
Abstract
Background
Hepatitis B virus (HBV) infection is a global public-health problem. Since the introduction of an effective vaccine, the epidemiology of HBV infection is changing. We aimed to estimate the prevalence of HBV infection in the Gulf Cooperation Council (GCC) region and delineate any variation in member-countries, special sub-groups, and over time.
Methods
This is a systematic review and meta-analysis to review studies of HBV prevalence in the GCC region. Databases were searched and all studies from inception to July 31st, 2021, were considered for inclusion. The pooled HBV prevalence was analyzed using the random-effect model after assessment for heterogeneity. True prevalence was adjusted using the Rogan-Gladen estimator. Pre-defined subgroup analysis was performed, and publication bias was assessed.
Results
Overall, 99 studies (n = 1,944,200 participants) met the inclusion criteria. The overall HBV apparent prevalence was 3.05% (95% CI 2.60, 3.52) and the true prevalence was 1.67% (95% CI 1.66, 1.68). The apparent prevalence varied between subgroups. Over time, the apparent prevalence of HBV infection has declined from 9.38% (95% CI 7.26, 11.74) before 1990 to 1.56% (95% CI 1.07, 2.12) during the period 2010 to 2020.
Conclusion
Over the last four decades the overall prevalence of HBV infection in the GCC region has decreased from high- to low-endemicity level. However, due to poor methodology of the included studies, further high-quality community-based studies are needed to obtain more precise estimate of HBV infection in this region.
Similar content being viewed by others


Introduction
Hepatitis B Virus (HBV) infection is a global health problem with an estimated 2 billion people worldwide exposed to the virus [1]. In 2019, the World Health Organization (WHO) estimated that approximately 296 million people worldwide are chronically infected by HBV making it one of the most common chronic infections on a global scale [2]. Patients with HBV infection have been shown to exert more health and economic burden on society compared to other patients [3, 4]. Despite the high morbidity and mortality associated with HBV infection, it remains a preventable disease. A DNA recombinant vaccine against HBV was approved and introduced into clinical practice in 1986 [5]. It was shown to be effective at reducing the risk of chronic HBV infection and subsequently reducing the risk of HBV-related complications [6].
The Gulf Council Cooperation (GCC) is a regional, intergovernmental, political and economic union located in the Middle East next to the Arabian gulf [7]. This union consists of 6 neighboring countries namely Kingdom of Saudi Arabia (KSA), Kuwait, United Arab Emirates (UAE), Bahrain, Oman and Qatar with an estimated combined population of 54 million people. These countries share many social, economic and cultural properties which makes it a distinctive union. Furthermore, these countries are unique in the Middle East region in being high-income countries with high Human Development Index hence sharing many of the properties of developed countries [8]. This may suggest that the HBV burden in this area is similar to developed countries. On the other hand, half of the people living in this region are non-nationals that come from areas of high HBV prevalence such as Africa and Asia. This matter is complicated further by the policies in the GCC that limits non-nationals from obtaining residency visa in case of HBV infection. Furthermore, universal childhood vaccination and mass vaccination programs against HBV likely resulted in lowering HBV prevalence in the GCC [9]. Although, there is no estimate of the overall HBV prevalence in the GCC region, the WHO estimates that 3.3% of the general population living in the Eastern Mediterranean region (EMR) are infected with HBV [10]. On the other hand, older studies from the GCC countries suggest that HBV infection may be hyperendemic in certain parts of the area [11].
Accurate estimate of the true prevalence of HBV infection in the GCC region is important to measure the burden of the infection and the outcomes of the practiced control measures. This ensures adequate resources are allocated by governments to tackle this public-health problem and achieve HBV elimination by 2030 as endorsed by Global Health Sector Strategy (GHSS) [2]. This systematic review and meta-analysis aims to review relevant studies of HBV infection prevalence in the GCC area, in order to; (1) estimate an overall prevalence of HBV for the GCC region and each of the member countries, (2) assess the change in the prevalence of HBV infection in the GCC over time, (3) estimate the prevalence of some population subgroups and risk groups in the region.
Methods
A systematic literature review and meta-analysis were conducted employing a predefined protocol based on Cochrane[12] and adhered to the reporting guidelines recommended by the Preferred Reporting Items for Systematic Review and Meta-analysis (Additional file 1: PRISMA) [13].
Search strategy, selection criteria and quality assessment
The research question was defined using PIOST. The inclusion criteria included observational studies regardless of the design (cross-sectional, cohort and case–control), published in peer-reviewed literature, and grey literature in any language up to July 2021, studied people of both gender, children and adults (older than 18 years), living in the GCC region during the study period and in all settings (healthcare and community-based studies). The status of HBV infection was assessed using a validated test to detect hepatitis B surface antigen (HBsAg), including Reverse Phase Passive Hemagglutination, Enzymes-linked Immunosorbent Assay (ELISA), Chemiluminescent Immunoassays, Chemiluminescent Microparticle Immunoassays (CMIA) and Radioimmunoassay.
The literature search used Medline, EMBASE and Global health databases, and both thesaurus searching (using MeSH) and free-text searching. Search options such as truncations and wild cards were utilized. Boolean operators and the subject headings comparable to the search terms were used when available. In addition, the reference list of reviewed articles were screened for any available references. EndNote™ (version 20.1) software was used as the reference manager for the study. The details of the search strategy are shown in Additional file 2: Appendix A1.
The retrieved study titles were screened, and the study was excluded if it did not relate to the study topic or duplicate. The abstracts of the remaining studies were screened and excluded if irrelevant. The full texts of the remaining studies were retrieved and their references searched for eligible articles. For the articles that were not immediately available, the authors and/or the journal were contacted to obtain a copy of the study. After full text assessment, studies that fulfilled the inclusion criteria were included in this study. The study screening and study selection was performed by the first author only.
