
Abstract
Background
There exists little literature on situational health literacy - that is, how an individual’s health literacy varies across different health literacy environments. However, one can consider the role of stress when examining the relationship between health situations and decision-making ability, and by proxy health literacy. The aim of this study was to assess the strength of the evidence on the relationship between health situations and patient stress, considered in the context of health professional perception, and determine what health situations act to influence patient stress.
Methods
A systematic review of English articles using PubMed, PsycINFO, CINAHL and Embase databases was conducted. Search terms focused on ‘patient’, ‘stress’, and ‘health care situations’. Only peer-reviewed original research with data on patient stress in the context of a health facility environment was included. Studies were screened and critically appraised by both authors. Study elements for extraction were defined by RO and extracted by JY.
Results
Twenty-four studies were included for narrative synthesis. Patients in Intensive Care Units were more stressed about factors relating to their physical discomfort, with some agreement from health care professionals. Parents of children in Intensive Care Units were more concerned with stressors relating to their child’s appearance and behaviour, and alteration in their parental role. Few studies examined health settings other than Intensive Care Units, and those that did varied greatly in terms of study design and population characteristics, lacking generalisability.
Conclusions
Overall, the findings of what patients find most stressful in Intensive Care Units can guide health care professionals practicing best practice care. However, the evidence on how patient stress is influenced by non-Intensive Care Unit health care settings is weak. Further research is needed to enhance current understanding of the interaction between patient stress and health care environments in both hospital and primary care settings.
Similar content being viewed by others

Background
Health literacy
Health literacy can be defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” [1]. Its importance is well established. Not only is low health literacy associated with poor health for individuals and poor financial outcomes for health systems [2, 3], it is also highly prevalent both in Australia and internationally [1, 4].
Increasingly, health literacy is recognised as dynamic, varying depending on the context and characteristics of individuals, environmental and social factors, and the demands and burdens placed on individuals [1, 5,6,7,8,9,10,11,12]. Indeed, a critical component of health literacy is the health literacy environment, which is the “infrastructure, policies, processes, materials, people and relationships that make up the health system and have an impact on the way that people access, understand, appraise and apply health-related information and services” [13]. However, despite a few key studies [14, 15], there is still little current literature on situational health literacy – that is, how an individual’s health literacy varies across different health literacy environments.
Stress can be considered when examining the relationship between health situations and decision-making ability, and by proxy health literacy. Much of the literature suggests that stress impairs decision-making ability [16, 17], through several mechanisms. Firstly, high stress levels have been found to cause inadequate consideration of alternatives, resulting in dysfunctional strategy use [16]. Additionally, there is an over-reliance on intuitive decision-making rather than strategic choice, reflecting an insufficient adjustment from automated responses [16]. Furthermore, stress triggers altered feedback processing, causing stressed individuals to make more disadvantageous choices [16]. Given the clear influence of stress on decision-making ability [16, 17], the focus of the current study is on what health situations act to influence patient stress.
Health situations and stress
Environmental factors are known to play a large role in increasing or decreasing patient stress [18]. Much of the literature focuses on stressors, both physical and psychological, associated with hospitalisation. These include lack of natural light, increased noise levels, presence of unwelcome smells or other sensations, absence of clocks, and a perception of crowding by unfamiliar people [19,20,21]. Intensive Care Units (ICUs) especially are known to be stressful environments [19], with specific stressors including experiencing pain, disruption of sleep-wake patterns, and intubation [22, 23]. A perceived lack of control over these physical environmental factors also increases patient stress [21, 24]. In addition, hospital patients are stressed by their inability to obtain desired information, and their fear of an unknown or serious illness [24]. Furthermore, decreased social support, such as with loss of contact with family and friends, and financial worries associated with hospitalisation and illness, have been identified as stressful for patients [19, 22, 24].
