
Abstract
Background
Lectures remain an important teaching method to present and structure knowledge to many students concurrently. Adequate measures are necessary to maintain the quality of the lectures. The aim of this study was to determine the impact on the lecture quality using written structured feedback and to compare the ratings of surgical lectures between students and surgical peers.
Methods
Prospective analysis of two consecutive surgical lecture series for undergraduate students at Goethe-University Medical School was performed before and after evaluation of the lecturers via independent written feedback from trained undergraduate students and surgeons. The 22-item feedback instrument covered three areas of performance: content, visualization, and delivery. Additional suggestions for improvement were provided from both students and surgical peers who anonymously attended the lectures. The lecturers, experienced surgeons, as well as the student and peer raters were blinded in terms of the aim and content of the study. Their response to the feedback was collected using a web-based 13-item questionnaire.
The Kendall’s-W coefficient was computed to calculate inter-rater reliability (IRR). Differences between ratings before and after feedback were analyzed using Student’s t-test for dependent samples. The Kolmogorov-Smirnov-test was used for independent samples.
Results
A total of 22 lectures from a possible 32 given by 13 lecturers were included and analyzed by at least three surgeons and two students. There were significant improvements in overall score as well as in the details of 9 of the 13 items were found. The average inter-rater reliability was 0.71. There were no differences in the ratings as a function of the rater’s level of expertise (peers vs. students).
We found that 13/23 lecturers (56.5%) answered the questionnaire, and 92% strongly agreed that the written feedback was useful. 76.9% of the lecturers revised their lecture based on the written feedback requiring on average 112.5 min (range from 20 to 300 min).
Conclusions
Overall, this study indicates that structured written feedback provided by trained peers and students that is subsequently discussed by the lecturers concerned is a highly effective and efficient method to improve aspects of lecturing. We anticipate that structured written feedback by trained students that is discussed by the lecturers concerned will improve lecturing.
Similar content being viewed by others


Background
Often criticized by teachers and students, lectures are still meaningful in medical education and are an efficient method of teaching [1–4]. Lectures are even more important with high student numbers because the lecturer can present information to many students at the same time and with the same learning outcome regardless of the number of students [5]. Furthermore students can learn from the lecturer’s experience and can discuss academic issues with her or him, and the lecturer can help them to prepare themselves for the faculty’s exams [1]. Medical knowledge continuously increases and is now available from everywhere via the internet. Thus, lectures can help the students to structure, assess and synchronize the available information based on the lecturers’ priorities. However, lectures can definitely be boring or demotivating if badly prepared. Thus, many authors analyze the quality criteria of successful lecturing [1, 5–10] including:
To improve one’s own teaching quality - especially regarding lecturing - a critical self-reflection of one’s own performance is necessary. Here, feedback plays an important role, because it improves knowledge and competence and helps to reflect on one’s performance [12–15].
However, non-specific, unclear, and irrelevant feedback is useless and may hinder the learning process [13].
Thus, feedback must fulfill defined quality criteria to be successful [12, 16, 17]. It must be constructive, specific and offer concrete suggestions for improvement [12, 17]. Furthermore it should be based on direct observations and be made timely [17, 18].
The easiest way to give feedback is orally. Direct talk between the person offering feedback and the receiver can be initialized via oral feedback. This feedback should be timely because important aspects might be forgotten if delayed due to the spontaneous character of oral feedback [19].
Another way of giving feedback is written feedback. It provides an enduring record and reference point that can be taken home [19]. This allows the receiver (e.g. the lecturer) to reflect on it repetitiously and to reread the personal feedback while they revise their lectures [11]. It also allows the receivers to directly compare with others [19]. Haghani et al. demonstrated that written feedback had a higher learning effect than oral feedback [20]. However, written feedback requires a time consuming preparation [19].
Feedback on teaching quality by peers has been shown to be very successful in terms of improving teaching quality. It is highly accepted by feedback providers and recipients [21–28].
Despite the advantages of peer feedback, students must realize the structure, learning objectives and aims of the lectures. The content and context must be presented more clearly to students than experts. Thus, their feedback is critical. On the other hand, student’s evaluations are influenced by many factors that cannot be influenced by the lecturer and lecture’s quality including age [29], expected grades in the relating tests [30], intrinsic motivation or general interest in the topic [31]. In fact, the lecture rating by students is often influenced by how entertaining the lecture is. Thus, a combination of student and peer feedback might be reasonable.