Quality assessment
Quality assessment of the included studies was performed using a standard tool (Additional file 2: Appendix B) that consists of criteria adapted from Cochrane guidelines [12] and Downs & Black guidelines for cross-sectional studies [14]. The tool assigned a score for different domains and a total score was calculated. Different tools were available for different study designs (cross-sectional, cohort and case–control). The assessment tool for cross-sectional studies measured the following: representativeness of the sample to the target population, measurement of the exposure using a valid tool, recognizing and addressing main potential confounders, utilizing and descripting appropriate statistical tools, addressing missing data, reporting confidence intervals, and estimating random variability in the data for the main outcome. For cohort and case–control studies, the tool measured similar variables with slight variation. The studies were categorized into “low”- and “high” quality based on the quality assessment tool using a cutoff of ≥ 5 points for cross-sectional studies, ≥ 6 points for case–control studies and ≥ 7 points for cohort studies with higher score corresponding to higher quality.
Extracting relevant data
Data extraction of the included studies was done systematically using data extraction forms and data were entered into database. The study population was categorized according to the perceived risk of acquiring HBV infection to, high-risk group that includes hemodialysis patients, Persons Who Inject Drugs (PWID), people with liver disease, patients who required repeated blood transfusion such as hereditary hemolytic anemia (e.g. sickle cell anemia and thalassemia) and congenital coagulopathy, and average-risk group that represents the general population, pregnant women, blood donors, army recruits, healthy adults/children, controls from case–control studies and health-care workers. The decision to include health-care workers in this category is related to the fact that despite their risk of exposure to HBV at work, they are usually fully vaccinated and they apply prophylactic measures of HBV transmission. This system was adopted with modification from a previously published study[15].
Analysis strategy
Meta-analyses were performed using STATA (version 15.1). Estimates were pooled using a DerSimonian-Laird random effect model which assumes that the true effect size could vary from study to study, and the true effects are normally distributed [16]. The magnitude of variation between studies due to heterogeneity was quantified using the Higgin’s I2 statistics and Cochran’s Q test. An I2 statistics was interpreted as percentages with values of 25%, 50% and 75% approximately corresponding low, moderate and high between-study heterogeneity [17]. A Cochran’s Q test p-value < 0.1 was consistent with significant heterogeneity. The fixed-effect model was used when heterogeneity was low, whereas the random-effect model was used when heterogeneity was high. In addition, a sensitivity analysis was performed after excluding studies with low quality measurement. Forrest plots with description of the findings were generated to present the results and calculate the point estimate and the 95% CI. Publication bias was assessed using Egger’s test and funnel plot. The pooled apparent prevalence was adjusted using the sensitivity and specificity of the used test to calculate the true prevalence according to Rogan-Gladen [18]. The true prevalence for studies that used ELISA [sensitivity 98% and specificity 97%] [19] and CMIA [sensitivity 88.9% and specificity 98.9%] [20] were calculated using the reported sensitivity and specificity of the test used and the pooled estimate from the meta-analysis.
Results
Literature search
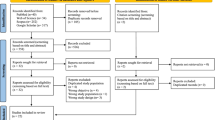
The flow diagram (Fig. 1) shows the number of articles identified, screened, and included in the systematic review. A total of 709 records were identified from the three searched databases. After removal of duplicates, the remaining records had the title and abstract screened for eligibility. Additional 406 records were excluded for ineligibility based on the initial screen. For the remaining records, full text was sought for retrieval and assessed for inclusion based on the inclusion criteria. References of potentially eligible records were screened for any additional studies not identified by the search strategy which identified 6 additional records. Out of the 148 records sought for full-text retrieval, 136 records were obtained. The remaining 12 records were unobtainable despite contacting the authors and/or journal (Additional file 2: Appendix A2). Finally, 37 records were excluded for reasons shown in Fig. 1, leaving 99 studies fulfilling the inclusion criteria and included in the final analysis.

PRISMA flow diagram showing the number of articles identified, screened and included
Study characteristics
The study characteristics are summarized in Table 1. The included 99 studies were in English language and covered the period from 1981 to 2020. Detailed summary of studies’ characteristics is shown in Additional file 2: Appendix C. Most studies were performed in KSA (n = 75) [10, 21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91], followed by Kuwait (n = 5) [92,93,94,95,96], UAE (n = 5) [97,98,99,100,101], Oman (n = 5) [102,103,104,105,106], Qatar (n = 4) [107,108,109,110] and finally Bahrain (n = 3) [111,112,113]. There was one study that was performed in both Bahrain and KSA [114] and another that included Oman, UAE and Qatar [115]. The average sample size of the country-specific studies varied, and while KSA had the highest number of studies, Bahrain had the largest number of sample size and contributed a higher proportion (45.5%) of studied participants in the GCC. Most studies were cross-sectional in design (n = 63), followed by retrospective cohort (n = 30), case–control (n = 5) and finally one prospective cohort study (n = 1). Most studies were peer-reviewed published studies (n = 94), but 4 studies were published as abstracts and one study was a PhD thesis. Most of the included studies (n = 87) were based entirely or partially in a health-care facility, while five were community-based [32, 33, 55, 67, 71]. ELISA was the most used diagnostic test (71 studies) followed by CMIA (7 studies). All studies reported apparent prevalence only.
Overall prevalence and by country
The estimated overall HBV prevalence in the GCC region was 3.05% (95% CI 2.60, 3.52%). The prevalence rates varied according to countries (Table 1, Forest plots and Additional file 2: Appendix D). The prevalence of HBV infection among the GCC countries varied between 0.80% in UAE to 3.73% in Oman (Fig. 2).

Geographical variation in hepatitis B virus prevalence among member countries of the Gulf Cooperation Council (source of figure: infogram.com)
True prevalence
Calculating the true HBV prevalence resulted in lower estimate in the GCC and all individual countries (Table 2).
