
Abstract
Background
A two-stage surgical strategy (debridement-negative pressure therapy (NPT) and flap coverage) with prolonged antimicrobial therapy is usually proposed in pressure ulcer-related pelvic osteomyelitis but has not been widely evaluated.
Methods
Adult patients with pressure ulcer-related pelvic osteomyelitis treated by a two-stage surgical strategy were included in a retrospective cohort study. Determinants of superinfection (i.e., additional microbiological findings at reconstruction) and treatment failure were assessed using binary logistic regression and Kaplan-Meier curve analysis.
Results
Sixty-four pressure ulcer-related pelvic osteomyelitis in 61 patients (age, 47 (IQR, 36–63)) were included. Osteomyelitis was mostly polymicrobial (73%), with a predominance of S. aureus (47%), Enterobacteriaceae spp. (44%) and anaerobes (44%). Flap coverage was performed after 7 (IQR, 5–10) weeks of NPT, with 43 (68%) positive bone samples among which 39 (91%) were superinfections, associated with a high ASA score (OR, 5.8; p = 0.022). An increased prevalence of coagulase negative staphylococci (p = 0.017) and Candida spp. (p = 0.003) was observed at time of flap coverage. An ESBL Enterobacteriaceae spp. was found in 5 (12%) patients, associated with fluoroquinolone consumption (OR, 32.4; p = 0.005). Treatment duration was as 20 (IQR, 14–27) weeks, including 11 (IQR, 8–15) after reconstruction. After a follow-up of 54 (IQR, 27–102) weeks, 15 (23%) failures were observed, associated with previous pressure ulcer (OR, 5.7; p = 0.025) and Actinomyces spp. infection (OR, 9.5; p = 0.027).
Conclusions
Pressure ulcer-related pelvic osteomyelitis is a difficult-to-treat clinical condition, generating an important consumption of broad-spectrum antibiotics. The lack of correlation between outcome and the debridement-to-reconstruction interval argue for a short sequence to limit the total duration of treatment.
Similar content being viewed by others


Background
Pressure ulcers are frequent and severe clinical conditions corresponding to localized areas of damaged skin and/or underlying tissues over a bony prominence. As resulting of pressure in combination with shear associated with immobility, these lesions mostly occur in para- or tetraplagic patients after spinal cord injury, or in geriatric or intensive care settings [1, 2]. Stage 4 lesions of the revised national pressure ulcer advisory panel (NPUAP) pressure injury staging system are associated with deep-seated infections, including contiguous osteomyelitis that has been reported in 17 to 32% of patients [3,4,5]. Local care and/or antimicrobial therapy alone are insufficient to manage these complex infections [6, 7]. Consequently, up to 27% of patients with primary diagnosis of pressure ulcer require a multidisciplinary approach with surgical flap reconstruction and prolonged antimicrobial therapy, leading to massive societal costs approaching 125,000 USD per episode [8,9,10].
In the absence of formal guidelines, medical and surgical practices are highly heterogeneous, as well as outcomes with failure rates ranging from 5 to 65% [8, 11,12,13,14]. Even if immediate reconstruction is proposed by some surgical teams [15], one of the most commonly accepted options for the treatment of sacral or ischial pressure ulcer-related chronic osteomyelitis is a two-stage surgical strategy. The first surgical step consists in debridement of devitalized tissue and allows the realization of multiple bone biopsies aiming for microbiological documentation [2, 16, 17], and is followed by negative pressure therapy (NPT) [18]. A reconstructive surgery is performed after control of the soft tissue infection, commonly using a regional myo- or fascio-cutaneous flap [19]. Antimicrobial therapy is started after the initial surgical debridement, adapted to bacteriological documentation, and prolonged for several weeks after flap coverage. In this context, the present study aimed to relate the experience of a French regional reference center for the management of complex bone and joint infection (CRIOAc Lyon) in such poorly evaluated two-stage surgical strategy, focusing on bacteriological findings and risk factor for treatment failure.
Methods
Inclusion criteria and data collection
This retrospective observational monocentric study included all adult patients with ulcer pressure-related sacral or ischial chronic osteomyelitis managed by a two-stage surgical strategy (i.e, debridement followed by NPT before myo- or fascio-cutaneous flap reconstruction) associated with prolonged antimicrobial therapy from January 1st 2012 to April 30th 2016. Patient identification was based on the prospective and exhaustive database of our regional reference center for the management of complex bone and joint infection. For each patient, extensive data were extracted from medical records, nursing charts and biological software, and recorded in a standardized anonymous case report form. Collected data included patients and osteomyelitis baseline characteristics, past medical history allowing the calculation of the modified comorbidity Charlson index as previously described [20], the precise surgical and medical therapeutic sequences, results of microbiological analysis at each surgical step, and outcome.
