
Abstract
Objectives
The association between concentrations of sulfur dioxide (SO2), nitrogen dioxide (NO2), carbon monoxide (CO), ozone (O3), and emergency ambulance dispatches (EADs) for asthma was explored in the central Sichuan Basin of southwestern China for the first time.
Methods
EADs for asthma were collected from the Chengdu First-Aid Command Center. Pollutant concentrations were collected from 24 municipal environmental monitoring centers and including SO2, NO2, CO, daily 8-h mean concentrations of O3 (O3-8 h), and particulate matter less than 2.5 μm in aerodynamic diameter (PM2.5). The climatic data were collected from the Chengdu Municipal Meteorological Bureau. All data were collected from years spanning 2013–2017. A time-stratified case-crossover design was used to analyze the data.
Results
After controlling for temperature, relative humidity, and atmospheric pressure, IQR increases in SO2 (13 μg/m3), NO2 (17 μg/m3), and CO (498 μg/m3) were associated with 18.8%, 11.5%, and 3.1% increases in EADs for asthma, respectively. The associations were strongest for EADs and SO2, NO2, and CO levels with 3-, 5-, and 1-day lags, respectively.
Conclusions
This study provides additional data to the limited body of literature for potential health risks arising from ambient gaseous pollutants. The results of the study suggest that increased concentrations of SO2, NO2, and CO were positively associated with emergency ambulance dispatches for asthma in Chengdu, China. Further studies are needed to investigate the effects of individual air pollutants on asthma.
Similar content being viewed by others


Introduction
Asthma is one of the most common chronic diseases globally. As many as 300 million people currently have asthma, and it accounts for about 1 in 250 deaths worldwide. Moreover, the prevalence and patient burden from asthma have been sharply increasing [1]. Estimates for the costs of asthma in six developed countries range from $300 to $1300 per patient per year adjusted to 1990 US dollars [2]. Additional analyses indicate that asthma is estimated to cost 1–2% of the total health care budget of developed economies. In particular, asthma prevalence is sharply rising in developing countries and regions with increasing urbanization and westernization when compared to developed countries.
Previous studies have demonstrated the relationship between ambient air pollutants and asthma [3,4,5,6]. For example, associations have been detected between ambient air pollutant concentrations and the rate of pediatric asthma emergency department visits in Atlanta, USA [7]. Furthermore, Cai et al. (2014) reported that sulfur dioxide (SO2) and nitrogen dioxide (NO2) levels are more associated with asthma hospitalization events in Shanghai, China compared to levels of particulate matter with aerodynamic diameters less than 10 μm (PM10) [3]. The effects of air pollutants on asthma prevalence can also be associated with specific geographic terrains, weather conditions, and ethnic populations [8,9,10,11]. Following these previous analyses, the goal of the present study was to evaluate the association between short-term exposure to ambient gaseous pollutants (SO2, NO2, carbon monoxide (CO), and ozone (O3)) and emergency ambulance dispatches (EADs) for asthma in a typical basin of southwestern China.
The prevalence of gaseous pollutants including SO2, NO2, CO, and O3 were evaluated in comparison with asthma prevalence in the Sichuan Basin. The Sichuan Basin is a typical basin of southwestern China and exhibits severe air pollution [12]. To our knowledge, this report is the first to investigate the association between gaseous pollutants and asthma in this region, and thus, represents an important contribution to understanding the relationship between pollution and asthma for this region, and in general. The city of Chengdu was used as the study area, which comprises a population of over 15 million people [13]. Chengdu features its own unique geographical and meteorological conditions that are due to its location at the central region of the Sichuan Basin. EADs for asthma cases were investigated that encompassed cases across the whole city owing to data from the city’s Municipal First-Aid Command System. The association between air pollutants and EADs for asthma has rarely been explored in previous studies. However, some studies have explored the associations between air pollutants and EADs for cardiovascular diseases, respiratory diseases, and other systemic diseases [14, 15]. Consequently, we conducted a time-stratified case-crossover experimental design to explore the association between ambient gaseous pollutants and EADs for asthma in the central Sichuan Basin of China for the first time.