Prevalence over time
Prior to the introduction of HBV vaccine in the early 1990s, the GCC region had a HBV prevalence of 9.38%, placing it in the high-endemicity category. The region moved to the intermediate-endemicity category during the 1990s (HBV prevalence 4.70%). After the Millennium, the GCC region moved to the low-intermediate endemicity with HBV prevalence of 2.11%. Finally, the region moved to the low-endemicity category after 2010 with the latest HBV infection estimate of 1.56% (Fig. 3).

The trend of hepatitis B virus infection prevalence over time in the Gulf Cooperation Council region (the shaded area represents the 95%CI)
Prevalence by risk group and setting
Among the risk groups, the prevalence was lowest among health-care workers (0.86%), followed by blood-donors (2.33%), pregnant women (2.66%), and finally hemodialysis patients (5.76%) (see Fig. 4a–d). The pooled HBV prevalence from the community-based studies was 4.21% (95% CI 1.39, 8.46).


a Forrest plot of hepatitis B virus prevalence among health-care workers Gulf Cooperation Council. b Forrest plot of hepatitis B virus prevalence among blood donors in the Gulf Cooperation Council. c Forrest plot of hepatitis B virus prevalence among hemodialysis patients in the Gulf Cooperation Council. d Forrest plot of hepatitis B virus prevalence among pregnant women in the Gulf Cooperation Council
Quality assessment and sensitivity analysis
The overall quality of the individual studies and detailed description are shown in Additional file 2: appendices C and E. Almost half of the included studies were of poor quality (n = 49, 49.5%). Most studies used convenient sampling (n = 94), did not address missing data (n = 93), report confidence intervals (n = 95), potential source of bias (n = 82) or estimate the random variability in the data (n = 87).
Since the meta-analysis of the overall population exhibited a considerable heterogeneity, subgroup analysis was done (Table 1). The heterogeneity remained high among all tested subgroups with I2 ranging between 81.2% and 99.7%. When low-quality studies were excluded in the sensitivity analysis, the HBV prevalence was found to be 2.96% (95% CI 2.40, 3.58) using random-effect model (I2 = 99.6%). Hence, the quality of the studies had little effect on the overall estimated HBV prevalence.
Publication bias
Asymmetrical distribution and gaps in the funnel plot indicate the presence of publication bias (Fig. 5), confirmed more objectively with the Egger’s test p-value < 0.001.

Funnel plot of included studies showing asymmetry in the distribution of the dots consistent with publication bias
Discussion
Interest in estimating the prevalence of HBV has been increasing over the last four decades in the GCC. This is shown by the five-fold increase in the number of publications addressing the prevalence of this infection in the region from only 11 studies covering the period of 1980–1990 to 50 studies published in the period 2010–2021. However, there is a clear discrepancy among the individual member countries of the GCC when it comes to the number of papers published in this field. KSA showed early and increasing interest in estimating the burden of HBV infection and this is manifested by the large number of publications (n = 76) spanning the period from 1982 to 2020 and matching the population trend in the GCC (71% of the total population). On the other hand, the other member countries had lower number of publications in this field (4–6 studies per country) and the least populated countries (Bahrain and Qatar) employed larger samples in their studies. However, it is encouraging to observe that these studies were published more recently confirming the recognition of the importance of HBV infection as a global and regional health problem.
In the current study, the overall HBV apparent and true prevalence, as measured by HBsAg, was 3.05% and 1.67% respectively in the GCC region using the data available from the 99 included studies published over the last four decades. However, when only the most recent studies (2010 to 2020) were analyzed separately, the overall HBV apparent prevalence was found to be 1.56%. This figure is much lower than the estimated WHO prevalence and the narrow confidence intervals for the prevalence (95% CI 1.07, 2.12) provides more evidence that the current HBV prevalence estimate is a better one and supports the conclusion that the GCC region is a low-endemicity region for HBV infection. Furthermore, the study showed variations in the prevalence of HBV among the different countries of the GCC. The prevalence was lowest in the UAE (0.80%) while it was highest in Oman (3.73%). The UAE stringent visa medical requirements regarding HBV that include retesting of certain work permit holders may be responsible [116]. However, The overlapping 95% confidence intervals of the prevalence between the GCC countries is suggestive of resemblance.
Even though the expatriates form 49% of the GCC population [117], this subgroup was underrepresented in the included studies (23 studies, 37.5% of total participants). Similarly, children were included in only 5 studies accounting for 2.1% of total participants in the current study. While suspected reluctancy of some expatriates to participate fearing negative implications to their work permit visa may be blamed, difficulty in recruiting children into studies, and/or underestimation of the importance of HBV infection among this group may be the reason. On the contrary, tested female proportion (45.5%) was overrepresented compared to both male and children GCC proportions. A clearer example of using convenient sampling is utilizing blood bank records to estimate HBV prevalence. This method will selectively favour healthy volunteers since older and unhealthy individuals are less likely to donate blood. Furthermore, in the GCC region, males are the predominant blood donors, resulting in overrepresentation of this gender in studies employed blood donors compared to females. All these factors and deficiencies were evident in 50% of the included studies and may resulted in methodologically weak level of evidence.
Children had lower prevalence of HBV (1.93%) compared to adults (3.05%) but the confidence intervals of both overlapped. Although, children constitute 22.1% of the population in the GCC, only 2.1% of the included studies participants (19 studies) were children [118]. Hence, this might be an imprecise estimate of the prevalence of HBV in children, and further larger pediatric studies are required to address this issue. A lower prevalence of HBV is expected as children are less likely to belong to high-risk population (e.g. PWID) or exposed to activities that increase the risk of HBV infection, such as needle stick injuries, compared to adults. However, this difference could be another reflection of the success of early interventions to reduce the risk of HBV infection. The current hepatology guidelines [1] suggest the initiation of anti-viral therapy for mothers with HBV infection during pregnancy and early administration of HBV vaccine (within 24 h of birth) to reduce the risk HBV infection. This practice may have resulted in lower rate of vertical transmission, hence lowering the risk of infection among children.
