
Abstract
Background
The leading cause of death among firefighters in the United States (U.S.) is cardiovascular events (CVEs) such as sudden cardiac arrest and myocardial infarction. This study compared the cost-effectiveness of three strategies to prevent CVEs among firefighters.
Methods
We used a cost-effectiveness analysis model with published observational and clinical data, and cost quotes for physiologic monitoring devices to determine the cost-effectiveness of three CVE prevention strategies. We adopted the fire department administrator perspective and varied parameter estimates in one-way and two-way sensitivity analyses.
Results
A wellness-fitness program prevented 10% of CVEs, for an event rate of 0.9% at $1440 over 10-years, or an incremental cost-effectiveness ratio of $1.44 million per CVE prevented compared to no program. In one-way sensitivity analyses, monitoring was favored if costs were < $116/year. In two-way sensitivity analyses, monitoring was not favored if cost was ≥ $399/year. A wellness-fitness program was not favored if its preventive relative risk was >0.928.
Conclusions
Wellness-fitness programs may be a cost-effective solution to preventing CVE among firefighters compared to real-time physiologic monitoring or doing nothing.
Similar content being viewed by others

Background
The United States (U.S.) fire service is a critical resource for public health and safety. According to the National Fire Protection Association, there are an estimated 30,052 fire departments and 1.1 million firefighters in the U.S. [1]. In 2013, firefighters responded to more than 370,000 residential fires [2]. The occupation is hazardous and poses a unique set of challenges for public health officials and administrators of fire departments. Cardiovascular disease is a leading cause of line-of-duty-death (LODD) among firefighters [3], and from 1995 to 2004, nearly half of all on-duty fatalities were linked to sudden cardiac death [4]. Data show that firefighters experience a disproportionately higher rate of cardiovascular events (CVEs) and mortality than individuals in other occupations, including police and other public safety workers [5]. Although fire suppression is physically strenuous and provides triggers for CVE [6, 7], a high prevalence of overweight, obesity, and physical inactivity among firefighters likely contributes to CVE in fire service [8, 9]. Efforts to reduce CVEs and improve firefighter health have increased; yet there are limited data and guidance on cost-effectiveness of diverse prevention strategies.
There are two commonly discussed approaches to reducing CVEs among firefighters. The first and most widely recognized approach is the adoption of a wellness and fitness program. Since 1997, the International Association of Firefighters, International Association of Fire Chiefs, and National Fallen Firefighters Foundation have advocated mandatory wellness and fitness programs for firefighters. Advocacy stems from an epidemic of overweight and obesity in the fire service – higher than the general population [9]. Where adopted, wellness and fitness programs have generally been successful at improving many metrics of fitness including higher cardiorespiratory capacity and improved body composition [10]. These programs have not been widely implemented in the fire service.
An alternative to wellness/fitness programs is use of real-time physiologic monitoring of firefighters during emergency duties to actively identify firefighters at risk of CVEs. These devices can be worn by firefighters for hours and are capable of collecting basic physiologic parameters such as heart rate, respiration, temperature, and electrocardiogram (ECG). Several devices are commercially available and a large study of physiologic monitoring has been funded by the U.S. Department of Homeland Security (HSHQDC-10-C-00089:P00001). The capabilities of these devices vary but commonly they measure heart rate or ECG and some surrogate of body temperature such as skin temperature or galvanic skin temperature. Devices may have built in alarms to warn the firefighter that they have reached some threshold value of physiology or may transmit data in real time to a monitoring station. Multiple studies have attempted to validate the devices within the context of fire suppression and it seems likely this trend in research of device application and functionality will continue [11, 12].
There is increasing evidence to support mandatory or voluntary wellness and fitness programs for primary prevention of CVE among firefighters and this approach has greater overall benefits for workforce health [13, 14]. However, the incomplete penetration of voluntary or mandatory wellness and fitness programs may require alternate strategies for reducing CVE, such as use of wearable real-time physiologic monitoring technology. There are limited data to support real-time physiologic monitors as a CVE prevention strategy, yet research continues in this area and future devices may support use in the fire service. Administrators at multiple levels of the fire service lack guidance to make informed decisions. What are the advantages and disadvantages of these strategies in the fire service from a cost perspective? We sought to provide information on cost-effectiveness to guide management of CVE risk in the fire service. We used decision analysis to perform a cost-effectiveness analysis comparing a wellness/fitness program, real-time monitoring, and doing nothing.
