
Abstract
Background
Despite differences in types of infection and causative organisms, pharmacokinetic-pharmacodynamic (PKPD) targets of vancomycin therapy derived from adult studies are suggested for neonates. We aimed to identify doses needed for the attainment of AUC/MIC > 400 and AUC/MIC > 300 in neonates with sepsis and correlate these targets with recommended doses and treatment outcome.
Methods
Neonates who had Vancomycin therapeutic drug monitoring (TDM) performed between January 1, 2010 and December 31, 2012 were studied. Clinical characteristics, episodes of Gram-positive sepsis with outcomes and all neonatal blood culture isolates in hospital were collected from medical records. To estimate probability of target attainment of AUC/MIC >400 and AUC/MIC >300 a 1000-subject Monte Carlo simulation was performed by calculating AUC using Anderson’s (Anderson et al. 2006) and TDM trough concentrations (Ctrough) based population PK models.
Results
Final dataset included 76 patients; 57 with confirmed Gram-positive sepsis. TDM was taken after the 1st to 44th dose. 84.1% of Ctrough were within the range 5–15 mg/L. Currently recommended doses achieved probability of the targets (PTA) of AUC/MIC >400 and AUC/MIC >300 in less than 25% and 40% of cases, respectively. Doses required for 80% PTA of AUC/MIC > 400 for MIC ≥2 mg/L resulted in Ctrough values ≥14 mg/L. Mean AUC/MIC values were similar in treatment failure and success groups.
Conclusion
With currently recommended vancomycin dosing the therapeutic target of AUC/MIC > 400 is achieved only by 25% of neonates. Appropriate PKPD targets and respective dosing regimens need to be defined in prospective clinical studies in this population.
Similar content being viewed by others


What is already known about this subject?
-
1.
Vancomycin PK has wide inter-individual variability, especially in neonates
-
2.
AUC/MIC > 400 is associated with improved treatment efficacy in adult MRSA pneumonia
-
3.
AUC/MIC > 400 is hardly achieved with currently recommended regimes in children
What this study adds?
-
1.
Trough concentrations of vancomycin required for AUC 400 in neonates are lower than reported for adults
-
2.
Based on actual MIC distribution of neonatal invasive CoNS strains, with current vancomycin dosing AUC/MIC of 400 is achieved in less than half of neonates. Vancomycin doses required for 80% probability of this target attainment are associated with potentially toxic trough levels.
-
3.
With current vancomycin dosing, treatment failure occurs in about a quarter of cases.
Background
With few exceptions coagulase-negative staphylococci (CoNS) have remained the most frequent causative agents of neonatal late onset sepsis over the last decades [1, 2]. Although CoNS sepsis is characterised by low mortality, the microorganism is known to be highly resistant to antibiotics - methicillin resistance exceeds 70% in most centres [3]. Therefore vancomycin has become the antimicrobial therapy of choice for targeted or empiric treatment of neonatal sepsis, especially in extremely premature babies [4]. However, despite extensive research and widespread use considerable controversies in vancomycin exposure required for optimal efficacy and consequently in dosing, remain [5, 6]. Poor tissue penetration of vancomycin suggests that different serum concentrations may be required depending on the site of infection, i.e. pneumonia vs blood stream vs bone infection [7]. Further complexity is added by pathogen-specific pharmacokinetic/pharmacodynamic (PK/PD) targets, supported by recent experimental studies. Leiva et al. have demonstrated in the neutropenic mouse thigh infection model without the use of a foreign body that to stop or kill methicillin-resistant S. epidermidis 2.5–3.0 times lower area under the curve to minimal inhibitory concentration ratios (AUC/MIC) were needed compared to values required for methicillin-susceptible S. aureus [8].
For neonates, in whom CoNS blood stream infections (BSI) predominate, effective vancomycin AUC/MIC has not been studied, but lower ratios could likely be sufficient as CoNS rarely invades tissues where vancomycin concentrations are lower than in blood.
Current vancomycin treatment in neonates is guided by the trough concentration (Ctrough) values derived from studies in adults and recommendations range between 5 and 20 mg/L. Modelling studies have shown that a Ctrough of at least 15 mg/L is required to achieve an AUC/MIC >400 for a pathogen with MIC of 1 mg/L in adults, but lower values of 8–9 mg/L for children and 7–11 mg/L for neonates have been suggested in recent studies using samples, collected for therapeutic drug monitoring (TDM), and population pharmacokinetic (popPK) analysis [5, 9–11]. Vancomycin Ctrough values used regularly in clinical practice unfortunately poorly predict AUC [12, 13]. Furthermore, total vancomycin concentrations are usually measured, but only unbound fraction of drug is active. Free vancomycin concentration cannot be predicted from total vancomycin concentration measurement [14].