Definitions
In the absence formal consensus, the diagnosis of osteomyelitis was based on clinical, radiological and microbiological findings [21]. Histological analysis was not routinely performed and consequently not included in the diagnosis criteria. Reported microbiological findings relied only on gold-standard sample management, consisting in prolonged (14 days) cultures of surgical bone biopsies performed after ulcer debridement. Results of superficial and/or soft tissue samples were excluded. To be considered as implicated in bone infection, potentially contaminant bacteria such as coagulase negative staphylococci (CoNS), Corynebacteria spp., or Propionibacterium spp. had to be yielded on at least two samples, as suggested by the US guidelines for the diagnosis of prosthetic joint infection [22], and taken into account by the treating clinician in the definitive antibiotic regimen. Superinfection referred to additional microbiological findings at time of flap reconstruction in comparison with debridement. Therapeutic failure included: i) the need for additional surgical procedure for septic reason after flap reconstruction; ii) relapse at the same site after discontinuing antimicrobial therapy; and/or iii) infection-related death.
Statistical analysis
Descriptive statistics were used to estimate the frequencies of the study variables, described as percentages (%) for dichotomous variables and as medians (interquartile range (IQR)) for continuous values. For each variable, the number of missing values was excluded from the denominator in percentage calculation. Non-parametric statistical methods were used to compare groups (Fisher exact test and Mann-Whitney U test), as appropriate. Kaplan-Meier curves allowed the comparison of failure-free survival between groups using the log-rank test. Determinants of superinfections and treatment failure were assessed using binary logistic regression, and expressed as odd ratio (OR) with 95% confidence interval (95%CI). Clinically pertinent variables with a p-value < 0.15 in the univariate analysis were included in the final multivariate models. A p-value < 0.05 was considered as significant. All analyses were performed using SPSS software version 19.0 (SPSS, Chicago, IL).
Results
Included population
Sixty-four pressure ulcer-related ischial (n = 43; 67.2%) or sacral (n = 20; 31.3%) osteomyelitis occurring in 61 patients (46 males, 71.9%; median age, 47.4 [IQR, 35.6–62.6]) were included. Contexts leading to pressure ulcer were mostly paraplegia (n = 41; 64.1%) and tetraplegia (n = 12; 18.8%). Patients had few comorbidities, including 9 (14.0%) with diabetes mellitus and 4 (6.3%) with heart failure or chronic liver disease, leading to a median modified Charlson’s comorbidity index of 3 (IQR, 2–5). Twenty-five (39.1%) were active smokers. A previous pressure ulcer at the same site was noted in 24 (37.5%) patients. A consumption of third generation cephalosporin, piperacilline-tazobactam, carbapenam and/or fluoroquinolone was reported in 8 (12.5%), 11 (17.2%), 11 (17.2%) and 8 (12.5%) cases, respectively. All patients’ characteristics are presented in Table 1.
Debridement
Lesions evolved from a median of 37.9 (IQR, 14.0–109.6) weeks before debridement. Fifty-seven (89.1%) cases required only one surgical debridement before reconstruction, while 7 (10.9%) had at least two debridements.
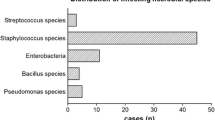
The majority of infections were polymicrobial (n = 47; 73.4%). Staphylococci were the most prevalent pathogens, isolated in 37 (57.8%) cases, and including: i) S. aureus (n = 30; 46.9%), among which 4 (13.3%) were methicillin-resistant (MRSA); and ii) CoNS (n = 9; 14.1%) among which 4 (44.4%) were methicillin-resistant (MRCoNS). Other bacterial species included 28 (43.8%) Enterobacteriaceae spp. among which 4 (14.8%) secreted extended spectrum betalactamase (ESBL), anaerobes (n = 28, 43.8%, including 7 Actinomyces spp. [10.9%]), and streptococci (n = 24; 37.5%). All microbiological results are detailed in Fig. 1.

Comparison of microbiological findings among bone biopsies performed at debridement and flap reconstruction
Empiric antimicrobial combinations mostly comprised vancomycin (n = 44; 69.8%), associated with piperacillin-tazobactam (n = 36; 57.1%) or carbapenem (n = 11; 22.2). Retrospectively, 82.5% were effective against the pathogens isolated from debridement bone biopsies. Antibiotic therapy was adapted to microbiological results before the flap closure in 49 (77.8%) patients (Table 2).