Methods
Study population
Our cost-effectiveness analysis took a fire department/local government administrator perspective, accessing the costs that they are subject to in seeking to prevent firefighter CVEs (Table 1).
We used a decision model to estimate the cost-effectiveness of options for addressing firefighter CVE risk. Decision analysis compares the value of different decision alternatives [15], and are widely used to address complex questions in diverse industries [16]. From a conceptual standpoint, decision analysis models are a framework for a math problem, with probabilities, costs, and outcomes for each strategy stated quantitatively and the expected value of each strategy calculated, then incrementally compared [17]. To test the robustness of analysis results, sensitivity analyses are then performed, systematically varying model parameters through plausible ranges [17]. When particular components of a decision are unknown, the combination of decision analysis modeling and sensitivity analysis can be particularly useful. In this case, where the benefits and costs of interventions to prevent CVE in firefighters are unclear, our analyses can illustrate which components/parameters related to decisions are most influential in driving analysis results and thus would be the most valuable areas for further research to decrease decision uncertainty. In addition, our analyses of can reveal, through sensitivity analyses, what components of a decision (e.g., probabilities and costs) would need to be in order for a given strategy to be favored. The University of Pittsburgh Institutional Review Board approved our study protocol.
Measures
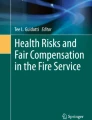
The effectiveness term of interest was CVE prevented, thus the calculated incremental cost-effectiveness ratio was cost per CVE prevented. We compared two interventions, wellness-fitness programs and real-time physiologic monitoring, which were compared to a third approach where no preventive program was undertaken (Fig. 1). We obtained one-year firefighter cardiovascular disease-related disability costs and cost of a worksite wellness/fitness program per employee per year from the published literature [18–20]. Real-time monitoring device costs were quoted estimates from Zephyr Technology Corporation and CARRE Technologies received March/April 2015. We calculated the 10-year probability of a CVE with the National Heart, Lung, and Blood Institute’s Risk Assessment Tool for Estimating Your 10-Year Risk of Having a Heart Attack (cvdrisk.nhlbi.nih.gov), using the following parameters: Age = 38, Gender = Male, Total Cholesterol = 156 mg/dL, HDL Cholesterol = 38 mg/dL, Smoker = No, Systolic Blood Pressure = 124 mm/Hg, On Medication for HBP = No), obtained from a longitudinal cohort study of firefighters [9]. Based on intervention effectiveness, strategies accounted for potential decreases in CVE rates and were varied in sensitivity analyses (Table 1).

Decision Tree. Figure 1 Notes/Legend: Schematic representation of the decision analysis model. Brackets indicate that the subsequent node will be attached to all prior branches of the decision tree
Statistical analyses
In cost effectiveness analyses, costs and health outcomes are incrementally compared between intervention strategies, using the formula \( \frac{\mathrm{Cost}\left(\mathrm{x}+1\right)-\mathrm{Cost}\left(\mathrm{x}\right)}{\mathrm{Effect}\left(\mathrm{x}+1\right)-\mathrm{Effect}\left(\mathrm{x}\right)}=\frac{\Delta \mathrm{Cost}}{\Delta \mathrm{Effect}} \) where Effect = the health outcome of a strategy and x is the rank order of a strategy after ordering by ascending cost [17]. The resulting incremental cost-effectiveness ratios, comparing the wellness-fitness program strategy and the real-time physiologic monitoring strategy, were then compared to firefighter disability costs: strategies with incremental costs per CVE event prevented greater than the disability cost were considered less affordable than programs with lesser costs. We used $2,000,000 as the 10-year disability cost, which was calculated after 3% per year discounting using the low end of the yearly cost range. All parameters were varied individually in 1-way sensitivity analyses over the ranges shown in Table 1 to test the robustness of the base care analysis results, which used the parameter point estimate values. Parameters whose variation caused the favored strategy to change were noted and, of these, selected parameters were examined further in multi-way analyses designed to outline scenarios where strategies could be considered economically reasonable when parameter values were varied over clinically plausible ranges. There is particular uncertainty regarding the effectiveness of wellness programs and physiologic monitors in preventing CVEs among firefighters. Therefore, we performed a series of 2-way sensitivity analyses, simultaneously varying them over their listed ranges in several monitoring cost scenarios.