The results of this review demonstrated a decreasing prevalence over time (Fig. 3) providing evidence of the efficacy of the national strategies including the HBV vaccination programs aiming to mitigate the spread of the virus in the GCC communities and reducing the burden of this infectious disease. In fact, prior to the introduction of the vaccine into the GCC region, HBV had overall prevalence of 9.38%, making it a high-prevalence region. But after incorporating the HBV vaccine into the vaccination programs after 1990, the prevalence have steadily decreased over the following three decades supporting the WHO recommendation for universal HBV vaccination [2]. The most recent estimate is 1.56% placing the GCC in the “low-endemicity” category. This transition will ultimately lead to decrease morbidity and mortality related to HBV, with subsequent reduction in health-care cost. Furthermore, the reduction of HBV prevalence in this region suggests that the GCC countries are in the correct pathway to eradicate HBV by 2030 in keeping with the GHSS target [2].
Strengths, limitations, and risk of biases
This study has several strengths. First, the search strategy included three commonly used databases along with searching references of reviewed studies. The exclusion criteria were kept to a minimum to increase sensitivity of the search and not to miss eligible articles. This ultimately led to the inclusion of 99 studies translating into over 1.9 million participants. This large number of included participants lead to improved HBV prevalence estimation, decreased the possibility of chance finding and narrowed the confidence intervals obtained for the main outcome. In addition, this thorough search led to the inclusion of studies that covered all member countries of the GCC region, different populations and time frames, increasing the generalizability of the findings. Another strength of the study was the use of quality assessment tool for the assessment of the quality of included studies and risk of bias. This assessment allowed the recognition of methodologically weak studies and performing sensitivity analysis excluding these studies, further confirming the observed prevalence. The use of a validated and reliable blood test to detect HBsAg and ascertain the outcome (HBV infection) as part of the inclusion criteria helped to reduce the risk of information bias. This is important since using non-accurate methods for detection of HBV infection (e.g. physical examination only or non-validated tests) may have resulted in biased results. Also, we used the random-effect model to account for heterogeneity. This is the first study to consider the unique demographic characteristics of the GCC countries population and the work permit health requirement in interpreting the results and calculate true prevalence.
However, this study has some limitations. The major limitation is related to the quality of the included studies. The overall quality assessment showed that half of the included studies were of poor quality, mainly related to the sampling technique used, adjustment for confounders and accounting for missing participants. Only 5 studies [32, 33, 55, 67, 71] utilized community-sampling which normally would provide better estimate of the general population prevalence of HBV. The included studies had evidence of significant heterogeneity as measured by I2 test and Cochran’s Q test. The source of the heterogeneity could be related to using different population groups (e.g. blood donors, hemodialysis, pregnant women). This issue of high heterogeneity is well-described for descriptive studies since they rely mostly on retrospective observational studies where controlling for different sources of bias might be more difficult compared to a controlled interventional study [119]. In addition, another source of heterogeneity is the inclusion of different time frames to estimate the pooled HBV prevalence. Methodologically, only one author screened and selected the available literature applying inclusion and exclusion criteria. While this is not in line with the best practices required for a systematic review, it was because of the nature and the specific requirements of an individual work within an academic path, and it was mitigated by an independent supervision by the second author in view of the peer review process.
The funnel plot test result and the low p-value of the Egger’s test could represent a true evidence of publication bias where studies that reported higher prevalence of HBV infection were more likely to be published. In addition, there were 12 potentially eligible studies that were unretrievable (Additional file 2: Appendix A2). In theory this could have introduced selection bias. However, this is less likely to have a significant impact on the overall estimate of this review given the large number of included studies (n = 99). Furthermore, most of the missing articles were published in the pre-2000 period, having even less impact on the estimate of the current HBV prevalence.
Conclusions and recommendations
The overall apparent prevalence of HBV infection in the GCC is 3.05% (95% CI 2.60%, 3.52) and the true prevalence is 1.67% (95% CI 1.66%, 1.68). Over the last four decades the overall apparent prevalence of HBV infection in the GCC region decreased from 9.38% (95% CI 7.26, 11.74) before 1990 to 1.56% (95% CI 1.07, 2.12) during the period 2010 to 2020. Therefore, the GCC region has successfully moved from high-endemicity region to low-endemicity region. However, due to poor methodology of the included studies, further high-quality, community-based studies are needed with focus on the prevalence in the general population.
Availability of data and materials
All data and statistical codes used to generate the results will be available on request to the corresponding author.
References
European Association for the Study of the Liver (EASL). Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;2017(67):370–98.
World Health Organization. Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. https://www.who.int/publications/i/item/9789240027077
Steinke DT, Weston TL, Morris AD, et al. Epidemiology and economic burden of viral hepatitis: an observational population based study. Gut. 2002;50:100–5.
Park H, Jeong D, Nguyen P, et al. Economic and clinical burden of viral hepatitis in California: a population-based study with longitudinal analysis. PLoS ONE. 2018;13: e0196452.
Meireles LC, Marinho RT, Van Damme P. Three decades of hepatitis B control with vaccination. World J Hepatol. 2015;7:2127–32.
Van Damme P. Long-term protection after hepatitis B vaccine. J Infect Dis. 2016;214:1–3.
Britannica, T Editors of Encyclopaedia (2021). Gulf Cooperation Council. Encyclopedia Britannica. http://www.britannica.com/topic/Gulf-Cooperation-Council
United Nations Development Programme (UNDP). Human Development Report 2020
AlFaleh F, AlShehri S, AlAnsari S, et al. Long-term protection of hepatitis B vaccine 18 years after vaccination. J Infect. 2008;57:404–9.
World Health Organization (WHO) 2020. Health and well-being profile of the Eastern Mediterranean Region. An overview of the health situation in the Region and its countries in 2019. https://applications.emro.who.int/docs/9789290223399-eng.pdf?ua=1&ua=1
Al-Faleh FZ, Hepatitis B. Infection in Saudi Arabia. Ann Saudi Med. 1988;8:474–80.