Flap reconstruction
The flap reconstruction was performed 6.6 (IQR, 4.9–9.6) weeks after debridement. Spectrum of antibiotic therapy was empirically re-expanded after the reconstruction step in 15 (23.1%) patients (Table 2).
Bacterial cultures of bone biopsies were positive in 43 (68.3%) cases. Fourteen (21.9%) patients had at least one bacteria already present in initial debridement bone samples. These persisting infections were due to Enterobacteriaceae spp. (n = 4), CoNS (n = 3), Corynebacteria spp. (n = 3), MSSA (n = 2), P. aeruginosa (n = 2), E. faecalis (n = 1), Finegoldia spp. (n = 1) and C. tropicalis (n = 1). However, patients with positive bone samples at time of flap reconstruction mostly had a superinfection (n = 39; 90.7%). Characteristics of patients with superinfection and univariate analysis for its determinants are provided in Table 1. In multivariate analysis, the only independent risk factor of superinfection was the ASA score (OR, 5.758; 95%CI, 1.284–25.833; p = 0.022). Post-debridement appropriate empiric antibiotic therapy was protective (OR, 0.069; 95%CI, 0.006–0.787; p = 0.031).
Compared to the initial bacteriological findings (Fig. 1), staphylococci were globally less represented (23.4%; p = 0.030), with a decrease in S. aureus prevalence (9.3%; p < 10− 3). Contrariwise, CoNS were increasingly found in 12 (27.9%) cases (p = 0.017) among which 83.3% were methicillin-resistant, without identified risk factor for MRCoSN superfinfection. A significant reduction in the proportion of streptococci (2.3%; p < 10− 3) and anaerobes (9.3% without any Actinomyces spp.; p < 10− 3) was observed. An ESBL-producing Enterobacteriaceae spp. was found in 11.6% of cases compared to 6.3% at the time of trimming (p = 0.480), such a superinfection being statistically associated with the use of fluoroquinolones in the previous 6 months (OR, 32.4; 95%CI, 2.820–372.319; p = 0.005). Pseudomonas aeruginosa superinfection (n = 7; 17.9%) was associated with a high modified Charlson’s comorbidity index (OR, 1.269; 95%CI, 0.997–1.614; p = 0.053) and multiple debridements (OR, 7.067; 95%CI, 0.946–52.766; p = 0.057). An increase in the prevalence of Candida albicans was finally observed (25.6% vs. 4.7%; p = 0.003), without identified predictive factor with respect of male sex (OR, 0.229; 95%CI, 0.053–0.987; p = 0.048). In particular, the use of broad spectrum betalacam antibiotic, including carbapenem (OR, 0.816; 95%CI, 0.151–4.403; p = 0.813), was not associated with fungal superinfection.
Antimicrobial therapy
All patients were initially treated intravenously; an oral switch could be possible for 24 (38.7%) of them, only. The total duration of antimicrobial therapy was 19.8 (IQR, 13.8–27.4) weeks, including 11.1 (IQR, 7.5–15.1) weeks after flap reconstruction. In patients with fungal infection and/or superinfection, antifungal drugs were prolonged for 25.9 (IQR, 15.3–26.9) weeks after flap reconstruction.
Outcome
Patients were followed-up for 59.1 (IQR, 37.1–121.3) weeks after debridement, 54 (IQR, 26.6–101.7) weeks after flap reconstruction, and 38.6 (IQR, 13.6–91.1) weeks after antimicrobial interruption. Fifteen (23.4%) treatment failures were diagnosed in a median delay of 12.4 (IQR, 7.3–28.3) weeks after flap coverage, necessitating an additional surgical procedure in 14 (93.3%) cases. Four patients died, including 2 deaths related to pressure ulcer-related infection. The diagnosis of treatment failure led to an increased in total antimicrobial therapy length from 9.7 (IQR, 6.8–13.6) weeks to 13.4 (IQR, 11.1–23.4) weeks (p = 0.011). The whole comparison between patients with favorable outcome and treatment failure, and risk factors for poor outcome (univariate analysis) are presented in Table 1. In multivariate analysis, independent determinants of treatment failure were the existence of a previous pressure ulcer located at the same site (OR, 5.701; 95%CI, 1.244–26.127; p = 0,025) and Actinomyces spp.-positive cultures at time of debridement (OR, 9.522; 95%CI, 1.290–70.296; p = 0,027). Results of failure-free survival curves analysis are presented in Fig. 2. Colostomy (n = 18; 28.1%), the delay between debridement and flap reconstruction, and admission in a rehabilitation center after the debridement (n = 16; 25.0%) and/or the flap coverage (n = 39; 60.9%) did not influence outcome.