The aim of this study is to analyze if student and expert raters are using the feedback sheet differently and to measure the impact of written, structured feedback on the quality of a lecture series in surgery for undergraduate medical students. We also want to analyze the lecturers’ response to this kind of feedback.
Methods
Study design
This study has a prospective design and analyzed the effect of structured written feedback given by students and peers on the lecture quality of a surgical lecture series for undergraduate medical students. The study was conducted according to ethical principles of the Helsinki Declaration (Ethical Principles for Medical Research Involving Human Subjects) and was approved by the ethics committee of the medical faculty of the Goethe University, Frankfurt, Germany.
Study protocol
The lecture series is part of the surgical curriculum for undergraduate medical students at Frankfurt Medical Faculty [32]. It takes place twice a year over an 8-week period for 4th year students in a six-year program. It consists of 32 lectures with a duration of 90 min each. The lectures cover the main topics in surgery as defined in the catalogue of learning objectives from the German Society of Surgery [33]. Table 1 shows the distribution of surgical disciplines.
The students’ attendance of the lectures is optional. However, the lecture series ends with an obligatory 50 item multiple-choice examination. Passing the examination is a prerequisite for participating in the following courses in the curriculum.
The lectures are given by experienced surgeons from the University hospital. They participate in undergraduate surgical training as part of their role as a medical teacher. Data were obtained from all lecturers regarding age and years of lecturing experience. The evaluation of all courses is a mandatory component based on the national regulations to study medicine. Still, lecturers were informed over the particular evaluation which was performed in all surgical lectures and had the possibility to dissent the use of their evaluation data for study purpose. Lecturers were blinded regarding the contents of the evaluation process and aim of the study.
Measurement
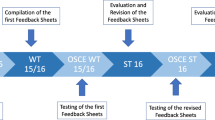
The study took place from April to June 2014 (lecture series 1) and October to December 2014 (lecture series 2). The evaluation sheet used was described by Ruesseler et al. [25] and is based on the publications by Newman [34, 35] as well as the quality criteria for lectures published in the literature [1, 5, 6]. Additional file 1 The 22- item instrument was divided into three categories: content/structure (10 items), visualization (5 items) and presentation (7 items). Each item was rated on a 5-point Likert scale (from 1 = did not show to 5 = excellent) with descriptive benchmarks for excellent (5), adequate (3) and poor performance (1) for each item [25, 34, 35]. Furthermore, each rater had to document the timetable of each lecture and describe the strength of each lecture and give suggestions for improvement.
The reviewer team consisted of 4 surgeons (peers) and 3 undergraduate medical students. The students attended the lecture series regularly; however, they received a compensation of 10 € per hour for participating as a reviewer. The reviewers were blinded for the study aim. To increase the inter-rater reliability, all reviewers received a two-hour training prior to the first and the second lecture series [25, 34]. During this training, they rated a videotaped lecture using the evaluation sheet. Afterwards, they discussed definitions, items, and their results with each other and talked about common rater errors (e.g. halo-effect).
Each of the 32 lectures was evaluated by at least two raters—one student and one surgeon (peer). They rated the lecture simultaneously and independently without agreement. Both lecture series were rated similarly. All student raters and most peers changed after the first lecture series to minimize the rerun bias.
All lecturers received standardized written feedback on their lecturing performance for each lecture three weeks prior to the second lecture series. For this, all ratings of a single lecture were averaged to a single score for each item on the assessment sheet. In their written feedback, each lecturer received the mean score of all lecturers for each item, the best and the worst score of all lecturers, as well as his own averaged score for each item. Furthermore, they received the timetable of their lecture and their lecture’s strengths and suggestions for improvement—especially for poorly scored items.
The results were anonymously presented and discussed during the monthly meeting of surgical medical teachers. The second lecture series was assessed and analyzed as described above. The lecturers’ reaction to the feedback was collected using a web-based questionnaire consisting of 13 items. The questionnaire was sent to all lecturers via email after their second lecture and prior to receiving their second feedback. A reminder to take the survey was sent after two weeks.
The dataset supporting the conclusions of this article and the evaluation sheet is included within the article and its additional files.