Stress-reducing environmental factors have also been identified. Viewing plants and nature has been shown to decrease patient stress [25], an effect which was reproduced by viewing photographs of plants or nature in a hospital waiting room [26]. In addition, environmental interventions that counter stress-inducing factors are thought to reduce patient stress [18]. Recommendations have been made for single-bed rather than multi-bed rooms, and elimination of noise sources, as these would lead to improved sleep [18]. Similarly, administrative and procedural information, external building cues, local information systems, and global structural redesign, have also been recommended as these interventions reduce spatial disorientation, and consequently decrease patient stress [18, 27]. These recommendations appear to also apply beyond hospitals to the primary care setting [28].
There are also other aspects of health situations that influence patient stress. These include the provider-consumer interaction – that is, what physicians say and how they deliver this information [29]. In particular, taking time, empathising with patients, and overall effective communication skills have been shown to help reduce patient stress [29, 30]. Additionally, the broader social, economic, and psychosocial contexts of stress can be considered. Constant exposure to socially and economically challenging environments has been shown to increase stress [31], while strong social support networks protect against stress and other environmental threats to health [31, 32].
Clearly, many health situations affect patient stress, potentially influencing decision-making ability and by proxy health literacy. However, the cumulative strength of the evidence on this relationship between health situations and patient stress has not been evaluated. The aim of this systematic review is to assess the strength of this evidence, and determine what health situations act to influence patient stress. In doing so, this study will also inform our understanding of health situations in supporting or constraining health literacy.
Methods
The study design of this systematic review was guided by the PRISMA Statement [33] (Appendix 1). Studies were identified by searching through the electronic databases PubMed, PsycINFO, CINAHL and Embase, with coverage from 1997 to February 2017. This timeframe was selected to provide a long enough period to comprehensively review the research, whilst maintaining the relevance of the health care context to contemporary practice. No grey literature was reviewed, and the reference lists of included articles were not searched for additional studies.
The search terms comprised of three components: patient; stress; and health care environment. Index terms were used when possible as appropriate for each database, and synonyms were included. Terms relating to stress of health care professionals or staff, and mental disorders of patients, were excluded from the search. In addition, the search was limited to journal articles published in English since 1997. The full search strategy is provided in Appendix 2.
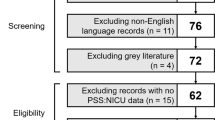
The study selection process is summarised in Fig. 1. Articles identified through the search process were screened by JY based on titles alone, removing articles that were not relevant to the current study question. The abstracts of the remaining articles were then assessed independently by JY and RO, applying the pre-determined inclusion and exclusion criteria (Table 1). Articles without abstracts were removed at this point. Disagreements regarding article inclusion or exclusion were resolved by a third reviewer, NA. Articles that were evaluated as sufficiently rigorous were included for critical appraisal. This process was completed independently by JY and RO, using an appraisal template adapted from Bush et al. [34] (Additional file 1). Articles of lower methodological strength, generally corresponding to a score of 0 or failing to score 2 in any of Appraisal Questions 1–5, were excluded. Discrepancies regarding the eligibility of articles at this stage were resolved by discussion between the two reviewers until agreement was reached. Eligible articles were included in the qualitative analysis.

Flow diagram of study selection process, including formal search, screening, application of inclusion and exclusion criteria, and critical analysis, with the number of articles included and excluded at each step. Adapted from the PRISMA Statement [33]
Data extraction items were defined by RO and extracted by JY from eligible articles. These data items included: study source, design, country, population characteristics, health care setting, measured variables, intervention, and outcomes. Due to the nature of the types of studies included, a narrative synthesis, rather than meta-analysis, was the more appropriate method of analysis.
Results
A total of 1506 unique articles were identified through the database searches conducted. Of these, 874 articles were excluded based on title-scanning as they were not addressing the research question. A further 573 were excluded based on abstract-scanning as they did not meet the inclusion and exclusion criteria. Full texts of the remaining 59 articles were critically appraised, and 24 were further excluded based on exclusion criteria whilst 11 were excluded after formal appraisal of methodological strength. The included articles received appraisal scores ranging from six to nine, out of a possible twelve. Overall, 24 articles were assessed to be eligible for data extraction and narrative synthesis, and were included in this systematic review (Fig. 1).