Materials and methods
Data collection
Data for EADs from asthma were collected from the Chengdu First-Aid Command Center from 1 January 2013 to 31 December 2017. The Chengdu First-Aid Command Center responds to all emergency calls for first aid in Chengdu, dispatches ambulances to transport patients to emergency hospitals, and serves residents of the entire city. EAD records include the patient identification number, gender, age, dispatch date, patient address, address code, chief complaint, and primary diagnosis. When a patient conducts an emergency call (number 120), their primary information including gender, age, and chief complaint is queried and recorded by operators at the Chengdu First-Aid Command Center. Patient identification numbers and dispatch dates are concomitantly generated automatically by the system. Primary diagnoses for patients are obtained by return calling the emergency hospital where the patient was dispatched immediately following the diagnosis. All case data from 1 January 2013 to 31 December 2017 were initially collected, and then only those with a primary diagnosis of asthma were used further.
Air pollutant concentrations were collected from all 24 Municipal Environmental Monitoring Centers in Chengdu from 1 January 2013 to 31 December 2017 (Fig. 1) and comprised data for SO2, NO2, CO, daily 8-h mean concentrations of O3 (O3-8 h), and particulate matter with aerodynamic diameters less than 2.5 μm (PM2.5). Daily mean concentrations for SO2, NO2, CO, O3-8 h, and PM2.5 were calculated using data for each pollutant from all 24 centers. Daily 8-h mean concentrations of O3 were defined as the highest 8-h mean concentration for O3 per day. If data from one or more centers were missing for a given day, data from the other centers would be used to calculate the mean concentrations that individuals were exposed to. Numerous previous analyses have considered weather conditions as confounding factors that should be adequately controlled for [16, 17]. Therefore, climatic parameters were collected from the Chengdu Municipal Meteorological Bureau from 1 January 2013 to 31 December 2017 that included daily mean temperature, relative humidity, and atmospheric pressure.

Study area and study locations within the city of Chengdu, China. The enlarged area depicts the spatial distribution of the 24 municipal environmental monitoring centers throughout Chengdu
Statistic analyses
Spearman’s correlational analyses were used to explore correlations between air pollutants and weather conditions. To estimate the association between gaseous pollutants and EADs for asthma, a time-stratified case-crossover methodology was used. The case-crossover method restricts the controls to the cases themselves. Consequently, the influence of confounding variables related to individual characteristics like gender, age, occupational hazards, smoking, and basic disease could be adequately controlled [18]. The R package “season” was used, allowing alternative values of controls to be set in the model. Time stratification was conducted to control for confounding variables due to long-term trends, seasonal patterns, and the day of the week [19]. Controls were restricted to the same weekday within the same month and year, relative to the corresponding cases. By controlling in this manner, the influences of trends due to time (long-term trends and seasonal patterns) and the day of the week are mitigated. The number of controls that were used was varied from three to four according to the number of days in a month. For example, if a case was dispatched to an emergency hospital on Friday, 23 September 2016, the case day was defined as the same day, and control days were assigned as all of the remaining Fridays in September 2016 (i.e., the 2nd, 9th, 16th, and 30th).
Delayed effects might exist between gaseous pollutant exposure and health outcomes [20,21,22]. To assess the potential for delayed effects on EAD instances for asthma, a single-day lag model for each gaseous pollutant was conducted by ranging the lag days from one to seven.
The influence of confounding variables including daily mean temperature, relative humidity, and atmospheric pressure was controlled by using natural cubic splines (ns) in the R software environment with 3° of freedom for smoothing in all models [23].
Sensitivity analyses were conducted in several manners to assess the robustness of the results. First, the setting of controls was varied. Three controls were restricted to one case in the models, while ignoring if cases and controls originated from the same month [24, 25]. Second, a two-pollutant model was assessed for each pollutant. Third, a multi-day moving average was calculated for pollutant concentrations extending from the day of analysis and up to 3 days prior (lag 01, lag 02, and lag 03, respectively). The concentrations for each pollutant from the day of EAD to 1-, 2-, and 3-days prior were used to calculate moving average concentrations to approximate exposures, rather than calculating mean concentrations for each pollutant on each day.
Model results are presented as odds ratios (ORs) with 95% confidence intervals (95% CI) with increased concentrations of each pollutant given per interquartile range (IQR) [25, 26]. The season package for R (version 3.5.1) was used for fitting the time-stratified case-crossover model [27].