Kaplan Meier curves for cumulative probability of treatment failure-free survival according to the two main risk factors highlighted in multivariate analysis, i.e., an history of previous ulcer at the same site (a) and Actinomyces spp. infection (b)
Discussion
Chronic osteomyelitis complicating end-stage pressure ulcers represent severe clinical conditions with poorly investigated management. This retrospective series provides interesting insights regarding the management of these complex bone infections, including among microbiological diagnosis and outcome of a two-stage surgical strategy in a referral center.
Diagnosis of pressure ulcer-related osteomyelitis is puzzling. Clinical assessment is often inaccurate [5], and no imaging techniques allow an acceptable discernment between osteomyelitis and pressure-related bone change, including magnetic resonance imaging [21, 23]. Histological analysis of bone biopsies does not appear to be more helpful [21]. For the microbiologist, the challenge is to distinguish between colonizing and invasive bacteria, as both originate from the commensal cutaneous and digestive flora. In the absence of validated discriminant criteria, we used a practice-based approach, considering only: i) the results of the bacteriological analysis of surgical bone biopsies sampled after the debridement step, with the exclusion of superficial and/or soft tissues samples [24]; and ii) virulent pathogens (i.e. S. aureus, Pseudomonas spp. …), and potentially contaminants if yielded on at least two samples as suggested by the US guidelines for the diagnosis of prosthetic joint infection [22], and taken into account by the treating clinician in the definitive antimicrobial regimen. The bacterial distribution observed in our study was consistent with other similar investigations, with a predominance of MSSA, streptococci, Enterobacteriaceae spp. and anaerobes [6, 21, 25]. While the diffusion of MRSA is actually controlled in Europe, ESBL-producing Enterobacteriaceae spp. are frequently implicated in pressure injury colonization and deep tissue infection, reaching 11.6% at the flap coverage step in our study. They have been associated with wound management in long-term care facilities, particularly in case of fluoroquinolone use [26], as well as highlighted by our results.
The management of chronic pelvic osteomyelitis requires a multidisciplinary approach, with comprehensive assessment of the patient’s general medical condition, proper positioning with four to six weeks of pressure off-loading on adapted support surfaces, optimized nutrition and psychosocial support [15, 27, 28]. A combined medical-surgical approach is mandatory, allowing a better outcome in case of osteomyelitis [6]. In this setting, multidisciplinary staff meetings in referral centers have not been evaluated in the specific field of pelvic osteomyelitis, but have demonstrated their advantages in orthopedic infections [29, 30]. In our center, they have made possible the crucial coordination of all the actors of the patients’ care, including the infectious disease specialists, orthopedic and plastic surgeons, microbiologists, radiologists, nuclear medicine specialists and rehabilitators. They allow an interdisciplinary decision for each complex patient case, with planning of the entire therapeutic sequence at the beginning of the patient management.
Concerning surgical strategy, some authors support a one-stage approach with immediate flap reconstruction even in case of local contamination [15]. However, among the 101 patients included in this study, bone biopsies were performed in 70% of cases and half were positive, only, so that the majority of patients were not suspected to have chronic osteomyelitis, even when it is a well-known risk factor for flap coverage failure [31, 32]. Additionally, a single-stage surgery does not allow the adaptation of the empiric antimicrobial therapy to microbiological results before flap closure; although an inappropriate initial treatment is associated with an over-risk of failure. Consequently, we believe that a first step of debridement is essential for the reduction of bacterial inoculum by necrotic tissues excision and adequate sequestrectomy, and for the realization of gold-standard bacterial samples [28, 33, 34].
Regarding antimicrobial therapy, the polymicrobial nature of pelvic osteomyelitis lead to a greater need of broad spectrum antimicrobials than in other bone infections [7]. An empiric combination of a broad-spectrum betalactam (i.e. piperacillin-tazobactam, or cefepim with metronidazole) and vancomycin can be proposed, thus targeting the most frequently involved microorganisms. An empiric prescription of a carbapenem might be only proposed to patient with high-risk of ESBL-producing Enterobacteriaceae spp., including those who had taken fluoroquinolones in the previous 6 months, as suggested by the determinants for ESBL-producing Enterobacteriaceae spp. superfinfection highlighted by our results.
As the delay between debridement and flap reconstruction does not appear to influence outcome, a short sequence can be proposed in order to reduce the length of antimicrobial therapy. An interval of 2 to 3 weeks between the two surgical steps could be reasonably proposed, allowing: i) the assessment of the evolution of the soft tissue condition; and ii) the adaptation of the antimicrobial spectrum to the definitive bacteriological culture results (requiring 2 weeks), if necessary. With regard of the high frequency of superinfections, broad spectrum antimicrobial therapy should be prolonged until the definitive culture results of the bacteriological sample performed during flap coverage which necessitate two additional weeks. A more targeted treatment – possibly relying on oral molecules with acceptable bone diffusion if available – should then be proposed for 4 additional weeks, leading to a total duration not exceeding 6 weeks after flap coverage as proposed in most similar studies [6, 35, 36], and more generally in adult chronic osteomyelitis [37, 38], in the absence of fungal or Actinomyces spp. infection that require at least 6 months of treatment [39, 40].