Results
In the base case, firefighters with no preventive program have a 1% CVE rate over 10 years. A wellness/fitness program prevented 10% of these, for an event rate of 0.9% at a cost of $1440 over 10 years, or an incremental cost-effectiveness ratio, compared to no program, of $1.44 million per CVE prevented. Physiologic real-time monitors had the same effectiveness as wellness/fitness programs and cost more. In this situation, physiologic monitors are a dominated strategy (the same or lesser effectiveness and higher costs) and would thus not be chosen. The strategy of implementing a wellness/fitness program is favored when using a $2 million per CVE prevented cost-effectiveness threshold.
In 1-way sensitivity analyses, only variation of the CVE probability, the wellness/fitness program CVE relative risk, wellness/fitness program costs, and yearly monitoring costs caused wellness/fitness programs to no longer be favored at a $2 million per CVE threshold. If CVE probability was <0.72% (base case value 1%), wellness/fitness program CVE relative risk was >0.928 (base case 0.9), or yearly wellness/fitness program costs were >$200 (base case $144), no program became the favored strategy. If yearly monitoring costs were <$116 (base case $399), monitoring became the favored strategy.
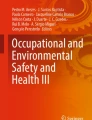
Two-way sensitivity analyses, simultaneously varying the relative effectiveness of wellness/fitness programs and monitoring over a range of monitoring cost scenarios, are shown in Fig. 2. Monitoring was never favored (at $2,000,000/CVE prevented), regardless of its cost, if its effectiveness relative risk is >0.98 or if its yearly maintenance cost is ≥$399. A wellness/fitness program is not favored if its relative risk is >0.928; at these relative risks, the no program strategy is favored if monitoring costs are high.

Sensitivity Analysis. Figure 2 Notes/Legend: Sensitivity analysis, varying the relative risk of CVEs with a wellness/fitness program (the x-axis of each graph), the relative risk with a monitor (the y-axis of each graph), the initial monitor cost (columns of graphs), and the yearly monitor maintenance cost as a percentage of the initial cost (rows of graphs). Shaded areas within each graph depict favored strategies when the willingness to pay is $2,000,000 per CVE avoided over a 10-year time horizon
Discussion
While increased fitness protects against cardiovascular disease [21], the cost-effectiveness of wellness/fitness programs versus real-time physiologic monitors for CVE prevention on the fire-ground is uncertain. With this in mind, we performed a cost-effectiveness analysis, not to find a definitive answer, but to define what the characteristics of interventions would need to be for them to be considered cost-effective. In our base case analysis, where the relative risk of CVE was 0.9 with either a wellness/fitness program or physiologic monitors compared to no program or monitor (i.e., the status quo in most departments), a wellness/fitness program, but not physiologic monitors, was considered cost-effective when the discounted cost of 10-years of disability, $2,000,000 per CVE prevented, was the cost-effectiveness criterion. This result is sensitive to variation of many model parameters, including intervention-specific CVE prevention and monitoring device cost. Our analysis points out what areas of uncertainty are most important to explore through further research and defines the importance of intervention cost on determinations of cost-effectiveness.
Adoption of wellness/fitness programs within the fire service has been slow but there is increasing awareness of the need to reduce CVE among firefighters. The National Fire Protection Agency – a global non-profit organization that promotes standard development, research, and education for the fire service – maintains a consensus-derived standard (NFPA 1583) that encourages fire departments to establish and provide health-related fitness programs. Firefighters in departments that operate well-developed wellness/fitness programs are healthier, more fit, and have fewer CVE risk factors [13]. Despite support for worksite programs and promising research findings [13], few fire departments require or mandate comprehensive wellness/fitness programs [22]. Our analyses suggest that worksite wellness/fitness programs may be cost-effective for many fire departments and provide the additional benefit of a fitter workforce.