Higgns JP, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions. Chichester (UK): John Wiley & Sons; 2019.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6: e1000097.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377–84.
Fadlalla FA, Mohamoud YA, Mumtaz GR, et al. The epidemiology of hepatitis C virus in the Maghreb region: systematic review and meta-analyses. PLoS ONE. 2015;10: e0121873.
DerSimonian R, Kacker R. Random-effects model for meta-analysis of clinical trials: an update. Contemp Clin Trials. 2007;28:105–14.
Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Rogan WJ, Gladen B. Estimating prevalence from the results of a screening test. Am J Epidemiol. 1978;107:71–6.
Amini A, Varsaneux O, Kelly H, et al. Diagnostic accuracy of tests to detect hepatitis B surface antigen: a systematic review of the literature and meta-analysis. BMC Infect Dis. 2017;17:698.
Inan N, Demirel A, Kabakoglu E, et al. Comparison of chemiluminescence microparticle immunoassay and electrochemiluminescence immunoassay for detection of HBsAg. Viral Hepatitis J. 2014;20(3):101–5.
Abdel-Ghaffar MH, Al-Harbi SA, Nivas RK, et al. Seroprevalence of hepatitis B and C viruses among population of Al-Quwayiyah Governorate, Saudi Arabia. Int J Curr Microbiol App Sci. 2015;4:666–73.
Abdullah SM. Prevalence of hepatitis B and C in donated blood from the Jazan region of Saudi Arabia. MJMS Malays J Med Sci. 2013;20:41–6.
Abdullah SM. Prevalence of hepatitis B and C virus infection and their co-relation with hematological and hepatic parameters in subjects undergoing premarital screening in the Jazan Region, Kingdom of Saudi Arabia. Pak J Med Sci. 2018;34:316–21.
Ageely H, Ayoola EA, Al-Hazmi M, et al. Spontaneous bacterial peritonitis in Saudi Arabian patients with non-alcoholic liver cirrhosis. Hepatogastroenterology. 2000;47:1649–53.
Ahmed MEK, Omer HA, Jubran I, et al. The decline of HCV and HBV infection prevalence among haemodialysis patients in Southern Saudi Arabia: a success story. Biomed Res. 2018;29:3688–91.
Alabdulmonem W, Shariq A, Alqossayir F, et al. Sero-prevalence ABO and Rh blood groups and their associated transfusion-transmissible infections among blood donors in the Central Region of Saudi Arabia. J Infect Public Health. 2020;13:299–305.
Al-Admawy AMO, Talukder MAS, Gilmore RF. Prevalence and acquisition rates of hepatitis BsAg in Riyadh Alkharj Hospital Programme. Saudi Med J. 1987;8:142–6.
Alaidarous M, Choudhary RK, Waly MI, et al. The prevalence of transfusion-transmitted infections and nucleic acid testing among blood donors in Majmaah, Saudi Arabia. J Infect Public Health. 2018;11:702–6.
Al-Ajlan A. Prevalence of hepatitis B and C among students of health colleges in Saudi Arabia. East Mediterr Health J. 2011;17:759–62.
Albadran A, Hibshi A, Saeed B, et al. Hepatitis B and C virus prevalence in couples attending an in vitro fertilization clinic in a tertiary care hospital in Saudi Arabia: comparison with ten years earlier. Ann Saudi Med. 2017;37:272–5.
Al-Bahrani A, Panhotra BR. Prevalence of HBsAG and ANTI-HCV antibodies in blood donors of the Al-Hasa Region of Saudi Arabia. Ann Saudi Med. 2001;21:234–5.
Al-Faleh FZ, Ayoola EA, Arif M. Seroepidemiology of hepatitis B virus infection in Saudi Arabian children: a baseline survey for mass vaccination against hepatitis B. J Infect. 1992;24:197–206.
Al-Faleh FZ, Al-Jeffri M, Ramia S, et al. Seroepidemiology of hepatitis B virus infection in Saudi children 8 years after a mass hepatitis B vaccination programme. J Infect. 1999;38:167–70.
Al-Fawaz I, Ramia S. Decline in hepatitis B infection in sickle cell anaemia and beta thalassaemia major. Arch Dis Child. 1993;69:594–6.
Al-Freihi HM. Prevalence of hepatitis B surface antigenemia among patients with Schistosoma mansoni. Ann Saudi Med. 1993;13:121–5.
Al-Ghamdi AA, Safi MAA. Prevalence of hepatitis B surface antigen and its association with anti-hepatitis C virus antibodies among pilgrims. J King Abdulaziz Univ Med Sci. 2015;22:1–7.
Al-Ghonaim MI, Abdel-Ghaffar MH, Alnomasy SF, et al. Prevalence of viral hepatitis among population of Al-Quwayiyah Governorate, Saudi Arabia. World J Pharm Res. 2012;1:1212–22.
Al Humayed SM. Seroprevalence of HBsAg among adolescents and adults in the Muhayil Aseer region of KSA: 25 years after the introduction of national vaccination. J Taibah Univ Med Sci. 2016;11:140–4.
Al Humayed SM, El-Mekki AA, Mahfouz AA. Hepatitis B virus infection in Aseer Region, south-western Saudi Arabia: a call for an immediate action against a preventable disease. Public Health. 2017;146:24–8.
Al-Humayed SM. Hepatitis B and C viral infections in Tihamet Aseer, South-Western Saudi Arabia: are there gender differences? Saudi J Med Med Sci. 2017;5:110–5.
Alhuraiji A, Alaraj A, Alghamdi S, et al. Viral hepatitis B and C in HIV-infected patients in Saudi Arabia. Ann Saudi Med. 2014;34:207–10.
Aljarbou AN. Current prevalence of HBV and HCV seropositivity: the initiative for attentiveness and deterrence of viral hepatitis in the Qassim region of Saudi Arabia. J Antivirals Antiretrovirals. 2012;4:75–9.