Statistical analysis
Statistical analysis used Microsoft Excel (Microsoft Corporation, Redmond, USA) for the personal characteristics of raters and lecturers and evaluation. SPSS Statistics version 19 (IBM, Armonk, USA) was used for the checklist results. After verifying the Gaussian distribution of the data, the values were presented as the mean ± standard deviation. The Kendall’s W coefficient was computed to calculate the inter-rater reliability (IRR). The rating differences before and after the feedback were analyzed using Student’s t-test for dependent samples as well as the Wilcoxon signed-rank test. For independent samples, we used the Student’s t-test for independent samples and the Kolmogorov-Smirnov test for independent samples.
Results
Each lecture series consisted of 32 lectures. For some lecture topics, the lecturer changed between series 1 and 2. These lectures were excluded from the study. Thus, a total of 22 lectures by 13 lecturers were included and analyzed. The epidemiological data of the lecturers are presented in Table 1.
Four surgeons (peers) (3 in series 1 and 4 in Series 2) and 3 undergraduate medical students (1 in series 1 and 2 in Series 2) were part of the reviewer team. The epidemiological data of the surgeons are presented in Table 1. The lectures were evaluated by 1.22 expert raters on average (maximum 3, minimum 0) and by 1.13 student raters on average (maximum 2, minimum 0).
Impact on content, structure and quality of the lectures
Figure 1 shows the overall results for series 1 and series 2 as well as the results for the three main categories. Significant improvements were found in the overall score and in the category ‘content/structure’. In the category ‘presentation’, the results tended to improve, but no significant changes were found. In the category ‘visualization’, the lecturers achieved good results similar to series 1. In this category, the results remained high without significant changes.

Mean rating of the evaluation in series 1 and series 2. Presented as mean ± std. dev. for the overall score and the main categories. Each item was rated on a 5-point Likert scale (from 5 = excellent to 1 = poor). In light grey ‘point of measurement 1’; in dark grey ‘point of measurement 2’; * p < 0.05; ** p < 0.01; ns p > 0.05
The detailed results for each item are presented in Table 2. For 9 items, we found significant differences in the scores after written feedback. Most of these were in the category ‘content/structure’. In the ‘presentation’ category, we found significant changes in two items. No significant changes were found in the category ‘visualization’.
There were no significant changes in the average length of the lectures from the first to the second lecture series (86.43 min ±5.78 in series 1 and 85.78 min ±11.21in series 2). The average length was 85 min for both series.
Inter-rater reliability
To determine the IRR of the lecture series evaluation, the results of all lectures were used (independent of study inclusion of the lecturer). The IRR (Kendall W) was 0.70 ± 0.12 on averaged for all reviewed lectures and 0.71 ± 0.11 for the included lectures. It was above 0.6 in 81% of the lectures. In 19%, it was between 0.4 and 0.6. For lecture series 1, the IRR was above 0.6 in 28 of the 29 lectures. It was between 0.4 and 0.6 in 1 of 29 lectures. In lecture 2, the IRR was above 0.6 for 20 of the 30 lectures and between 0.4 and 0.6 for 10 of the 30 lectures. None of the IRR values were below 0.4.
There were no differences in the ratings as a function of the rater’s level of expertise (peers vs. students) (Table 3).
Results of the questionnaire
We found that 13 of the 23 lecturers (56.5%) answered the questionnaire. Whilst more than 92% strongly agreed or agreed with the statement ‘In total, I rate the written feedback as beneficial’, only one lecturer disagreed (Fig. 2).

Results of lecturers’ questionnaires. Presented as a 6-point-Likert-Scale
76.9% of the lecturers reported that they revised their lecture based on the written feedback requiring on average 112.5 min (range from 20 min to 300 min). They stated that the precise recommendations for improvement were extremely useful.
Discussion
Feedback is essential for learning [12–15, 36]. In this study, we demonstrated the effects of structured written feedback given by students and peers on a lecture series in surgery. The strongest improvement from the written feedback was shown in the category content/structure—especially regarding the items “Presents goal of the talk” or “Providing a clear algorithm”. These are essential for the students as they improve learning aptitude [1].
Ruesseler et al. hypothesized that improvements in the category “Presentation” can only be achieved after didactical training based on the results of their study [25]. In contrast to these findings, we demonstrate improvements in the category “Presentation”, especially for the items “Speech flow” and “Invitation to questions”. We found that these results as well as “Time management” increased significantly. In our opinion, this is one of the main reasons for the increased results—the lecturers simply had more time to take care of the speech flow because of more effective time management. In addition, the lecturers in Ruesseler et al. already achieved superior results in this category by the first lecture series. Thus, it was more difficult to improve here because their results were already good.