Use of real-time physiologic monitoring is novel and attractive because the greatest risk of CVE among firefighters predominately occurs around emergency activities, such as fire suppression [12]. Firefighters identified to be at risk of a CVE on the fireground may be quickly extricated in hopes of preventing CVE. Use of real-time physiologic monitors may extend beyond the fireground and aid in early identification of distress occurring hours after a high-stress incident. Unfortunately, research exploring use and utility of continuous physiologic monitoring is incomplete and information on cost limited [11, 12]. This creates a dilemma for fire department administrators and physician medical directors. The technology is available and many firefighters do not participate in worksite wellness/fitness programs, thus physiologic monitoring may be considered in spite of limited evidence for effectiveness. We determined that if physiologic monitors have the same effectiveness as wellness/fitness programs and they cost more than fitness/wellness programs, monitors would not be favored. Sensitivity analyses suggest real-time monitors are not favored when monitoring program maintenance costs are ≥$399 per year or if the relative risk of CVE with monitor use is >0.98. With time, the unit costs may decline with increased market penetration and competition, making the monitoring strategy more cost-effective if this occurs.
Limitations
Our analysis is limited by data availability, which led us to use the analysis to understand and illustrate the importance of uncertain parameter values. We used data published in peer-reviewed manuscripts and quoted values of equipment provided from vendors. We varied all parameters widely in sensitivity analyses. Our findings highlight the need for future research comparing the effectiveness of diverse wellness/fitness programs and understanding whether these programs should be mandatory or voluntary. Although continuous, real-time physiologic monitoring is available and heavily marketed to the fire service, there are no established thresholds of physiology currently measured by these devices (e.g., a critical temperature) that can consistently predict unstable physiology or imminent collapse. In addition to understanding the costs of implementation, future research must elucidate the utility, impact, and cost of real-time physiologic monitoring devices during and post fire-ground events.
In addition, our use of CVE as the effectiveness term will not capture other benefits that might occur as a result of intervention programs, such as improved quality of life, better prevention of, or outcomes from other disease processes, or longer life span. Similarly, our use of a fire department/local government perspective, rather than a broader health care system or societal perspective, might also bias against an intervention.
We did not consider strategies that are uncommonly used in the US, a potential limitation. For this reason we did not consider programs combining wellness efforts and monitoring, wellness/fitness programs that are not on site, or the use of routine periodic cardiac testing in our analysis.
Conclusions
We conclude that wellness/fitness programs may be a cost-effective solution to preventing CVE among firefighters, being more often favored in the likeliest parameter value ranges. With mature technology, real-time continuous physiologic monitoring may be useful in certain scenarios; however understanding the likelihood of such scenarios will require better and more transparent information on monitoring costs and preventive effectiveness.
Abbreviations
- CVE:
-
Cardiovascular event
- ECG:
-
Electrocardiogram
- FEMA:
-
Federal emergency management agency
- HBP:
-
High blood pressure
- HDL:
-
High density lipoprotein
- LODD:
-
Line of duty death
- U.S.:
-
United States of America
References
Haynes HJG, Stein GP. U.S. Fire department profile 2013. Quincy: National Fire Protection Association; 2014.
USFA. Residential building fires (2011–2013), vol. 16. Emmitsburg: U.S. Department of Homeland Security, U.S. Fire Administration, National Fire Data Center; 2015.
Soteriades ES, Smith DL, Tsismenakis AJ, Baur DM, Kales SN. Cardiovascular disease in US firefighters: a systematic review. Cardiol Rev. 2011;19(4):202–15.
Fahy RF. U.S. Firefighter fatalities Due to sudden cardiac death, 1995–2004. In: National fire protection association. Quincy: National Fire Protection Association; 2005. p. 1–9.
CDC. Fatalities among volunteer and career firefighters --United States, 1994–2004. MMWR Morb Mortal Wkly Rep. 2006;55(16):453–5.