We assumed that compared to S. aureus infection in adults, lower AUC/MIC ratio is needed for the treatment of neonatal CoNS sepsis because CoNS are less invasive and rarely cause other infection than BSI. In addition higher free drug concentration can be assumed in neonates due to lower protein levels and drug protein binding capability of neonatal plasma and elevated bilirubin which competes with drugs for binding sites to albumin [15–17]. Finally in our study we used MIC values of CoNS causing neonatal sepsis rather than fixed MIC values from databases.
We aimed, first, to identify neonatal vancomycin doses needed for 80% and 90% probability of target attainment (PTA) of AUC/MIC >400 and AUC/MIC >300 using minimal inhibitory concentration (MIC) distribution of invasive neonatal CoNS isolates from our hospital; second, to characterise the PTA for these targets with currently recommended TDM guided dosing, and third, to correlate individual AUC/MIC ratios with clinical outcome.
Methods
Study design
The clinical and laboratory data were collected retrospectively from hospital records and vancomycin concentrations from laboratory databases. Microsoft Excel spreadsheets were used to create the study database. Neonates and infants <90 days of postnatal age (PNA) admitted to Tartu University Hospital between January 1, 2010 and December 31, 2012 were included.
All neonates/infants with at least one vancomycin concentration in the database were eligible. The following data were collected: demographic parameters (gestational age [GA] and PNA, postmenstrual age (PMA), birth- and current weight [BW and CW], gender), therapeutic interventions during vancomycin treatment (mode of ventilation, presence and removal of indwelling catheters and vasoactive treatment), creatinine concentrations (measured by Jaffe kinetic method) at ±72 h of TDM time and reasons for vancomycin treatment, classified as culture proven Gram-positive sepsis, clinical sepsis and no Gram-positive sepsis [18]. Sepsis was considered culture proven if the patient had a Gram-positive pathogen isolated from blood and vancomycin treatment was given for at least 72 h; and clinical sepsis if blood culture was negative but the patient had clinical signs/symptoms suggestive of sepsis and vancomycin treatment was given for at least 72 h. All remaining cases were categorised as no Gram-positive sepsis.
Vancomycin dosing and TDM
Vancomycin was given as a 60 min infusion at the dose recommended in Neofax (Table 1) [19]. Individual dose adjustments based on the TDM results were performed at the discretion of the treating physician. Start and termination of vancomycin therapy, dosing regimen and infusion time prior to TDM sample and TDM sampling time were collected.
In our hospital vancomycin TDM samples are routinely taken an hour before the 3rd or 4th dose and thereafter at the discretion of the treating physician. Vancomycin concentrations were measured by commercial fluorescence polarization immunoassay according to manufacturers’ instructions (Cobas Integra 400/800 Analyzer, Roche, Mannheim, Germany). TDM samples taken up to 2 h before the next dose were designated Ctroughs.
Microbiological data
Of all Gram-positive isolates obtained from blood cultures up to 5 days before and/or during vancomycin treatment of study patients were identified from the databases of the Department of Clinical Microbiology. Microorganisms were identified by the VITEK 2 microbial identification system, (bioMérieux, Lyon, France). MICs were determined using E-tests (AB Biodisk, Sweden and Liofilchem, Italy). The interpretative criteria recommended by the CLSI (2010) and by EUCAST (2011, 2012) were applied.
Additionally, vancomycin MIC data of all CoNS strains isolated from blood cultures of patients aged <90 days, admitted to our hospital during the study period, were extracted from the database of the Clinical Microbiology Department.
Assessment of late onset sepsis (LOS) outcome
Outcome was assessed in patients with culture proven sepsis and categorised as follows: (1) eradication – negative culture within 72 h of vancomycin treatment and clinical improvement (stabilization of hemodynamics and resolution of respiratory distress symptoms); (2) presumed eradication – repeat blood culture not taken within 72 h of vancomycin treatment and clinical improvement; (3) persistence – phenotypically similar microorganisms isolated from blood after 72 h of vancomycin treatment; (4) presumed persistence – blood culture not taken and no clinical improvement or worsening of clinical condition; (5) new infection – phenotypically different CoNS spp. in blood culture after at least 72 h of vancomycin treatment; (6) relapse – positive blood culture with phenotypically similar microorganism more than 96 h after completion of vancomycin treatment. In the PK/PD analysis the first two categories were classified as success and all others as failure, including one death.