Pressure ulcer-related osteomyelitis outcome is poor, with an overall failure rate approaching 25% in our series. Some studies reported lower failure rates, but are associated with important bias: i) most of them used less stringent criteria for defining failure; ii) they not exclusively included patients with osteomyelitis; and iii) most had a shorter length of follow-up. For example, in a North-American study based on a national surgery database, flap coverage of pressure ulcer was associated with a recurrence rate of 1.9% with 4.7% of iterative surgical procedure but in a delay of 30 days, only [8]. However, we demonstrated that the diagnosis of failure usually occur later, in a median of 3 months after flap coverage, mostly necessitating reoperation. In a comparable series, Brunel et al. noted initial and final healing rates of 42% and 37%, only, with a relapse rate of 18% [21]. Other studies with extensive length follow-up showed similar results [11, 15, 32, 41]. Additionally, our institution is a labeled referral center for the management of complex bone and joint infection, leading to the recruitment of the most complex – and consequently the most at-risk of failure – situations, which can explain such a high treatment failure rate.
Risk factors for treatment failure are poorly known. Multiple pressure ulcers occur in more than one-third of patients, and constitute in our series a risk factor for treatment failure, as already suggested by two previous studies [11, 14]. To date, no bacteriological factor had been related to treatment failure. Interestingly, we highlighted an increased risk of failure in Actinomyces spp. osteomyelitis, which is a difficult-to-treat anaerobic bacteria that should not be considered as a contaminant and contrariwise requires prolonged (≥ 6 months) antimicrobial therapy [40]. Other previously described risk factors for treatment failure include ischial location, poor diabetes control, impaired nutrition status, active smoking, corticosteroid use and cardiovascular disease [11, 14, 32, 42,43,44,45]. The benefit of colostomy is still debated. No impact has been highlighted in our series regarding the risk of superinfection or treatment failure. Additionally, this procedure is at-risk of complications in frail patients and of questionable efficacy [46]. On the other hand, it provides a dry and clean environment that should theoretically limit the risk of fecal contamination of the debrided ulcer and promote flap healing [47].
This study is subject to some limitations, inherent to its retrospective and unicentric nature. In particular, the small sample size and the lack of controls restricts the interpretation of outcome data, event if suggesting interesting insights toward the management of pelvic osteomyelitis. However, larger and controlled evaluation are now mandatory to refine the comprehension and management of these complex bone infections.
Conclusions
Pressure ulcer-related pelvic osteomyelitis is associated with a high risk of treatment failure despite a complex surgical management and an important consumption of broad-spectrum antimicrobials, thus requiring a collaborative medical-surgical management driven by a trained multidisciplinary team in a reference center. A two-step surgical strategy (debridement – NPT – flap reconstruction) can be proposed, although a short interval (2–3 weeks) between the two procedures might be sufficient, allowing improvement of soft tissue conditions and prospective adaptation of empirical antimicrobial therapy, without excessively lengthening the total duration of treatment.
Abbreviations
- 95%CI:
-
95% Confidence interval
- ASA:
-
American society of anesthesiologists
- CoNS:
-
Coagulase negative staphylococci
- ESBL:
-
Extended spectrum betalactamase
- IQR:
-
Interquartile range
- MRCoNS:
-
Methicillin-resistant coagulase negative staphylococci
- MRSA:
-
Methicillin-resistant Staphylococcus aureus
- MSCoNS:
-
Methicillin-susceptible coagulase negative staphylococci
- MSSA:
-
Methicillin-susceptible Staphylococcus aureus
- NPT:
-
Negative pressure therapy
- NPUAP:
-
National pressure ulcer advisory panel
- OR:
-
Odd ratio.
References
Bauer K, Rock K, Nazzal M, Jones O, Qu W. Pressure ulcers in the United States’ inpatient population from e2008 to 2e012: results of a retrospective Nationwide study. Ostomy Wound Manage. 2016;62:30–8.
Bauer J, Phillips LG. MOC-PSSM CME article: Pressure sores. Plast Reconstr Surg. 2008;121:1–10.
Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieggreen M. Revised National Pressure Ulcer Advisory Panel Pressure Injury Staging System: revised pressure injury staging system. J Wound Ostomy Cont Nurs. 2016;43:585–97.
