
Abstract
Background
In patients with triple valve replacement developing third-degree atrioventricular block (AVB), the most appropriate approach for permanent pacemaker implantation remains questionable.
Case presentation
In this case presentation, we first described the approach of implantation of the cardiac resynchronization therapy pacemaker (CRT-P) via one bipolar pacing lead in middle cardiac vein (MCV) and one quadripolar pacing lead in anterior interventricular vein (AIV) in a patient developing complete AVB, who had been previously diagnosed with rheumatic valvular heart disease with triple valve replaced. After the CRT-P implantation, the two pacing leads in coronary sinus (CS) provided a dual-site ventricular pacing from the anterior septum and posterior septum, which resulted in a narrow QRS complex and an increased ventricular synchrony. During the long-term follow-up, no deterioration of heart function was documented and pacing parameters remained good.
Conclusion
In this patient developing complete AVB with triple valve replaced, our approach of CRT-P implantation provides an effective and reliable ventricular pacing, and is an alternative option when transvenous right ventricular pacing, transseptal left ventricular pacing and transpericardial epicardium pacing are not possible. Further prospective randomized trials are required to confirm the efficiency of our approach of dual-site ventricular pacing by CRT-P in this kind patients.
Similar content being viewed by others

Background
In rheumatic heart disease patients with triple mechanical valve replacement and complete atrioventricular block (AVB), the most appropriate and beneficial method of pacemaker implantation remains questionable. With the tricuspid mechanical valve replaced, endocardial pacing of the right ventricle is not possible because such a manipulation may cause disastrous damage to the prosthetic valve [1]. In addition, left ventricular endocardial pacing via the atrial septum puncture was contraindicated due to the replacement of the mitral mechanical valve [2]. Epicardial pacing was also limited because of rheumatic pericardial adhesion and unsatisfying pacing parameters [3]. In this kind patients, a single lead in the coronary sinus (CS) to pace the left ventricle has been reported [3,4,5], however, it may lead ventricular dyssynchronization, and in the event of CS lead dislodgement or malfunction, the underlying complete AVB could be life-threatening. Here, we presented a case where we applied dual-site ventricular pacing by cardiac resynchronization therapy pacemaker (CRT-P) implantation, with one bipolar pacing lead in the middle cardiac vein (MCV) and one quadripolar pacing lead in the anterior interventricular vein (AIV) to simultaneously stimulate the ventricle in a patient with triple valve replacement.
Case presentation
A 42-year-old woman with a history of rheumatic valvular heart disease and permanent atrial fibrillation underwent open triple valvotomy 14 years ago and routinely took the warfarin to anti-coagulate since then. The international normalized ratio of prothrombin time (PT-INR) was monitored every 2 weeks to keep it range between 2.5 and 3.5 s. She complained of persistent abdominal distension and repeated exertional dyspnea for 2 years at admission. Physical examination showed obvious body signs of right heart failure, including jugular vein distention, lower limb pitting edema. The 12-lead surface ECG showed atrial fibrillation rhythm with narrow QRS complex. The transthoracic echocardiography indicated a normal ventricular size of 35 mm with left ventricular ejection fraction (LVEF) of 65% and a moderate stenosis of tricuspid valve with the pressure gradient across the tricuspid valve of 8 mmHg. Laboratory examination revealed the NT-pro-BNP of 1780 ng/ml. Due to progression of heart failure from her valvular heart disease, she underwent tricuspid valve replacement again (Medtronic bileaflet prosthesis). On the second day after surgery, the patient developed sudden cardiac arrest with bedside electrocardiographic monitor recording atrial fibrillation, complete third-degree AVB with repeated episodes of torsade de point secondary to the long QT interval (0.6 s). Thus, a permanent pacemaker was required to oppose this malignant arrhythmia.