The study designs of included research were mostly descriptive – of the 24 studies, nineteen (79%) were cross-sectional surveys, one used a descriptive qualitative design, and only four were experimental. Included studies were also internationally diverse. Nine studies were set in Asia, eight in Europe, six in the USA, two in Brazil, and one in New Zealand. Furthermore, all studies were conducted in hospital settings, with the majority (71%) set in ICUs (nine adult, eight paediatric/neonatal). Regarding participants, eight studies focused on parents and sixteen on patients, with five of the latter also including health care professionals. Most participants were adults, with only Causey et al. [35] recruiting children and adolescents, and Yeh et al. [36] recruiting patients as young as fifteen years. Finally, the measured variable, stress, was assessed with validated tools in most studies (92%), while Larsen, Larsen and Birkelund [37] conducted participant observation and interviews, and Lilja, Ryden and Fridlund [38] measured serum cortisol (Table 2).
Patient and parental stressors in ICU
Considering the nine studies that ranked patient stressors in ICU [19, 22, 23, 39,40,41,42,43,44], the items from the ICU Stressor (or similar) scales that were rated highly most frequently related to physical discomfort. As examples, top ten stressors included ‘being in pain’ in all studies, and ‘being unable to sleep’ in all but one study. Overall, seven of thirteen (54%) items in the physical discomfort subscale were listed as top ten in two or more studies. In contrast, only 35% of stressors relating to psychological distress, and 36% stressors relating to the ICU environment, were ranked highly in at least two studies. No stressors relating to treatment procedures were listed more than once in the top ten (Table 3).
Comparing stressors as ranked by patients with health care professional rankings, shows that some stressors were also ranked consistently highly by health care professionals across studies, such as ‘being in pain’, ‘being tied down by tubes’, and ‘having tubes in your nose/mouth’. However, for the most part, stressors were evaluated differently by patients and health care professionals, with significant differences between scores on stressor scales in some studies [22, 23]. In particular, Biancofiore et al. [22] found that patients used a score of 1 (not stressful) more frequently than health care professionals when rating stressors, while health care professionals tended to use scores of 2, 3 and 4 (increasing stressfulness) more frequently (Table 3).
For parents, stressors relating to the appearance and behaviour of their child, or alteration of their parental role, were ranked most highly in almost all studies. Parental role alteration, and child appearance and behaviour were ranked first and second respectively by parents in studies of Franck et al. [47], Nizam and Norzila [51], and Reid and Bramwell. On the other hand, stressors relating to staff communication and behaviour, and the ICU environment, were consistently at the bottom of parent rankings (Table 3).
Non-ICU settings
Seven of the 24 studies examined health care environments other than ICU. These included a psychiatric inpatient unit; medical, oncology and surgical wards; haemodialysis units across various medical centres, regional and community hospitals; and a radiology department waiting room. The designs of these seven studies varied greatly, ranging from cross-sectional survey, to qualitative and experimental, the interventions of which showed inconsistent effects (Table 2).
Children and adolescents admitted to an inpatient psychiatric unit appeared to be more stressed by separation from their friends and family, and their loss of autonomy, than by other aspects of the health care environment such as the psychiatric setting and staff interaction [35]. More broadly, stressors were found to be perceived differently by patients depending on the type of health facility. Yeh et al. [36] showed that issues such as physical symptoms, dependency on medical staff, and role ambiguity, were rated higher by patients in ‘Religious Affiliated’ hospitals, while patients in ‘Veterans/Army’ hospitals experienced significantly higher stress in food and fluid restriction, and dependency on medical staff, than patients in ‘For Profit’ hospitals.
Larsen, Larsen and Birkelund [37] found, through interviews with cancer patients, several recurring themes relating to the health care environment. These included the health effects, both positive and negative, of a health care setting, and the implications of (lack of) patient privacy, such as withholding information from doctors, avoiding other patients, and preferring single-bed rooms. Despite these apparent shortcomings of their accommodation, the patients maintained a sense of acceptance of and resignation to the hospital environment.