PK/PD analysis
A two-step approach as described below was employed
Anderson population model
Population PK analysis with 1-compartment linear model, zero-order input (1 h intravenous infusion) and 1-order elimination as described by Anderson et al. was used to estimate population parameters for clearance (Cl) and volume of distribution (Vd) [20]. Cl was standardised to a 70-kg person using allometric scaling (Fal = [Wt/70]0.75). Hill equation was used to estimate the maturation of Cl in Anderson model: FPMA = PMA^(HillCl)/(PMA^HillCl + EMATCl_50^HillCl). Renal function (RF) standardized to a 70-kg person was estimated as a component of creatinine production rate (CPR = 516 × exp(K_age × [(PMA − 40)/12]) μmol h − 1) and serum creatinine. Serum creatinine values, mean ± SD assuming a log-normal distribution, were fixed according to PMA and were based on previously published data [21]. Simulations showed that when applying renal function component as described by Anderson et al. the Cl values were positively skewed [20]. Thus, simulation procedure the RF component was fixed as 1 to avoid distorting the values.
Vd was standardised to a 70-kg person using allometric coefficient 1 (Fal = Wt/70). In the Anderson model, significant covariates were weight and PMA, hence, Cl and Vd was generated for eight PMA groups with respective weight categories. Significant covariates were continuous positive airway pressure (CPAP) ventilation for Cl, increasing clearance by 3%, and the use of inotropes for Vd, increasing Vd by 19% [20].
TDM population model
A two-compartmental population PK model parameterized by Cl, intercompartmental clearance (Q), distribution volume in central compartment (Vc) and distribution volume in peripheral compartment (Vp) was created. Bayesian posterior distribution of model parameters were estimated using nonparametric adaptive grid algorithm for study patients based only on their TDM values [22].
Simulations of target attainment with current dosing
Simulations were carried out using the above described models. First, Anderson's popPK model was used with collected subjects’ covariate information for retrieval of individual PK parameters. Individual AUC values were evaluated from: AUC = (24*D)/(CL*tau), where tau equals the interval between infusions (h). Second, TDM population model based on individual Bayesian posterior predictions were used and fitted concentration curves were constructed for each subject. Twenty four hour individual AUCs at steady state were calculated using the trapezoidal approximation method of fitted concentration curves.
1000 virtual MIC values were generated by bootstrapping vancomycin MICs of CoNS isolates in our database. A discrete distribution of variables was assumed. AUC values obtained by both methods were bootstrapped to 1000 virtual subjects along with MIC values and 500 such data sets were simulated for AUC/MIC targets. PTA values of 80% and 90% were found over target levels of AUC/MIC > 400 and AUC/MIC > 300. The higher target was chosen as being associated with clinical efficacy in adult MRSA pneumonia and the most frequently quoted also in neonatal PKPD simulation studies in recent years [23]. A lower target was also tested, as different pathogen structure and disease (blood stream vs lung tissue penetration) as well as lower protein binding suggest lower optimal exposure for neonates. Empirical confidence intervals were identified from performed simulations.
Calculation of vancomycin doses needed for therapeutic target attainment
Using Monte Carlo simulations (MCS), vancomycin doses needed to achieve 80% and 90% PTA of AUC/MIC > 400 and AUC/MIC >300 were estimated for 1000 virtual subjects. Vancomycin MIC distribution of CoNS isolates from our database and fixed MIC values of 1, 2 and 4 mg/L were used as base levels for target simulations. The Cl and Vd derived from the Anderson population model, predicted with and without CPAP ventilation and inotropes, were used to calculate individual AUC and vancomycin MIC values of CoNS isolates. AUC and MIC values were bootstrapped assuming discrete distribution. Simulated vancomycin doses needed to achieve 90% and 80% PTA of AUC/MIC >400 and AUC/MIC >300 and model predicted Cl for each PMA group were used to calculate corresponding vancomycin maximum concentrations (Cmax) and Ctroughs at steady state.
Correlation of AUC/MIC with outcome
Dosing data and Ctrough concentrations of the study population were used to estimate individual AUC/MIC values in subjects with positive blood cultures. Multiple LOS episodes were handled as separate cases if at least 96 h interval between vancomycin treatment episodes was present. Individual AUC/MIC estimates were obtained matching specific case-wise averaged AUC values with the corresponding MIC values. In case of mixed infections AUC/MIC values were obtained for each isolate separately.
All calculations were performed with the R Project for Statistical Computing (version 2.15.2 (2012-10-26), The R Foundation for Statistical Computing) and Pmetrics package [22, 24]. Comparison of PK characteristics was done with Mann–Whitney-Wilcoxon test and outcome association to AUC/MIC with Kruskal-Wallis chi-squared test.
The protocol was approved by the Ethics Committee of the University of Tartu. Informed consent was not needed due to retrospective nature of the study.