Consistent with previous findings [11, 22–24, 37] we demonstrated the high acceptance of feedback given by peers—even if the lecturers were blinded regarding the evaluation process. Most lecturers rated the written feedback as beneficial and revised their lectures after the feedback. Unlike these existing studies, we decided to blind the lecturers under evaluation. Thus, we could measure the unadulterated effect and reaction to the feedback without biasing it by only evaluating those lecturers willing to be evaluated. This could correspond to those who were already motivated to teach effectively. However the generalizability of the questionnaire results is limited because only as 56% of our lecturers responded to the questionnaire.
On the other hand, the risk of negative reactions to unheralded feedback is much higher. Consistent with the findings of Eraut et al. [12], we were confronted with some misinterpretations of the intended feedback - especially for “Presentation”, e.g., one lecturer misunderstood some items as an estimation of his own personal behavior. To minimize these misapprehensions, many authors describe pre-observation meetings [22, 23, 38, 39]. Even if we decided not to hold these meetings because of the reasons described above, we will proceed with the evaluations of the lectures in this lecture series—future lecturers will be informed about the ongoing evaluation. Thus, based on the lecturer’s evaluation on the past lecture series, the reviewers and lecturers harmonized topics of personal interest via the following evaluation.
Each lecturer received written feedback consisting of his own evaluation embedded within the anonymized results of the best and worst lecturer as a ranking. Following the first feedback and a growing discussion between the lecturers regarding their ratings, we observed a growing competition between the lecturers. That is, “If Prof. X has a case presentation and is well rated, then I’ll do the same!” This competition can highly improve a lecture if the lecturer uses the written standardized feedback. However, it can also be disadvantageous, e.g., one of the lecturers focused only on improving his presentation of learning objectives. The outcome here was a lecture that presented the importance of learning objectives and his learning objectives of the present lecture for about 20 min. This caused him to run out of time for remainder of his lecture, which he did not revise. On the other hand, those lecturers who already achieved good results and who were best ranked in comparison to all other lecturers did not see the necessity to change.
We showed high IRR between all reviewers using the standardized evaluation sheet. However, this might be a limitation because not all reviewers changed after the first lecture series. Thus, these reviewers could be biased by their experiences in the first lecture series. This bias was not seen because of the high IRR between all reviewers—both expert and student groups as well as persisting and interchanged reviewers.
Based on our results, we demonstrated that the results and quality of the evaluation are not influenced by the reviewers’ level of training when using a standardized evaluation sheet as presented here. Our study shows that even student ratings based on a validated evaluation sheet are comparable to evaluations created by peers using the same metric. We confirmed that the bias in student evaluations as emphasized in the literature [29–31] can be minimized using a validated questionnaire and reviewer training. The training does not need to be longer than an hour. This method is an efficient option for a good and valid evaluation/feedback and thus we decided to have further evaluations done only by trained students. This facilitated evaluations with lower personnel costs. In an upcoming project, we will evaluate if the positive impact of this kind of feedback will be persistent when only students provide feedback.
This study is limited in that we did not analyze the effects of the revised lectures on students’ medical knowledge acquisition. To the best of our knowledge, such a study has not yet been conducted yet—perhaps because of the challenges inherent in designing such a study, e.g. designing a test with comparative difficulty and comparative tested learning objectives in two consecutive semesters without the two student groups exchanging the test items. Another limitation is the lack of a control group. Because of the small number of lecturers in the lecture series, we made a conscious decision to not create a control group. Other than these limits, the effectiveness of any type of feedback compared to giving no feedback is already proven. Thus, the control group would have been disadvantaged from the beginning.
In this study, lecturers who received good evaluations asked for a certificate of their teaching performance within this lecture series. They suggested that they needed tribute for being a good teacher from the faculty. This is consistent with the results of Müller-Hilke [40]. She demonstrated that medical teachers’ highest motivation is “Fame and glory”. To boost the tribute to excellent teaching, the educational committee of the department of surgery at our faculty decided to perpetuate the evaluation and to implement an award for the most highly evaluated lecturer as well as the best evaluated department.