Several studies investigated whether altering aspects of the health care setting would impact patient stress. Beukeboom, Langeveld and Tanja-Dijkstra [26] tested the effect of exposure to nature on stress, and found that both real plants and posters of plants significantly lowered the stress of patients in a waiting room. This effect was at least partially mediated by the perceived attractiveness of the room. Additionally, music therapy appeared to decrease both psychosocial and physiological stress for patients in haemodialysis units [53]. On the other hand, preoperative information provided by an anaesthetic nurse had no significant impact on patient stress [38]. Only one study compared inpatient and outpatient settings, which found no significant differences in stress between the two groups, in patients awaiting pacemaker implantation [54].
Discussion
Summary of evidence
There are several main findings regarding what was identified as stressful about health care settings. Firstly, patients in ICU were consistently more stressed about factors relating to their physical discomfort, than those relating to psychological distress or the ICU environment. Meanwhile, apart from some similarity with stressors relating to physical discomfort, health care professionals placed importance on different stressors to patients, and generally rated them as more highly stressful to patients than did patients. Additionally, parents of children in ICU consistently placed the most importance on stressors relating to their child’s appearance and behaviour, and alterations in their parental role, while being less concerned about stressors relating to staff communication and behaviour, and the sights and sounds of the ICU environment. Overall, the strength of the evidence for these findings is acceptable, and while difficult to apply to non-ICU settings, can be expected to be consistent between ICUs especially given the international diversity of the included studies.
Adult patients in an oncology ward often found their lack of privacy, related to the architecture in multiple-bed rooms, stressful and non-healing [37]. That this finding is not entirely consistent with the above studies, where stressors relating to the health care environment were less worrisome, may be explained by the different study designs and health settings. In addition, children and adolescents in a psychiatric unit appeared to find separation from family and friends, and loss of autonomy, more stressful than staff interactions and the psychiatric environment. However, the evidence for this finding is less robust given no studies other than that of Causey et al. [35] investigated this population and health care setting.
The nature of the health care setting appeared to have variable effect on patient stress. Broadly, the type of health care facility, specifically its ownership, influenced how stressors were perceived by its patients [36]. In contrast, no differences in levels of patient stress were found between inpatient and outpatient health settings [54]. Admittedly, these results are difficult to compare as the studies were very different, in terms of study design, population characteristics, and assessment tool.
The experimental studies found that exposure to nature and plants, and music therapy, decreased patient stress, while pre-operative provision of information had no such reduction on patient stress. These findings, while promising, carry less weight than the previous outcomes. One of the main reasons for this is that across the few included experimental studies, the population, setting, interventions, and measured outcomes all differ. Furthermore, they lack generalizability – for example, the music intervention used by Cantekin and Tan [53] was Turkish art music songs, the effect of which may be difficult to reproduce in other populations. Therefore, the evidence of these outcomes is relatively weak.
This systematic review set out to firstly assess the strength of evidence on the relationship between health care situations and patient stress, and secondly determine what health care situations act to influence patient stress. It has partially met these aims. Certainly, this study confirms that ICUs are indeed stressful environments and produces some detail on specific stressors; however, the evidence for other outcomes in different health care settings is insufficiently robust.
The importance of stress in the relationship between health situations and decision-making ability relates to the way high stress levels result in dysfunctional strategies, over-reliance on intuitive decision-making, and more disadvantageous choices [16]. This implies that patients in stressful health situations such as ICU would have impaired decision-making abilities and likely constrained health literacy. How specific features of these health situations lead to patient stress, and how stressors in these contexts affect decision-making ability are important areas to examine further.
Limitations
The study has several limitations. Firstly, the review process may have been limited by the search strategy. The diversity of the literature around stress and healthcare made it difficult to develop a strategy with sufficient sensitivity and specificity. This meant that a large variety of articles, often tangential to the topic, were identified, and additionally the risk of missing key articles was increased. This may have been exacerbated by the restriction to only English-language publications. Furthermore, no additional searches were conducted for grey literature, and articles were not drawn from reference lists of included studies, or those citing included studies. This may have introduced a degree of publication bias. Another limitation was the lack of weighted scoring in the appraisal tool, meaning no explicit cut-off value could be set as an inclusion or exclusion criterion.