Results
Study population
In total, of 201 vancomycin TDM measurements from 80 eligible patients were registered in the laboratory database. Medical records of four patients were not available and they were excluded. The final dataset included 76 patients with 88 vancomycin treatment episodes and 186 TDM data points; in 83 episodes vancomycin was given for more than 72 h. In 5 cases, one treated for suspected meningitis, three without confirmed infection and two with Gram-negative infection, vancomycin treatment was discontinued. Among vancomycin treated patients 57 episodes were culture proven, seven with two different Gram-positive microorganisms.
Demographic parameters of the study population are shown in Table 2. Overall 39/57 patients with proven LOS had successful outcome (eradication – 37, presumed eradication – 2) and 18/57 were classified as failures (persistence – 10, presumed persistence – 1, new infection – 5, relapse – 2).
Microorganisms
Vancomycin MIC distribution of all 187 neonatal CoNS blood isolates is shown in Fig. 1. The median MIC value was 1.0 mg/L (range 0.2–3.0; IQR, 0.8–1.5); 59% of isolates had a MIC ≤1.0 mg/L. Among study patients 99/104 blood cultures were positive for CoNS (S. haemolyticus 38, S. epidermidis 37, S. hominis 12, S. warneri 8, S. capitis 1, S. saprophyticus 2, S. lentus 1), 4/104 for E. faecalis and 1/104 for S. parasanguis. Their median MIC value was 1.0 mg/L (range 0.5–3.0); similar to the entire CoNS dataset.

Distribution of vancomycin MIC values of all neonatal blood CoNS isolates from the Tartu University Hospital in 2010–2012
PK characteristics of the study population
Vancomycin TDM measurements were taken after the 1st to 44th dose (median 5; IQR 3–8) between 4.5 h and 24 h after the start of infusion. The median number of TDMs per patient was 2 (range 1–9); Ctrough of 5–10 mg/L was achieved in 63.6% and 10–15 mg/L in 20.5% of cases. There were 9.3% and 7.3% samples with vancomycin concentration below 5 mg/L and above 15 mg/L, respectively.
PK parameters (shown as mean ± SD) obtained from the Anderson model were Vd = 0.61 ± 0.05 L/kg; Cl = 0.06 ± 0.01 L/h*kg and parameters obtained from the popPK model were Vc = 0.13 ± 0.06 L/kg; Cl = 0.06 ± 0.02 L/h*kg; Q = 0.36 ± 0.10 L/h*kg; Vp = 0.76 ± 0.22 L/kg.
Mean (SD) vancomycin AUC values obtained in TDM and the Anderson model were similar 280.6 ± 102.0 mg/kg*L and 287.1 ± 74.2 mg/kg*L, respectively. AUC values throughout the studied GA range were similar (data not shown).
Clinical outcome vs AUC/MIC in subjects with culture proven sepsis
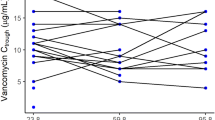
Only 34% and 12% of subjects with positive blood cultures achieved AUC/MIC ≥300 and AUC/MIC ≥400, respectively. Clinical outcome and individual AUC/MIC values of culture positive LOS episodes are shown in Fig. 2. The AUC/MIC ratio between patients with clinical success (median 268.6; IQR 130.7–326.5) and failure (median 210.1; IQR 149.5–319.1) was similar.

Boxplot of TDM based vancomycin AUC/MIC and clinical outcome of culture proven LOS. Black bold line is median and whiskers show lower and upper quartiles
PTA in study population
MCS results of 90% PTA in the whole study population with current dosing are presented in Fig. 3. Target of AUC/MIC >300 was achieved in less than 40% and AUC/MIC >400 in less than 25% of subjects regardless of used calculation method.

90% PTA with 95% confidence intervals (error bars) with the current dosing for MIC distribution of neonatal blood isolates in the study group, AUC calculation was based on TDM and Anderson model [19]
Vancomycin doses required for 80% PTA
Simulated daily doses of vancomycin required for 80% PTA by PMA band are shown in Tables 3 and 4, respectively. Since only 25% of TDM patients were receiving CPAP and 46% were supported with inotropes, only data of non-CPAP with the use of inotropes are presented. For 80% PTA of AUC/MIC >300 the calculated doses were similar to those in NeoFax up to MIC of 2.0 mg/L, inclusive. The corresponding Ctrough values remained ≤20 mg/L, whereas for MIC of 4.0 mg/L the corresponding vancomycin Ctrough levels ranged between 21.8–31.6 and 28.7–41.0 mg/L for AUC/MIC >300 and AUC/MC >400, respectively. Mean actually used vancomycin doses (data not shown) were below those required for 80% PTA of AUC/MIC >300 and AUC/MIC >400 for MIC of ≥2.0 mg/L and for AUC/MIC >400 for MIC distribution of all neonatal blood CoNS isolates from our hospital.