Al-Zaiti SS, Rittenberger JC, Reis SE, Hostler D. Electrocardiographic responses during fire suppression and recovery among experienced firefighters. J Occup Environ Med. 2015;57(9):938–42.
Colburn D, Suyama J, Reis SE, Morley JL, Goss FL, Chen YF, Moore CG, Hostler D. A comparison of cooling techniques in firefighters after a live burn evolution. Prehosp Emerg Care. 2011;15(2):226–32.
Jahnke SA, Poston WS, Haddock CK, Jitnarin N. Obesity and incident injury among career firefighters in the central United States. Obesity. 2013;21(8):1505–8.
Poston WS, Haddock CK, Jahnke SA, Jitnarin N, Tuley BC, Kales SN. The prevalence of overweight, obesity, and substandard fitness in a population-based firefighter cohort. J Occup Environ Med. 2011;53(3):266–73.
Osilla KC, Van Busum K, Schnyer C, Larkin JW, Eibner C, Mattke S. Systematic review of the impact of worksite wellness programs. Am J Manag Care. 2012;18(2):e68-81. Review. PubMed PMID:22435887.
Dolezal BA, Boland DM, Carney J, Abrazado M, Smith DL, Cooper CB. Validation of heart rate derived from a physiological status monitor-embedded compression shirt against criterion ECG. J Occup Environ Hyg. 2014;11(12):833–9.
Smith DL, Haller JM, Dolezal BA, Cooper CB, Fehling PC. Evaluation of a wearable physiological status monitor during simulated fire fighting activities. J Occup Environ Hyg. 2014;11(7):427–33.
Poston WS, Haddock CK, Jahnke SA, Jitnarin N, Day RS. An examination of the benefits of health promotion programs for the national fire service. BMC Public Health. 2013;13(805):1–14.
Leffer M, Grizzell T. Implementation of a physician-organized wellness regime (POWR) enforcing the 2007 NFPA standard 1582: injury rate reduction and associated cost savings. J Occup Environ Med. 2010;52(3):336–9.
Petitti DB. Introduction. In: Meta-analysis, decision analysis, and cost-effectiveness analysis: methods for quantitative synthesis in medicine. 2nd ed. New York: Oxford University Press; 2000. p. 1–12.
Petitti DB. Overview of the methods. In: Meta-analysis, decision analysis, and cost-effectiveness analysis: methods for quantitative synthesis in medicine. 2nd ed. New York: Oxford University Press; 2000. p. 13–32.
Gold MR, Siegel JE, Russell LB, Weinstein MC. Cost effectiveness in health and medicine. New York: Oxford University Press; 1996.
Ratchford EV, Carson KA, Jones SR, Ashen MD. Usefulness of coronary and carotid imaging rather than traditional atherosclerotic risk factors to identify firefighters at increased risk of cardiovascular disease. Am J Cardiol. 2014;113(9):1499–504.
Baicker K, Cutler D, Song Z. Workplace wellness programs can generate savings. Health Aff (Millwood). 2010;29(2):304–11.
Naydeck BL, Pearson JA, Ozminkowski RJ, Day BT, Goetzel RZ. The impact of the highmark employee wellness programs on 4-year healthcare costs. J Occup Environ Med. 2008;50(2):146–56.
Tanasescu M, Leitzmann MF, Rimm EB, Hu FB. Physical activity in relation to cardiovascular disease and total mortality among men with type 2 diabetes. Circulation. 2003;107(19):2435–9.
Kuehl KS, Elliot DL, Goldberg L, Moe EL, Perrier E, Smith J. Economic benefit of the PHLAME wellness programme on firefighter injury. Occup Med (Lond). 2013;63(3):203–9.
Acknowledgements
None.
Funding
Work performed on this study was supported by a grant from the Federal Emergency Management Agency (FEMA) – Grant Number: EMW-2011-FP-00651. Interpretations of study findings do not represent the opinions or views of FEMA.