Conclusions
Overall, this study indicates that structured written feedback provided by trained peers and students and discussed by the lecturers concerned is a highly effective and efficient method to improve aspects of lecturing. We anticipate that structured written feedback by trained students and discussed by the lecturers concerned will improve lecturing.
Abbreviations
- IRR:
-
Inter-rater reliability
References
Brown G, Manogue M. AMEE Medical Education Guide No. 22: Refreshing lecturing: A guide for lecturers. Med Teach. 2001;23(3):231–44.
Charlton BG. Lectures are such an effective teaching method because they exploit evolved human psychology to improve learning. Med Hypotheses. 2006;67(6):1261–5.
Graffam B. Active learning in medical education: Strategies for beginning implementation. Med Teach. 2007;29(1):38–42.
Charlton BG. Science school and culture school: Improving the efficiency of high school science teaching in a system of mass science education. Med Hypotheses. 2006;67(1):1–5.
Gelula MH. Effective lecture presentation skills. Surg Neurol. 1997;47(2):201–4.
Kessler CS, Dharmapuri S, Marcolini EG. Qualitative analysis of effective lecture strategies in emergency medicine. Ann Emerg Med. 2011;58(5):482–9. e487.
McLeod PJ, Steinert Y, Meagher T, McLeod A. The ABCs of pedagogy for clinical teachers. Med Educ. 2003;37(7):638–44.
Gelula MH. Preparing and organizing for a lecture. Surg Neurol. 1997;47(1):86–8.
Copeland HL, Longworth DL, Hewson MG, Stoller JK. Successful lecturing: A prospective study to validate attributes of the effective medical lecture. J Gen Intern Med. 2000;15(6):366–71.
Roopa S, Geetha MB, Rani A, Chacko T. What type of lectures students want? - A reaction evaluation of dental students. J Clin Diagn Res. 2013;7(10):2244–6.
Lyon Jr HC, Holzer M, Reincke M, et al. Improvements in teaching behavior at two German medical schools resulting from a modified Flanders interaction analysis feedback intervention process. Med Teach. 2014;36(10):903–11.
Eraut M. Feedback. Learn Health Soc Care. 2006;5(3):111–8.
Nesbitt A, Pitcher A, James L, Sturrock A, Griffin A. Written feedback on supervised learning events. Clin Teach. 2014;11(4):279–83.
Parboteeah S, Anwar M. Thematic analysis of written assignment feedback: implications for nurse education. Nurse Educ Today. 2009;29(7):753–7.
van de Ridder JM, Stokking KM, McGaghie WC, ten Cate OT. What is feedback in clinical education? Med Educ. 2008;42(2):189–97.
Newton PM, Wallace MJ, McKimm J. Improved quality and quantity of written feedback is associated with a structured feedback proforma. J Educ Eval Health Prof. 2012;9:10.
Bienstock JL, Katz NT, Cox SM, et al. To the point: Medical education reviews--providing feedback. Am J Obstet Gynecol. 2007;196(6):508–13.
Ramani S, Krackov SK. Twelve tips for giving feedback effectively in the clinical environment. Med Teach. 2012;34(10):787–91.
Taylor T. Learning from feedback2005.
Haghani F, Hatef Khorami M, Fakhari M. Effects of structured written feedback by cards on medical students’ performance at Mini Clinical Evaluation Exercise (Mini-CEX) in an outpatient clinic. J Adv Med Educ Prof. 2016;4(3):135–40.
Beckman TJ. Lessons learned from a peer review of bedside teaching. Acad Med. 2004;79(4):343–6.
DiVall M, Barr J, Gonyeau M, et al. Follow-up assessment of a faculty peer observation and evaluation program. Am J Pharm Educ. 2012;76(4):61.
Sullivan PB, Buckle A, Nicky G, Atkinson SH. Peer observation of teaching as a faculty development tool. BMC Medical Education. 2012;12:26.
Trujillo JM, DiVall MV, Barr J, et al. Development of a peer teaching-assessment program and a peer observation and evaluation tool. Am J Pharm Educ. 2008;72(6):147.
Ruesseler M, Kalozoumi-Paizi F, Schill A, et al. Impact of peer feedback on the performance of lecturers in emergency medicine: a prospective observational study. Scand J Trauma Resusc Emerg Med. 2014;22(1):71.