Discussion
Based on vancomycin TDM results and actual MIC values of neonatal CoNS isolates we showed that with currently recommended NeoFax dosing regimen the 80% PTA of AUC/MIC >400 and AUC/MIC >300 is achievable only in less than half of infected neonates. Furthermore, targeting less susceptible organisms (MIC values of >2.0 mg/L) achievement of 80% PTA of AUC/MIC >400 would require the use of much higher vancomycin doses that result in Ctrough levels well above 20 mg/L. These results suggest that current dosing recommendations in NeoFax [and likely also in British National Formulary (BNF)] may not be adequate for treatment of neonatal CoNS sepsis. The same conclusion was reached by authors who studied vancomycin Ctroughs achieved by neonates and compared these to vancomycin MICs of CoNS isolates [25].
However, when interpreting these results several outstanding issues remain before firm conclusions can be drawn for everyday practice. First, the most appropriate AUC/MIC ratio for treatment of CoNS infections that are predominantly BSI rather than deep-sided infections has been defined neither in neonates nor in adults. In a recent study Ramos-Martín et al. used hollow fibre infection model (HFIM) and a novel rabbit model of neonatal central-line associated blood stream infections (CLABSI) and bridged these data to neonates using popPK techniques and MCS. Both experimental models suggested higher AUC/MIC targets for neonates (665 for the HFIM and 520 for the CLABSI model) than are currently proposed for adult MRSA infection to achieve maximal killing, prevent emergence of a resistant subpopulation and suppress C-reactive protein in the setting of a retained central line [26]. Whether such high levels are required or can be safely used in clinical settings for every (premature) neonate if central line is removed or if vancomycin is given empirically or if clinical rather than culture proven LOS is managed, is still debatable and will be tested in a clinical study before recommendation for clinical practice can be made [27]. In contrast, other experimental data of thigh infection in mice suggest that the required AUC/MIC ratio for treatment of CoNS infection is about 2.5 to 3 times lower than that required for treatment of S.aureus infection [8]. Moreover, higher free drug concentration can be assumed in neonates due to lower drug protein binding capacity of neonatal plasma and elevated bilirubin which competes with drugs for binding sites to albumin [15–17].
Our findings that there was no association between AUC/MIC ratio and outcome do not prove that such association does not exist. First, one should bear in mind these data are retrospectively collected and thus outcome measures may be prone to bias. Second, it may well be that AUC/MIC ratio of 300 and 400 assessed by us are too similar to detect difference between these two ratios. We believe that more data with a larger dataset in clinical CoNS infections are needed in terms of optimal AUC/MIC ratio before firm conclusions on adequacy of current dosing recommendations can be drawn.
We and others have shown that to achieve AUC/MIC value of 400 the vancomycin trough levels around 10 mg/L or slightly higher are required provided that MIC value of an infecting organisms is ≤1 mcg/ml. The latter was the median value of Gram positive isolates in our hospital as well. If however, the distribution of actual isolates was used in simulations it appeared that only approximately 35% of neonates achieved AUC/MIC values of 300 and less than 22% of 400 suggesting that these targets are not achieved with current dosing in the majority of patients. However, one should emphasize once again that we still do not know whether these targets are required at all.
We have recently shown that in fact 75% of vancomycin doses used in European NICUs are lower than recommended by BNF (and also by NeoFax) [28]. We speculated that one reason for that might a fear of toxicity by neonatologists but acknowledge that this was not specifically studied by us. Association between vancomycin Ctrough and risk of nephrotoxicity as a function of intensity and duration of therapy, compounded by additional risk factors, is suggested but data in the literature are too inconsistent to demonstrate direct causal relationship with kidney or to define certain nephrotoxic levels for neonates [29, 30]. Steady-state concentration of ≥28 mg/L has been associated with increased risk of renal toxicity in patients treated with continuous infusions [31]. Studies with intermittent treatment have suggested Ctrough level >15 mg/L for increased risk of nephrotoxicity in adults and children [32, 33]. Applying Ctrough 15 mg/L as nephrotoxic breakpoint all doses needed for achievement of AUC/MIC >300 and AUC/MIC >400 for pathogens with MIC ≥2.0 mg/L resulted in nephrotoxic values or remained slightly lower in more mature neonates. Studies evaluating long term effects of vancomycin therapy on hearing in neonates are almost entirely missing [34, 35]. Thus far there is no indication on vancomycin ototoxicity [36]. Such studies are complex and should include control group as several neonatal conditions (e.g. hypoxia, sepsis, bronchopulmonary dysplasia, genetic abnormalities etc.) have been associated with hearing disturbances [37].