Results
A total of 2669 EADs for asthma were observed in Chengdu between 1 January 2013 and 31 December 2017. The mean concentrations of SO2, NO2, CO, O3-8 h, and PM2.5 were 21.6, 41.5, 1124.2, 92.4, and 70.5 μg/m3, respectively, while increases in their IQRs were 13, 17, 498, 74, and 53 μg/m3, respectively. The values for mean daily temperature, relative humidity, and atmospheric pressure were 17.0 °C, 77.7%, and 951.7 hpa, respectively (Table 1).
Spearman’s correlation analysis indicated the presence of correlations among several air pollutants, including SO2 and NO2 (r = 0.474, P < 0.05), SO2 and CO (r = 0.615, P < 0.05), SO2 and O3-8 h (r = − 0.047, P < 0.05), SO2 and PM2.5 (r = 0.622, P < 0.05), NO2 and CO (r = 0.678, P < 0.05), NO2 and O3-8 h (r = − 0.195, P < 0.05), NO2 and PM2.5 (r = 0.785, P < 0.05), CO and O3-8 h (r = − 0.383, P < 0.05), CO and PM2.5 (r = 0.817, P < 0.05), and O3-8 h and PM2.5 (r = − 0.205, P < 0.05). In addition, correlations were observed between air pollutants and weather conditions (Table 2). The concentrations of SO2, NO2, and CO were remarkably higher during winter than during summer, while O3 concentrations were highest in the summers of each year. The EADs were also relatively higher during winters (Fig. 2).

Seasonal trends of monthly mean concentrations of SO2, NO2, CO, and O3, and EADs
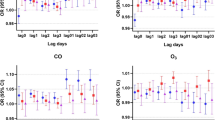
After controlling for temperature, relative humidity, and atmospheric pressure, an IQR increase (13 μg/m3) of SO2 was significantly and positively associated with EADs for asthma at lag 2 day (OR = 1.126, 95% CI 1.014–1.251) and lag 3 day (OR = 1.188, 95% CI 1.075–1.312). In addition, an IQR increase (17 μg/m3) for NO2 was significantly and positively associated with EADs for asthma at lag 0 day (OR = 1.086, 95% CI 1.009–1.168), lag 3 day (OR = 1.111, 95% CI 1.031–1.197), lag 4 day (OR = 1.093, 95% CI 1.015–1.176), lag 5 day (OR = 1.115, 95% CI 1.036–1.200), and lag 6 day (OR = 1.103, 95% CI 1.026–1.187). Finally, an IQR increase (498 μg/m3) of CO was significantly and positively associated with EADs for asthma at lag 1 day (OR = 1.031, 95% CI 1.003–1.059) (Fig. 3). The days corresponding to the greatest effects due to SO2, NO2, and CO were 3, 5, and 1 day lags, respectively.

Association between EADs for asthma and IQR increases for SO2, NO2, CO, and O3 over lag 0 to lag 7 days. All models were adjusted for temperature, relative humidity, and atmospheric pressure
In the two-pollutant models, there was an association between cases and SO2 at lag 3 day after adjusting for PM2.5 (OR = 1.204, 95% CI 1.058–1.371), NO2 (OR = 1.157, 95% CI 1.004–1.333), CO (OR = 1.193, 95% CI 1.077–1.321), and O3 (OR = 1.174, 95% CI 1.060–1.301). There was also an observed association between cases and NO2 at lag 5 day after adjusting for SO2 (OR = 1.158, 95% CI 1.042–1.288), CO (OR = 1.115, 95% CI 1.034–1.202), and O3 (OR = 1.111, 95% CI 1.031–1.197). Lastly, an association was observed for CO at lag 1 day after adjusting for SO2 (OR = 1.029, 95% CI 1.001–1.058) and O3 (OR = 1.032, 95% CI 1.004–1.060) (Table 3).
Restricting three fixed controls to one case instead of restricting cases and controls to being from the same month resulted in similar values and trends of ORs for each pollutant (Fig. 4). In addition, ORs calculated via different lag-day structures (lag 01, lag 02, and lag 03, respectively) were similar to those from the single-day lag models (Table 4). Thus, these sensitivity analyses suggest that the results of the models were reliable.