In addition, a limitation of the data analysis was the diverse nature of the included studies, with study designs, patient populations, health settings, interventions, and outcome measure often differing across studies. Moreover, a narrative synthesis, which was necessary given the types of include studies, cannot provide the same degree of strength of evidence as a meta-analysis. That the main findings of the analysis were drawn mostly from studies set in the ICU also limits the generalizability of the review. One issue specific to these studies is that using the stressor scales as assessment tools presupposes the factors that patients find stressful, and may not account for other relevant stressors.
Implications
An important next step would be to investigate patient stress in the context of health care settings other than the ICU. These should include not just other aspects of the hospital setting, such as different wards or waiting rooms, but also extend to the primary care setting. While an enhanced primary care environment has been associated with decreased patient anxiety and improved patient satisfaction [28], further research could enhance current understanding of the interaction between patient stress and this environment. As individual stressors are increasingly identified, future research could also investigate the effects of interventions that target these stressors. Ultimately, given the original focus on decision-making and health literacy, future research must directly investigate health literacy levels of patients and how this is influenced by different health care settings. Furthermore, this research should examine other aspects of the health literacy environment, such as relationships, infrastructure, and policies. Studies of this kind will more likely have lasting impact on clinical practice and health care design.
Conclusions
Overall, this systematic review has revealed that the evidence on how patient stress is influenced by non-ICU health care settings is weak. That being said, this review does show what patients find most stressful in the ICU, and these findings can guide health care professionals practicing best practice care.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- CCU:
-
Critical care unit
- DV:
-
Dependent variable
- GCU:
-
General care unit
- HCP:
-
Health care professional
- ICU:
-
Intensive care unit
- NICU:
-
Neonatal intensive care unit
- PHDU:
-
Paediatric high dependency unit
- PICU:
-
Paediatric intensive care unit
- PSS:
-
Parental stressor scale
- SD:
-
Standard deviation
References
Institute of Medicine Committee on Health Literacy. In: Nielsen-Bohlman L, Panzer AM, Kindig DA, editors. Health literacy: a prescription to end confusion. Washington, DC: National Academies Press (US); 2004.
DeWalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy and health outcomes. J Gen Intern Med. 2004;19(12):1228–39.
Baker DW, Gazmararian J, Green D, Parker R, Peel J, Ren J, et al. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. Am J Public Health. 2002;92(8):1278–83.
ABS. Health Literacy, Australia. In: ABS, editor. Cat No 42330. Canberra: Australian Bureau of Statistics; 2008.
Martin LT, Schonlau M, Haas A, Rosenfeld L, Derose KP, Buka SL, et al. Patient activation and advocacy: which literacy skills matter most? J Health Commun. 2011;16(Suppl 3):177–90.
Johnson A. Health literacy, does it make a difference? Aust J Adv Nurs. 2014;31(3):39–45.
Baker DW. The meaning and the measure of health literacy. J Gen Intern Med. 2006;21(8):878–83.
Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. 2000;15(3):259–67.
Jordan JE, Buchbinder R, Osborne RH. Conceptualising health literacy from the patient perspective. Patient Educ Couns. 2010;79(1):36–42.
Rudd RE. Improving Americans' health literacy. N Engl J Med. 2010;363(24):2283–5.
Brach C, Keller D, Hernandez LM, Baur C, Dreyer B, Schyve P, et al. Ten attributes of health literate health care organizations. Washington, DC: Institute of Medicine of the National Academies; 2012.
Pleasant A, Rudd R, O’Leary C, Paasche Orlow M, P. Allen M, Alvarado-Little W, et al. Considerations for a New Definition of Health Literacy. Washington, DC: National Academy of Medicine; 2016.
Health literacy: Taking action to improve safety and quality. Sydney: Australian Commission on Safety and Quality in Health Care; 2014.
Nutbeam D. The evolving concept of health literacy. Soc Sci Med (1982). 2008;67(12):2072–8.
Sorensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80.
Starcke K, Brand M. Decision making under stress: a selective review. Neurosci Biobehav Rev. 2012;36(4):1228–48.
Schwabe L, Wolf OT. Stress-induced modulation of instrumental behavior: from goal-directed to habitual control of action. Behav Brain Res. 2011;219(2):321–8.