Snydman L, Chandler D, Rencic J, Sung YC. Peer observation and feedback of resident teaching. Clin Teach. 2013;10(1):9–14.
Wilkerson L, Irby DM. Strategies for improving teaching practices: a comprehensive approach to faculty development. Acad Med. 1998;73(4):387–96.
Nelson MS. Peer evaluation of teaching: an approach whose time has come. Acad Med. 1998;73(1):4–5.
Hatfield CL, Coyle EA. Factors that influence student completion of course and faculty evaluations. Am J Pharm Educ. 2013;77(2):27.
Kidd RS, Latif DA. Student evaluations: Are they valid measures of course effectiveness? Am J Pharm Educ. 2004;68(3):61.
Rindermann H. Bedingungs- und Effektvariablen in der Lehrevaluationsforschung: Konzeption und Prüfung des Münchner multifaktoriellen Modells der Lehrveranstaltungsqualität. Unterrichtswissenschaft. 1999;27(4):357–80.
Russeler M, Weber R, Braunbeck A, et al. Training of practical clinical skills in surgery - a training concept for medical students. Zentralbl Chir. 2010;135(3):249–56.
Kadmon M, Bender MJ, Adili F, et al. [Competency-based medical education: National Catalogue of Learning Objectives in surgery]. Chirurg. 2013;84(4):277–85.
Newman LR, Lown BA, Jones RN, Johansson A, Schwartzstein RM. Developing a peer assessment of lecturing instrument: Lessons learned. Acad Med. 2009;84(8):1104–10.
Newman LR, Brodsky DD, Roberts DH, et al. Developing expert-derived rating standards for the peer assessment of lectures. Acad Med. 2012;87(3):356–63.
Clynes MP, Raftery SE. Feedback: An essential element of student learning in clinical practice. Nurse Educ Pract. 2008;8(6):405–11.
de la Cruz MS, Kopec MT, Wimsatt LA. Resident perceptions of giving and receiving peer-to-peer feedback. J Grad Med Educ. 2015;7(2):208–13.
Rees EL, Davies B, Eastwood M. Developing students’ teaching through peer observation and feedback. Perspect Med Educ. 2015;4(5):268–71.
Pattison AT, Sherwood M, Lumsden CJ, Gale A, Markides M. Foundation observation of teaching project--A developmental model of peer observation of teaching. Med Teach. 2012;34(2):e136–142.
Müller-Hilke B. A qualitative study to investigate the acceptance of performance-based allocation of resources for the improvement of education at German medical schools. GMS Z Med Ausbild. 2010;27(3):Doc43.
Acknowledgements
None.
Funding
This study was funded by the German Federal Ministry of Education and Research (grant 01PL12038A) as part of the joint research project, “Practical clinical competence—a joint program to improve training in surgery.” All authors declare that they have no further conflicts of interest. The founder had no influence on the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Availability of data and materials
Evaluation Sheet and dataset are included within the additional files. The original documents were in German and translated in English for this publication.
Authors’ contributions
MR and JS were project leader and were responsible for study conception, training of the reviewers and had full access to all data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. MR, JS, SH and MJ conducted the reviews. BB was responsible for the data analysis and interpretation. BB conducted the statistical analysis. MR, JS and FA contributed to this statistical analysis and were involved in the interpretation of the data. JS and MR wrote the final draft of the manuscript. SH, MJ, BB and FA contributed to the final draft. All authors have read and approved the manuscript.
Competing interests
Dr. M. Ruesseler is an Associate Editor of BMC Medical Education. All authors declare that they have no further conflicts of interest.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The study was conducted according to ethical principles of the Helsinki Declaration (Ethical Principles for Medical Research Involving Human Subjects) and was approved by the ethics committee of the medical faculty of the Goethe University, Frankfurt, Germany. The evaluation of all courses is a mandatory component based on the national regulations to study medicine. Still, lecturers were informed over the particular evaluation which was performed in all surgical lectures and had the possibility to dissent the use of their evaluation data for study purpose. Lecturers were blinded regarding the contents of the evaluation process and aim of the study.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
Evaluation sheet lecturers in surgery. (DOCX 98 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Sterz, J., Höfer, S.H., Bender, B. et al. The effect of written standardized feedback on the structure and quality of surgical lectures: A prospective cohort study. BMC Med Educ 16, 292 (2016). https://doi.org/10.1186/s12909-016-0806-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-016-0806-y