Association between EADs for asthma and IQR increases in SO2, NO2, CO, and O3 levels with lag 0 to lag 7 days. The results derive from controlled analyses after altering the lag structure for each pollutant by restricting three fixed controls to one case
Discussion
A significantly positive association was observed between EADs and gaseous pollutants when using a time-stratified case-crossover methodology. After controlling for temperature, relative humidity, and atmospheric pressure, IQR increases in SO2 (13 μg/m3), NO2 (17 μg/m3), and CO (498 μg/m3) were associated with 18.8%, 11.5%, and 3.1% increases in EADs for asthma, respectively. These effects were most notable for SO2, NO2, and CO at 3-, 5-, and 1-day lags, respectively. Furthermore, associations were observed between EADs for asthma and SO2 and NO2 when using lag models with other days of lag. Delay effects were only observed between asthma and exposure to SO2, CO, and EADs, but not between asthma incidences and NO2. Moreover, the health impacts of NO2 exposure as measured by EADS for asthma were similar among 3- to 6–day lag windows. IQR increases for NO2 at 3-, 4-, 5-, and 6-day lags were associated with 11.1%, 9.3%, 11.5%, and 10.3% increases in EADs for asthma, respectively, indicating that there may be a plateauing lag period for the association between NO2 and EADS for asthma. Several studies have suggested that further investigations are needed to evaluate the association between O3 and asthma in the Sichuan Basin [28, 29]. However, an association between exposure to O3 and EADs for asthma was not observed in our analyses. The major sources of SO2, NO2, CO, and O3 pollutants in Chengdu arise from industrial emissions and fuel combustion. In addition, traffic emissions also contribute to ambient NO2 and CO levels [30, 31]. The concentrations of gaseous pollutants exhibited typical seasonal trends. Specifically, the concentrations of SO2, NO2, and CO were remarkably higher during winters, which may be due to reduced dilution efficiency via air flow diffusion, and increases in biomass fuel combustion for heating. In addition, higher O3 concentrations in summer were likely caused by increased sunlight. Nevertheless, the aforementioned seasonal trends were accounted for in our analyses by using the case-crossover method.
The results reported here are consistent with those from previous studies. Ding et al. [32] explored the association between air pollution and hospital visits for asthma attack in children of Chongqing, China using a case-crossover analysis. The analysis indicated that increases of 10 μg/m3 concentrations in SO2, NO2, and CO were associated with 4.2%, 9.0%, and 0.4% increases in hospital visits for asthma attacks in children [32]. Furthermore, an analysis of several cities in the USA, including Atlanta, Dallas, and St. Louis [33], revealed associations between pollutant concentrations and asthma emergency department visits. In particular, the associations were strongest for patients in the 5–18-year age group, wherein the ratios per IQR (5 p.p.b. for SO2, 12 p.p.b. for NO2, 0.5 p.p.m. for CO, and 28 p.p.b. for O3) were 1.01%, 1.05%, 1.03, and 1.07%, respectively. Similarly, a cohort study in Denmark comprising 53,695 people [34] indicated that NO2 levels were associated with increased risk of hospitalization for asthma, with an adjusted hazard ratio per IQR (5.8 μg/m3) of 1.12. Likewise, a cohort study of 5349 children attending kindergarten and first grade in Southern California [35] revealed associations between new-onset asthma and NO2 levels.
The lag days exhibiting the greatest effect for each pollutant were used for two-pollutant models. Modeling revealed that ORs for NO2 decreased after adjusting for PM2.5, and a similar decrease was observed for CO after adjusting for PM2.5, and NO2. These results are consistent with those from previous studies [32], indicating the presence of synergistic effects among air pollutants towards disease incidence.
SO2 has long been considered an environmental cause of asthma. For example, Romanoff discussed the toxic effects of SO2 fume inhalation on bronchial asthma in 1939 [36]. One possible mechanism underlying aggravation of asthma by SO2 could be that SO2 derivatives increase the expression levels of EGF, EGFR, ICAM-1, and COX-2 proteins in BEP2D cells. The upregulation of these proteins then results in mucus over-production and inflammatory responses [37]. An experiment with newborn Sprague–Dawley rats sensitized to ovalbumin revealed that SO2 could be a universal factor in airway inflammatory processes that specifically exacerbates airway hyperresponsiveness (AHR) in asthmatics [38]. The underlying mechanism of this response could be due to increases in Penh (an indicator of AHR), that then increases antibody IL-4 production in serum and increases airway smooth muscle cell stiffness and contractility.