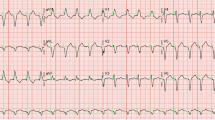
After taking full consideration of the patient’s basic situations, the CRT-P implantation via two pacing leads in cardiac venous system to provide dual-site ventricular pacing was primarily planned. As the patient with triple mechanical valve replaced had a relatively higher risk for thrombosis, the oral warfarin was not interrupted before operation. The instant blood test prior to operation showed a PT-INR of 2.42 s. The intravenous unfractionated heparin was used during the procedure to keep an activated clotting time (ACT) range between 250 and 300 s. Electric surgical knives were applied to stop bleeding of the incision during the whole procedure. A guiding catheter was delivered via left subclavian vein puncture to access the coronary sinus ostium, which was located between the inferior vena cava and the mechanical tricuspid valve on the inferior aspect of the atrial septum. A retrograde occlusion venogram was then performed to evaluate the anatomy of the cardiac venous system. As the lateral cardiac vein was too thin and the posterolateral vein was too tortuous for pacing leads to access, the MCV and the AIV were selected as target vessels for pacing leads placement. A quadripolar pacing lead (Quartet LV lead model 1458Q, St Jude Medical) was introduced into the AIV, while bipolar pacing lead (Quick Flex μ model 1258 T, St Jude Medical) into the MCV, both leads were secured to the pectoral muscle fascia and attached to a CRT-P (Allure Quadra™ CRT-P, St Jude Medical), Fig. 1. For the patient was in the permanent atrial fibrillation rhythm, the atrial lead placement was abandoned due to the inability to achieve an atrioventricular synchrony. The pacing rate was initially set at 100 bpm in a VVI pacing mode (ventricle paced, ventricle sensed, pacing is inhibited if beat is sensed). By the procedure of pacing interval optimization between the two pacing leads, we obtained a relatively narrowest QRS duration of 116 ms among all bipolar and unipolar pacing configurations, using the vector from the proximal tip (P4) of quadripolar lead to the coil of bipolar lead in MCV, vector P4–MCV coil, Fig. 2 and Table 1. At the beginning of the pacemaker implantation, the quadripolar lead paced with a capture threshold of 1.75 V at 1.0 ms pulse width with an impedance of 430 Ω, while the bipolar lead paced with a capture threshold of 1.5 V at 1.0 ms pulse width with an impedance of 600 Ω, using the vector P4–MCV coil. After the operation, the compression of pacemaker pocket with elastic bandage was immediately performed and removed after 48 h, no pocket hematoma and other bleedings was found, the PT-INR was measured of 2.28 s 24 h later. The left ventricular systolic function was evaluated with Simpsons method by transthoracic echocardiography within the first 24 h after pacemaker implantation. The ventricular dual-site pacing exhibited an obvious acute hemodynamic improvement over single-site pacing (LVEF: ventricular dual-site pacing 71.5 ± 0.96% vs ventricular single-site pacing 62.9 ± 2.38%), and the best left ventricular systolic function was obtained by ventricular dual-site pacing of P4 combined with MCV, Table 2. A remarkable decline in pacing threshold of both leads was found 2 months later, the quadripolar lead paced with a capture threshold of 0.75 V at 0.5 ms pulse width with an impedance of 490 Ω while the bipolar lead paced with a capture threshold of 1.25 V at 0.8 ms pulse width with an impedance of 550 Ω using the vector P4–MCV coil. During one-year follow-up, the patient was VVI pacing mode dependent with an intrinsic heart rhythm of atrial fibrillation with complete AVB. She did not present deteriorations of heart function in transthoracic echocardiography (LVEDD 40 mm, LVEF 75.4%, see Fig. 3) with 6-min walking test recording a walking distance more than 450 m, meanwhile, CRT programming control showed good pacing parameters all the time.

A quadripolar pacing lead (Quartet LV lead model 1458Q, StJude Medical) was introduced into anterior interventricular vein (AIV), while a bipolar pacing lead (QuickFlex μ model 1258 T, St Jude Medical) into middle cardiac vein (MCV). a. Anteroposterior position. b. Right anterior oblique position

The procedure of pacing interval optimization between the two pace leads

Systolic heart function evaluated by Simpsons method
Discussion
In this case, we first described the method of implantation of CRT-P with two pacing leads in coronary venous system, which provided an effective dual-site ventricular pacing in a patient developing complete atrioventricular block after triple mechanical valves replacement.
In this patient, as the mechanical tricuspid and mitral valves implanted, placing pacing lead in right ventricular endocardium across the tricuspid valve was forbidden because of underlying risk of valve damage and failure, in addition, delivering pacing lead to left ventricular endocardium via the atrial septum puncture was also contraindicated due to the potential damage to the mitral valve [1, 2]. The method of placing an epicardial pacing lead via the thoracotomy was technically challenging, because of severe pericardial adhesion caused by the rheumatic heart disease and previous surgery in this patient, meanwhile, in such a situation, long-term epicardial pacing tended to be unreliable with high pacing thresholds [3]. The method of the coronary sinus single-site ventricular pacing was also taken into consideration [4]. Recently, a retrospective clinical study reported that in patients with tricuspid valvular replacement, coronary sinus single-site left ventricular pacing was a feasible alternative to right apical ventricular pacing. However, this study also revealed that long-term coronary sinus single-site pacing resulted in an inferior left ventricular systolic function compared with standard cardiac resynchronization therapy, in addition, in their study, a patient of long-term coronary sinus single-site ventricular pacing was found developing pacing-induced cardiomyopathy with progressive decline in LVEF [5]. Moreover, in this patient of complete AVB, if single pacing lead in coronary sinus was selected, in the event of coronary sinus lead dislodgement or malfunction, the underlying complete AVB could be life-threatening. Based on these considerations, the idea of CS single-site pacing was abandoned. The outcomes of BLOCK-HF research indicated that the superior long-term clinical and functional benefit of dual-site ventricular pacing in patients with AV block and mild/moderate heart dysfunction compared with single-site ventricular pacing [6]. Thus, in this patient, after full consideration, the dual-site ventricular pacing via coronary sinus method was primarily chosen. Different from classical cardiac resynchronization therapy with dual-site pacing (LV free wall pacing from the coronary venous system in conjunction with RV apical pacing), in this patient, we performed dual-site ventricular pacing via coronary sinus by implantation of CRT-P with one bipolar lead in the MCV and one quadripolar lead in the AIV, which provided an anterior ventricular wall pacing in conjunction with a posterior ventricular wall pacing. By our method of ventricular dual-site pacing in coronary sinus, increased ventricular electrical and mechanical synchronization was obtained, long-term follow up also showed a good clinical outcome. However, before our approach of dual-site CS pacing can be recommended to more patients, a prospective study is needed to prove this preliminary finding.