Although numerous studies on vancomycin PK using various models and popPK approach have been published almost all of them including our study are based on the samples collected for TDM purposes in everyday practice and are thus prone to high variability in sample collection and used laboratory methods; all this affecting final results [38, 39]. Prospectively designed studies with rich or semi-rich sampling are scarce or outdated in neonates [40]. At present NeoVanc project sponsored by EU FP7 is aiming to fill these gaps. The project aims to define the most optimal PD target using in vitro hollow fibre and in vivo rabbit model of CoNS sepsis. The preclinical data will be validated in the multicentre randomised controlled trial comparing efficacy and safety of standard to optimised vancomycin dosing regimen in neonates and infants with sepsis caused by CoNS. The long term effects of vancomycin blood concentrations on renal and hearing function will be evaluated as well [27].
Several limitations of the study need to be noted. The relatively small number of participants in each GA band may have under- or overestimated the within group variability. Due to the retrospective nature only Ctrough data were available, as monitoring of peak concentration has been found of no value in guiding vancomycin therapy [9]. Concomitant medications and underlying illness may have influenced PK of vancomycin and minor fluctuations may have occurred in recorded Ctrough collection time. Microbiological outcome may have been affected by combination of antibacterial drugs used in the beginning of the treatment episode.
Conclusions
Currently recommended dosing regimens are not appropriate to achieve vancomycin PK/PD target of AUC/MIC >400, as recommended for adult MRSA infection, or even AUC/MIC >300, since the target is reached in less than 40% of neonates with sepsis. Adequately designed preclinical and clinical studies should first establish optimal PK/PD targets for CoNS BSI, second define optimal dosing regimen to achieve these targets for premature neonates and third to identify prevalence and risk factors of vancomycin induced nephro- and ototoxicity among neonates in long term follow up studies. When making recommendations for treatment of CoNS infection in neonates appropriate balance between relatively benign outcome and potential toxicity should be weighted.
Abbreviations
- AUC/MIC:
-
Area under the curve to minimal inhibitory concentration ratio
- BNF:
-
British national formulary
- BSI:
-
Blood stream infection
- BW:
-
Birth weight
- Cl:
-
Clearance
- CLABSI:
-
Central-line associated blood stream infection
- CLSI:
-
The clinical & laboratory standards institute
- Cmax :
-
Maximum concentration
- CoNS:
-
Coagulase-negative staphylococcus
- CPAP:
-
Continuous positive airway pressure
- CPR:
-
Creatinine production rate
- Ctrough :
-
Trough concentration
- CW:
-
Current weight
- EUCAST:
-
The European committee on antimicrobial susceptibility testing
- FP7:
-
Seventh framework programme for research and technological development
- GA:
-
Gestational age
- HFIM:
-
Hollow fibre infection model
- LOS:
-
Late onset sepsis
- MCS:
-
Monte Carlo simulation
- MRSA:
-
Methicillin-resistant staphylococcus aureus
- PKPD:
-
Pharmacokinetic-pharmacodynamic
- PMA:
-
Postmenstrual age
- PNA:
-
Postnatal age
- PopPK:
-
Population pharmacokinetics
- PTA:
-
Probability of the target
- Q:
-
Intercompartmental clearance
- RF:
-
Renal function
- TDM:
-
Therapeutic drug monitoring
- Vc:
-
Distribution volume in central compartment
- Vd:
-
Volume of distribution
- Vp:
-
Distribution volume in peripheral compartment.
References
Bizzarro M, Shabanova V, Baltimore R, Dembry L, Ehrenkranz R, Gallagher P. Neonatal sepsis 2004–2013: the rise and fall of coagulase-negative staphylococci. J Pediatr. 2015;166:1193–9.
Dong Y, Speer CP. Late-onset neonatal sepsis: recent developments. Arch Dis Child Fetal Neonatal Ed. 2015;100:F257–63.
Diekema DJ, Pfaller MA, Schmitz FJ, Smayevsky J, Bell J, Jones RN, et al. Survey of infections due to staphylococcus species: frequency of occurrence and antimicrobial susceptibility of isolates collected in the United States, Canada, Latin America, Europe, and the Western Pacific Region for the SENTRY antimicrobial surveillance program. Clin Infect Dis. 2001;32 Suppl 2:S114–32.
Isaacs D. A ten year, multicentre study of coagulase negative staphylococcal infections in Australasian neonatal units. Arch Dis Child - Fetal Neonatal Ed. 2003;88:F89–93.
