S. Food assistance programmes are indirectly associated with anaemia status in children under 5 years old in Mexico. Br J Nutr. 2016;116(6):1095–102.
Barquera-Cervera S, Rivera-Dommarco J, Gasca-García A. Food and nutrition policies and programs in México. Salud Publica Mex. 2001;5:464–77.
Rivera JA, Shamah T, Villalpando S, Monterrubio E. Effectiveness of a large-scale iron-fortified milk distribution program on anemia and iron deficiency in low-income young children in Mexico. Am J Clin Nutr. 2010;91(2):431–9.
Cuevas-Nasu L, Rivera-Dommarco JA, Shamah-levy T. Inseguridad alimentaria y estado de nutrición en menores de cinco años de edad en Mexico. [Food insecurity and nutritional status in children under five years of age in Mexico]. Salud Publica Mex. 2014;56(2):47–53.
Morales-Rúan M, Villalpando S, García-Guerra A, Shamah-Levy T, Robledo-Pérez R, Ávila-Arcos MA, et al. Iron, zinc, copper and magnesium nutritional status in Mexican children aged 1 to 11 years. Salud Pública de Mex. 2012;54:125–34.
Subramaniam G, Girish M. Iron deficiency anemia in children. Indian J Pediatr. 2015;82(6):558–64.
Rivera JA, Pedraza LS, Aburto TC, Batis C, Sanchez-Pimienta TG, Gonzalez de Cosio T, et al. Overview of the dietary intakes of the Mexican population: results from the National Health and nutrition survey 2012. J Nutr. 2016;146(9):1851S–5S.
Deming DM, Afeiche MC, Reidy KC, Eldridge AL, Villalpando-Carrión S. Early feeding patterns among Mexican babies: Findings from the 2012 National Health and Nutrition Survey and implications for health and obesity prevention. BMC Nutr. 2015;1(40):1-14.
Platel K, Krishnapura S. Bioavailability of micronutrients from plant foods: an update. Food Sci Nutr. 2016;56(10):1608–19.
Moretti D. Plant-based diets and iron status. Vegetarian and Plant-Based Diets in Health and Disease Prevention. 1st ed. London: Academic Press; 2017. p. 715–27.
Bell S, Becker W, Vásquez-Caicedo A, Hartmann B, Møller A, Butriss J. Report on nutrient losses and gains factors used in European food composition databases. Karlsruhe: EuroFIR; 2006. Available from: http://www.langual.org/Download/RecipeCalculation/Belletal-ReportonNutrientLossesandGainsFactorsusedinEuropeanFoodCompositionDatabases.pdf.
Acknowledgements
The authors thank Cloe Rawlinson for the English language editing.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
SRR conceptualized and designed the research; YVA and EMF analyzed the data; YAV and SRR wrote the paper; AGG gave key insights for the final manuscript; YVA and SRR had primary responsibility for final content. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The research, biosecurity, and ethics committees of the National Institute of Public Health (INSP, by its Spanish acronym) in Cuernavaca, Morelos, Mexico, approved the 2012 ENSANUT. The parents or guardians of the children signed an informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare having no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Venegas-Aviles, Y., Rodríguez-Ramírez, S., Monterrubio-Flores, E. et al. Sociodemographic factors associated with low intake of bioavailable iron in preschoolers: National Health and Nutrition Survey 2012, Mexico. Nutr J 19, 57 (2020). https://doi.org/10.1186/s12937-020-00567-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-020-00567-3