Exposure to ambient NO2 may enhance bronchial hypersensitivity to asthma, promote allergen sensitization to inhaled antigens, and increase the risk of exacerbating asthma following respiratory infections [39,40,41,42]. Mechanisms underlying the exacerbation of asthma by NO2 that may be of particular significance include the following: (1) enhancing induction of apoptosis in normal human bronchial epithelial cells and inducing cell damage [43]. 2) Inducing an upregulation of IL-5, IL-10, IL-13, and ICAM-1 antibodies in the bronchial epithelium, thereby exerting a “pro-allergic” effect [44].
A relationship between ambient CO levels and asthma incidence has been demonstrated in many previous studies [7, 32, 33, 45, 46]. However, the biological mechanism underlying this association has not yet been determined. Norris et al. (1999) considered CO as a general indicator for the effects of air pollution [47]. In contrast to the above studies, recent studies have suggested that CO may potentially play a protective role in respiratory systems [48]. Ameredes et al. (2003) reported that exposure to CO could reduce airway hyperresponsiveness in mice [49]. Further, the study suggested that the response was associated with a guanosine-3,5-monophosphate (cGMP) mechanism both in the presence and absence of airway inflammation. Moreover, Song et al. (2002) suggested that CO could induce significant antiproliferative effects for human airway smooth muscle cells [50]. Thus, further studies are needed to more clearly discern the mechanism underlying the exacerbation of asthma by CO.
This study features three distinct strengths that increase the significance of the observations reported here. First, this is the first study to explore the association between gaseous pollutants and EADs for asthma in the central Sichuan Basin of southwestern China. Although the Bejing–Sichuan belt is located in one of two severe air pollution belts of China [12], investigations of pollution and pollution risks have lagged in the Sichuan Basin due to the relatively depressed economic conditions in the region [13]. The recent improvement and establishment of monitoring systems in the Sichuan Basin have provided opportunities to now conduct such investigations. In addition, several factors render the area a unique research resource that can help fill knowledge-gaps concerning pollution risks in the region. These include the uniquely dense population, different sources of air pollutants, different diffusional dilution conditions, and significantly different economic levels in the Sichuan Basin compared to eastern areas and cities. Second, emergency ambulance dispatch data for the whole city were used in our study due to the unique advantage of the Chengdu First-Aid Command System. City-wide data such as these have been rarely used in previous studies. Third, the city of Chengdu is large and densely populated, which is advantageous for assessing the effects of air pollutants on disease incidence.
However, some limitations were also evident in this study. First, concentrations of air pollutants were obtained from fixed municipal environmental monitoring centers, and thus, individual exposure data were not evaluated. Second, this study was conducted for the central Sichuan Basin. The specific geographical features and weather conditions of the region should be considered, and generalizations of these results should be treated cautiously. Third, not all asthma patients call for emergency ambulances when disease states occur. Consequently, we conducted a time-stratified case-crossover analysis based on individuals from which cumulative effects could not be obtained.
Conclusions
This study provides important data to advance our limited understanding of potential health risks due to ambient gaseous pollutants. Importantly, these data suggest that increased concentrations of SO2, NO2, and CO were significantly and positively associated with emergency ambulance dispatches for asthma in Chengdu, China. Further studies are needed to assess the effects of various individual air pollutants on asthma.
Abbreviations
- AP:
-
Atmospheric pressure
- CI:
-
Confidence interval
- CO:
-
Carbon monoxide
- EADs:
-
Emergency ambulance dispatches
- IQR:
-
Interquartile range
- NO2 :
-
Nitrogen dioxide
- O3 :
-
Ozone
- O3-8 h:
-
Daily 8-h mean concentration for O3
- OR:
-
Odds ratio
- PM2.5 :
-
Particulate matter less than 2.5 μm in aerodynamic diameter
- SD:
-
Standard deviation
- SO2 :
-
Sulfur dioxide
- tpd:
-
Times per day
References
Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma: executive summary of the GINA dissemination committee report. Allergy. 2004;59(5):469–78.
Sullivan S, Elixhauser A, Buist AS, Luce BR, Eisenberg J, Weiss KB. National Asthma Education and Prevention Program working group report on the cost effectiveness of asthma care. Am J Respir Crit Care Med. 1996;154(3_pt_2):S84–95.
Cai J, Zhao A, Zhao J, Chen R, Wang W, Ha S, Xu X, Kan H. Acute effects of air pollution on asthma hospitalization in Shanghai, China. Environ Pollut. 2014;191:139–44.