Al-Mandeel HM, Manahel A, Fatimah A, et al. Seroprevalence of hepatitis B and C, and human immunodeficiency viruses in Saudi pregnant women and rates of vertical transmission. Kuwait Med J. 2015;47:221–4.
Al-Mazrou YY, Al-Jeffri M, Khalil MKM, et al. Screening of pregnant Saudi women for hepatitis B surface antigen. Ann Saudi Med. 2004;24:265–9.
Al-Mutairi HH, Al-Ahmari MM, Al-Zahran BH, et al. Prevalence of serological markers and nucleic acid for blood-borne viral infections in blood donors in Al-Baha, Saudi Arabia. J Infect Dev Ctries. 2016;10:619–25.
Omar ASA, Zuebi FE. Disease markers in blood donors at King Fahad Hospital. Al Baha Ann Saudi Med. 1996;16:37–41.
Alqahtani JM, Abu-Eshy SA, Mahfouz AA, et al. Seroprevalence of hepatitis B and C virus infections among health students and health care workers in the Najran region, southwestern Saudi Arabia: the need for national guidelines for health students. BMC Public Health. 2014;14:577.
Alqahtani SM, Alsagaby S, Mir SA, et al. Seroprevalence of viral hepatitis B and C among blood donors in the Northern Region of Riyadh Province, Saudi Arabia. Healthcare. 2021;9:934.
Al-Raddadi RM, Dashash NA, Alghamdi HA, et al. Prevalence and predictors of hepatitis B in Jeddah city, Saudi Arabia: a population-based seroprevalence study. J Infect Dev Ctries. 2016;10:1116–23.
Alrowaily MA, Abolfotouh MA, Ferwanah MS. Hepatitis B virus sero-prevalence among pregnant females in Saudi Arabia. Saudi J Gastroenterol. 2008;14:70–2.
AlShamlan NA, Al Shammari MA. Hepatitis B-C and human immunodeficiency virus: seroprevalence and associated factors among health students in Saudi Arabia. Hosp Pract. 2021;49(3):221–8.
Alshayea AI, Eid GE, El-Hazmi MM, et al. Prevalence and characterization of occult hepatitis B infection among blood donors in central Saudi Arabia. Saudi Med J. 2016;37:1114–9.
Al-Sohaibani MO, Al-Sheikh EH, Al-Ballal SJ, et al. Occupational risk of hepatitis B and C infections in Saudi medical staff. J Hosp Infect. 1995;31:143–7.
Alshomrani AT. Prevalence of human immunodeficiency virus, hepatitis C virus, and hepatitis B virus infection among heroin injectors in the central region of Saudi Arabia. Saudi Med J. 2015;36:802–6.
Alswaidi FM, O’Brien SJ. Is there a need to include HIV, HBV and HCV viruses in the Saudi premarital screening program on the basis of their prevalence and transmission risk factors? J Epidemiol Community Health. 2010;64:989–97.
Altamimi W, Altraif I, Elsheikh M, et al. Prevalence of HBsAg and anti-HCV in Saudi blood donors. Ann Saudi Med. 1998;18:60–2.
Al-Thaqafy MS, Balkhy HH, Memish Z, et al. Hepatitis B virus among Saudi National Guard Personnel: seroprevalence and risk of exposure. J Infect Public Health. 2013;6:237–45.
Al-Wayli HM. Prevalence of hepatitis B surface antigen in a Saudi hospital population. Saudi Med J. 2009;30:448–9.
Alzahrani FM, Shaikh SS, et al. Prevalence of Hepatitis B Virus (HBV) among blood donors in Eastern Saudi Arabia: results from a five-year retrospective study of HBV seromarkers. Ann Lab Med. 2019;39:81–5.
Ankra-Badu GA, Ahmad M, Sowayan S, et al. Demographic characteristics of seropositive donors in Al-Khobar. Ann Saudi Med. 2001;21:113–6.
Arif M, Al-Momen AK, Huraib S, et al. Baseline seroepidemiology of hepatitis B virus infection in two Saudi high-risk groups: patients on haemodialysis and patients with congenital bleeding disorders. Trans Royal Soc Trop Med Hyg. 1989;83:256–7.
Ayoola AE, Tobaigy MS, Gadour MO, et al. The decline of hepatitis B viral infection in South-Western Saudi Arabia. Saudi Med J. 2003;24:991–5.
Bajhmoum W. Clinical and Laboratory Features of HIV/AIDS in the Kingdom of Saudi Arabia. Liverpool School of Tropical Medicine. Volume PhD: University of Liverpool, 2014. https://livrepository.liverpool.ac.uk/2014239/
Bakir TMF, Kurbaan KM, Al Fawaz I, et al. Infection with hepatitis viruses (B and C) and human retroviruses (HTLV-1 and HIV) in Saudi children receiving cycled cancer chemotherapy. J Trop Pediatr. 1995;41:206–9.
Bani I, Mahfouz MS, Maki E, et al. Prevalence and risk factors of hepatitis B virus among pregnant women in Jazan region-Kingdom of Saudi Arabia. J Biol Agric Healthc. 2012;2:45–8.
Bashawri LA, Fawaz NA, Ahmad MS, et al. Prevalence of seromarkers of HBV and HCV among blood donors in eastern Saudi Arabia, 1998–2001. Clin Lab Haematol. 2004;26:225–8.
Eifan SA, Qamar S, Hanif A, et al. Seroprevalence of Hepatitis B, Hepatitis C and Human Immunodeficiency Virus in Al-khraj region. Biomed Res. 2015;26:147–51.
Eisa ZM, Eifan SA, Al-Sum BA. Prevalence of HBV, HCV, and HIV infections among individuals included in premarital screening program at Jazan Province, Saudi Arabia. Indian J Public Health Res Dev. 2012;3(4):23–6.