Ulrich RS, Quan X, Zimring C, Joseph A, Choudhary R. The role of the physical environment in the hospital of the 21st century: a once-in-a-lifetime opportunity. Concord: The Center for Health Design; 2004.
Dias Dde S, Resende MV, Diniz GC. Patient stress in intensive care: comparison between a coronary care unit and a general postoperative unit. Revista Brasileira de terapia intensiva. 2015;27(1):18–25.
Cordova AC, Logishetty K, Fauerbach J, Price LA, Gibson BR, Milner SM. Noise levels in a burn intensive care unit. Burns. 2013;39(1):44–8.
Devlin AS, Arneill AB. Health care environments and patient outcomes: a review of the literature. Environ Behav. 2003;35(5):665–94.
Biancofiore G, Bindi ML, Romanelli AM, Urbani L, Mosca F, Filipponi F. Stress-inducing factors in ICUs: what liver transplant recipients experience and what caregivers perceive. Liver Transpl. 2005;11(8):967–72.
Novaes MA, Knobel E, Bork AM, FO P, Nogueira-Martins LA, Ferraz MB. Stressors in ICU: perception of the patient, relatives and health care team. Intensive Care Med. 1999;25(12):1421–6.
van Servellen G, Lewis CE, Leake B. The stresses of hospitalization among AIDS patients on integrated and special care units. Int J Nurs Stud. 1990;27(3):235–47.
Ulrich RS. Health benefits of gardens in hospitals. Plants for People; International Exhibition Floriade. Netherlands: 2002.
Beukeboom CJ, Langeveld D, Tanja-Dijkstra K. Stress-reducing effects of real and artificial nature in a hospital waiting room. J Altern Complement Med. 2012;18(4):329–33.
Maqbool T, Raju S, In E. Importance of patient-centred signage and navigation guide in an orthopaedic and plastics clinic. BMJ Qual Improv Rep. 2016;5(1):u209473.w3887.
Rice G, Ingram J, Mizan J. Enhancing a primary care environment: a case study of effects on patients and staff in a single general practice. Br J Gen Pract. 2008;58(552):e1–8.
Ptacek JT, Ptacek JJ. Patients' perceptions of receiving bad news about cancer. J Clin Oncol. 2001;19(21):4160–4.
Roter DL, Hall JA, Kern DE, Barker LR, Cole KA, Roca RP. Improving physicians' interviewing skills and reducing patients' emotional distress. A randomized clinical trial. Arch Intern Med. 1995;155(17):1877–84.
Bruce MA, Beech BM, Sims M, Brown TN, Wyatt SB, Taylor HA, et al. Social environmental stressors, psychological factors, and kidney disease. J Investig Med. 2009;57(4):583–9.
Ozbay F, Johnson DC, Dimoulas E, Morgan CA, Charney D, Southwick S. Social support and resilience to stress: from neurobiology to clinical practice. Innov Clin Neurosci. 2007;4(5):35–40.
Moher D, Liberati A, Tetzlaff J, Altman DG. The Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med. 2009;6(7):e1000097.
Bush R, Boyle F, Ostini R, Ozolins I, Brabant M, Jimenez Soto E, et al. Advancing health literacy through primary health care systems. 2010.
Causey DL, McKay M, Ronsenthal C, Darnell C. Assessment of hospital-related stress in children and adolescents admitted to a psychiatric inpatient unit. J Child Adolesc Psychiat Nurs. 1998;11(4):135–45.
Yeh SC, Huang CH, Chou HC, Wan TT. The influence of facility ownership structure on individual responding to stress: a multilevel model. Health Serv Manag Res. 2009;22(2):62–70.
Larsen LS, Larsen BH, Birkelund R. A companionship between strangers - the hospital environment as a challenge in patient-patient interaction in oncology wards. J Adv Nurs. 2014;70(2):395–404.
Lilja Y, Ryden S, Fridlund B. Effects of extended preoperative information on perioperative stress: an anaesthetic nurse intervention for patients with breast cancer and total hip replacement. Intens Crit Care Nurs. 1998;14(6):276–82.