Chen K, Glonek G, Hansen A, Williams S, Tuke J, Salter A, Bi P. The effects of air pollution on asthma hospital admissions in Adelaide, South Australia, 2003–2013: time-series and case–crossover analyses. Clin Exp Allergy. 2016;46(11):1416–30.
Nishimura KK, Galanter JM, Roth LA, Oh SS, Thakur N, Nguyen EA, Thyne S, Farber HJ, Serebrisky D, Kumar R, et al. Early-life air pollution and asthma risk in minority children. The GALA II and SAGE II studies. Am J Respir Crit Care Med. 2013;188(3):309–18.
Pénard-Morand C, Raherison C, Charpin D, Kopferschmitt C, Lavaud F, Caillaud D, Annesi-Maesano I. Long-term exposure to proximity air pollution and asthma and allergies in urban children. Eur Respir J. 2010;36(1):33–40.
Strickland MJ, Darrow LA, Klein M, Flanders WD, Sarnat JA, Waller LA, Sarnat SE, Mulholland JA, Tolbert PE. Short-term associations between ambient air pollutants and pediatric asthma emergency department visits. Am J Respir Crit Care Med. 2010;182(3):307–16.
Bowatte G, Lodge C, Lowe AJ, Erbas B, Perret J, Abramson MJ, Matheson M, Dharmage SC. The influence of childhood traffic-related air pollution exposure on asthma, allergy and sensitization: a systematic review and a meta-analysis of birth cohort studies. Allergy. 2015;70(3):245–56.
Grineski SE, Staniswalis JG, Peng Y, Atkinson-Palombo C. Children’s asthma hospitalizations and relative risk due to nitrogen dioxide (NO2): effect modification by race, ethnicity, and insurance status. Environ Res. 2010;110(2):178–88.
Guan W-J, Zheng X-Y, Chung KF, Zhong N-S. Impact of air pollution on the burden of chronic respiratory diseases in China: time for urgent action. Lancet. 2016;388(10054):1939–51.
Samoli E, Nastos PT, Paliatsos AG, Katsouyanni K, Priftis KN. Acute effects of air pollution on pediatric asthma exacerbation: evidence of association and effect modification. Environ Res. 2011;111(3):418–24.
Han L, Zhou W, Li W, Li L. Impact of urbanization level on urban air quality: a case of fine particles (PM2.5) in Chinese cities. Environ Pollut. 2014;194:163–70.
http://tjj.sc.gov.cn/tjcbw/tjnj/2017/zk/indexch.htm. Accessed 8 Oct 2018.
Liu R, Zeng J, Jiang X, Chen J, Gao X, Zhang L, Li T. The relationship between airborne fine particle matter and emergency ambulance dispatches in a southwestern city in Chengdu, China. Environ Pollut. 2017;229:661–7.
Michikawa T, Ueda K, Takeuchi A, Tamura K, Kinoshita M, Ichinose T, Nitta H. Coarse particulate matter and emergency ambulance dispatches in Fukuoka, Japan: a time-stratified case-crossover study. Environ Health Prev Med. 2015;20(2):130–6.
Chen R, Huang W, Wong CM, Wang Z, Thach TQ, Chen B, Kan H, Group CC. Short-term exposure to sulfur dioxide and daily mortality in 17 Chinese cities: the China air pollution and health effects study (CAPES). Environ Res. 2012;118:101–6.
Tao Y, Mi S, Zhou S, Wang S, Xie X. Air pollution and hospital admissions for respiratory diseases in Lanzhou, China. Environ Pollut. 2014;185:196–201.
Yang C, Peng X, Huang W, Chen R, Xu Z, Chen B, Kan H. A time-stratified case-crossover study of fine particulate matter air pollution and mortality in Guangzhou, China. Int Arch Occup Environ Health. 2012;85(5):579–85.
Guo Y, Tong S, Zhang Y, Barnett AG, Jia Y, Pan X. The relationship between particulate air pollution and emergency hospital visits for hypertension in Beijing, China. Sci Total Environ. 2010;408(20):4446–50.
Belleudi V, Faustini A, Stafoggia M, Cattani G, Marconi A, Perucci CA, Forastiere F. Impact of fine and ultrafine particles on emergency hospital admissions for cardiac and respiratory diseases. Epidemiology. 2010;21(3):414–23.