El Beltagy KE, Al Balawi IA, Almuneef M, et al. Prevalence of hepatitis B virus markers among blood donors in a tertiary hospital in Tabuk, northwestern Saudi Arabia. Int J Infect Dis. 2008;12:495–9.
Elbjeirami W, Al-Jedani H, Arsheed N, et al. Prevalence and trends of HBV, HCV, and HIV serological and NAT markers and profiles in Saudi blood donors. J Blood Disord Transfus. 2015;6:280.
El-Hazmi MAF, Hepatitis B. Markers in Saudi Arabia: a comparative study in different regions. Ann Saudi Med. 1986;6:185–90.
El-Hazmi MM. Prevalence of HBV, HCV, HIV-1, 2 and HTLV-I/II infections among blood donors in a teaching hospital in the central region of Saudi Arabia. Saudi Med J. 2004;25:26–33.
Ikram MH, Ali SI, Khawaja FI, et al. Hepatitis B virus markers among the blood donors in Medina Munawara. Ann Saudi Med. 1988;8:470–3.
Kashgari RH, Mohamad AA. Seroepidemiology of hepatitis B virus (HBV) and hepatitis C virus (HCV) and relationship to alanine transferase (alt) in saudi workers at yanbu industrial city. J Fam Community Med. 1997;4:24–9.
Khalil MKM, Al-Mazrou YY, Al-Jeffri M, et al. Serosurvey of hepatitis B surface antigen in pregnant Saudi women. East Mediterr Health J. 2005;11:640–7.
Khan LA, Khan SA. Prevalence of hepatitis B and C markers in patients on maintenance hemodialysis in Najran. Saudi Med J. 2001;22:641–2.
Mahaba HM, El-Tayeb Ael K, El-Sekibi DK, et al. Pattern of HBsAg positivity in selected groups At King Khalid General Hospital-Hail Region, Kingdom of Saudi Arabia. J Fam Community Med. 1997;4:30–6.
Mahmoud MIH, Habib F. Review of the status of the HBsAg among the pregnant women attended primary health care centers (PHCCs) in Medina, Saudi Arabia between 2008 and 2010. J Am Sci. 2012;8:519–23.
Mansoor AA, Salih AI, Al-Jaroudi DH. Screening of hepatitis B and C and human immunodeficiency virus in infertile couples in Saudi Arabia. Saudi Med J. 2011;32:260–4.
Mehdi SR, Avinash P, Al-Abdul Rahim KA. Prevalence of hepatitis B and C among blood donors. Saudi Med J. 2000;21:942–4.
Mehdi SR, Al Ajlan AR. Hepatitis B&C virus infection in cases of Non-Hodgkin’s lymphoma in Saudi Arabia. Turk J Hematol. 2006;23:200–4.
Njoh J. The prevalence of hepatitis B surface antigen (HBsAg) among drug-dependent patients in Jeddah. Saudi Arabia East Afr Med J. 1995;72:198–9.
Panhotra BR, Al-Bahrani A, Ul-Hassan Z. Epidemiology of antibody to hepatitis B core antigen screening among blood donors in Eastern Saudi Arabia need to replace the test by HBV DNA testing. Saudi Med J. 2005;26:270–3.
Parande CM, Arya SC, Ashraf SJ. Hepatitis B virus among Saudi children in Gizan. Saudi Arabia Infect. 1986;14:223–5.
Ramia S, Abdul-Jabbar F, Bakir TM, et al. Vertical transmission of hepatitis B surface antigen in Saudi Arabia. Ann Trop Paediatr. 1984;4:213–6.
Sadik AS, Alzailayee AA, Foda MB. Serological and molecular detection of hepatitis B viral antibodies and its surface antigen in blood samples of different age stages at Taif Governorate, KSA. Int J Curr Microbiol App Sci. 2014;3:758–73.
Yaega S, Aegaehes S, Aals M. Seropositivity of TTIs among blood donors in Hail, Saudi Arabia, from 2014 to 2015. Asian Pac J Trop Dis. 2016;6:141–6.
Shabanah W, Bukhari A, Alandijani A, et al. Prevalence of HBV and assessment of Hepatitis B vaccine response among dental health care workers in dental teaching hospital, Umm Al-Qura University, Saudi Arabia. Egypt J Immunol. 2019;26:11–7.
Shatoor AS, Zafer MH. Hepatitis B virus markers in male blood donors. Bahrain Med Bull. 2002;24:138–40.
Sheth KV, Godwin JT. Hepatitis B virus markers in male saudi blood donors. Ann Saudi Med. 1986;6:3–7.
Zaini RG, Dahlawi H. The prevalence of infectious diseases among blood donors in King Abdul-Aziz General Hospital. Makkah Revista Kasmera. 2017;45:97–106.
Al-Mutairi BSN. Hepatitis B and hepatitis C virus prevalence among sexually transmitted disease patients in farwania region of Kuwait. Sexually Transmitted Infections. Conference: STI and AIDS World Congress 2013;89.
Al-Nakib B, Al-Nakib W, Bayoumi A, et al. Hepatitis B virus (HBV) markers among patients with chronic liver disease in Kuwait. Trans R Soc Trop Med Hyg. 1982;76:348–50.
Altawalah H, Al-Houli M, Madi N, et al. Prevalence of blood borne viruses in the dialysis unit, mubarak Al-Kabeer hospital, Kuwait. Kuwait Med J. 2015;47:30–2.
Altawalah H, Essa S, Ezzikouri S, et al. Hepatitis B virus, hepatitis C virus and human immunodeficiency virus infections among people who inject drugs in Kuwait: a cross-sectional study. Sci Rep. 2019;9:6292.
Ameen R, Sanad N, Al-Shemmari S, et al. Prevalence of viral markers among first-time Arab blood donors in Kuwait. Transfusion. 2005;45:1973–80.