Stockmann C, Hersh AL, Roberts JK, Bhongsatiern J, Korgenski EK, Spigarelli MG, et al. Predictive performance of a vancomycin population pharmacokinetic model in neonates. J Infect Dis Ther. 2015;4:187–98.
Labreche MJ, Graber CJ, Nguyen HM. Recent updates on the role of pharmacokinetics-pharmacodynamics in antimicrobial susceptibility testing as applied to clinical practice. Clin Infect Dis. 2015;61:1446–52.
Stockmann C, Roberts JK, Yu T, Constance JE, Knibbe CAJ, Spigarelli MG, et al. Vancomycin pharmacokinetic models: informing the clinical management of drug-resistant bacterial infections. Expert Rev Anti Infect Ther. 2014;12:1371–88.
Leiva ML, Imbett S, Gómez PJ, González M, Rodriguez AC, Agudelo M, et al. Successful Growth of Staphylococcus epidermidis in the Neutropenic Mouse Thigh Infection Model (NMTIM) without the Use of a Foreign Body. Pap Present 54th Intersci Conf Antimicrob Agents Chemother. Washington: ICAAC; 2014.
Rybak M, Lomaestro B, Rotschafer JC, Moellering R, Craig W, Billeter M, et al. Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American society of health-system pharmacists, the infectious diseases society of America, and the society of infectious diseases pharmacists. Am J Health Syst Pharm. 2009;66:82–98.
Le J, Bradley JS, Murray W, Romanovski GL, Tran TT, Nguyen N, et al. Improved vancomycin dosing in children using area under the curve exposure. Pediatr Infect Dis J. 2013;32:e155–63.
Frymoyer A, Hersh LA, El-Komy HM, Gaskari S, Su F, Drover RD, et al. Association between vancomycin trough concentration and AUC in neonates. Antimicrob Agents Chemother. 2014;58:6454–61.
Nicasio AM, Bulitta JB, Lodise TP, D’Hondt RE, Kulawy R, Louie A, et al. Evaluation of once-daily vancomycin against methicillin-resistant Staphylococcus aureus in a hollow-fiber infection model. Antimicrob Agents Chemother. 2012;56:682–6.
Neely MN, Youn G, Jones B, Jelliffe RW, Drusano GL, Rodvold KA, et al. Are vancomycin trough concentrations adequate for optimal dosing? Antimicrob Agents Chemother. 2014;58:309–16.
Berthoin K, Ampe E, Tulkens PM, Carryn S. Correlation between free and total vancomycin serum concentrations in patients treated for Gram-positive infections. Int J Antimicrob Agents. 2009;34:555–60.
Notarianni JL. Plasma protein binding of drugs in pregnancy and in neonates. Clin Pharmacokinet. 1990;18:20–36.
Brodersen R, Honoré B. Drug binding properties of neonatal albumin. Acata Paediatr Scand. 1989;78:342–6.
Robertson A, Brodersen R. Effect of drug combinations on bilirubin-albumin binding. Dev Pharmacol Ther. 1991;17:95–9.
Marakala V, Avinash SS, Shivashankara AR, Malathi M, Kumar A. Serum creatinine assay: enzymatic vs kinetic Jaffe’s method. J Evol Med Dent Sci. 2012;1:328–34.
Young TE, Magnum B. Neofax. 23rd ed. Montvale: Thomas Reuters; 2010.
Anderson BJ, Allegaert K, Van den Anker JN, Cossey V, Holford NHG. Vancomycin pharmacokinetics in preterm neonates and the prediction of adult clearance. Br J Clin Pharmacol. 2006;63:75–84.
Cuzzolin L, Fanos V, Pinna B, di Marzio M, Perin M, Tramontozzi P, et al. Postnatal renal function in preterm newborns: a role of diseases, drugs and therapeutic interventions. Pediatr Nephrol. 2006;21:931–8.
Neely MN, van Guilder MG, Yamada WM, Schumitzky A, Jelliffe RW. Accurate detection of outliers and subpopulations with Pmetrics, a nonparametric and parametric pharmacometric modeling and simulation package for R. Ther Drug Monit. 2012;34:467–76.
Moise-Broder PA, Forrest A, Birmingham MC, Schentag JJ. Pharmacodynamics of vancomycin and other antimicrobials in patients with Staphylococcus aureus lower respiratory tract infections. Clin Pharmacokinet. 2004;43:925–42.
R Core Team. R: A Language and Environment for Statistical Computing. Vienna: R foundation for statistical computing; 2012.
Sinkeler FS, de Haan TR, Hodiamont CJ, Bijleveld YA, Pajkrt D, Mathôt RAA. Inadequate vancomycin therapy in term and preterm neonates: a retrospective analysis of trough serum concentrations in relation to minimal inhibitory concentrations. BMC Pediatr. 2014;14:193–8.