Hweidi IM. Jordanian patients' perception of stressors in critical care units: a questionnaire survey. Int J Nurs Stud. 2007;44(2):227–35.
Lam Soh K, Geok Soh K, Ahmad Z, Raman RA, Japar S. Perception of intensive care unit stressors by Malaysian Federal Territory hospitals. Contemp Nurse. 2008;31(1):86–93.
Pang PS, Suen LK. Stressors in the ICU: a comparison of patients' and nurses' perceptions. J Clin Nurs. 2008;17(20):2681–9.
Samuelson KAM, Lundberg D, Fridlund B. Stressful experiences in relation to depth of sedation in mechanically ventilated patients. Nurs Crit Care. 2007;12(2):93–104.
So HM, Chan DSK. Perception of stressors by patients and nurses of critical care units in Hong Kong. Int J Nurs Stud. 2004;41(1):77–84.
Yava A, Tosun N, Unver V, Cicek H. Patient and nurse perceptions of stressors in the intensive care unit. Stress Health. 2011;27(2):e36–47.
Board R, Ryan-Wenger N. Stressors and stress symptoms of mothers with children in the PICU. J Pediatr Nurs. 2003;18(3):195–202.
Board R. Father stress during a child's critical care hospitalization. J Pediatr Health Care. 2004;18(5):244–9.
Franck LS, Cox S, Allen A, Winter I. Measuring neonatal intensive care unit-related parental stress. J Adv Nurs. 2005;49(6):608–15.
Ichijima E, Kirk R, Hornblow A. Parental support in neonatal intensive care units: a cross-cultural comparison between New Zealand and Japan. J Pediatr Nurs. 2011;26(3):206–15.
Lee SY, Lee KA, Rankin SH, Alkon A, Weiss SJ. Acculturation and stress in Chinese-American parents of infants cared for in the intensive care unit. Adv Neonatal Care. 2005;5(6):315–28.
Miles MS, Burchinal P, Holditch-Davis D, Brunssen S, Wilson SM. Perceptions of stress, worry, and support in black and white mothers of hospitalized, medically fragile infants. J Pediatr Nurs. 2002;17(2):82–8.
Nizam M, Norzila MZ. Stress among parents with acutely ill children. Med J Malaysia. 2001;56(4):428–34.
Reid T, Bramwell R. Using the parental stressor scale: NICU with a British sample of mothers of moderate risk preterm infants. J Reprod Infant Psychol. 2003;21(4):279–91.
Cantekin I, Tan M. The influence of music therapy on perceived stressors and anxiety levels of hemodialysis patients. Ren Fail. 2013;35(1):105–9.
Müller-Nordhorn J, Schüler G, Roll S, Willich SN. Implantation of a cardiac pacemaker - comparison of subjective stress and mood between in- and outpatients. Clin Res Cardiol. 2006;95(10):539–46.
Acknowledgements
We acknowledge Noor Aljassim for her assistance in the review process
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
RO was the major contributor to the overall study conception and design. The systemic search of electronic databases was performed by JY. Studies were screened and critically appraised by both authors. Study elements for extraction were defined by RO and extracted by JY. Both authors analysed and interpreted the data. The manuscript was drafted by JY and revised in consultation with RO. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: APPENDIX 3.
Critical Appraisal Tool
Appendices
APPENDIX 1: PRISMA Checklist
Section/topic | # | Checklist item | Reported on page # |
|---|---|---|---|
TITLE | |||
Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | 1 |
ABSTRACT | |||
Structured summary | 2 | Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number. | 2, 3 |
INTRODUCTION | |||
Rationale | 3 | Describe the rationale for the review in the context of what is already known. | 4–6 |
Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | 6 |
METHODS | |||
Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number. | |
Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. | 6, 7 |
Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | 6 |
Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | 29 |
Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). | 7 |
Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. | 8 |
Data items | 11 | List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. | 8 |
Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. | 7 |
Summary measures | 13 | State the principal summary measures (e.g., risk ratio, difference in means). | 8 |
Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | 8 |
Page 1 of 2.