In this patient, due to a relatively higher thrombotic risk associated with triple mechanical valve replacement, the oral anticoagulant therapy of warfarin was not interrupted and a bridging therapy with low-molecular-weight heparin (LMWH) was not initiated. Though this protocol was some different from the standard anticoagulation protocol at the time of pacemaker implantation, which required stopping oral anticoagulation therapy and initiating a bridging therapy with subcutaneous LMWH, no pocket hematoma and thromboembolic events was found in this patient. Our observation further confirmed the safety of anticoagulation protocol proposed by the POCKET study [7].
Conclusions
CRT-P implantation with two pacing leads in coronary sinus can provide an effective and reliable dual-site ventricular pacing. Further prospective randomized trials are required to confirm the efficiency of our approach of dual-site ventricular pacing by CRT-P.
Abbreviations
- ACT:
-
Activated clotting time
- AIV:
-
Anterior interventricular vein
- AVB:
-
Atrioventricular block
- CRT-P:
-
Cardiac resynchronization therapy pacemaker
- CS:
-
Coronary sinus
- LMWH:
-
Low-molecular-weight heparin
- LVEDD:
-
Left ventricular end diastolic diameter
- LVEF:
-
Left ventricular ejection fraction
- MCV:
-
Middle cardiac vein
- PT-INR:
-
International normalized ratio of prothrombin time
- VVI:
-
ventricle paced, ventricle sensed, pacing is inhibited if beat is sensed
References
Lee ME. Special considerations in ventricular pacing in patients with tricuspid valve disease. Ann Thorac Surg. 1983;36(1):89–92.
Bracke FA, van Gelder BM, Dekker LR, Houthuizen P, Ter Woorst JF, Teijink JA. Left ventricular endocardial pacing in cardiac resynchronisation therapy: moving from bench to bedside. Neth Heart J. 2012;20(3):118–24.
Vijayakumar M, Kamath P, Pai PG. Permanent pacing in a patient with tricuspid prosthesis--widening therapeutic use of coronary sinus. Indian Heart J. 2013;65(5):611–3.
Sideris S, Drakopoulou M, Oikonomopoulos G, Gatzoulis K, Stavropoulos G, Limperiadis D, Toutouzas K, Tousoulis D, Kallikazaros I. Left ventricular pacing through coronary sinus is feasible and safe for patients with prior tricuspid valve intervention. Pacing Clin Electrophysiol. 2016;39(4):378–81.
Noheria A, van Zyl M, Scott LR, Srivathsan K, Madhavan M, Asirvatham SJ, McLeod CJ. Single-site ventricular pacing via the coronary sinus in patients with tricuspid valve disease. Europace. 2017. Epub ahead of print.
Goldschmidt H. Biventricular pacing for atrioventricular block and systolic dysfunction. N Engl J Med. 2013;369(6):578–9.
Malagu M, Trevisan F, Scalone A, Marcantoni L, Sammarco G, Bertini M. Frequency of “pocket” hematoma in patients receiving vitamin K antagonist and antiplatelet therapy at the time of pacemaker or cardioverter defibrillator implantation (from the POCKET study). Am J Cardiol. 2017;119(7):1036–40.
Acknowledgements
None.
Funding
This case presentation is supported by Zhejiang Provincial Public Technology Application Research Project (Grant No. 2016C33181).
Availability of data and materials
The data and materials of this manuscript available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
ZC, LWQ, LYZ, LH, LZR, CJH and LJF collected, analyzed and interpreted the data, ZC and LJF performed the operation and drafted the article. CJF revised written English of the article. All authors have seen and approved the final version of the manuscript being submitted. The article is the authors’ original work, hasn’t received prior publication and isn’t under consideration for publication elsewhere.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This was a case presentation of a patient treated at the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University. The treatment this patient received was considered standard care for her condition. The Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University approved the present case presentation.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images and tables. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Zheng, C., Lin, WQ., Lin, YZ. et al. Case presentation: implantation of cardiac resynchronization therapy pacemaker via the coronary sinus in a patient with triple valve replacement. BMC Cardiovasc Disord 18, 37 (2018). https://doi.org/10.1186/s12872-018-0775-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-018-0775-7