Sugarman B, Hawes S, Musher DM, Klima M, Young EJ, Pircher F. Osteomyelitis beneath pressure sores. Arch Intern Med. 1983;143:683–8.
Darouiche RO, Landon GC, Klima M, Musher DM, Markowski J. Osteomyelitis associated with pressure sores. Arch Intern Med. 1994;154:753–8.
Bodavula P, Liang SY, Wu J, VanTassell P, Marschall J. Pressure ulcer-related pelvic osteomyelitis: a neglected disease? Open Forum Infect Dis. 2015;2:ofv112.
Ramaesh R, Gaston MS, Simpson AHRW. Chronic osteomyelitis of the pelvis. Acta Orthop Belg. 2013;79:280–6.
Diamond S, Moghaddas HS, Kaminski SS, Grotts J, Ferrigno L, Schooler W. National Outcomes after pressure ulcer closure: inspiring surgery. Am Surg. 2016;82:903–6.
McCarthy JE, Rao VK. Systematic review and operative technique of recalcitrant pressure ulcers using a fillet flap technique. Plast Reconstr Surg Glob Open. 2016;4:e1001.
Brem H, Maggi J, Nierman D, Rolnitzky L, Bell D, Rennert R, Golinko M, Yan A, Lyder C, Vladeck B. High cost of stage IV pressure ulcers. Am J Surg. 2010;200:473–7.
Kierney PC, Engrav LH, Isik FF, Esselman PC, Cardenas DD, Rand RP. Results of 268 pressure sores in 158 patients managed jointly by plastic surgery and rehabilitation medicine. Plast Reconstr Surg. 1998;102:765–72.
Homma K, Murakami G, Fujioka H, Fujita T, Imai A, Ezoe K. Treatment of ischial pressure ulcers with a posteromedial thigh fasciocutaneous flap. Plast Reconstr Surg. 2001;108:1990–6. discussion 1997
Tavakoli K, Rutkowski S, Cope C, Hassall M, Barnett R, Richards M, Vandervord J. Recurrence rates of ischial sores in Para- and tetraplegics treated with hamstring flaps: an 8-year study. Br J Plast Surg. 1999;52:476–9.
Keys KA, Daniali LN, Warner KJ, Mathes DW. Multivariate predictors of failure after flap coverage of pressure ulcers. Plast Reconstr Surg. 2010;125:1725–34.
Larson DL, Hudak KA, Waring WP, Orr MR, Simonelic K. Protocol management of late-stage pressure ulcers: a 5-year retrospective study of 101 consecutive patients with 179 ulcers. Plast Reconstr Surg. 2012;129:897–904.
National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. 2014 prevention and treatment of pressure ulcers: clinical practice guideline. 2014. http://www.npuap.org/resources/educational-and-clinical-resources/prevention-and-treatment-of-pressure-ulcers-clinical-practice-guideline. Accessed 20 March 2017.
Eckardt JJ, Wirganowicz PZ, Mar T. An aggressive surgical approach to the management of chronic osteomyelitis. Clin Orthop. 1994;298:229–39.
Dumville JC, Webster J, Evans D, Land L. Negative pressure wound therapy for treating pressure ulcers. Cochrane Database Syst Rev. 2015;(5):CD011334.
Sameem M, Au M, Wood T, Farrokhyar F, Mahoney J. A systematic review of complication and recurrence rates of musculocutaneous, fasciocutaneous, and perforator-based flaps for treatment of pressure sores. Plast Reconstr Surg. 2012;130:67e–77e.
Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47:1245–51.
Brunel AS, Lamy B, Cyteval C, Perrochia H, Téot L, Masson R, Bertet H, Bourdon A, Morquin D, Reynes J, Le Moing V, OSTEAR study group. Diagnosing pelvic osteomyelitis beneath pressure ulcers in spinal cord injured patients: a prospective study. Clin Microbiol Infect. 2016;22(267):e1–8.
Osmon DR, Berbari EF, Berendt AR, Lew D, Zimmerli W, Steckelberg JM, Rao N, Hanssen A, Wilson WR. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2013;56:e1–25.
Larson DL, Gilstrap J, Simonelic K, Carrera GF. Is there a simple, definitive, and cost-effective way to diagnose osteomyelitis in the pressure ulcer patient? Plast Reconstr Surg. 2011;127:670–6.
Rudensky B, Lipschits M, Isaacsohn M, Sonnenblick M. Infected pressure sores: comparison of methods for bacterial identification. South Med J. 1992;85:901–3.