Kamouchi M, Ueda K, Ago T, Nitta H, Kitazono T. Fukuoka stroke registry I: relationship between asian dust and ischemic stroke: a time-stratified case-crossover study. Stroke. 2012;43(11):3085–7.
Yang Y, Cao Y, Li W, Li R, Wang M, Wu Z, Xu Q. Multi-site time series analysis of acute effects of multiple air pollutants on respiratory mortality: a population-based study in Beijing, China. Sci Total Environ. 2015;508:178–87.
Hastie TJ. Generalized linear models. Statistical models in S; 1992.
Janes H, Sheppard L, Lumley T. Case-crossover analyses of air pollution exposure data: referent selection strategies and their implications for bias. Epidemiology. 2005;16(6):717–26.
Jung CR, Young LH, Hsu HT, Lin MY, Chen YC, Hwang BF, Tsai PJ. PM2.5 components and outpatient visits for asthma: a time-stratified case-crossover study in a suburban area. Environ Pollut. 2017;231(Pt 1):1085–92.
Lin H, An Q, Luo C, Pun VC, Chan CS, Tian L. Gaseous air pollution and acute myocardial infarction mortality in Hong Kong: a time-stratified case-crossover study. Atmos Environ. 2013;76:68–73.
Guo Y, Tong S, Li S, Barnett AG, Yu W, Zhang Y, Pan X. Gaseous air pollution and emergency hospital visits for hypertension in Beijing, China: a time-stratified case-crossover study. Environ Health. 2010;9(1):57.
Lin S, Liu X, Le LH, Hwang S-A. Chronic exposure to ambient ozone and asthma hospital admissions among children. Environ Health Perspect. 2008;116(12):1725–30.
McDonnell WF, Abbey DE, Nishino N, Lebowitz MD. Long-term ambient ozone concentration and the incidence of asthma in nonsmoking adults: the Ahsmog study. Environ Res. 1999;80(2):110–21.
Chen T-M, Kuschner WG, Gokhale J, Shofer S. Outdoor air pollution: nitrogen dioxide, sulfur dioxide, and carbon monoxide health effects. Am J Med Sci. 2007;333(4):249–56.
Li J, Wang Z, Akimoto H, Yamaji K, Takigawa M, Pochanart P, Liu Y, Tanimoto H, Kanaya Y. Near-ground ozone source attributions and outflow in central eastern China during MTX2006. Atmos Chem Phys. 2008;8(24):7335–51.
Ding L, Zhu D, Peng D, Zhao Y. Air pollution and asthma attacks in children: a case–crossover analysis in the city of Chongqing, China. Environ Pollut. 2017;220:348–53.
Alhanti BA, Chang HH, Winquist A, Mulholland JA, Darrow LA, Sarnat SE. Ambient air pollution and emergency department visits for asthma: a multi-city assessment of effect modification by age. J Exposure Sci Environ Epidemiol. 2015;26:180.
Andersen ZJ, Bønnelykke K, Hvidberg M, Jensen SS, Ketzel M, Loft S, Sørensen M, Tjønneland A, Overvad K, Raaschou-Nielsen O. Long-term exposure to air pollution and asthma hospitalisations in older adults: a cohort study. Thorax. 2011;67(1):6–11.
McConnell R, Islam T, Shankardass K, Jerrett M, Lurmann F, Gilliland F, Gauderman J, Avol E, Künzli N, Yao L, et al. Childhood incident asthma and traffic-related air pollution at home and school. Environ Health Perspect. 2010;118(7):1021–6.
Romanoff A. Sulfur dioxide poisoning as a cause of asthma. J Allergy. 1939;10:166–9.
Li R, Meng Z, Xie J. Effects of sulfur dioxide derivatives on four asthma-related gene expressions in human bronchial epithelial cells. Toxicol Lett. 2007;175(1):71–81.
Song A, Liao Q, Li J, Lin F, Liu E, Jiang X, Deng L. Chronic exposure to sulfur dioxide enhances airway hyperresponsiveness only in ovalbumin-sensitized rats. Toxicol Lett. 2012;214(3):320–7.
Bevelander M, Mayette J, Whittaker LA, Paveglio SA, Jones CC, Robbins J, Hemenway D, Akira S, Uematsu S, Poynter ME. Nitrogen dioxide promotes allergic sensitization to inhaled antigen. J Immunol. 2007;179(6):3680–8.