Al-Amad SH. Prevalence of hepatitis B, C, and HIV among patients attending a teaching dental hospital: a 7-year retrospective study from the United Arab Emirates. Saudi Med J. 2018;39:500–5.
Al-Owais A, Al-Suwaidi K, Amiri N, et al. Use of existing data for public health planning: a study of the prevalence of hepatitis B surface antigen and core antibody in Al Ain Medical District, United Arab Emirates. Bull World Health Organ. 2000;78:1324–9.
Al Shaer L, Abdulrahman M, John TJ, et al. Trends in prevalence, incidence, and residual risk of major transfusion-transmissible viral infections in United Arab Emirates blood donors: impact of individual-donation nucleic acid testing, 2004 through 2009. Transfusion. 2012;52:2300–9.
Fakhry SM, Al-Dawilah TA, Mehta SH. Prevalence of Hepatitis B virus (HBV) and Hepatitis C virus (HCV) in young adults in United Arab Emirates (UAE). Hepatology. 2011;54:607A.
Trad O, Hayek M, Jumaa P, et al. Seroprevalence of hepatitis B, hepatitis C and HIV among multiply transfused thalassemic children treated at Tawam Hospital. Emir Med J. 2003;21:17–20.
Al-Awaidy ST, Bawikar SP, Al-Busaidy SS, et al. Progress toward elimination of hepatitis B virus transmission in Oman: impact of hepatitis B vaccination. Am J Trop Med Hyg. 2013;89:811–5.
Al-Dhahry SHS, Aghanashinikar PN, Al-Marhuby HA, et al. Hepatitis B, delta and human immunodeficiency virus infections among Omani patients with renal diseases: a seroprevalence study. Ann Saudi Med. 1994;14:312–5.
Alkindi S, Al-Umairi N, Jaju S, Pathare A. Prevalence of Hepatitis B, Hepatitis C, and HIV in multiply transfused sickle cell disease patients from Oman. Mediterr J Hematol Infect Dis. 2019;11(1): e2019058.
Kaminski G, Alnaqdy A, Al-Belushi I, et al. Evidence of occult hepatitis B virus infection among Omani blood donors: a preliminary study. Med Princ Pract. 2006;15:368–72.
Soliman AT, Bassiouny MR, Elbanna NA. Study of hepatic functions and prevalence of hepatitis-B surface antigenaemia in Omani children with sickle cell disease. J Trop Pediatr. 1995;41:174–6.
Aabdien M, Selim N, Himatt S, et al. Prevalence and trends of transfusion transmissible infections among blood donors in the State of Qatar, 2013–2017. BMC Infect Dis. 2020;20(1):617.
Al Mannai H, Riad H. Seroprevalence of hepatitis B and C viruses in lichen planus patients in Qatar. J Am Acad Dermatol. 2010;62:AB128.
Hamilton BH, Paoloni JA, Chalabi H. Epidemiology of hepatitis B among professional male athletes in Qatar. Saudi Med J. 2010;31:678–83.
Rikabi A, Bener A, Al-Marri A, et al. Hepatitis B and C viral infections in chronic liver disease: a population based study in Qatar. East Mediterr Health J. 2009;15:778–84.
Al-Mahroos FT, Ebrahim A. Prevalence of hepatitis B, hepatitis C and human immune deficiency virus markers among patients with hereditary haemolytic anaemias. Ann Trop Paediatr. 1995;15:121–8.
Janahi EM. Prevalence and risk factors of hepatitis B virus infection in Bahrain, 2000 through 2010. PLoS ONE. 2014;9(2): e87599.
Yousif A, Wallace M, Baig B. The seroprevalence of syphilis, toxoplasmosis and hepatitis B in patients in Bahrain infected with human immunodeficiency virus. Trans R Soc Trop Med Hyg. 1994;88:60.
Almawi WY, Qadi AA, Tamim H, et al. Seroprevalence of hepatitis C virus and hepatitis B virus among dialysis patients in Bahrain and Saudi Arabia. Transpl Proc. 2004;36:1824–6.
Al-Awaidy S, Abu-Elyazeed R, Al-Hosani H, et al. Sero-epidemiology of hepatitis B infection in pregnant women in Oman, Qatar and the United Arab Emirates. J Infect. 2006;52:202–6.
Government of United Arab Emirates. Health Conditions for UAE residence 2021. https://u.ae/en/information-and-services/health-and-fitness/health-conditions-for-uae-residence-visa
World Health Organization (WHO). World Health Organization Regional Office for the Eastern Mediterranean: WHO, 2021. https://www.emro.who.int/entity/statistics/statistics.html
The Statistical Centre for the Cooperation Council for the Arab Countries of the Gulf (GCC-STAT). GCC population 2020 Report. https://gccstat.org/images/gccstat/docman/publications/population2020_2_1.pdf
Kim KW, Lee J, Choi SH, et al. Systematic review and meta-analysis of studies evaluating diagnostic test accuracy: a practical review for clinical researchers-Part I. General guidance and tips. Korean J Radiol. 2015;16:1175–87.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
AAA conceptualized the study, formulated the research questions, contributed to the definition of the search strategy, performed the first screening of titles and full texts reviews, read the full texts of the selected articles to assess eligibility for inclusion, data extraction and statistical analysis, assessed the risk of bias for the included studies, analyzed the results, drafted all sections of the manuscript and prepared Tables and Figures under MNAS supervision. MNAS conceptualized the study, contributed to the formulation of the research questions, revised the search strategy, the screening of titles and full texts, the data extraction from the selected articles, the assessment of risk of bias for the included studies, the analysis of results, and commented and edited all sections of the manuscript. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA checklist.
Additional file 2
. Appendix.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alali, A.A., Abo-Shehada, M.N. Prevalence of Hepatitis B Virus infection in the Gulf Cooperation Council: a systematic review and meta-analysis. BMC Infect Dis 22, 819 (2022). https://doi.org/10.1186/s12879-022-07806-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-022-07806-4