Dana AN, Bauman WA. Bacteriology of pressure ulcers in individuals with spinal cord injury: what we know and what we should know. J Spinal Cord Med. 2015;38:147–60.
Lim CJ, Cheng AC, Kennon J, Spelman D, Hale D, Melican G, Sidjabat HE, Paterson DL, Kong DC, Peleg AY. Prevalence of multidrug-resistant organisms and risk factors for carriage in long-term care facilities: a nested case-control study. J Antimicrob Chemother. 2014;69:1972–80.
Reddy M, Gill SS, Kalkar SR, Wu W, Anderson PJ, Rochon PA. Treatment of pressure ulcers: a systematic review. JAMA. 2008;300:2647–62.
Rennert R, Golinko M, Yan A, Flattau A, Tomic-Canic M, Brem H. Developing and evaluating outcomes of an evidence-based protocol for the treatment of osteomyelitis in stage IV pressure ulcers: a literature and wound electronic medical record database review. Ostomy Wound Manage. 2009;55:42–53.
Bauer S, Bouldouyre M-A, Oufella A, Palmari P, Bakir R, Fabreguettes A, Gros H. Impact of a multidisciplinary staff meeting on the quality of antibiotherapy prescription for bone and joint infections in orthopedic surgery. Med Mal Infect. 2012;42:603–7.
Uçkay I, Vernaz-Hegi N, Harbarth S, Stern R, Legout L, Vauthey L, Ferry T, Lübbeke A, Assal M, Lew D, Hoffmeyer P, Bernard L. Activity and impact on antibiotic use and costs of a dedicated infectious diseases consultant on a septic orthopaedic unit. J Inf Secur. 2009;58:205–12.
Han H, Lewis VL, Wiedrich TA, Patel PK. The value of Jamshidi core needle bone biopsy in predicting postoperative osteomyelitis in grade IV pressure ulcer patients. Plast Reconstr Surg. 2002;110:118–22.
Bamba R, Madden JJ, Hoffman AN, Kim JS, Thayer WP, Nanney LB, Spear ME. Flap reconstruction for pressure ulcers: an outcomes analysis. Plast Reconstr Surg Glob Open. 2017;5:e1187.
Maslauskas K, Samsanavicius D, Rimdeika R, Kaikaris V. Surgical treatment of pressure ulcers: an 11-year experience at the Department of Plastic and Reconstructive Surgery of Hospital of Kaunas University of medicine. Med Kaunas Lith. 2009;45:269–75.
Schiffman J, Golinko MS, Yan A, Flattau A, Tomic-Canic M, Brem H. Operative debridement of pressure ulcers. World J Surg. 2009;33:1396–402.
Jugun K, Richard J-C, Lipsky BA, Kressmann B, Pittet-Cuenod B, Suvà D, Modarrassi A, Uçkay I. Factors associated with treatment failure of infected pressure sores. Ann Surg. 2016;264:399–403.
Marriott R, Rubayi S. Successful truncated osteomyelitis treatment for chronic osteomyelitis secondary to pressure ulcers in spinal cord injury patients. Ann Plast Surg. 2008;61:425–9.
Rod-Fleury T, Dunkel N, Assal M, Rohner P, Tahintzi P, Bernard L, Hoffmeyer P, Lew D, Uçkay I. Duration of post-surgical antibiotic therapy for adult chronic osteomyelitis: a single-Centre experience. Int Orthop. 2011;35:1725–31.
Lazzarini L, Lipsky BA, Mader JT. Antibiotic treatment of osteomyelitis: what have we learned from 30 years of clinical trials? Int J Infect Dis. 2005;9:127–38.
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, Reboli AC, Schuster MG, Vazquez JA, Walsh TJ, Zaoutis TE, Sobel JD. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62:e1–50.
Valour F, Sénéchal A, Dupieux C, Karsenty J, Lustig S, Breton P, Gleizal A, Boussel L, Laurent F, Braun E, Chidiac C, Ader F, Ferry T. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014;7:183–97.
Vincent P-L, Pinatel B, Viard R, Comparin J-P, Gir P, Voulliaume D. The gluteus maximus inferior split-muscle flap for the cover of ischiatic pressure ulcers: study of 61 cases. Ann Chir Plast Esthet. 2016;61:845–52.
Foster RD, Anthony JP, Mathes SJ, Hoffman WY, Young D, Eshima I. Flap selection as a determinant of success in pressure sore coverage. Arch Surg. 1997;132:868–73.
Niazi ZB, Salzberg CA, Byrne DW, Viehbeck M. Recurrence of initial pressure ulcer in persons with spinal cord injuries. Adv Wound Care J Prev Heal. 1997;10:38–42.