Availability of data and materials
Data for this study were obtained from existing, publicly available sources. Data for our calculation came from a publicly available peer-reviewed publication (Poston WS, et al.: The prevalence of overweight, obesity, and substandard fitness in a population-based firefighter cohort. J Occup Environ Med 2011, 53(3):266–273). We used these data to calculate the 10-year probability of a CVE with the National Heart, Lung, and Blood Institute’s Risk Assessment Tool located at the following website: (cvdrisk.nhlbi.nih.gov). Some data were obtained from private companies providing device cost related information. These latter data will not be shared for purposes of continued data analysis and development of future related research protocols. Please contact co-author Dr. David Hostler with questions regarding device cost estimates: dhostler@buffalo.edu.
Authors’ contributions
All authors participated in generation of the study idea and aims. All authors participated in data collection. Author KJS was the lead data analyst and guided interpretation of study findings. All authors participated in drafting and approving the manuscript for submission to peer-review.
Author’s information
Dr. Hostler is a world-renowned expert in physiology and health of firefighters. Dr. Patterson is a renowned expert in safety of public safety firefighters and emergency personnel. He is also experienced in developing and testing cost models. Dr. Smith is expert in cost-effectiveness (CE) analyses and has applied CE modeling to numerous research questions relevant to clinical care and public health. See select relevant citations below.
Dr. Hostler:
1: Hostler D, Colburn D, Rittenberger JC, Reis SE. Effect of Two Work-to-Rest Ratios on Cardiovascular, Thermal, and Perceptual Responses During Fire Suppression and Recovery. Prehosp Emerg Care. 2016 Apr 14:1–7. [Epub ahead of print] PubMed PMID: 27077784.
2: Al-Zaiti S, Rittenberger JC, Reis SE, Hostler D. Electrocardiographic Responses During Fire Suppression and Recovery Among Experienced Firefighters. J Occup Environ Med. 2015 Sep;57(9):938–42. doi: 10.1097/JOM.0000000000000507. PubMed PMID: 26340281.
Dr. Patterson:
1: Patterson PD, Suyama J, Reis SE, Weaver MD, Hostler D. What does it cost to prevent on-duty firefighter cardiac events? A content valid method for calculating costs. Adv Prev Med. 2013;2013:972724. doi: 10.1155/2013/972724. Epub 2013 Dec 22. PubMed PMID: 24455288; PubMed Central PMCID: PMC3881339.
2: Patterson PD, Jones CB, Hubble MW, Carr M, Weaver MD, Engberg J, Castle N. The longitudinal study of turnover and the cost of turnover in emergency medical services. Prehosp Emerg Care. 2010 Apr-Jun;14(2):209–21. doi: 10.3109/10903120903564514. PubMed PMID: 20199235; PubMed Central PMCID: PMC2883888.
Dr. Smith:
1: Smith KJ, Kuo S, Zgibor JC, McTigue KM, Hess R, Bhargava T, Bryce CL. Cost effectiveness of an internet-delivered lifestyle intervention in primary care patients with high cardiovascular risk. Prev Med. 2016 Jun;87:103–9. doi: 10.1016/j.ypmed.2016.02.036. Epub 2016 Feb 24. PubMed PMID: 26921656.
2: Michaelidis CI, Zimmerman RK, Nowalk MP, Smith KJ. Cost-effectiveness of programs to eliminate disparities in elderly vaccination rates in the United States. BMC Public Health. 2014 Jul 15;14:718. doi: 10.1186/1471-2458-14-718. PubMed PMID: 25023889; PubMed Central PMCID: PMC4223514.
3: Smith KJ, Wateska A, Nowalk MP, Raymund M, Lee BY, Zimmerman RK, Fine MJ. Cost-effectiveness of procalcitonin-guided antibiotic use in community acquired pneumonia. J Gen Intern Med. 2013 Sep;28(9):1157–64. doi: 10.1007/s11606-013-2400-x. PubMed PMID: 23463457; PubMed Central PMCID: PMC3744292.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The University of Pittsburgh Institutional Review Board approved this study as exempt from human subjects research (protocol number: PRO14070193).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Patterson, P.D., Smith, K.J. & Hostler, D. Cost-effectiveness of workplace wellness to prevent cardiovascular events among U.S. firefighters. BMC Cardiovasc Disord 16, 229 (2016). https://doi.org/10.1186/s12872-016-0414-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-016-0414-0