Section/topic | # | Checklist item | Reported on page # |
|---|---|---|---|
Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). | |
Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified. | |
RESULTS | |||
Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. | 8 |
Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | 8, 9, 16, 17 |
Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). | 17–20 |
Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. | 17–20 |
Synthesis of results | 21 | Present results of each meta-analysis done, including confidence intervals and measures of consistency. | 17–20 (narrative synthesis) |
Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | |
Additional analysis | 23 | Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). | |
DISCUSSION | |||
Summary of evidence | 24 | Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers). | 11–13 |
Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias). | 13, 14 |
Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence, and implications for future research. | 14, 15 |
FUNDING | |||
Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. | 22 |
From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi:https://doi.org/10.1371/journal.pmed1000097
For more information, visit: www.prisma-statement.org.
Page 2 of 2
APPENDIX 2
Search strategy: PubMed
-
1.
“Patients” [Mesh]
-
2.
“Research Subjects” [Mesh]
-
3.
“Men” [Mesh]
-
4.
“Women” [Mesh]
-
5.
“Visitors to Patients” [Mesh]
-
6.
1 OR 2 OR 3 OR 4 OR 5
-
7.
“Stress, Psychological” [Mesh]
-
8.
“Stress, Physiological” [Mesh]
-
9.
“Anxiety” [Mesh]
-
10.
Distress
-
11.
Strain
-
12.
7 OR 8 OR 9 OR 10 OR 11
-
13.
6 AND 12
-
14.
“patient stress”
-
15.
13 OR 14
-
16.
“Compassion Fatigue” [Mesh]
-
17.
“Burnout, Professional” [Mesh]
-
18.
“Mental Disorders” [Mesh]
-
19.
16 OR 17 OR 18
-
20.
15 NOT 19
-
21.
“Environment” [Mesh]
-
22.
“Health Facilities” [Mesh]
-
23.
21 OR 22
-
24.
20 AND 23
Search strategy: PsycInfo
-
1.
“Anxiety” [Index Term]
-
2.
“Chronic Stress” [Index Term]
-
3.
“Distress” [Index Term]
-
4.
“Environmental Stress” [Index Term]
-
5.
“Financial Strain” [Index Term]
-
6.
“Physiological Stress” [Index Term]
-
7.
“Psychological Stress” [Index Term]
-
8.
“Stress” [Index Term]
-
9.
“Stress Reactions” [Index Term]
-
10.
1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9
-
11.
“Environment” [Index Term]
-
12.
“Environmental Enrichment” [Index Term]
-
13.
“Facility Environment” [Index Term]
-
14.
“Learning Environment” [Index Term]
-
15.
“Therapeutic Environment” [Index Term]
-
16.
11 OR 12 OR 13 OR 14 OR 15
-
17.
10 AND 16
-
18.
Any Field: “Journal”
-
19.
Year: 1997 to 2007
-
20.
Population Group: Human
-
21.
17 AND 18 AND 19 AND 20
Search strategy: CINAHL
-
1.
MH “Patients+”
-
2.
MH “Stress+”
-
3.
1 AND 2
-
4.
“patient stress”
-
5.
3 OR 4
-
6.
MH “Caregiver Burden”
-
7.
MH “Compassion Fatigue”
-
8.
MH “Stress, Occupational+”
-
9.
6 OR 7 OR 8
-
10.
5 NOT 9
-
11.
MH “Health Facilities+”
-
12.
10 AND 11
Search strategy: Embase
-
1.
‘stress’/exp.
-
2.
‘patient’/exp.
-
3.
1 AND 2
-
4.
‘patient stress’
-
5.
3 OR 4
-
6.
‘burnout’/exp.
-
7.
‘caregiver burden’/exp.
-
8.
‘job stress’/exp.
-
9.
6 OR 7 OR 8
-
10.
5 NOT 9
-
11.
‘health care facility’/exp
-
12.
10 AND 11
-
13.
[1997–2017]/py
-
14.
[humans]/lim
-
15.
[English]/lim
-
16.
[article]/lim
-
17.
12 AND 13 AND 14 AND 15 AND 16
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yeh, J., Ostini, R. The impact of health literacy environment on patient stress: a systematic review. BMC Public Health 20, 749 (2020). https://doi.org/10.1186/s12889-020-08649-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-020-08649-x