Goodman CM, Cohen V, Armenta A, Thornby J, Netscher DT. Evaluation of results and treatment variables for pressure ulcers in 48 veteran spinal cord-injured patients. Ann Plast Surg. 1999;42:665–72.
Schryvers OI, Stranc MF, Nance PW. Surgical treatment of pressure ulcers: 20-year experience. Arch Phys Med Rehabil. 2000;81:1556–62.
Deshmukh GR, Barkel DC, Sevo D, Hergenroeder P. Use or misuse of colostomy to heal pressure ulcers. Dis Colon rectum. 1996;39:737–8.
Stone JM, Wolfe VA, Nino-Murcia M, Perkash I. Colostomy as treatment for complications of spinal cord injury. Arch Phys Med Rehabil. 1990;71:514–8.
Ferry T, Boucher F, Chateau J, Shipkov H, Daoud F, Braun E, Triffault-Fillit C, Perpoint T, Laurent F, Mojallal AA, Chidiac C, Valour F, on behalf on the Lyon BJI study group. Pressure ulcer-related osteomyelitis: evaluation of a two-stage surgical strategy (debridement, negative pressure therapy and flap coverage), with prolonged antimicrobial therapy. ID week 2017, San Diego, CA, USA. Poster abstract section “Clinical: Bone and joint infection”, Abstract number 224. Available at: https://idsa.confex.com/idsa/2017/webprogram/Paper63764.html. Accessed 23 Mar 2018.
Acknowledgements
Lyon Bone and Joint Infection Study Group.
Coordinator: Tristan Ferry; Infectious Diseases Specialists – Tristan Ferry, Florent Valour, Thomas Perpoint, André Boibieux, François Biron, Patrick Miailhes, Florence Ader, Agathe Becker, Sandrine Roux, Claire Triffault-Fillit, Fatiha Daoud, Johanna Lippman, Evelyne Braun, Christian Chidiac, Yves Gillet, Laure Hees; Surgeons – Sébastien Lustig, Elvire Servien, Yannick Herry, Romain Gaillard, Antoine Schneider, Michel-Henry Fessy, Anthony Viste, Philippe Chaudier, Romain Desmarchelier, Tanguy Mouton, Cyril Courtin, Lucie Louboutin, Sébastien Martres, Franck Trouillet, Cédric Barrey, Francesco Signorelli, Emmanuel Jouanneau, Timothée Jacquesson, Ali Mojallal, Fabien Boucher, Hristo Shipkov, Mehdi Ismail, Joseph Chateau; Anesthesiologists – Frédéric Aubrun, Isabelle Bobineau, Caroline Macabéo; Microbiologists – Frederic Laurent, François Vandenesch, Jean-Philippe Rasigade, Céline Dupieux; Imaging – Fabien Craighero, Loic Boussel, Jean-Baptiste Pialat; Nuclear Medicine – Isabelle Morelec, Marc Janier, Francesco Giammarile; PK/PD specialists – Michel Tod, Marie-Claude Gagnieu, Sylvain Goutelle; Prevention of infection – Solweig Gerbier-Colomban, Thomas Benet; Clinical Research Assistant – Eugénie Mabrut.
A part of this work was presented in the poster section “Clinical: Bone and joint infection” (Abstract #224) on Thursday, October 5, 2017 at the IDWeek 2017 (San Diego, CA, USA) [48].
Funding
The study was founded by the Hospices Civils de Lyon and was carried out as part of our routine work. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Consortia
Contributions
JA participated in the design of the study, in the acquisition and interpretation of data, helped to statistical analysis and drafted the manuscript. TF participated in the design of the study and in the acquisition of data. TF, FD, EB, CTF, TP, CC and FV medically managed the included patients, helped to the interpretation of medical data and to draft the manuscript. FB, JC, HS and AAM surgically managed the included patients, helped to the interpretation of surgical data and to draft the manuscript. FL performed the microbiological analysis, helped to the interpretation of microbiological data and to draft the manuscript. FV conceived of the study, participated in its design and coordination, helped to statistical analysis and to draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study (ClinicalTrial.gov registration number NCT03010293) received the approval of the French South-East Ethics Committee (reference number QH20–2014). In accordance with French legislation, written informed consent was not required for any part of the study.
Competing interests
There is no conflict of interest, for all authors.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Andrianasolo, J., Ferry, T., Boucher, F. et al. Pressure ulcer-related pelvic osteomyelitis: evaluation of a two-stage surgical strategy (debridement, negative pressure therapy and flap coverage) with prolonged antimicrobial therapy. BMC Infect Dis 18, 166 (2018). https://doi.org/10.1186/s12879-018-3076-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-018-3076-y