Ramos-Martín V, Johnson A, Livermore J, McEntee L, Whalley S, Docobo-Pérez F, et al. Pharmacodynamics of vancomycin for CoNS infection: experimental basis for optimal use of vancomycin in neonates. J Antimicrob Chemother. 2016;71:992–1002.
NeoVanc. Available from: http://www.neovanc.org/en/ Accessed 30 Jun 2015
Metsvaht T, Nellis G, Varendi H, Nunn AJ, Graham S, Rieutord A, et al. High variability in the dosing of commonly used antibiotics revealed by a Europe-wide point prevalence study: implications for research and dissemination. BMC Pediatr. 2015;15:41–50.
Martin JH, Norris R, Barras M, Roberts J, Morris R, Doogue M, et al. Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Clin Biochem Rev. 2010;31:21–4.
de Hoog M, Mouton JW, van den Anker JN. Vancomycin: pharmacokinetics and administration regimens in neonates. Clin Pharmacokinet. 2004;43:417–40.
Ingram PR, Lye DC, Tambyah PA, Goh WP, Tam VH, Fisher DA. Risk factors for nephrotoxicity associated with continuous vancomycin infusion in outpatient parenteral antibiotic therapy. J Antimicrob Chemother. 2008;62:168–71.
Cano EL, Haque NZ, Welch VL, Cely CM, Peyrani P, Scerpella EG, et al. Incidence of nephrotoxicity and association with vancomycin use in intensive care unit patients with pneumonia: retrospective analysis of the IMPACT-HAP Database. Clin Ther. 2012;34:149–57.
McKamy S, Hernandez E, Jahng M, Moriwaki T, Deveikis A, Le J. Incidence and risk factors influencing the development of vancomycin nephrotoxicity in children. J Pediatr. 2011;158:422–6.
de Hoog M, van Zanten AB, Hop CW, Overbosch E, Weisglas-Kuperus N, van den Anker NJ. Newborn hearing screening: Tobramycin and vancomycin are not risk factors for hearing loss. J Pediatr. 2003;142:41–6.
Vella-Brincat JWA, Begg EJ, Robertshawe BJ, Lynn AM, Borrie TL, Darlow BA. Are gentamicin and/or vancomycin associated with ototoxicity in the neonate? A retrospective audit. Neonatology. 2011;100:186–93.
Lestner JM, Hill LF, Heath PT, Sharland M. Vancomycin toxicity in neonates: a review of the evidence. Curr Opin Infect Dis. 2016 [Epub ahead of print]
Maqbool M, Najar BA, Gattoo I, Chowdhary J. Screening for hearing impairment in high risk neonates: A hospital based study. J Clin Diagn Res. 2015;9:SC18–21.
Oyaert M, Peersman N, Kieffer D, Deiteren K, Smits A, Allegaert K, et al. Novel LC–MS/MS method for plasma vancomycin: Comparison with immunoassays and clinical impact. Clin Chim Acta. 2015;441:63–70.
Zhao W, Kaguelidou F, Biran V, Zhang D, Allegaert K, Capparelli EV, et al. External evaluation of population pharmacokinetic models of vancomycin in neonates: The transferability of published models to different clinical settings. Br J Clin Pharmacol. 2013;75:1068–80.
Pacifici G, Allegaert K. Clinical pharmacokinetics of vancomycin in the neonate: a review. Clinics. 2012;67:831–7.
Acknowledgements
The authors would like to thank study nurse Eve Kaur who helped to create study database.
Funding
The study was supported by Institutional grant of Estonian Science Foundation (IUT-15024); EU FP7 funded Archimedes Foundation Project (No 3.2.1001.11–0032); Estonian Science Foundation (PUT-1197).
Availability of data and materials
We will make our de-identified data available on request.
Administrative permission was required to access database of Tartu University Hospital health records.
Authors’ contributions
HP – study design, data collection and study coordination, data analysis, manuscript writing. KO – study design, data analysis, manuscript writing. TT – PK/PD analysis and modelling, manuscript writing. TM – study design, data analysis, manuscript writing. KL – microbiological testing and interpretation. IL – study design, data interpretation, manuscript writing. All authors approved the manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The protocol was approved by the Ethics Committee of the University of Tartu. Informed consent was not needed due to retrospective nature of the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Padari, H., Oselin, K., Tasa, T. et al. Coagulase negative staphylococcal sepsis in neonates: do we need to adapt vancomycin dose or target?. BMC Pediatr 16, 206 (2016). https://doi.org/10.1186/s12887-016-0753-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-016-0753-0