Linaker CH, Coggon D, Holgate ST, Clough J, Josephs L, Chauhan AJ, Inskip HM. Personal exposure to nitrogen dioxide and risk of airflow obstruction in asthmatic children with upper respiratory infection. Thorax. 2000;55(11):930–3.
Orehek J, Massari JP, Gayrard P, Grimaud C, Charpin J. Effect of short-term, low-level nitrogen dioxide exposure on bronchial sensitivity of asthmatic patients. J Clin Invest. 1976;57(2):301–7.
Strand V, Rak S, Svartengren M, Bylin G. Nitrogen dioxide exposure enhances asthmatic reaction to inhaled allergen in subjects with asthma. Am J Respir Crit Care Med. 1997;155(3):881–7.
Ayyagari VN, Januszkiewicz A, Nath J. Effects of nitrogen dioxide on the expression of intercellular adhesion molecule-1, neutrophil adhesion, and cytotoxicity: studies in human bronchial epithelial cells. Inhal Toxicol. 2007;19(2):181–94.
Pathmanathan S, Krishna MT, Blomberg A, Helleday R, Kelly FJ, Sandström T, Holgate ST, Wilson SJ, Frew AJ. Repeated daily exposure to 2 ppm nitrogen dioxide upregulates the expression of IL-5, IL-10, IL-13, and ICAM-1 in the bronchial epithelium of healthy human airways. Occup Environ Med. 2003;60(11):892–6.
Clark NA, Demers PA, Karr CJ, Koehoorn M, Lencar C, Tamburic L, Brauer M. Effect of early life exposure to air pollution on development of childhood asthma. Environ Health Perspect. 2010;118(2):284–90.
Lin M, Chen Y, Burnett RT, Villeneuve PJ, Krewski D. Effect of short-term exposure to gaseous pollution on asthma hospitalisation in children: a bi-directional case-crossover analysis. J Epidemiol Community Health. 2003;57(1):50–5.
Norris G, YoungPong SN, Koenig JQ, Larson TV, Sheppard L, Stout JW. An association between fine particles and asthma emergency department visits for children in Seattle. Environ Health Perspect. 1999;107(6):489–93.
Ryter SW, Kim HP, Nakahira K, Zuckerbraun BS, Morse D, Choi AMK. Protective functions of heme oxygenase-1 and carbon monoxide in the respiratory system. Antioxid Redox Signal. 2007;9(12):2157–73.
Ameredes BT, Otterbein LE, Kohut LK, Gligonic AL, Calhoun WJ, Choi AMK. Low-dose carbon monoxide reduces airway hyperresponsiveness in mice. Am J Phys Lung Cell Mol Phys. 2003;285(6):L1270–6.
Song R, Mahidhara RS, Liu F, Ning W, Otterbein LE, Choi AMK. Carbon monoxide inhibits human airway smooth muscle cell proliferation via mitogen-activated protein kinase pathway. Am J Respir Cell Mol Biol. 2002;27(5):603–10.
Acknowledgements
We thank the Chengdu First-Aid Command Center, the Chengdu Municipal Environmental Monitoring Center, and the Chengdu Municipal Meteorological Bureau for providing data.
Funding
This study was funded by the Special Foundation of Basic Science and Technology Resources Survey of the Ministry of Science and Technology (No. 2017FY101200), the China Short-Term Health Effects of Air Pollution Study (China SHEAP Study; No. 2016YFC0206500), the Sichuan Provincial Medical Research Youth Innovation Project (No. Q17070), and the Sichuan Provincial Cadre Health Care Research Project (No. ZH2018-1801).
Availability of data and materials
The datasets used in the current study are available from the corresponding author for reasonable requests.
Author information
Authors and Affiliations
Contributions
JYC coordinated the study, performed the data analysis, and drafted the manuscript. XYJ, CLS, and RCL contributed to the statistical analyses. RL contributed to obtaining the air pollution and health data. LZ organized and coordinated the study, and edited the manuscript. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable. This study does not involve experimental animals or individual information of human subjects. The Chengdu First–Aid Command Center provided the data used in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chen, J., Jiang, X., Shi, C. et al. Association between gaseous pollutants and emergency ambulance dispatches for asthma in Chengdu, China: a time-stratified case-crossover study. Environ Health Prev Med 24, 20 (2019). https://doi.org/10.1186/s12199-019-0773-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12199-019-0773-0